
Abstract
Peritonitis caused by atypical and rare pathogens is challenging to diagnose. Although the International Society for Peritoneal Dialysis (ISPD) guidelines significantly improve the diagnostic rate by placing peritoneal dialysis fluid into blood culture bottles, peritonitis caused by atypical pathogens, such as tuberculosis and fungi, is difficult to diagnose due to challenges in culturing these organisms using traditional methods, leading to high mortality. Metagenomic next-generation sequencing (mNGS) technology has been widely used as an accurate diagnostic technique for infectious diseases. First used in identifying and quantifying environmental micro-organisms, mNGS technology can identify rare, novel, difficult-to-detect and mixed pathogens directly from clinical samples, and has potential in predicting antibiotic resistance. This paper summarizes the application of mNGS in atypical and rare pathogens peritonitis clinical cases in recent years, and provides reference for the diagnosis of peritonitis in combination with new ISPD guidelines and diagnostic techniques. The development and principles of mNGS technology, diagnostic efficiency in peritonitis, challenges in diagnosis of atypical and rare pathogen-associated peritonitis, and application of mNGS technology are discussed in detail. The development of mNGS technology provides clinicians with powerful tools to more accurately identify and treat peritonitis. Future research needs to focus on reducing costs, improving test accessibility, and developing new bioinformatics tools to better integrate mNGS results into clinical practice.
Keywords
Introduction
Peritoneal dialysis (PD) as a renal replacement therapy for end-stage renal disease patients has been favored by more and more uremic patients. 1 Although advances in technology and standardization of procedures have significantly reduced the incidence of peritonitis, according to an annual peritonitis incidence statistic that includes 33 national registries, the average peritonitis incidence rate decreased from 0.6 cases per patient year (PPY) in 1992 to 0.3 cases PPY in 2019. 2 However, peritonitis is still one of the main reasons for PD patients to withdraw from treatment. Even in the early stages of dialysis, more than one-third of patients withdrew due to infection. 3 The SONG-PD initiative also emphasizes that PD-related infection is the primary core outcome of PD and a core indicator of treatment quality.4,5 Among the pathogens of peritonitis, the most common microorganisms are aerobic bacteria, such as Staphylococcus aureus, coagulase-negative staphylococci. Gram-positive bacteria still dominate the proportion of peritonitis, and the culture-negative rate in many regions is still higher than the ISPD recommendation of 15%—Thailand (28%), Japan (21%), the United States (16%), and Canada (16%). 6 A recent study from Thailand suggested that up to 11% of cases may be caused by atypical pathogens of this type, including mycobacteria (2%) and fungi (9%). 7 According to the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS), fungal peritonitis accounts for only 1–3% of cases in various countries. 6 Despite this relatively low incidence, the diagnosis of atypical pathogens in culture-negative peritonitis remains challenging due to the low abundance of atypical pathogens and the limitations of conventional culture methods. This diagnostic difficulty may result in delayed treatment, which is associated with a higher mortality rate. This type of peritonitis occurs in cases of low immunity, malnutrition, antibiotic resistance, they may not be detected in conventional bacterial cultures, or because their culture conditions are special, require longer times and specific culture conditions, and are often difficult to treat, resulting in adverse outcomes and even death of patients. While the ISPD guidelines do not explicitly define the term “atypical pathogen-associated peritonitis,” they do discuss culture-negative peritonitis and organisms that are difficult to culture using conventional methods. These organisms include Mycobacterium tuberculosis, non-tuberculous mycobacteria (NTM), and rare pathogens such as Ureaplasma, Mycoplasma, anaerobes, and viruses. 8 Metagenomic next-generation sequencing (mNGS) technology, as a precision diagnostic tool for infectious diseases, has been widely applied. Initially used for the identification and quantification of environmental microbes, mNGS can directly detect rare, novel, hard-to-detect, and mixed pathogens from clinical samples and holds potential for predicting antibiotic resistance. 9 Therefore, this review summarizes and discusses mNGS used in clinical cases of atypical and rare pathogen peritonitis in recent years, aiming to provide a reference for peritonitis diagnosis in combination with updated ISPD guidelines and advances in new diagnostic techniques.
Development and principle of mNGS technology
Since the advent of the first-generation sequencing technology, great progress has been made in sequencing technology through continuous iteration of sequencing technology and sequencing platform. The mNGS continues to develop rapidly in the global sequencing market due to its high throughput, rapid turnaround, broad coverage, and ability to detect pathogens without prior assumptions, 10 which plays an important role in identifying complex and atypical infections (such as Chlamydia psittaci, Legionella, difficult-to-culture anaerobic bacteria and mycobacteria), zoonotic pathogens, newly emerging RNA and DNA viruses play an important role. 11 In previous reports, mNGS has been successfully applied to dozens of sample types such as cerebrospinal fluid, respiratory secretions, feces, urine, blood and tissues. 12 It has shown great advantages in diagnosing complex infections such as those associated with bloodstream infections, respiratory infections, bone and joint infections and encephalitis.13–16 The metagenomic sequencing process includes sample collection, transportation, nucleic acid extraction and enrichment, library sequencing, bioinformatics analysis, and suspicious pathogen reporting. Figure 1 shows a complete flow chart for mNGS testing of dialysate from peritonitis patients. A comprehensive nucleic acid sequencing process, including wet and dry experiments. Wet experiments involve extracting nucleic acids (RNA and DNA) from samples, performing reverse transcription of RNA, preparing sequencing libraries, and sequencing itself. The dry experimental steps include base calling, data preprocessing, removal of host nucleic acid sequences, database alignment, taxonomic classification, and ultimately identification of microorganisms. The entire process, from sample processing to data analysis, aims to identify the composition of sequencing libraries, which can be targeted, DNA amplified, or both. 18 Guidelines from various countries recommend minimizing any errors in the workflow in accordance with ISO (International Organization for Standardization) standards to ensure the accuracy and reliability of next-generation sequencing (NGS) in the diagnosis of infectious diseases.19–21 As the field of clinical mNGS continues to evolve, standardized protocols, bioinformatics workflows, and reference databases are crucial for facilitating the widespread adoption of mNGS in clinical microbiology laboratories. 22 The mNGS database includes reference genomes of humans and microorganisms, and the mNGS microbial genome database includes genomes of more than 12,000 bacteria, 18,000 fungi, 4600 viruses, and 100 parasites, with assembly quality reaching the standard of a complete genome or chromosome. 23 The Pathogens Metagenomics Database (PMDB) of BGI reported to include approximately 36,000 pathogens, covering a broad range of bacteria, viruses, fungi, and parasites, as well as drug-resistant genes. 17 The core equipment of mNGS technology mainly includes high-throughput sequencers, which are key tools for large-scale DNA or RNA sequencing. The current mainstream second-generation sequencing platforms include Illumina, which leads with its wide application and high market share, Thermo Fisher, which has an advantage in the clinical field with its fast and easy operation, and MGI Tech Co., Ltd (MIG), which stands out in the China market.
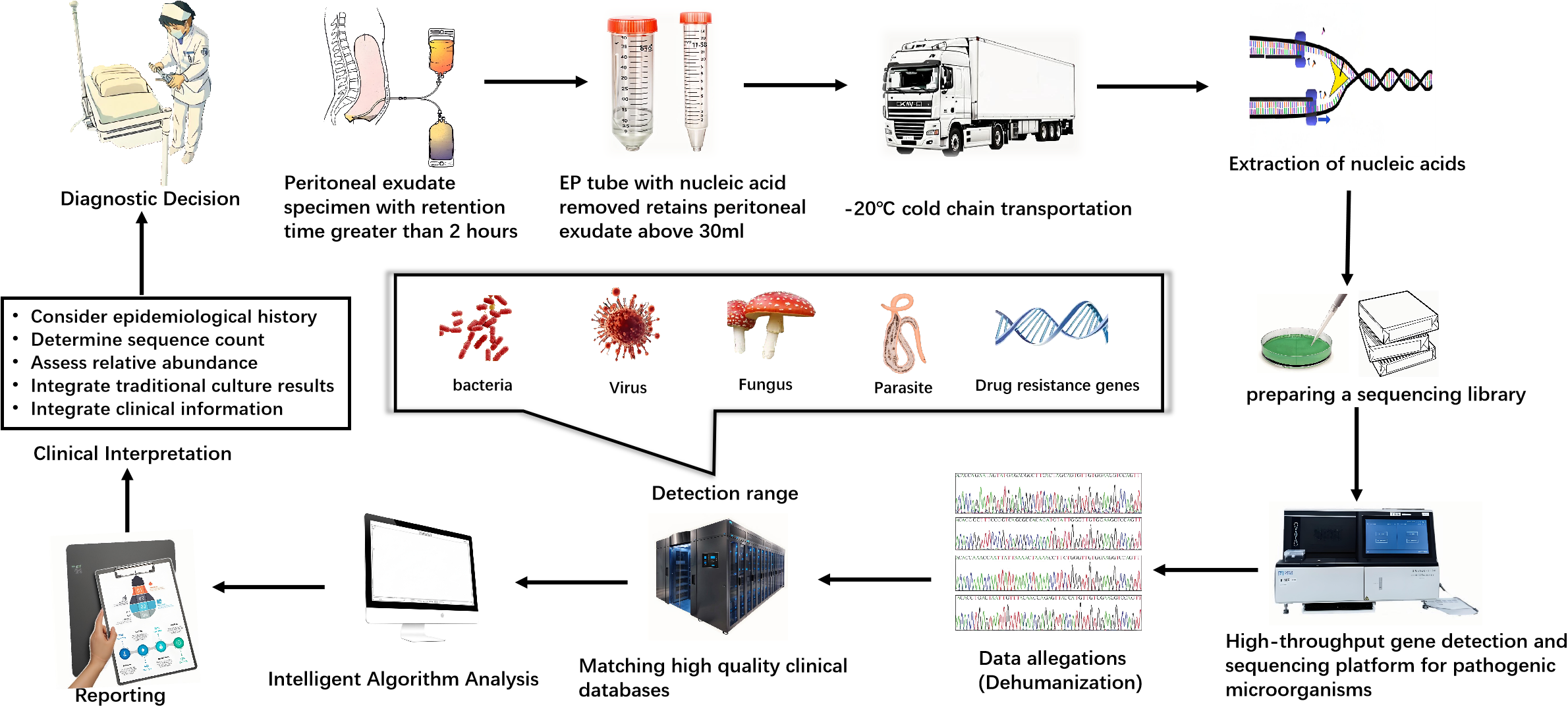
Schematic diagram of a general workflow for metagenomic next-generation sequencing for diagnostic clinical use. The detection process of mNGS in patients with peritonitis includes sample collection, transportation, nucleic acid extraction and enrichment, database sequencing, letter analysis and suspicious pathogen report. Nucleic acids of all microorganisms in dialysate were extracted and sequenced on a high-throughput sequencing platform. The PMDB of BGI reported to include approximately 36,000 pathogens, covering a broad range of bacteria, viruses, fungi, and parasites, as well as drug-resistant genes. 17 mNGS: metagenomic next-generation sequencing; PMDB: Pathogens Metagenomics Database.
Diagnostic efficacy of mNGS in peritoneal dialysis associated peritonitis
The updated ISPD 2022 guidelines recommend that the blood culture bottle(s) be the preferred technique for bacterial culture of PD effluent (PDE; 1C), and if more than 15% of peritonitis cases are culture-negative, sampling and culture methods should be reviewed and improved. 8 However, due to the presence of atypical pathogens and the problem of culture methods, the proportion of culture-negative peritonitis in some centers may even reach 40%. 24 The 2022 ISPD guidelines mention new technologies such as polymerase chain reaction (PCR) and 16SrRNA gene sequencing, but there is no evidence to prove that they are superior to traditional methods.8,25 A large sample study including 511 cases showed that the sensitivity of mNGS in detecting infectious and non-infectious diseases (50.7%) was significantly higher than that of culture (35.2%). 12 The development of mNGS technology provides a new way to diagnose the difficult diagnosis of peritonitis. Table 1 summarizes recent studies on mNGS in peritonitis. In 2020, the first report of a single-center study in southern China verified the detection efficiency of mNGS for peritonitis pathogens, and the detection rate of dialysate pathogens in mNGS was significantly higher than that of traditional culture method (86.67% vs. 60.00%, P = 0.039). 31 In another study, the sensitivity and specificity of mNGS method were 96.77% and 83.33%, and those of blood culture bottle method were 70.97% and 100%. 29 Compared with patients receiving antibiotic treatment, the negative rate of traditional culture method is higher. We can still use mNGS to confirm peritonitis on the day of peritonitis onset and within 2 days thereafter, cause the cell free-DNA (cfDNA) concentration in the PD fluid will increase during this period. 26 In another study of the diagnosis of peritonitis after antibiotic use, the mNGS method was superior to the blood culture bottle method. In the antibiotic use group, the positive rate was 92% with mNGS method and 38% with blood culture method (p = 0.016). 28 Moreover, the application of mNGS shortened the detection time, which was 25 (24–27) versus 89 (73–122) hours lower than that of the traditional microbial culture method (P < .001). 30 Although traditional culture can provide pathogen identification and drug sensitivity results within 48 h at the fastest, the rapid reporting time (about 25 h 30 ) of mNGS significantly shortens the time to diagnosis. For those patients with positive cultures, our moderately accelerated reporting time enables clinicians to adjust treatment earlier, reduce unnecessary broad-spectrum antibiotic use, and reduce the risk of superinfection and development of resistance. Finally, the ability to detect co-infections with multiple types of pathogens is that a significant advantage for mNGS, including (any type of organism, e.g., mixed infection of bacteria and virus), 34 about 15% of the infections found in cases using the mNGS method are multiple infections. 31
Metagenomic next generation sequencing (mNGS) studies in peritonitis.
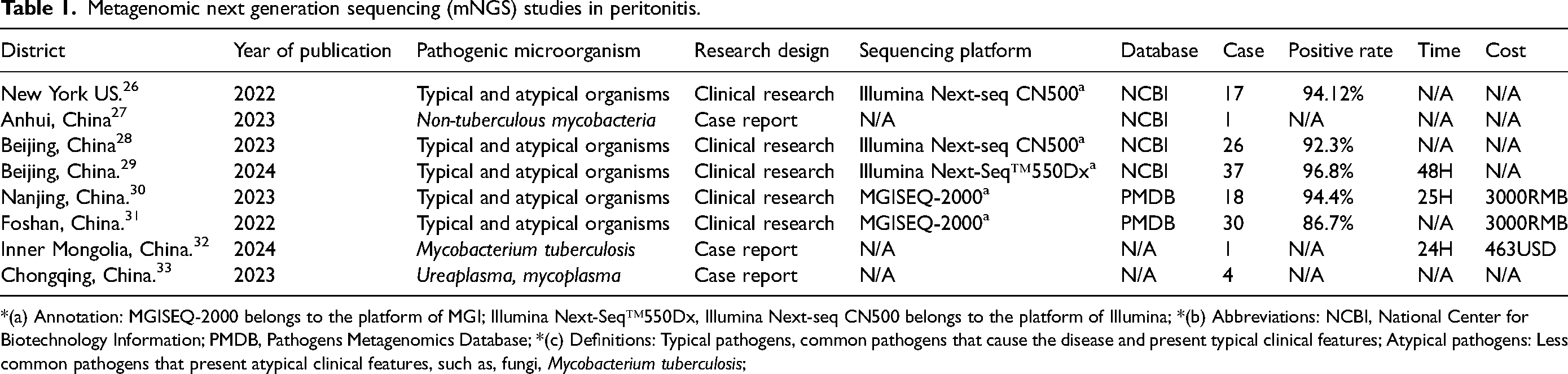
*(a) Annotation: MGISEQ-2000 belongs to the platform of MGI; lllumina Next-Seq™550Dx, lllumina Next-seq CN500 belongs to the platform of Illumina; *(b) Abbreviations: NCBI, National Center for Biotechnology Information; PMDB, Pathogens Metagenomics Database; *(c) Definitions: Typical pathogens, common pathogens that cause the disease and present typical clinical features; Atypical pathogens: Less common pathogens that present atypical clinical features, such as, fungi, Mycobacterium tuberculosis;
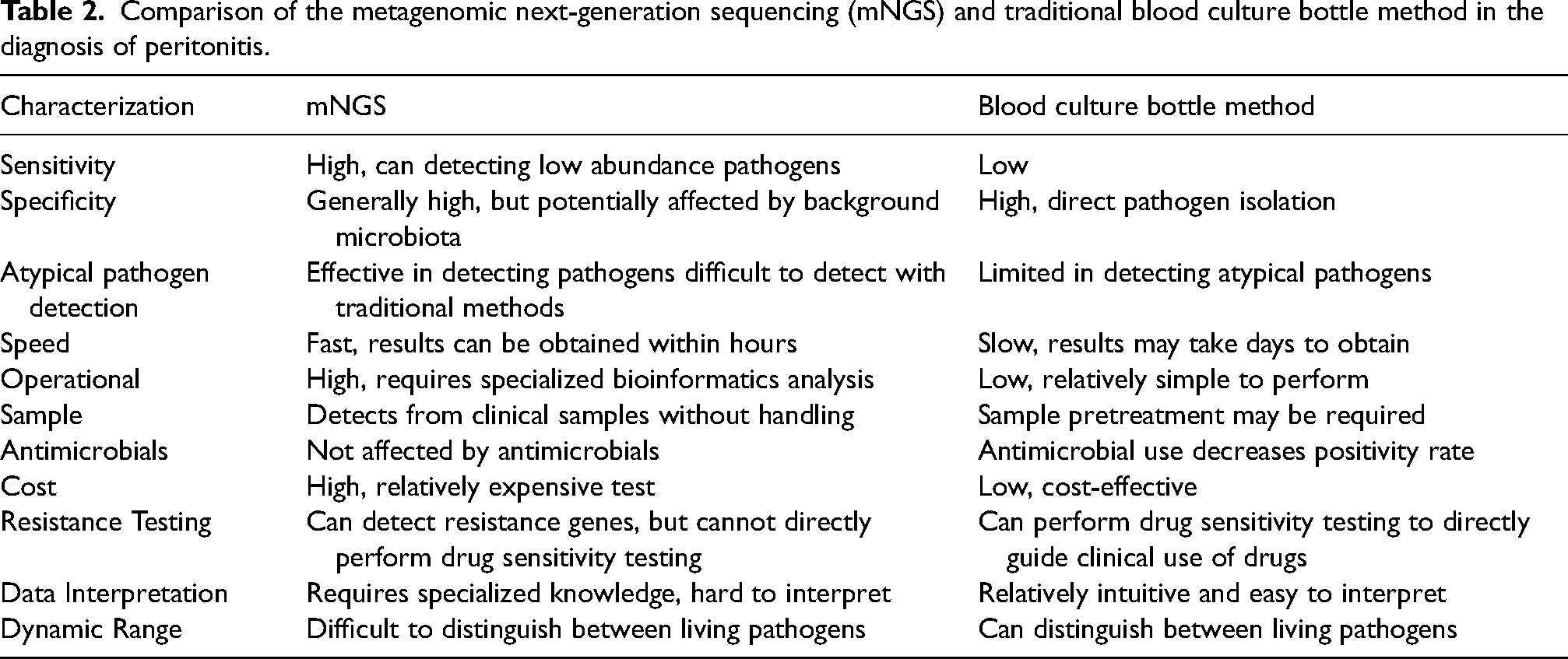
Comparison of the metagenomic next-generation sequencing (mNGS) and traditional blood culture bottle method in the diagnosis of peritonitis.
The limitations of mNGS in diagnosing peritonitis
Although mNGS has many traditional advantages, it still has some practical shortcomings. First, although the potential for cost reductions compared to traditional culture methods is large, ranging from $2000 to $4000 per sample, the high price and unfriendly health care policies discourage many patients.
35
The cost of a single mNGS test in Shanghai is approximately 3500 RMB, and it can increase to 4500–6500 RMB ($600–$900) for combined DNA/RNA analysis. However, costs may vary depending on the provider and the scope of the test.
36
Without medical insurance, it is still relatively expensive for ordinary people. In the next few years, the cost is expected to drop to 800–1000, or even lower, which will make it affordable for more patients. Despite this, the application of mNGS in certain clinical scenarios, such as severe pneumonia and neurological infections, has shown cost-effectiveness, especially in improving diagnostic accuracy and reducing medical costs.16,37 Second, the biological activity of pathogens cannot be determined by gene sequencing. Finally, mNGS cannot be used for drug sensitivity testing, the later can only be cultured by blood routine method. Lastly, mNGS cannot directly perform susceptibility testing which still relies on traditional blood culture methods. Although mNGS can detect bacterial resistance genes and sequence them, it is reported that in bone and joint infections, the accuracy of predicting antibiotic sensitivity is only 76.5%.
38
Although bacterial drug resistance genes can be detected, their rapid changes–such as mutations and horizontal transfer–can lead to dynamic changes in the resistance phenotype. For example, resistance genes in some bacteria may mutate under different environmental pressures, such as exposure to antibiotics, thereby altering their resistance characteristics. This dynamism creates uncertainty in predicting the microbial resistance phenotype based solely on the presence of resistance genes.
39
Since the essence of mNGS is the sequencing of pathogen genetic material (nucleic acids) for diagnosis, it cannot distinguish between live and dead bacteria in the sample. Even if the nucleic acid sequences of pathogens are detected, it cannot be determined whether these pathogens have the ability to cause infection. That is, the detection of pathogen sequences does not necessarily represent actual infection, which may lead to false-positive results. However in clinical practice, the pathogen sequences detected in the mNGS test reports are combined with clinical manifestations and common sense for comprehensive judgment. Microorganisms with low reads are not considered pathogenic, and should be considered as skin colonizing bacteria, contamination, or other false-positive results. It has been reported that mNGS is not more sensitive than culture in identifying common bacteria, which is able to identify the vast majority (74%) compared to sequencing, and that the mNGS technique for detecting common bacterial infections may not be as advantageous as atypical organisms for bacteria-associated pneumonia.12,40 It should be noted that although there is a high positive rate, both culture-positive and mNGS-negative results are found in these studies. This situation is interpreted as being due to the thick cell wall of some bacteria (Streptococcus), which makes it difficult to extract genetic material, but shows negative results. This also suggests that it is better for us to use both test methods together and verify each other. We have summarized the advantages and disadvantages of mNGS compared with traditional blood culture methods in
The mNGS utilization in clinical practice
China issued an expert consensus on the application of mNGS technology in critical infection detection in 2019, in which the following six indicators for mNGS detection were suggested: (1) Pathogens should be identified as soon as possible in critical cases; (2) pathogens should be identified as soon as possible for special patients such as immunosuppressed hosts, patients with underlying diseases, and patients with severe infections who have been repeatedly hospitalized; (3) patients with repeated negative traditional microbial detection techniques and poor treatment results; (4) suspected cases of new pathogens indicating possible clinical infectivity to some extent; (5) suspected cases of infection with specific pathogens; (6) chronic fever and/or infection with other clinical symptoms of unknown cause; 41 These application conditions are consistent with the treatment requirements for atypical pathogens and refractory peritonitis. The guidelines from the U.S. Food and Drug Administration (FDA) have also recognized the particular value of mNGS for critically ill patients with lower respiratory tract infections and special infections such as subacute or chronic meningitis, which require special samples like bronchoalveolar lavage fluid and cerebrospinal fluid. However, the guidelines also mention that mNGS is suitable for opportunistic infections and mixed infections in immunocompromised patients, and infections with a wide variety of pathogens. 42 Therefore, mNGS is particularly valuable in dealing with peritonitis, especially when patients experience recurrent or refractory peritonitis. The decision to use mNGS can be based on the following situations: (1) For patients with complex clinical histories: Older patients, those with a history of lupus, taking anti-rejection drugs (indicating a high risk of low immunity), or with previous episodes of peritonitis, may benefit from mNGS due to the complexity of their condition and the potential for atypical or multiple pathogens. (2) When conventional cultures are negative or inconclusive: In cases where culture results are negative or white blood cell counts in PDE do not decrease despite treatment, mNGS can provide a more comprehensive analysis to identify the causative pathogens. (3) In the presence of mixed infections or unidentified pathogens: When culture results are positive but the patient's condition does not improve, suggesting possible mixed infections or atypical pathogens, mNGS can help detect a broader range of pathogens and guide targeted treatment. (4) Post catheter removal: After the removal of the catheter, if there is encapsulation of peritoneal fluid, mNGS can play a significant role in identifying any remaining or emerging pathogens that may contribute to persistent symptoms. (5) Prior to antibiotic use: In cases where antibiotics have been administered before a formal empirical treatment regimen is established, mNGS can still detect the presence of pathogens that may have been masked by prior antibiotic exposure. In summary, mNGS should be used in clinical practice when traditional diagnostic methods fall short, especially in complex cases of PDAP, to ensure timely and accurate identification of pathogens and to inform effective treatment strategies. We have summarized the relevant timing for prioritizing the clinical application of mNGS based on the characteristics of peritonitis in Figure 2.
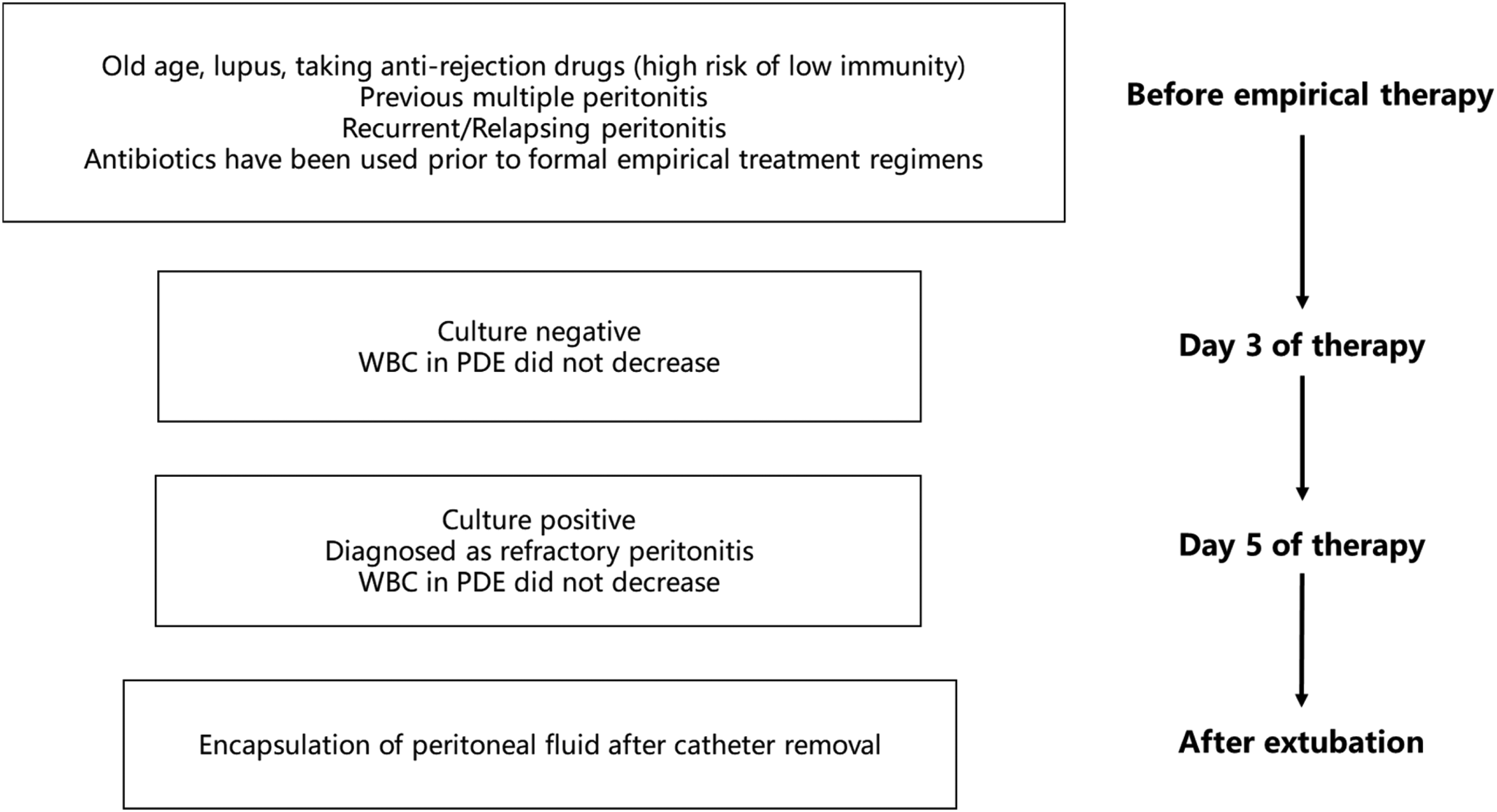
Timing for prioritizing the clinical application of mNGS based on the characteristics of peritonitis.
Peritonitis with atypical and rare pathogens: a challenge for early diagnosis
Tuberculosis and non-tuberculosis mycobacteria
Early diagnosis of peritonitis due to tuberculosis is difficult, and although acid-fast bacilli smears are currently positive in 73% of cases, PD catheter removal is due to delayed diagnosis in approximately 53% of cases. 43 Although PD catheter removal does not appear to improve survival. 44 Because guidelines call for early conversion to hemodialysis and PD catheter removal of patients whose ascites leukocytes fail to fall to 100*106/L by day 5 of treatment to avoid severe peritonitis complications. 45 As the gold standard for diagnosis, acid-fast bacilli take a long time to culture (often more than 6.7 weeks). 46 In addition, a meta-analysis showed that although adenosine deaminase alone often has a high specificity (0.96 (95% CI: 0.94–0.97)), the results are easily affected by non-tuberculosis factors such as liver disease. 47 Both BCG vaccination and natural infection with tuberculosis can cause a positive PPD test reaction. 48 Peritoneal biopsy is also considered one of the gold standards for the diagnosis of tuberculous peritonitis, but its use is often limited due to its traumatic nature. 49 Enzyme-Linked Immunospot assay for Interferon-gamma (IFN-γELISPOT) test is currently a useful adjunct to the diagnosis of active tuberculosis, and PD fluid test may be a more effective and accurate vehicle for the diagnosis of CAPD complicated with tuberculous peritonitis than peripheral blood. 50 The detection of M tuberculosis DNA using real-time PCR analysis including Xpert MTB/RIF technology (Molecular assays based on semi-nested real-time quantitative PCR techniques), although rapid, highly sensitive, highly specific, and simple to perform, is typically used in patients with highly suspected tuberculous peritonitis based on reported cases. And the technology usually relies on the specific nucleic acid sequence of the pathogen, these techniques require validation in the context of a high suspicion of the pathogen for a definitive diagnosis (It would be impractical and wasteful to perform this type of test on every patient in the early stages of peritonitis), thus having certain limitations in early diagnosis.51,52 Because it is difficult to extract the DNA of M tuberculosis, the specific sequences of M tuberculosis complex including Mycobacterium bovis, Mycobacterium africanum and Mycobacterium minium are usually detected to improve the detection rate. 32 In studies using mNGS for peritonitis diagnosis, 5% of peritonitis pathogens were M tuberculosis, and dialysis culture was negative, which may remind us that peritonitis caused by M tuberculosis is underestimated. Since M tuberculosis is not a common bacterium in the abdominal cavity, it is considered positive when the number of detected mycobacterial sequences is ≥1. 31 The diagnosis of not-tuberculosis mycobacteria(NTM) peritonitis is challenging, similar to that of M tuberculosis, with symptoms and signs difficult to distinguish from conventional PD peritonitis or tuberculous peritonitis. Acid-fast stains are difficult to distinguish between M tuberculosis and NTM, and the positive rate of acid-fast staining in a study of Mycobacterium abscessus peritonitis was only 40%. 53 A systematic review of 57 cases of NTM peritonitis found that treatment was delayed for up to 4 weeks, and acid-fast staining was often not routinely performed at PD centers. 54 Moreover, because M abscessus tends to form biofilms, colonize and infect catheters, it is easy to be considered a culture-negative exit infection or tunnel infection, increasing the chance of misdiagnosis. 55 Studies utilizing mNGS to detect pathogens in peritonitis have identified M tuberculosis in approximately 5% of cases. Notably, NTM were not detected in these mNGS studies, which correlates with the lower incidence of NTM in peritonitis.29,31 Although culture is still considered the gold standard for diagnosis, a recent report of metagenomic sequencing detected three species in dialysate, including Mycobacterium smegmatis, M abscessus, and Mycobacterium goodii was then identified as a pathogenic agent by final clinical presentation rather than M smegmatis isolated by conventional culture methods. 27 Diagnostic challenges for tuberculosis and NTM include slow growth in culture, resulting in prolonged diagnostic time, susceptibility to environmental contamination, and lack of specificity in clinical presentation, which is easily confused with peritonitis associated with conventional PD.
Fungus
Candida is the most common pathogen, accounting for 74.5% of all fungal peritonitis cases, with Candida albicans accounting for 55.7% and Candida species other than C albicans accounting for 44.3%. 56 In cohorts in southern China and North America, Candida accounts for 80%–90%.57,58 It usually grows rapidly in culture, but other fungi may take several weeks. Especially for non-Candida species such as Aspergillus, Cryptococcus, since these species are difficult to detect by gram staining of PD permeate smears. 59 Fungal peritonitis should also be considered for culture-negative peritonitis, long-term antibiotic use, and patients with diabetes mellitus or immunocompromised individuals. Although false positives have been reported, β(1→3)-d-glucan or galactomannan may be important early diagnostic markers for such highly suspicious patients.60,61 Early diagnosis of fungal peritonitis is important. 0% mortality has been reported if catheter removal is performed within 24 h and 31% mortality if catheter removal is delayed 24 h. Delayed catheter removal more than 24 h after diagnosis of fungal peritonitis is an independent risk factor for predicting mortality in patients with fungal peritonitis. 56 Molecular biological techniques such as PCR and RNA gene sequencing can be used to identify fungal peritonitis at an early stage. When mNGS is used to diagnose fungi, the diagnostic threshold is that the number of sequences is greater than 50, which can be considered as a positive result. Both C albicans and C albicans have reported mNGS detection.28,29
Anaerobic bacteria
According data from Australia and New Zealand Dialysis and Transplant Registry (ANZDATA), anaerobic PD peritonitis accounts for only 0.1% of single-pathogen peritonitis, rising to 1.1% if only polymicrobial episodes are considered. 62 In the report of Chao et al., ten cases of anaerobic PD peritonitis were reported, of which Bacteroides fragilis was the most common anaerobe species, accounting for 4 isolates, is a gram-negative anaerobe, usually associated with intestinal microbiota, but rare in peritonitis. Early diagnosis and treatment are essential to improve the prognosis of patients with anaerobic peritonitis, which has a conflicting overall prognosis with an 80% antibiotic cure rate and a relatively high mortality rate (10%), this suggests that timely diagnosis and treatment can significantly improve cure rates and reduce mortality. 63 Domingues et al. 64 mentioned that because anaerobic bacteria need special conditions to grow, traditional culture sometimes leads to false negative results due to insufficient conditions, while molecular diagnostic techniques such as PCR technology are not limited by these conditions.So they can reduce the occurrence of false negative results for anaerobic peritonitis. In Guangzhou, China, it was reported that mNGS technology was used to successfully diagnose and treat refractory peritonitis cases with Bacillus thetaiotaomicron and Ureaplasma parvum,this two cases dialysate cultures were negative. 65
Ureaplasma
Microorganisms of the genus Ureaplasma are a class of prokaryotes without cell walls, they can be cultured using mycoplasma culture media, they are increasingly being discovered using molecular techniques. 66 In recent years, a number of peritonitis cases have been reported in which Ureaplasma-induced peritonitis was diagnosed using 16SrRNA gene PCR or NGS technology. Among them, Ureaplasma parvum and Ureaplasma urealyticum are two common ureaplasmas that cause human genital tract infections. Infections are more common in infected women after urogenital tract operations or surgeries and have been reported to cause peritonitis many times.33,67–69 Ureaplasma urealyticum was also found in a study (included 18 cases) on the application of mNGS diagnosis of peritonitis, indicates that the potential incidence of this pathogen is not low. 30 It is believed that with the promotion of technologies such as PCR, 16S sequencing and mNGS, more types of atypical pathogens can be discovered.
Viruses
Due to the particular conditions required for virus cultivation, there is currently little attention and few reports on peritonitis caused by such pathogens. In studies using mNGS in southern China, herpes simplex virus type 5 (HHV-5) and herpes simplex virus type 6B (HHV-6B) were found. In another study detecting peritonitis pathogens with mNGS, herpes simplex virus type 5 (HHV-5) and herpes simplex virus type 6A (HHV-6A) were also identified.28,31 Given the widespread presence of herpes viruses in the population, many people carry these viruses without exhibiting symptoms. These viruses may remain dormant in the body's nerve cells and reactivate under certain conditions, such as stress, illness, or immune suppression. The detection of herpes viral DNA in samples through mNGS does not necessarily correlate with active disease. It may simply reflect a latent infection.
Conclusions
mNGS technology has significantly improved the pathogen detection rate in the diagnosis of peritonitis with atypical and rare pathogens, reducing patients' hospitalization time and medical expenses. By improving the detection rate of pathogens, reducing misdiagnosis and unnecessary use of antibiotics, and reducing the development of drug resistance, medical resources can be saved and the diagnosis of mixed infections can be made possible. Despite the current limitations such as high cost, inability to determine pathogen bioactivity, and inability to perform drug sensitivity tests, the price of mNGS testing is expected to gradually decrease with increasing market competition and further technological development, and the government reimbursement mechanism of medical insurance institutions will also be strengthened. Future research needs to focus on reducing costs, improving accessibility of testing, and developing new bioinformatics tools. Enhance clinicians' understanding and application of mNGS technology so that they can better integrate mNGS results into clinical practice.
Disclaimer
Since some references may not be directly accessible, certain claims may require further verification against primary sources. We have made every effort to ensure the accuracy of all information, but we recommend that readers consult the original sources when necessary to validate the relevant data.
Footnotes
Author contributions
DX, CX, ZZ are contributed equally to this work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.