
Abstract
Background
Peritoneal dialysis (PD)-related pleuroperitoneal communication is strongly associated with PD discontinuation. Video-assisted thoracoscopic surgery (VATS) has emerged as a promising therapeutic approach. However, there are still challenges in detecting diaphragmatic defects under conventional thoracoscopy, and the repair methods vary significantly.
Methods
We have developed an intervention protocol for pleuroperitoneal communication that includes single-port VATS utilizing near-infrared fluorescence with indocyanine green, as well as the management of perioperative kidney care and PD reinitiation. Patients who underwent VATS for pleuroperitoneal communication repair from September 2022 to March 2024 were identified at a single center. The procedures and outcomes were evaluated, and the success rate of PD resumption was compared with that of a historical cohort treated with non-surgical therapies.
Results
A total of 6 patients underwent VATS. The age was 48.7 ± 11.8 years, 2 were female, and the PD vintage was 8.7 (2.0–28.4) months. Non-dialysis therapy (n = 4) or temporary hemodialysis (n = 2) was prescribed during PD suspension. Fluorescence thoracoscopy identified diaphragmatic defects in all patients, including lesions that were unrecognizable under white light. Mechanical pleurodesis by direct suture of the defects with local mechanical reinforcement was performed. All patients reinitiated PD 15–30 days postoperatively, with no recurrence during a follow-up of 17.0 ± 6.4 months. The success rate significantly exceeded that in the patients who underwent PD suspension or chemical pleurodesis (100% vs. 29%, p = 0.005).
Conclusions
The minimally invasive VATS integrating fluorescence with indocyanine green and pleurodesis with multiple mechanical reinforcements, along with appropriate perioperative care and an incremental approach to resume PD, was a reliable treatment for PD-related pleuroperitoneal communication.
Keywords
Introduction
Pleuroperitoneal communication is a rare mechanical complication of peritoneal dialysis (PD). The prevalence ranges from 0.7% to 2.5% in adult patients.1–4 It predominantly occurs on the right side, 5 infrequently on the left or bilaterally, and very occasionally, an isolated pericardial effusion can be the only manifestation. 6 Possible mechanisms include congenital and acquired diaphragmatic defects, pleuroperitoneal pressure gradient, and lymph drainage disorders. When there is a defect in the diaphragm, the gradient between the increased intra-abdominal pressure (IAP) and the physiological negative pressure in the pleural space moves dialysate into the thoracic cavity.
Despite its rarity, pleuroperitoneal communication often leads to PD discontinuation and transfer to hemodialysis.1–4 The effect of non-surgical therapy is unsatisfactory.3,7 Conservative treatment, defined as temporary interruption of PD for 2–6 weeks, is reported to lead to spontaneous healing of the diaphragm in 53% cases, and chemical pleurodesis by intrathoracic administration of sclerosing agents via a chest tube is associated with a suboptimal success rate as low as 48%. 1
Video-assisted thoracoscopic surgery (VATS) has emerged as a therapy for this complication, and various surgical repair techniques have been reported. However, the recurrence rate still can be high unless the defects on the diaphragm are precisely ascertained and securely repaired during the surgery.
Indocyanine green is a fluorochrome with absorption and emission peaks in the near-infrared spectrum (750–1400 nm). The favorable optical properties and extremely low toxicity enable real-time, enhanced visualization of anatomical structures under fluorescence. 8 Over the last decade, indocyanine green fluorescence imaging has become a rapidly developing technical innovation for intraoperative navigation, gaining traction in general, visceral and transplant surgery. 9 A few case reports illustrate the use of indocyanine green to identify diaphragmatic defects during VATS in the setting of pleuroperitoneal communication.10–13
Under the close collaboration between thoracic surgeons and PD staff, we have established an approach that successfully identifies and corrects pleuroperitoneal communication, by minimally invasive single-port VATS integrating indocyanine green fluorescence imaging. The present work provides a comprehensive introduction of the technique, outlines the protocols for perioperative management and PD reinitiation, and evaluates the effectiveness and safety.
Methods
Study design
The study included PD patients diagnosed with pleuroperitoneal communication and treated with VATS at Renji Hospital, School of Medicine, Shanghai Jiao Tong University, from September 2022 to March 2024. All participants were followed up until January 31, 2025. The characteristics, treatments, and outcomes of the patients were reviewed. Data on patients receiving non-surgical treatments were obtained from a historical cohort at our center between January 1998 and August 2022. The success rate of PD resumption without recurrence was compared between the VATS group and the historical cohort. This study adhered to the principles of the Declaration of Helsinki. It was approved by the Ethics Committee of Renji Hospital, School of Medicine, Shanghai Jiao Tong University (LY2024–268-B).
Diagnosis and preoperative management
Thoracentesis and concomitant pleural drain were performed when there was significant hydrothorax and suspected pleuroperitoneal communication. It was diagnosed either by an elevated glucose concentration gradient between thoracic drainage and a simultaneous blood sample, or by a positive contrast computed tomography (CT) peritoneography. PD was suspended once the diagnosis was confirmed, and the PD catheter was flushed and then blocked with 20 mL saline containing 2000 U heparin once a week to maintain patency. Hydrothorax was drained as completely as possible. During PD suspension, non-dialysis therapy including restrictions on sodium, fluid, and protein intake, diuretics, correction of acid-base and electrolyte disturbance, etc. was applied to patients with sufficient residual kidney function, while hemodialysis using a central venous catheter was prescribed if the patient was dialysis-dependent.
Surgery procedure
A bag of 2 L glucose-based PD fluid (PDF) containing 25 mg indocyanine green was intraperitoneally infused 20 to 30 min before the procedure. Under general anesthesia, the patient was placed in a hemilateral decubitus position and intubated with a double-lumen endotracheal tube, deflating the lung on the affected side. Manual compression was used to increase IAP. A 4-cm incision was made at the sixth or seventh intercostal space on the anterior axillary line of the affected side, serving as the sole entry for the near-infrared fluorescence thoracoscope and operative instruments. The diaphragm was completely and carefully inspected via thoracoscope under white light first, and then rechecked using fluorescence. After identifying the culprit sites, the defects, along with the surrounding normal diaphragmatic tissue, were grasped using forceps and continuously closed with 3–0 unidirectional barbed sutures (V-LocTM 180; Covidien, Mansfield, MA, USA). Polyester (PE) cardiovascular patches (Shanghai Chest Medical Instruments Co., Ltd, Shanghai, China) were tailored into appropriate sizes and then sutured in an interrupted mattress manner with the ligation to create a sandwich-like structure, serving as a reinforcement. In the last 3 cases, we added an absorbable polyglycolic acid (PGA) felt (80 × 60 mm; Neoveil, GUNZE Ltd, Tokyo, Japan) to cover the repair. A chest tube was inserted for drainage following the procedure in all patients.
Postoperative care
After the surgery, complications were monitored, and non-dialysis therapy or hemodialysis continued. The timing for PD reinitiation was a joint decision by thoracic surgeons and nephrologists. Initially, daytime ambulatory PD was applied with a reduced volume, namely 1.0–1.2 L, and the patient was asked to keep the trunk upright when there was PDF dwelled and avoid movements associated with significantly increased IAP. The number of exchanges was tailored to confer a cumulative daily dose to keep the patient safe, usually 3 or 4 times per day. Volume status, symptoms of uremia and laboratory parameters were closely assessed. Ultrasonography for pleural effusion was repeated before and after PD reinitiation and increase of dwell volume, until patient's original PD prescription was resumed for at least 1 month without evidence of recurrence.
Statistical analysis
Data are presented as absolute number (percentage) for categorical variables, mean ± SD for normally distributed continuous variables, and median (interquartile range) for nonnormally distributed continuous variables. Comparison between the VATS group and the historical cohort on patient characteristics and outcomes used t-test, Mann–Whitney U test, Fisher's exact test, and Likelihood ratio test where appropriate. Statistical analyses were performed using SPSS, version 25 (IBM Corp., Armonk, New York, USA). A two-tailed p value <0.05 was considered statistically significant.
Results
From January 1998 to March 2024, there were 2508 patients commencing PD at our center. A total of 32 (1.3%) individuals were diagnosed with pleuroperitoneal communication, among whom 6 patients underwent VATS, and the historical cohort consisted of 26 patients treated with non-surgical interventions.
Characteristics of the patients undergoing VATS are shown in Table 1. For this group, the age was 48.7 ± 11.8 years, 2 were female, glomerulonephritis was the underlying kidney disease for all, none comorbid with diabetes, 5 were on continuous ambulatory PD and 1 was on automated PD, and RKF was 4.3 ± 4.4 ml/min. The PD duration was 8.7 (2.0–28.4) months at diagnosis. The historical cohort shared similar characteristics (Table 2). Massive right-sided hydrothorax was found in all 6 patients, and the diagnosis was confirmed by thoracocentesis (n = 4) or CT peritoneography (n = 2). The median duration of preoperative PD suspension was 9 (6, 16) days. During this period, 2 patients underwent temporary hemodialysis and 4 received non-dialysis therapy.
Characteristics of the pleuroperitoneal communication patients treated with minimally invasive VATS.
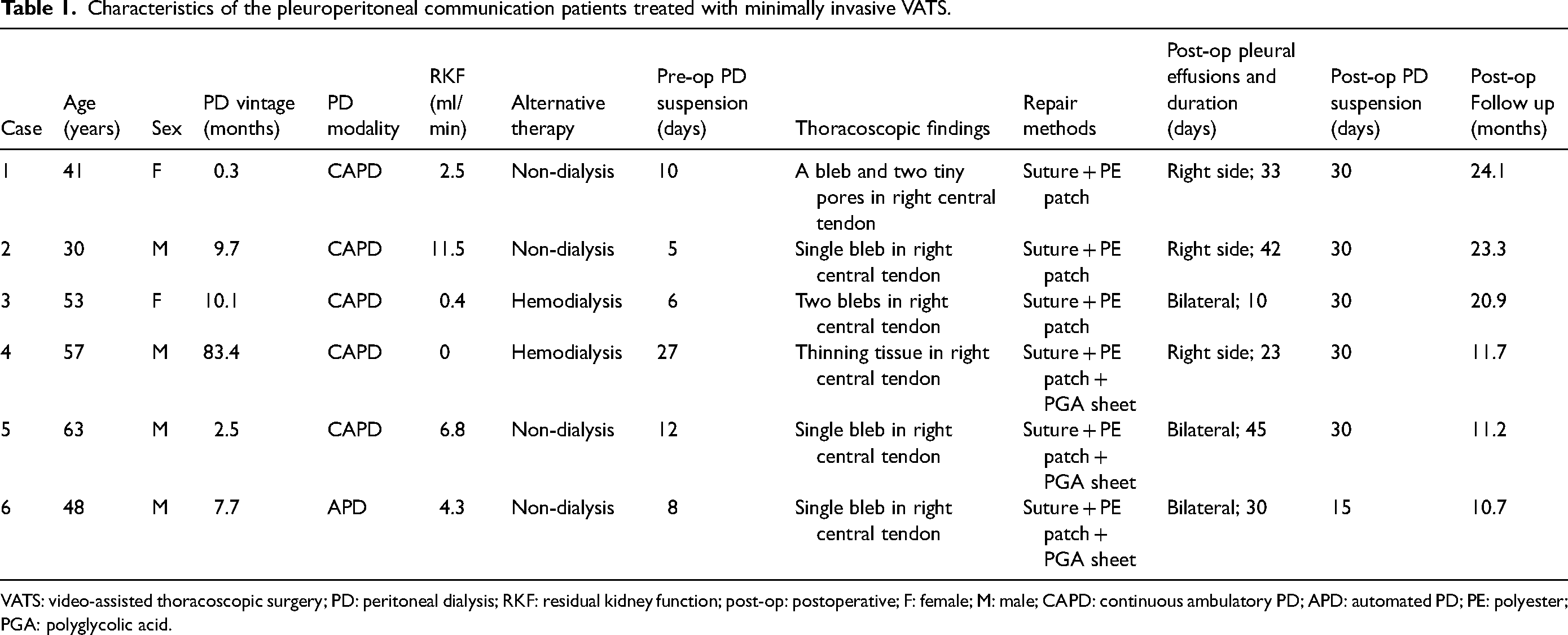
VATS: video-assisted thoracoscopic surgery; PD: peritoneal dialysis; RKF: residual kidney function; post-op: postoperative; F: female; M: male; CAPD: continuous ambulatory PD; APD: automated PD; PE: polyester; PGA: polyglycolic acid.
Characteristics of patients undergoing VATS or non-surgical therapy
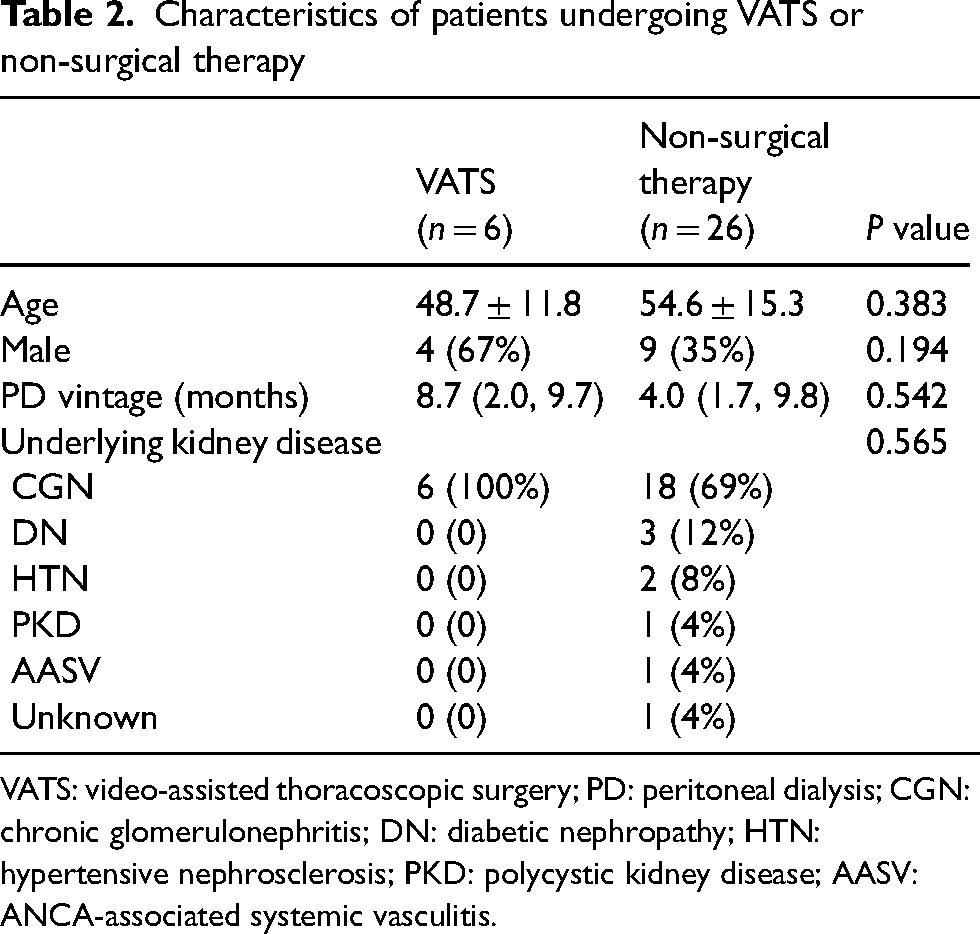
VATS: video-assisted thoracoscopic surgery; PD: peritoneal dialysis; CGN: chronic glomerulonephritis; DN: diabetic nephropathy; HTN: hypertensive nephrosclerosis; PKD: polycystic kidney disease; AASV: ANCA-associated systemic vasculitis.
During the operation, a thoracoscope using white light showed a single inflated bleb in central tendon in 5 patients, while in Case 4 no obvious breakage was observed. When switching to fluorescence, the lesions appeared bright green, and the near-infrared camera provided high-contrast images that more clearly revealed the defects. Of particular note were the findings by fluorescence in Cases 1, 3, and 4. In Case 4, a thinning in the middle of the central tendon, estimated to be 35 × 20 mm in area, was found (Figure 1(a)). In Case 1, two subtle tiny pores, located 5 to 10 mm away from the major bleb already identified under white light, were revealed under fluorescence; in Case 3, a negligible bleb was identified 20 mm distant from the major bleb (Figure 1(b)). The distribution of the defects is summarized in Figure 2. The lesions were sutured and reinforced by PE patches for Cases 1–3 (Figure 3), and a PGA felt was additionally applied for Cases 4–6.
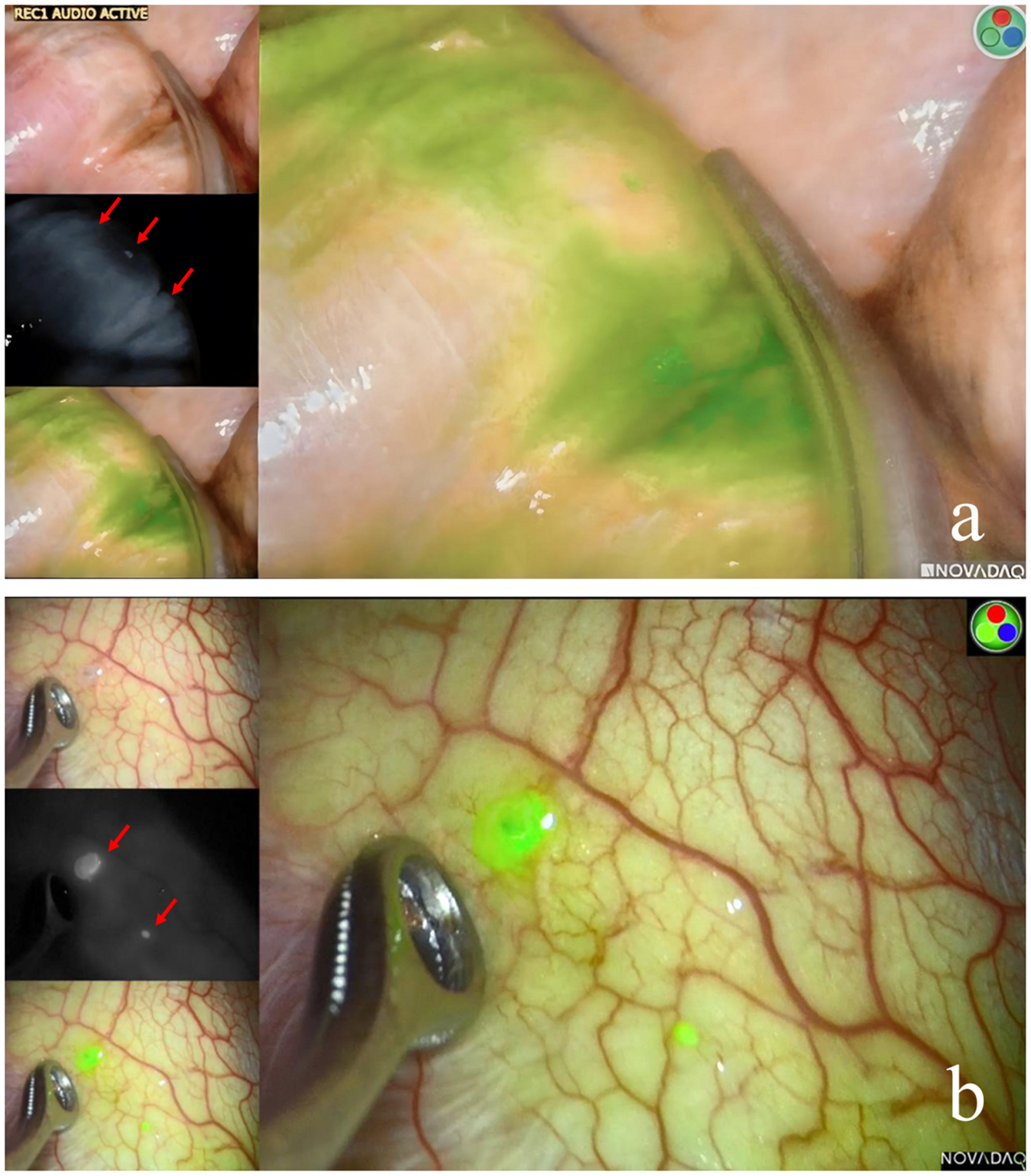
Thoracoscopic findings under white light and by near-infrared fluorescence with indocyanine green. In Case 4 (a), no obvious breakage was observed under white light (left upper panel). Upon switching to fluorescence, a green-stained thinning in the center of central tendon was confirmed, with an estimated area of 35 × 20 mm (left lower panel and right panel), and the near-infrared camera provided high-contrast images that confirmed the presence of lesions (left middle panel, arrows). In Case 3 (b), a major bleb was found in central tendon under white light (left upper panel), while fluorescence identified an additional negligible bleb 20 mm distant from the major one (left middle, left lower, and right panels)
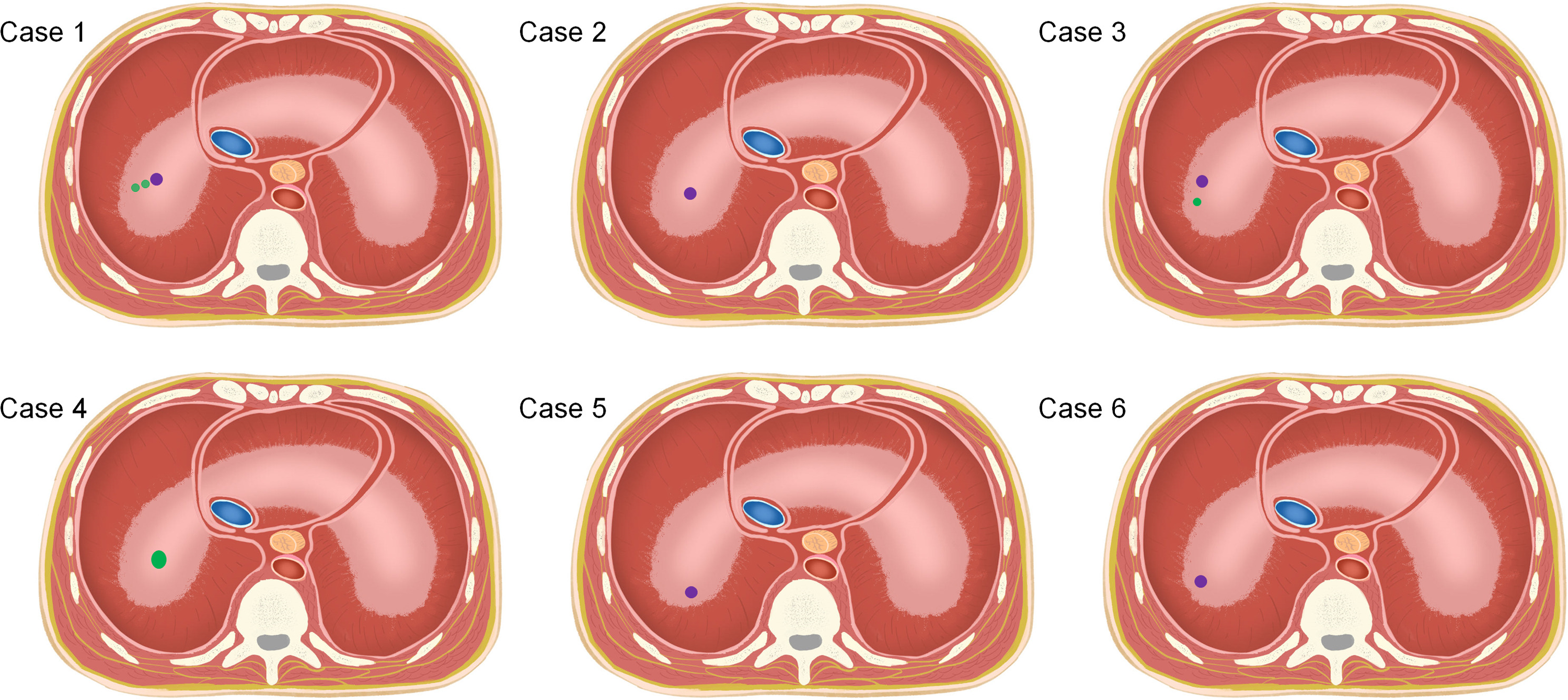
Distribution of diaphragmatic defects of pleuroperitoneal communication. Purple dots represent major blebs discovered under white light, and green dots represent tiny blebs, pores, or thinning of central tendon identified by near-infrared fluorescence with indocyanine green
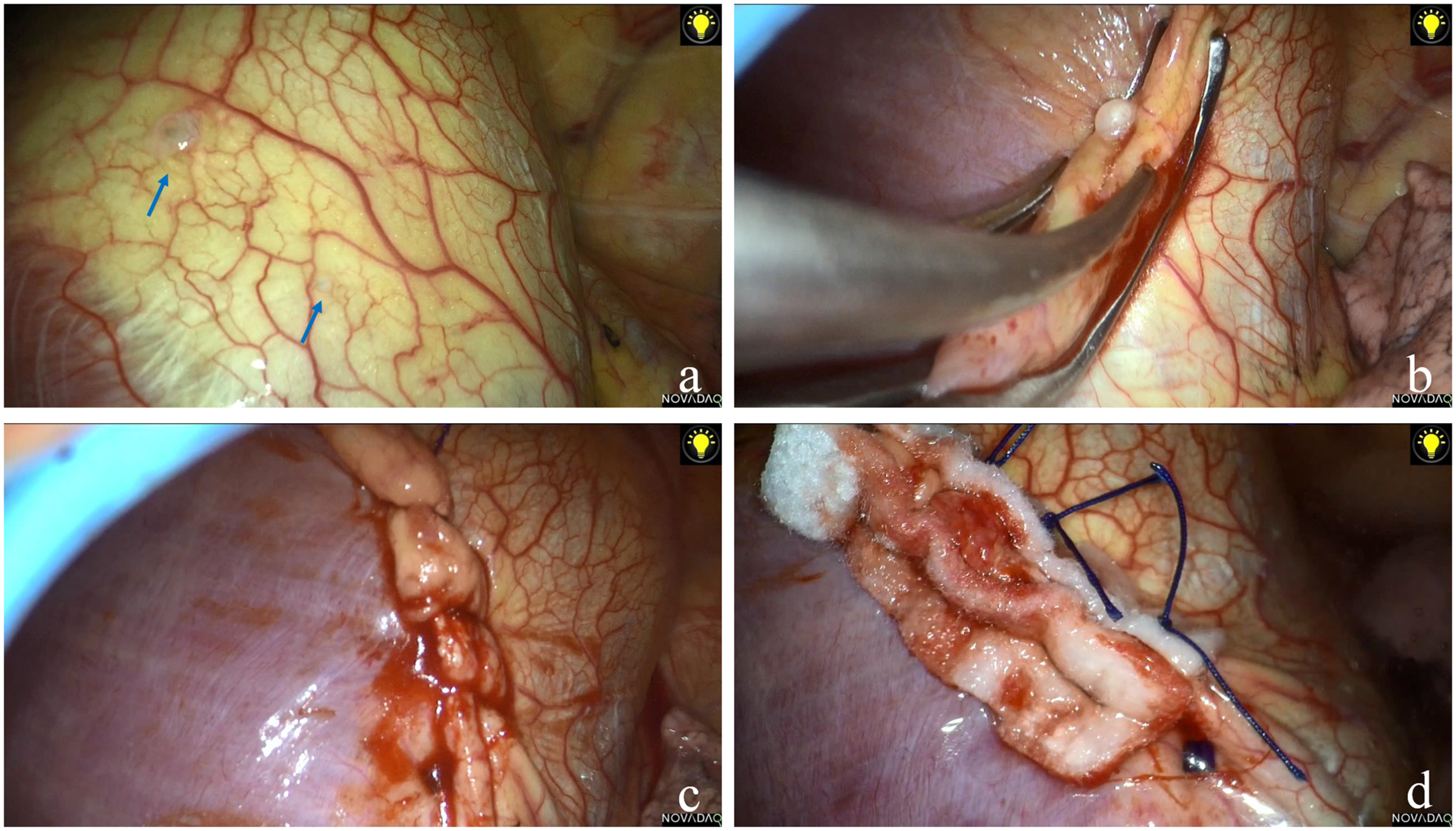
The procedure of defect ligation during video-assisted thoracoscopic surgery. Case 3 was selected for illustration. Two blebs, one major and one minor, were identified (3a, arrows). The defects together with the surrounding normal diaphragmatic tissue were grasped using forceps (3b) and continuously sutured (3c). Polyester cardiovascular patches were tailored into appropriate sizes and were sutured with the ligation to create a sandwich-like structure as a reinforcement (3d).
The drain tube was removed when drainage was less than 200 mL/day, typically 2–3 days postoperatively. All patients showed a small amount of unilateral or bilateral pleural effusions on ultrasonography, which usually persisted for over a month and were then completely absorbed. Case 5 developed transient postoperative urinary retention, which was considered to be anesthesia-related. There was no surgical complication.
PD suspension lasted for 30 days after operation in 5 patients, except for Case 6. This patient developed uremic symptoms while on non-dialysis therapy. PD was reinitiated 15 days postoperatively after careful evaluation. No evidence of recurrence was observed in any of the patients during a period of 17.0 ± 6.4 months, and the original prescriptions were resumed in all patients 1–2 months after PD reinitiation. By the end of the follow-up, the patient in Case 1 had received kidney transplantation, while the others remained on PD.
In the historical cohort, PD suspension for at least 1 month before rechallenge was applied in 12 patients; chemical pleurodesis through a chest tube was performed in 5 others, including 3 using lentinan and 2 using elemene; no PD salvage was attempted in the remaining 9. Only 5 patients resumed PD successfully, including 2 treated with PD interruption and 3 with chemical pleurodesis. The success rate in 17 patients who underwent PD suspension or chemical pleurodesis was significantly lower than that in the VATS group (29% vs. 100%, p = 0.005). In addition, 4 patients reported moderate to severe pain after chemical pleurodesis, with 2 of them experiencing mild fever.
Discussion
The present report introduces an effective and safe method of minimally invasive VATS guided by indocyanine green for PD-related pleuroperitoneal communication repair. Our practice is characterized by single-port thoracoscope technique, precise lesion identification by indocyanine green fluorescence imaging, direct closure of the diaphragmatic defects combined with local reinforcement, and cautious approaches to restart PD.
Similar with previous reports,2,4 pleuroperitoneal communication occurred in 1.3% of the PD patients at our center during the past 26 years. In recent years, innovations in VATS have optimized the management and have provided better outcomes compared to non-surgical treatments. The VATS techniques are heterogeneous, as biportal and triportal approaches are the most common, sometimes combined with laparoscope.4,14–19 In contrast, the single-port method we have adopted minimizes surgical trauma.
VATS enables direct visualization of diaphragmatic defects and targeted pleurodesis. According to our observation, the defects can be bleb-like, pore, and thinning of the diaphragm, predominantly in the central tendon, and multiple lesions are not uncommon. It is noteworthy that the detectability of the defects largely depends on their size and permeability, and occult ones can be missed when observed under white light.
It is crucial to precisely locate the lesion in the diaphragm for pleuroperitoneal communication repair during VATS. However, Chen et al. 20 reported that 77% of the cases showed no visible diaphragmatic pathology under thoracoscope in the absence of dye and increased IAP, and the recurrence rate was 26% in this context. Increased IAP can be achieved by pneumoperitoneum via PD catheter or an extra laparoscopic port, which provides a pressure of 8–20 cmH2O, and it makes the defects more distinguishable.4,18 We apply manual compression to increase IAP, and it is evenly effective but more simple and less invasive. Dyes in PDF further facilitate identification of the culprit sites. Methylene blue is traditionally used,4,16 but sometimes it may be too faint to be recognized by naked eyes, and chemical peritonitis is a concern.
Fluorescence imaging with indocyanine green or indigo carmine can be more sensitive in defining diaphragmatic lesions.10,15,17 Near-infrared fluorescence light penetrates several millimeters below the tissue surface, providing a satisfactory optical window for visualizing subsurface structure. 21 There have been a few cases illustrating the application of indocyanine green for intraoperative identification of diaphragmatic defects in adult and pediatric PD patients.10–13 Interestingly, Inanaga et al. presented a case in which positioning of the communication site failed by indigo carmine but succeeded by indocyanine green. 10 As we have observed, it can disclose various types of defects, even those that are tiny or merely weakened tissue insignificant under white light. Our findings suggest that near-infrared indocyanine green fluorescence imaging could add significant value to identification of defects during VATS. However, the appropriate timing for infusing indocyanine green-containing PDF remains to be addressed. Insufficient dwell time may lead to false negatives, especially when the defect is tiny or when the preoperative PD suspension lasts long enough to allow spontaneous healing to some extent. On the other hand, a prolonged dwell period, along with rapid migration of PDF, may result in dissemination and accumulation of the dye in the thoracic cavity, causing visual contamination under fluorescence. This could potentially interfere with discrimination of the defect. Despite this paradox, our protocol successfully revealed diaphragmatic defects in all cases of the present series.
Repair techniques include mechanical and chemical pleurodesis, or a combination of both. Mechanical pleurodesis refers to direct suture, either manually or using a surgical stapler, with or without mesh or PGA sheet completely or partially covering the diaphragm.3,17,19,22 Nemeth et al. and Tsubouchi et al. reported recurrence after mesh repair without suture.19,22 Therefore, direct suture of the defects and diaphragm fold for thinning of the tissue is essential. Successful chemical pleurodesis alone during VATS has been reported,7,10,16 and various sclerosing agents that can promote inflammatory reaction and adhesion are employed4,10,15,16,20; however, conjunction with mechanical repair appears to be more effective. 20 In the present series, mechanical pleurodesis was exclusively applied to all patients by ligaturing a single lesion or adjacent multiple ones together with surrounding tissue in a continuous suture, and then the ligation was strengthened by adding non-absorbable materials tightly on both sides to form a sandwich-like structure, intending to trigger tissue proliferation and to further reinforce the repair; for the last 3 cases, an additional PGA sheet as another layer of the mechanical barrier was added. The method provides multiple reinforcement measures with enough redundancy, and the effectiveness is supported by our preliminary results. In addition, although we have not encountered such a case yet, we plan to suture a PE patch along the edge of the central tendon and then completely cover the diaphragm with a PGA felt if no definite defect can be identified.
Postoperative care includes monitoring of surgical complications, decision of timing to resume PD, adjustment of PD prescription, and evaluation of recurrence. There is no consensus on postoperative duration before PD can be reinitiated, and it varies from 1 day to months according to previous reports.3,4,10,15–20,22 When PD is restarted, an incremental strategy is recommended, and initially a dwell volume of 1.0–1.5 L may be suitable.10,17 We adopted relatively longer PD suspension to ensure complete healing. Previous studies indicate that vertical positions generate greater IAP compared to supine position. 23 The measurements reflect the pressure in the pelvis, where the catheter tip is located. However, it is unclear how body positions affect the pressure conducted towards the diaphragm. We speculate that keeping the trunk upright when there is minimal dwell volume may be helpful to minimize the stress on the diaphragm.
As we observed, mild spontaneous pleural effusions could persist for a period, possibly due to operation-related intrathoracic inflammation. It is important to repeat imaging examinations and, if there is any, to discriminate pleural effusion from pleuroperitoneal communication recurrence after PD resumption, especially in the early phase and at the time of dwell volume increment. Our results demonstrated the efficacy of the cautious approaches to resume PD, and whether the time of PD suspension can be shortened needs further evaluation.
There are limitations in this study. We acknowledge that the retrospective design and small sample size preclude definitive validation of our methods. Although our approach resulted in appreciably better detection of the defects, this study did not directly compare VATS techniques with and without fluorescence imaging. As such, the significance of identifying the defects during surgery remains unconfirmed. Moreover, the success rate of non-surgical treatments in our historical cohort was notably lower than that reported in prior studies.1,3 This control group comprised cases spanning over two decades. In the early years, we were less experienced in managing this complication, and a considerable number of patients opted to switch to hemodialysis directly. In vivo administration of talc is unapproved in our country, and chemical pleurodesis using other sclerosing agents was infrequently used due to concerns about excessive inflammation. In addition, it is possible that the patients had compromised healing capacities.
In summary, we report an approach that successfully identifies and repairs PD-related pleuroperitoneal communication, by minimally invasive single-port VATS using near-infrared fluorescence with indocyanine green and the protocol of appropriate perioperative care. Further modification of the techniques and validation in larger sample study are warranted.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author contributions
YH, FW and YQ conceived the study. QY, YH and LH participated in gaining ethical approval, data collection and analysis. QL performed peritoneography analysis. YQ and LH performed the surgery. QY and LH wrote the first draft of the manuscript. YH, FW, YQ, YZ, QL, NZ, and GL revised the manuscript. All authors approved the final version.
Ethical approval
This study was approved by the Ethics Committee of Renji Hospital, School of Medicine, Shanghai Jiao Tong University (LY2024-268-B).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent to participate
Written informed consent was obtained from patients who are still available. For patients who have deceased or been lost to follow-up, informed consent was waived given the retrospective nature of this study.
Informed consent to publish
Written informed consent for individual patient information and images to be published was provided by the patients
Acknowledgements
The authors would like to thank our PD nursing staff, particularly Ms. Jiaying Huang, Ms. Yanna He, and Ms. Xinhui Ma, for their work.