
Abstract
Background
There are inequalities in resource allocation and services across peritoneal dialysis (PD) centers in China. This study aimed to explore the association between hospital type (university-affiliated vs. non-university-affiliated hospitals) and clinical outcomes in PD patients.
Methods
Data from the Peritoneal Dialysis Telemedicine-assisted Platform cohort was analyzed. The primary outcome was all-cause mortality, while secondary outcomes included hemodialysis transfer and first-episode PD-related peritonitis. Univariable and multivariable Fine–Gray models were used to calculate subdistribution hazard ratios (SHRs). Propensity-score matched analyses and sensitivity analyses restricted to incident patients were also performed.
Results
A total of 7416 PD patients were enrolled (June 2016 to April 2019), with a median follow-up of 29.0 months. University-affiliated hospitals’ patients (n = 4806) were younger, had better nutritional status, and higher socio-economic status than those in non-university-affiliated hospitals (n = 2610). University-affiliated hospitals exhibited a lower risk for all-cause mortality (SHR: 0.72, 95% confidence interval (CI): 0.61–0.85, p < 0.001), higher hemodialysis transfer (SHR: 1.31, 95% CI: 1.08–1.60, p < 0.01), but no association with first-episode peritonitis in multivariable analyses. After propensity-score matching, university-affiliated hospitals were still associated with lower all-cause mortality (SHR: 0.74, 95% CI: 0.61–0.91, p < 0.01) and a higher risk of hemodialysis transfer (SHR: 1.52, 95% CI: 1.19–1.94, p < 0.01). Comparable results for all-cause mortality and first-episode peritonitis also found in incident patients.
Conclusion
In China, PD patients in university-affiliated hospitals had lower mortality but a higher risk of hemodialysis transfer. Further studies are needed to understand these findings and inform future practices and resource allocations.
Keywords
Introduction
Dialysis population continue to grow rapidly worldwide, 1 and also in China, 2 resulting in a shortage of resources for dialysis.3,4 Peritoneal dialysis (PD) is more cost-efficient than hemodialysis, and could be applied for patients with end-stage kidney disease in various circumstances, especially in developing countries.5,6 However, according to the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS) data, the clinical outcomes of PD patients vary significantly across different centers.7–10 This has given rise to the need to investigate the characteristics of centers and their association with outcomes.
Previous studies have indicated that PD center sizes are closely associated with clinical outcomes, such as mortality, hemodialysis transfer, and PD-related peritonitis.11–13 In China, there are inequalities in resource allocation and available services across centers, which is not matched to center sizes.14,15 Compared to the developed regions, PD centers in the undeveloped regions in the central and western provinces, despite their large sizes, are not necessarily equipped with healthcare resources. 16 It is noteworthy that university-affiliated hospitals in our country have generally carried out PD programs for a longer period of time, and they have well-established workflows and more experienced PD teams as compared with non-university-affiliated hospitals. We therefore hypothesized that PD patients in university-affiliated hospitals may have better prognosis.
Hence, we aimed to explore the association between hospital type, that is, university-affiliated and non-university-affiliated hospitals, and the clinical outcomes of PD patients through a national multicenter cohort study that accounts for potential confounders. Our findings will provide valuable evidence for physicians and health policymakers to develop strategies to improve health equity in China, as well as for other developing countries.
Materials and methods
Study design
This multicenter prospective cohort study was an affiliated study of the Peritoneal Dialysis Telemedicine-assisted Platform Cohort Study (PDTAP Study). Center enrollment, participants’ eligibility, and enrollment details have been listed in detail in a previous article. 17 All participants signed an informed consent form after the center received ethics board approval in accordance with the Declaration of Helsinki. As part of informed consent, all participants agreed to the use of their individual data in future studies.
Study setting and participants
A total of 27 hospitals from all seven geographical regions of China (northwest, northeast, north, central, southwest, southeast, and south) participated in the PDTAP study. During the enrollment phase, all incident and prevalent patients receiving PD were included. In addition to the inclusion and exclusion criteria published in a previous article, 17 patients with missing socio-economic data were also excluded.
Clinical variables and center characteristics
Data collection and elements of the database were published in a previous article. 17 Patients’ demographics, primary disease, comorbidity data, dialysis prescription, and clinical outcomes were recorded by the PD staff. Laboratory data were exported from the Laboratory Information Management System of hospitals directly or input by the PD staff in some units. Center characteristics for each PD center were collected including center volume, years since PD initiation, proportion of patients with cross-city PD treatment, patient-to-physician ratio, patient-to-nurse ratio, number of beds, hemodialysis machine in the nephrology department, and whether the center was a quality control center.
Socio-economic variables
Socio-economic data was collected within 1 week preceding PD catheter implantation, including hospital type, regional economic level, education level, residence, medical insurance type, income, travel distance, and travel time.
Hospital type was classified as either university-affiliated hospitals or non-university-affiliated hospitals (Supplementary Figure 1). The regional economic level, reflecting the difference in regional location, was classified as high or low based on whether it exceeded the median GDP per capita (¥59,410, or US$8371) in the province of residence as of 2021. 18 Educational level was categorized into two groups based on whether it was high school or above. Residence was classified as urban or rural. Medical insurance type was divided into insurance for urban residents or other types. Income, defined as yearly household income per person, was categorized into high and low groups based on whether it exceeded the disposable income per capita in the province of residence as of 2021. 18 Travel time and distance were reported by patients from their homes to the designated hospitals.
Outcome events
The primary outcome was defined as all-cause mortality while on PD. The secondary outcomes included hemodialysis transfer and first-episode PD-related peritonitis during the study follow-up period. Hemodialysis transfer was defined as patients on PD switched to hemodialysis for more than 3 months. 19 All patients were followed up until hemodialysis transfer, kidney transplantation, death, or the end of the study (31 December 2020).
Statistical analyses
Variables were presented based on the data distribution and differences were compared across hospital types. The median survival time was estimated using Kaplan–Meier survival analysis. A univariable Fine–Gray competing risk model was used to identify all significant clinical and socio-economic variables to be associated with outcomes. Hemodialysis transfer and transplant were considered a competing risk event for all-cause mortality. Deaths and transplant were considered competing risk events for hemodialysis transfer, while deaths, hemodialysis transfer, and transplant were considered competing risk events for first-episode PD-related peritonitis. Multivariable analysis was then applied to identify independent associations between hospital type and outcomes adjusted for significant variables with p < 0.2 in univariable analyses. Multicollinearity was assessed using the variance inflation factor (VIF), and variables with VIF > 5 were excluded. In the final multivariable model, to mitigate the risk of generating overly narrow confidence intervals (CIs) due to univariable filtering, the subdistribution hazard ratios (SHRs), along with 95% CIs and p-values, were reported after applying the selection procedures using the ‘selectiveInference’ package in R 4.3.1.
To reduce confounding and bias, propensity-score matching (1:1) within a caliper of 0.02 was used to balance significant risk factors between patients in different hospital types. All available variables were included, and logistic regression modeled the odds of being treated at university-affiliated versus non-university-affiliated hospitals. Propensity scores derived from this model were used for matched analysis. Propensity-score matching was repeated for all outcomes, followed by formal sensitivity analyses restricted to incident PD patients for all outcomes examined.
All probabilities were two-tailed and the level of significance was set at 0.05. All statistical analyses were performed using SPSS 27.0 (SPSS Inc., Chicago, Illinois, USA), STATA 17.0 (Stata Corp. LP, College Station, Texas, USA), and R 4.3.1 (R Project for Statistical Computing).
Results
Patient and center characteristics
A total of 7416 PD patients who met the eligibility criteria between 1 June 2016 and 30 April 2019 were included in the study, and followed up until 31 December 2020 (Figure 1). The median follow-up period was 29.0 (interquartile range: 14.3–45.0) months. The baseline characteristics of the whole cohort are presented in Table 1. There were 3576 incident patients and 3840 prevalent patients in the total cohort, and the follow-up time was 25.0 (interquartile range: 16.0–35.0) months and 34.0 (interquartile range: 14–50) months, respectively. The baseline characteristics between incident and prevalent patients are presented in Supplementary Table 1.
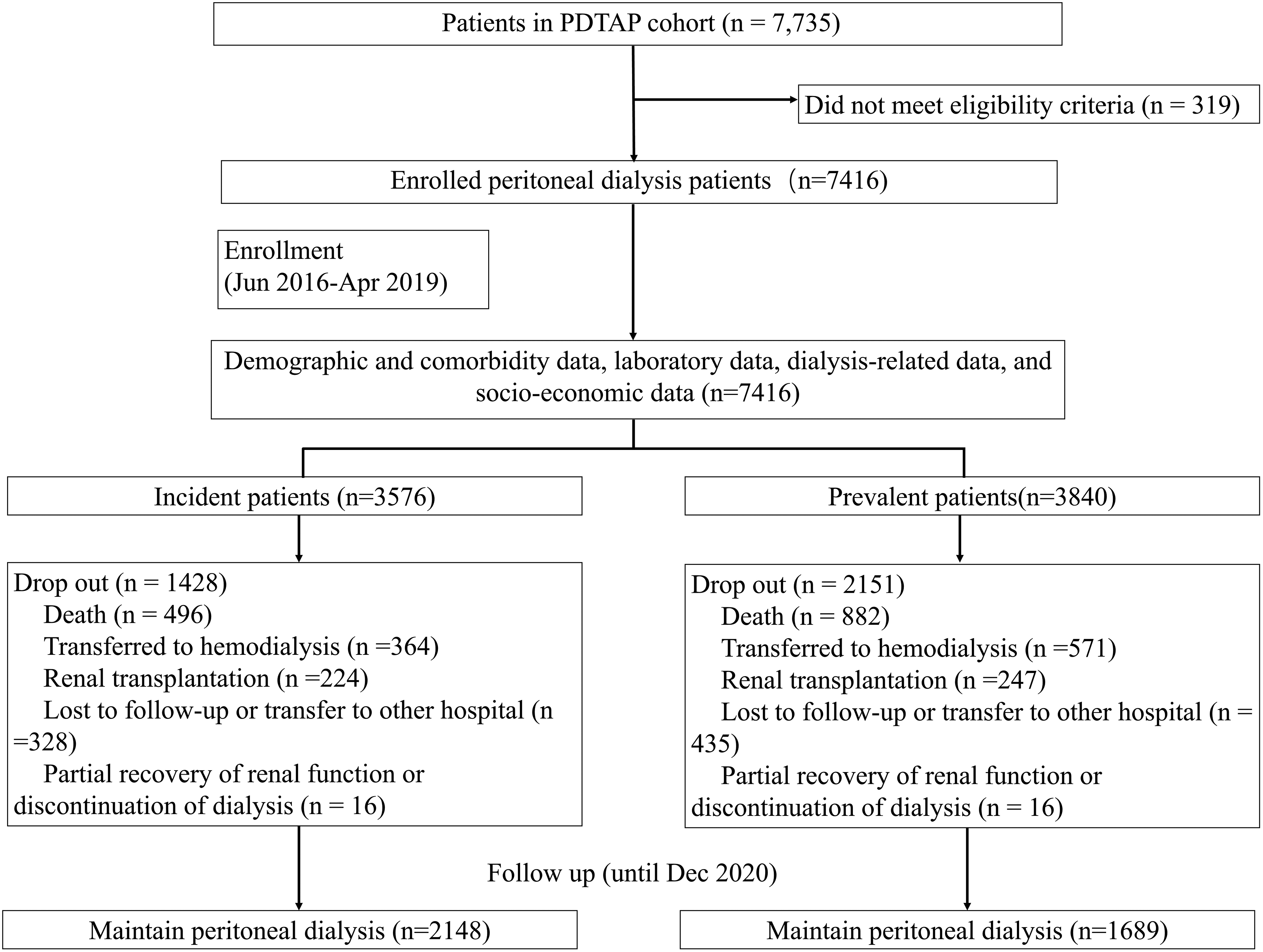
Study flow chart.
Baseline characteristics of patients in the university-affiliated hospitals and non-university-affiliated hospitals. a
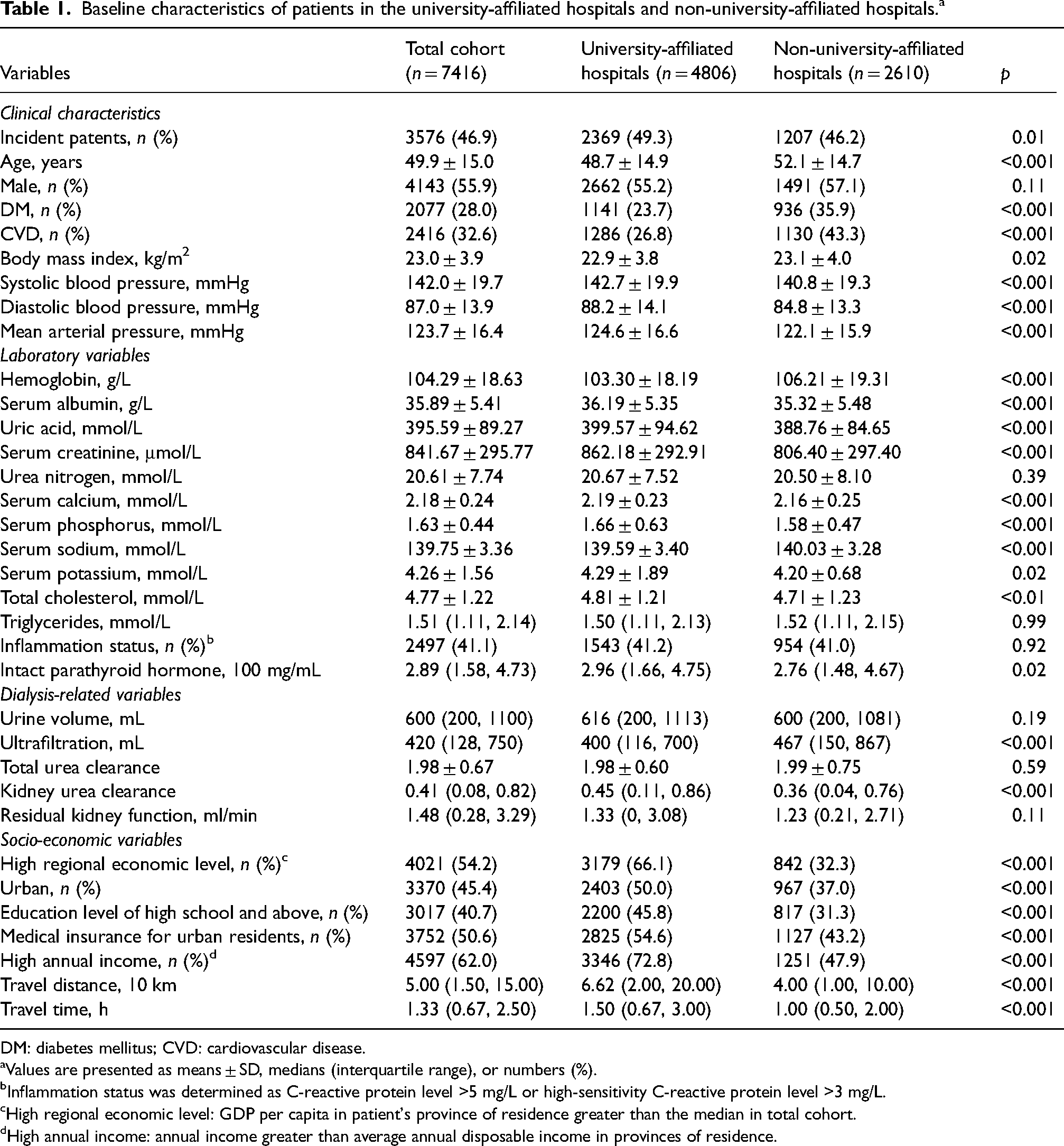
DM: diabetes mellitus; CVD: cardiovascular disease.
Values are presented as means ± SD, medians (interquartile range), or numbers (%).
Inflammation status was determined as C-reactive protein level >5 mg/L or high-sensitivity C-reactive protein level >3 mg/L.
High regional economic level: GDP per capita in patient's province of residence greater than the median in total cohort.
High annual income: annual income greater than average annual disposable income in provinces of residence.
A total of 4806 PD patients were treated in university-affiliated hospitals, while 2610 received treatment in non-university-affiliated hospitals (Table 1). Patients in university-affiliated hospitals were younger and had significantly higher levels of serum albumin, uric acid, calcium, phosphorus, potassium, total cholesterol, intact parathyroid hormone, and kidney urea clearance (p < 0.05 or <0.001). As for socio-economic variables, patients in the university-affiliated hospital group were more likely to reside in urban and economically developed regions, possess better education, higher income, and greater coverage from urban resident medical insurance (p < 0.001), but they experienced longer travel times and travel distances to their hospitals (p < 0.001) (Table 1 and Supplementary Figure 2).
In terms of center characteristics, 14 university-affiliated hospitals and 13 non-university-affiliated hospitals were included (Table 2). Compared to non-university-affiliated hospitals, university-affiliated hospitals had longer years since PD initiation, higher number of beds in the nephrology department, and a higher proportion of patients with cross-city PD treatment (p < 0.05). University-affiliated hospitals also had larger center volumes, higher patient-to-physician and patient-to-nurse ratios, and a slightly lower number of hemodialysis machines, although these differences were not statistically significant.
Center characteristics in the university-affiliated hospitals and non-university-affiliated hospitals.
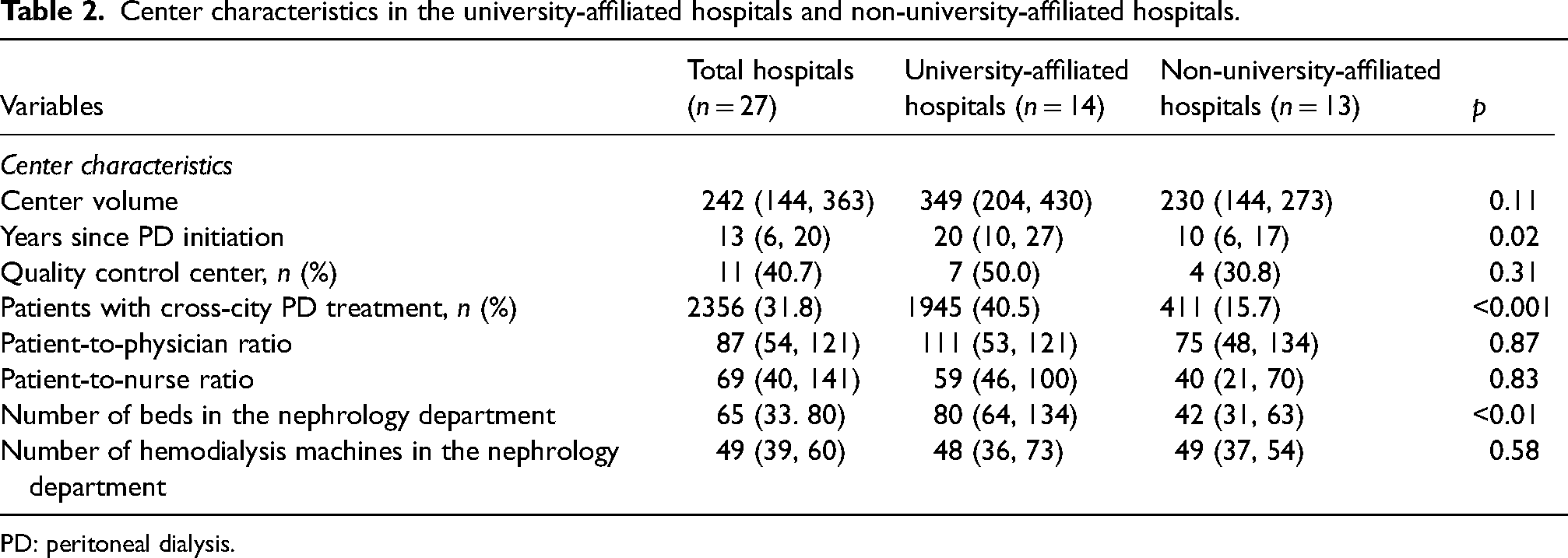
PD: peritoneal dialysis.
Association between hospital type and clinical outcomes
All-cause mortality
As shown in Supplementary Table 2, during the study follow-up period, there were 1378 (18.6%) patients who died, of whom 754 (15.7%) were receiving their treatments at university-affiliated hospitals compared to 624 (23.9%) from non-university-affiliated hospitals (p < 0.001). The median time to death was 16.0 (95% CI 14.5–17.6) months in the university-affiliated hospital group versus 14.0 (95% CI 13.4–16.6) months in the non-university-affiliated hospital group. Although the top three causes of death were consistent, patients in the university-affiliated hospitals experienced fewer cardiovascular deaths and severe malnutrition compared to non-university-affiliated hospitals (p < 0.05).
In the multivariable competing risk regression analysis, university-affiliated hospitals were still associated with a lower risk for all-cause mortality compared to non-university-affiliated hospitals (SHR 0.72, 95% CI 0.61–0.85, p < 0.001) (Table 3). Other characteristics associated with the risk of death included age, diabetes mellitus, cardiovascular disease (CVD), serum albumin, serum creatinine, serum phosphorus, serum sodium, inflammation status, and urine volume (Supplementary Table 3).
SHR for clinical outcomes in different hospital types.
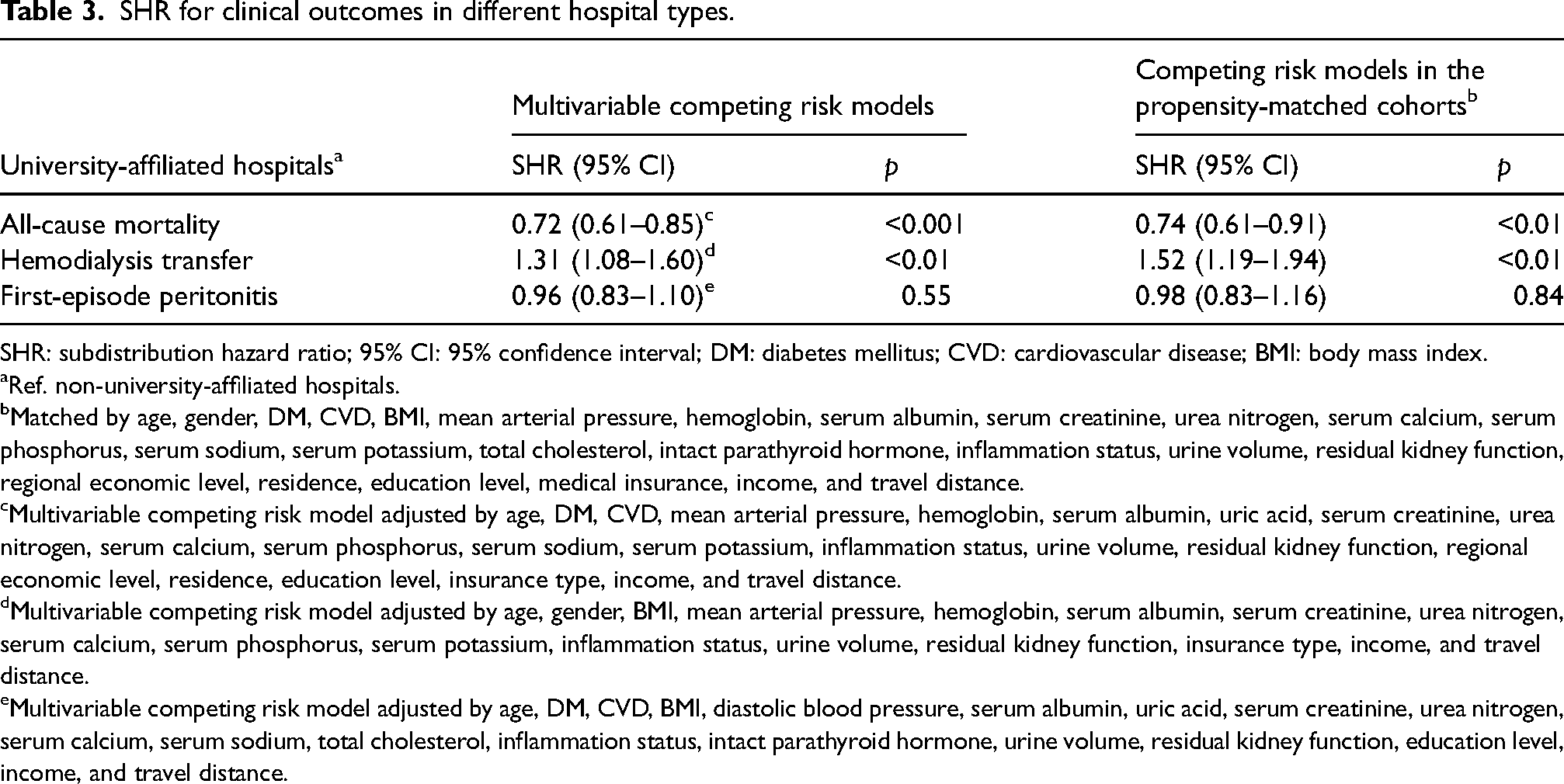
SHR: subdistribution hazard ratio; 95% CI: 95% confidence interval; DM: diabetes mellitus; CVD: cardiovascular disease; BMI: body mass index.
Ref. non-university-affiliated hospitals.
Matched by age, gender, DM, CVD, BMI, mean arterial pressure, hemoglobin, serum albumin, serum creatinine, urea nitrogen, serum calcium, serum phosphorus, serum sodium, serum potassium, total cholesterol, intact parathyroid hormone, inflammation status, urine volume, residual kidney function, regional economic level, residence, education level, medical insurance, income, and travel distance.
Multivariable competing risk model adjusted by age, DM, CVD, mean arterial pressure, hemoglobin, serum albumin, uric acid, serum creatinine, urea nitrogen, serum calcium, serum phosphorus, serum sodium, serum potassium, inflammation status, urine volume, residual kidney function, regional economic level, residence, education level, insurance type, income, and travel distance.
Multivariable competing risk model adjusted by age, gender, BMI, mean arterial pressure, hemoglobin, serum albumin, serum creatinine, urea nitrogen, serum calcium, serum phosphorus, serum potassium, inflammation status, urine volume, residual kidney function, insurance type, income, and travel distance.
Multivariable competing risk model adjusted by age, DM, CVD, BMI, diastolic blood pressure, serum albumin, uric acid, serum creatinine, urea nitrogen, serum calcium, serum sodium, total cholesterol, inflammation status, intact parathyroid hormone, urine volume, residual kidney function, education level, income, and travel distance.
After propensity-score matching, a total of 1082 matched pairs were created. There was no difference in the key factors that were unbalanced in the entire population between the two groups after matching (Supplementary Table 4). Compared to the non-university-affiliated hospital group, patients in the university-affiliated hospital group continued to exhibit a significantly lower risk for all-cause mortality in the matched cohort (SHR 0.74, 95% CI 0.61–0.91, p < 0.01) (Table 3).
Hemodialysis transfer
During the study follow-up period, a total of 935 (12.6%) patients transferred to hemodialysis, of whom 657 (13.7%) were in the university-affiliated hospital group compared to 278 (10.7%) in the non-university-affiliated hospital group (p < 0.001) (Supplementary Table 2). The median time to hemodialysis transfer was 15.0 (95% CI 13.5–16.6) months in the university-affiliated hospital group versus 14.0 (95% CI 12.0–16.0) months in the non-university-affiliated hospital group. Regarding the causes of transfer to hemodialysis, the university-affiliated hospital group recorded more cases of severe fluid overload (p < 0.001), but fewer cases of PD-related infection (p < 0.001) compared to the non-university-affiliated hospital group. In the matched cohort, more patients from the university-affiliated hospital group were transferred to hemodialysis (i.e. 152 vs. 111, p < 0.01) compared to those in the non-university-affiliated hospital group.
After multivariable adjustment, the association between the university-affiliated hospitals and hemodialysis transfer was significant (SHR 1.31, 95% CI 1.08–1.60, p < 0.01, reference:non-university-affiliated hospitals) (Table 3). Other characteristics associated with the risk of hemodialysis transfer included age, body mass index, serum albumin, and urine volume (Supplementary Table 5). In the matched cohort, patients in the university-affiliated hospital group still had a significantly higher risk of hemodialysis transfer compared to those in the non-university-affiliated hospital group (SHR: 1.52, 95% CI: 1.19–1.94, p < 0.01) (Table 3).
First-episode peritonitis
During the study follow-up period, first-episode peritonitis occurred in a total of 1583 (21.3%) patients of whom 976 (20.3%) were in the university-affiliated hospital group, compared to 607 (23.3%) in the non-university-affiliated hospital group (p < 0.001) (Supplementary Table 2). The median time to first-episode peritonitis was 13.0 (95% CI: 11.7–14.3) months in the university-affiliated hospital group versus 10.0 (95% CI: 9.0–11.0) months in the non-university-affiliated hospital group. In terms of outcomes from first-episode peritonitis, the university-affiliated hospitals had a lower percentage of hemodialysis transfer (6.9% vs. 8.1%) and a numerically higher percentage of deaths (2.9% vs. 2.8%) compared to the non-university-affiliated hospitals, but these differences were not statistically significant.
In the multivariable analysis, the association between university-affiliated hospitals and first-episode peritonitis was not significant (SHR: 0.96, 95% CI: 0.83–1.10, p = 0.55, reference: non-university-affiliated hospitals, same below) (Table 3). Characteristics associated with the risk of first-episode peritonitis included age, serum albumin, uric acid, serum creatinine, total cholesterol, inflammation status, and urine volume (Supplementary Table 6). After propensity-score matching, there was still no association between university-affiliated hospitals and first-episode peritonitis (SHR: 0.98, 95% CI: 0.83–1.16, p = 0.84).
Sensitivity analysis
In the multivariable analysis with incident patients only, consistent results were found for all-cause mortality (SHR: 0.71, 95% CI: 0.54–0.95, p = 0.02, reference: non-university-affiliated hospitals, same below) and first-episode peritonitis (SHR 0.98, 95% CI: 0.79–1.21, p = 0.83). However, compared to the total cohort, there were not significant association between university-affiliated hospitals and hemodialysis transfer in incident population (SHR: 1.04, 95% CI: 0.77–1.41, p = 0.80) (Supplementary Tables 7 to 10). After propensity-score matching, consistent results were found for all-cause mortality (SHR: 0.58, 95% CI: 0.43–0.84, p < 0.01), hemodialysis transfer (SHR: 1.20, 95% CI: 0.80–1.80, p = 0.38), and first-episode peritonitis (SHR: 0.82, 95% CI: 0.61–1.09, p = 0.17).
Discussion
Through this multicenter, prospective, PD cohort study in China, it was suggested that being treated in university-affiliated hospitals was independently associated with a lower mortality. After adjustment for confounding factors using propensity-score matching, it was found that patients in these hospitals exhibited a significantly lower risk for all-cause mortality but had a higher risk of hemodialysis transfer.
As shown in our data, university-affiliated hospitals had a larger PD center volume (i.e. 349/center vs. 230/center), and a higher number of beds in the nephrology department (i.e. 80 vs. 42). Notably, the center-clustering effect is still prominent in China.14,20 Our data supported the importance of the center effect in an independently lower risk for all-cause mortality, as was proposed by previous studies.13,21,22 Whether this can be attributed to their advanced experience in training staff on PD patient care, managing PD-related complications, and adherence to standardized clinical pathways based on evidence-based best practices remains unclear. Further studies are needed to investigate and reduce the gap in the quality of care.
Interestingly, the patients from the university-affiliated hospitals in the study faced greater travel distances (i.e. 66.2 vs. 40.0 km) and longer travel times (i.e. 1.50 vs. 1.00 h) from their hospitals. Besides, the proportion of patients with cross-city PD treatment was also significantly higher in university-affiliated hospitals (i.e. 40.5% vs. 15.7%). This trend reflects cross-city mobility, which is common among patients in China. 23 The lack of a strict referral system, regional health inequity and a shortage of nephrology specialty in our country are major factors contributing to this mobility,24,25 which exacerbates the disease burden on patients and leads to the wastage of additional medical and social resources. 26 This phenomenon may also suggest that patients with cross-city PD treatment cared more about their healthcare and were willing to spend more time and money to seek what they consider to be “excellent care,” which could potentially impact their prognosis.
As the demand for kidney replacement therapy continues to rise, the capacity of PD centers in university-affiliated hospitals may become increasingly strained.1,27,28 Therefore, there is an urgent need to address disparities in health quality. Possible solutions include the establishment of national regional medical centers 29 and the formation of medical alliances focused on nephrology or PD specialties,17,30 which may help standardize care practices across different PD centers. The association of telemedicine-based technology and remote patient management with the reduction in all-cause mortality, CVD mortality, and hemodialysis transfer in our country has been proven. 31
Our study revealed a higher risk of hemodialysis transfer among the patients in the university-affiliated hospitals after propensity-score matching, which contrasted with some previous findings.32,33 When restricted to incident patients only, there were not significant association between hospital type and hemodialysis transfer. One potential explanation is that the patients in university-affiliated hospitals were more likely to occur hemodialysis transfer due to volume overload, which is less obvious in incident patients with shorter dialysis duration. This could imply more timely monitor on volume status of patients, and heightened concern for worse outcomes such as cardiovascular events in these centers. Additionally, the university-affiliated hospitals may have established a referral system and a collaborative care team within the nephrology department to support the transfer of dialysis modality.34,35 Overall, when considering both death outcomes and hemodialysis transfers together,36,37 university-affiliated hospitals demonstrated better dialysis treatment sustainability since they had significantly fewer deaths.38,39 The reason for the lower hemodialysis transfer during peritonitis occurrences in university-affiliated hospitals is unclear. More detailed information on their preventive measures, diagnostic techniques, and treatment protocols during peritonitis episodes is needed to explain our findings. 13
This study represents the first comprehensive analysis of the association between university-affiliated hospitals and clinical outcomes in PD patients. Its strengths include a large sample size, comprehensive clinical measures, and robust endpoints that align with the core outcomes identified by the Standardized Outcomes in Nephrology-Peritoneal Dialysis, including all-cause and cause-specific mortality and transfer to hemodialysis. 36 Multivariable adjustment and statistical matching were also applied, which reduced potential confounding effects inherent in observational studies.
Nevertheless, there are limitations to consider. First, all the PD centers included in the PDTAP study were tertiary hospitals located in urban areas, excluding primary and secondary hospitals. The selection of PD centers was not random, which could introduce inherent biases in the patient populations. Additionally, the higher socio-economic status of patients in the university-affiliated hospitals could influence outcomes despite our adjustments for various confounding factors. Finally, due to the observational nature of the study, we could not establish a cause–effect relationship between hospital type and worse clinical outcomes.
In conclusion, we observed that hospital type is associated with all-cause mortality and hemodialysis transfer in the PD population. This study presents the association between health inequality and clinical outcomes and provides real-world evidence of gaps in PD healthcare resources, offering valuable insights for health policymakers, especially in developing countries. To improve health equity in China, further interventions, such as establishing national regional medical centers and creating medical alliances focused on PD, should be explored.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608251350202 - Supplemental material for Hospital type and clinical outcomes in peritoneal dialysis: Findings from the PDTAP study
Supplemental material, sj-docx-1-ptd-10.1177_08968608251350202 for Hospital type and clinical outcomes in peritoneal dialysis: Findings from the PDTAP study by Qinghua Wang, Yong Zhang, Shaomei Li, Huayi Pei, Jinghong Zhao, Ying Zhang, Zibo Xiong, Yumei Liao, Ying Li, Qiongzhen Lin, Wenbo Hu, Yulin Li, Zhaoxia Zheng, Liping Duan, Gang Fu, Shanshan Guo, Beiru Zhang, Rui Yu, Fuyun Sun, Xiaoying Ma, Li Hao, Guiling Liu, Zhanzheng Zhao, Jing Xiao, Xuanyi Du, Tianrong Ji, Caili Wang, Lirong Deng, Yingli Yue, Shanshan Chen, Zhigang Ma, Yingping Li, Li Zuo, Huiping Zhao, Xianchao Zhang, Xuejian Wang, Yirong Liu, Xinying Gao, Xiaoli Chen, Hongyi Li, Shutong Du, Cui Zhao, Zhonggao Xu, Li Zhang, Hongyu Chen, Li Li, Lihua Wang, Yan Yan, Yingchun Ma, Yuanyuan Wei, Jingwei Zhou, Yan Li, Yingdong Zheng, Yulan Shen, Jie Dong and the PDTAP working group in Peritoneal Dialysis International
Supplemental Material
sj-doc-1-ptd-10.1177_08968608251350202 - Supplemental material for Hospital type and clinical outcomes in peritoneal dialysis: Findings from the PDTAP study
Supplemental material, sj-doc-1-ptd-10.1177_08968608251350202 for Hospital type and clinical outcomes in peritoneal dialysis: Findings from the PDTAP study by Qinghua Wang, Yong Zhang, Shaomei Li, Huayi Pei, Jinghong Zhao, Ying Zhang, Zibo Xiong, Yumei Liao, Ying Li, Qiongzhen Lin, Wenbo Hu, Yulin Li, Zhaoxia Zheng, Liping Duan, Gang Fu, Shanshan Guo, Beiru Zhang, Rui Yu, Fuyun Sun, Xiaoying Ma, Li Hao, Guiling Liu, Zhanzheng Zhao, Jing Xiao, Xuanyi Du, Tianrong Ji, Caili Wang, Lirong Deng, Yingli Yue, Shanshan Chen, Zhigang Ma, Yingping Li, Li Zuo, Huiping Zhao, Xianchao Zhang, Xuejian Wang, Yirong Liu, Xinying Gao, Xiaoli Chen, Hongyi Li, Shutong Du, Cui Zhao, Zhonggao Xu, Li Zhang, Hongyu Chen, Li Li, Lihua Wang, Yan Yan, Yingchun Ma, Yuanyuan Wei, Jingwei Zhou, Yan Li, Yingdong Zheng, Yulan Shen, Jie Dong and the PDTAP working group in Peritoneal Dialysis International
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National High Level Hospital Clinical Research Funding (Scientific and Technological Achievements Transformation Incubation Guidance Fund Project of Peking University First Hospital), CAMS Innovation Fund for Medical Sciences, National High Level Hospital Clinical Research Funding (High Quality Clinical Research Project of Peking University First Hospital), Scientific Research Project of Capital Health Development (grant number: 2022CX09, 2019-I2M-5-046, 2022CR82, 2020-2-4079).
Ethical approval
This study protocol was reviewed and approved by the Ethics Committee of Peking University First Hospital, approval number [2018-100]. Written informed consent was obtained from participants before the study.
Informed consent to participate
Written informed consent was obtained from participants before the study.
Informed consent to publish
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Author contributions
Research idea and study design: JD; data acquisition: HY Pei, YL Li, YM Liao, J Xiao, QZ Lin, LP Duan, TR Ji, R Yu, GL Liu, LR Deng, L Li, HP Zhao, Y Zhang, Y Yan, YP Li, XJ Wang, XY Gao, L Zhang, C Zhao, HY Li, SS Chen, YY Wei, and Yan Li; statistical analysis: QH Wang and JD; and supervision or mentorship: SM Li, JH Zhao, ZB Xiong, ZZ Zhao, Y Li, ZX Zheng, G Fu, SS Guo, XY Ma, XY Du, WB Hu, FY Sun, BR Zhang, L Hao, CL Wang, HY Chen, L Zuo, YL Shen, LH Wang, ZG Ma, XC Zhang, YR Liu, ZG Xu, ST Du, XL Chen, YL Yue, YC Ma, JW Zhou, YD Zheng and JD. All authors read and approved the final manuscript. Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions about the accuracy or integrity of any portion of the work are appropriately investigated and resolved. JD takes responsibility that this study has been reported honestly, accurately, and transparently, that no important aspects of the study have been omitted, and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Acknowledgements
The authors express their appreciation to the patients, doctors, and nursing staff of all PD centers of Peking University First Hospital, the Second Hospital of Hebei Medical University, Xinqiao Hospital of Army Medical University, Peking University Shenzhen Hospital, the First Affiliated Hospital of Zhengzhou University, the Third Hospital of Hebei Medical University, Handan Central Hospital, Peking Haidian Hospital, People's Hospital of Qinghai Province, Cangzhou Central Hospital, the Second Affiliated Hospital of Harbin Medical University, Sheng Jing Hospital affiliated to China Medical University, the Second Affiliated Hospital of Anhui Medical University, the First Affiliated Hospital of BaoTou Medical College, People's Hospital of Chuxiong, Peking University People's Hospital, Beijing Miyun District Hospital, Second Hospital of Shanxi Medical University, People's Hospital of Gansu, Pingdingshan First People's Hospital, the First People's Hospital of Xining, First Hospital of Jilin University, Cangzhou People's Hospital, Taiyuan Central Hospital, People's Hospital of Langfang, Beijing Charity Hospital, and Beijing Dongzhimen Hospital.
Availability of data and materials
The data that support the findings of this study will not be openly available because of sensitivity. Data are located in controlled access data storage in accordance with regulations of China on Human Genetic Resources Management.
Trial registration
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.