
Abstract
Identifying risk factors that pre-dispose people on peritoneal dialysis (PD) to develop exit site infections (ESIs) may help improve prevention and treatment. Given the differences anatomically, hormonally and of the microbiota profile between males and females, we hypothesised that there is a difference in ESI incidence, outcomes, and the epidemiology of organism-specific ESI between males and females. This study was a retrospective case note review of all PD patients at our centre between 2012 and 2024. Of the 486 patients on PD, 202 (42%) were female and 273 positive swabs from 151 patients were identified (0.18 patient episodes/year). We found no statistically significant difference in the incidence of ESI between sexes in our cohort. Gram-positive organisms accounted for 126/273 (46.2%) of all ESI swabs, suggesting that current empiric antibiotic therapy potentially offers effective treatment for less than half of ESI only. We found significant morbidity from ESI: 39 (14%) patients developed peritonitis and 40 (15%) required catheter removal. Sex had no influence on ESI incidence, microbiology of infection or outcome.
Background
Peritoneal dialysis (PD)-related infections have been ranked as the most critically important clinical outcomes in PD by patients, carers and clinicians. 1 Identifying risk factors that pre-dispose people on PD to develop exit site infections (ESIs) may help improve prevention and treatment. 2
Data on ESI incidence and microbiology are not routinely recorded in large registry datasets such as the US Renal Data System (USRDS), the Australian and New Zealand Dialysis and Transplant (ANZDATA) registry, or the UK Renal Registry (UKRR). 3 Consequently, differences in epidemiology, microbiology and ESI-related morbidity and mortality have not been explored.
Sex is a biological variable that affects both susceptibility and immunological response to infectious diseases, and can influence illness severity and outcomes. 4 Many common bacterial pathogens exhibit a sex preference, with most showing a male bias. 5 Experimental models have consistently shown a survival advantage and protective effect of sex hormones in females 6 with several studies suggesting that PD peritonitis rates are significantly higher in males.7,8 However, multiple studies have also found that peritonitis-related mortality is significantly higher in females9-11: the reason for this disparity is not clear.
The most common exogenous route to the peritoneal cavity is via contamination with skin pathogenic bacteria through the exit site (ES) and tunnel.12,13 Endogenous contamination of the peritoneal cavity can occur, through haematogenous spread, vaginal leakage and disruption of the intestinal epithelial barrier with subsequent translocation of microorganisms.12,13
Given the differences anatomically, hormonally and of the microbiota profile between males and females, we hypothesised that there is a difference in ESI incidence, outcomes, and the epidemiology of organism-specific ESI between the two sexes.
Methods
This is a retrospective case note review of all incident culture positive ES swabs from PD patients at our centre between 01/01/2012–01/01/2024: ethical approval was therefore not required. At our centre, all positive ES swabs are routinely recorded into a central database. Culture negative ES swabs are not routinely recorded, therefore culture negative ESI were excluded from this study. We were unable to locate ESI records for a 5-month period 2018–2019 when clinical records transitioned from paper to electronic recording. Only straight neck, straight tip, double cuff catheters are used at our centre and all patients were trained in standard exit site (ES) care, using mupirocin at the time of ES dressings.
Data were transcribed from patient medical records and included age, sex, organism isolated on ES swab, cause of end-stage kidney disease (ESKD), comorbidities, date of PD catheter insertion, intervention/treatment(s) including catheter removal and/or catheter replacement and peritonitis incidence. Sex of the patient was doctor-determined and confirmed with case records.
Statistical differences between groups were analysed using an unpaired t-test for parametric data, and Mann–Whitney test for nonparametric data. Data were tested for normality of distribution using the Shapiro–Wilk normality test. A Fishers exact test was used to compare categorical data. For this, data were analysed using the GraphPad Prism 9.2 software package (GraphPad Software, San Diego, California USA). A Poisson Regression Model was used to account for potential non-independence and clustering of data. This model was implemented in R using the ‘dplyr’ package (R version 4.1.3, 2022-03-10). P-values of <0.05 were considered significant.
Results
Demographics
During the 12-year study period, 202/486 patients on PD were female (42%). 273 positive swabs from 151 patients (66F, 85M) were identified (0.18 patient episodes/year), which is within the recommended rate of <0.4 episodes/year in the ISPD 2023 guidelines. 2
Females had a younger mean age at time of ESI compared to males (57.5 years vs 63.9 years, p = 0.0006) (Table 1), but when multiple infections in the same individual were accounted for through poisson regression analysis (multivariate analysis), age did not influence the likelihood of ESI infection (Table 2).
Cohort demographics.
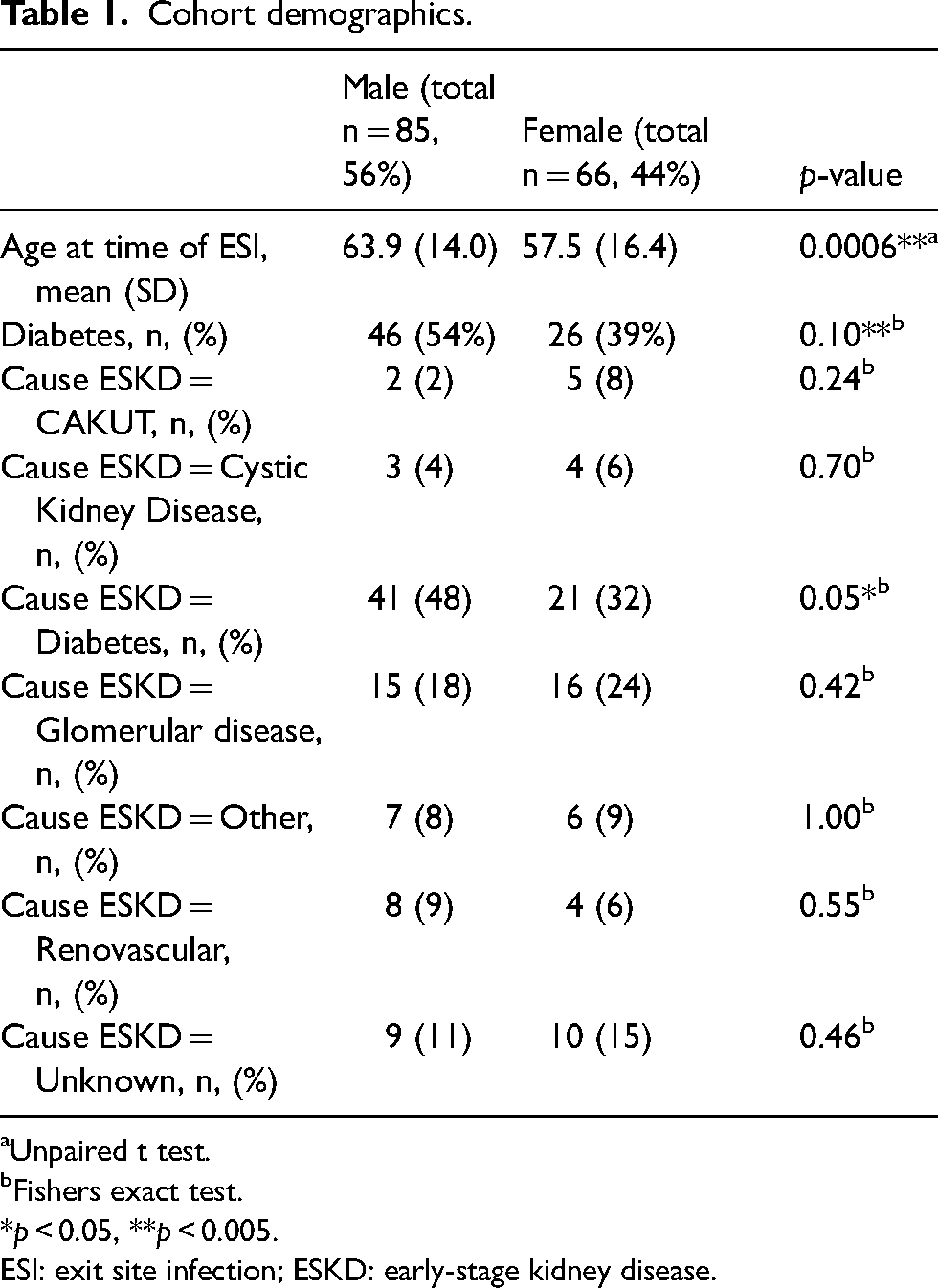
Unpaired t test.
Fishers exact test.
*p < 0.05, **p < 0.005.
ESI: exit site infection; ESKD: early-stage kidney disease.
Multivariable regression model.
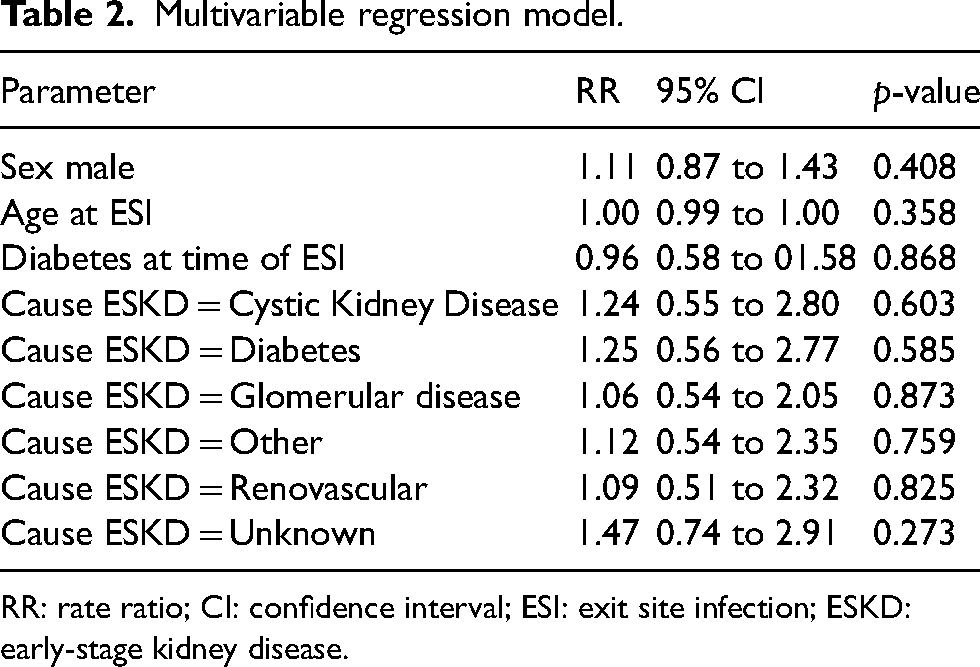
RR: rate ratio; CI: confidence interval; ESI: exit site infection; ESKD: early-stage kidney disease.
Men were more likely to have diabetes as their cause of ESKD than women (48% vs 32%, p = 0.05, Table 1) but there was no significant difference in the overall number of men and women with diabetes as a comorbidity (54% vs 39%, p = 0.10). On multivariate analysis, diabetes did not influence the likelihood of ESI (Table 2). There were no significant differences amongst other causes of ESKD between the sexes (Table 1).
Exit site infections
There was no difference seen in the mean interval between PD insertion and ESI in males and females (723 days vs. 730 days, p = 0.97). 126/273 (46.2%) of ESI cultures were from Gram-positive organisms. Twice as many positive ES swabs for anaerobes came from male patients, but this did not reach statistical significance (Figure 1). Sex did not influence the likelihood of ESI infection (p = 0.41, Table 2).
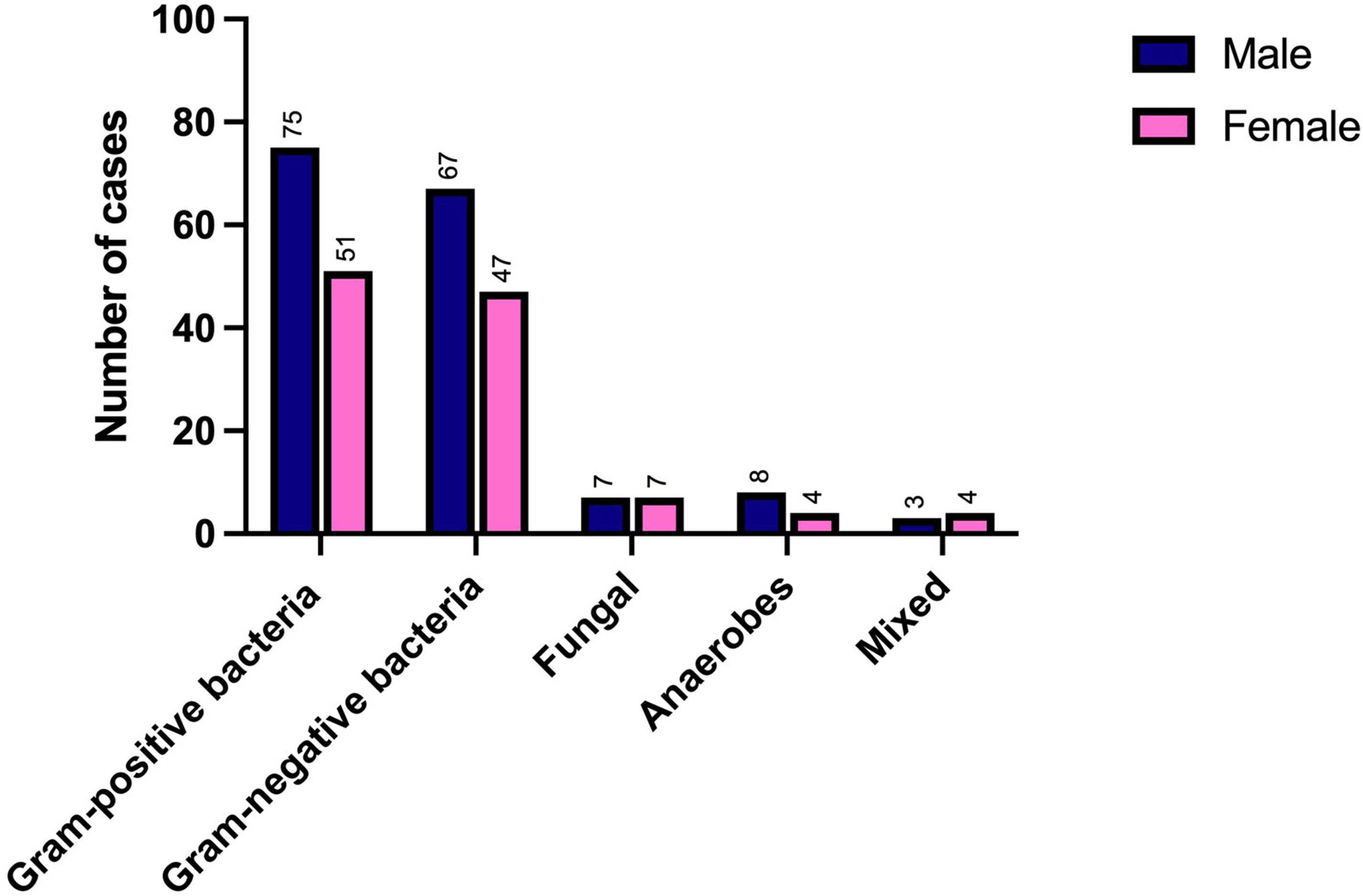
Epidemiology of microorganisms grown from positive exit site swabs. No significant differences in incidence between males and females across any group of microorganisms were seen.
Clinical outcomes
39/273 (14%) ESI resulted in peritonitis (14F, 25M) and 40/273 (15%) ESI required catheter removal and/or replacement (18F, 22M). Of the 40 ESI requiring catheter removal, 7 cases were due to concomitant peritonitis (3F, 4M).
There were no sex differences in incidence of ESI-associated peritonitis (p = 0.49) nor ESI-associated catheter removal (p = 0.86). Of the ESI resulting in peritonitis (same organism seen in all cases), 19/39 (49%) ESI cultures were from Gram-positive bacteria (with Staphylococcus aureus accounting for 17/19 (89%) cases). 18/39 (46%) were Gram-negative bacteria (with Pseudomonas aeruginosa accounting for 12/18 cases and Klebsiella pneumonia 3/18 cases). The remaining 2/39 cases of peritonitis resulted from fungal infection.
Discussion
This is one of the largest series of ESI reported. We found significant morbidity from ESI but that sex has no influence on ESI likelihood, microbiology of infection or ESI outcome. Our findings also emphasise the changing epidemiology of PD-related infections.
Current International Society for Peritoneal Dialysis (ISPD) guidelines suggest using antibiotics with ‘S. aureus coverage’ as first-line antibiotic therapy for ESI-associated infections 2 as historically Gram-positive infection has predominated in most countries. 14 Old studies (2006) showed 62% of peritonitis infections in the USA and 61% in Canada were caused by Gram-positive organisms, 15 but these rates had fallen to 37% and 45%, respectively, by 2020. 7 This may relate to the use of mupiricin for ES care, as per the ISPD guidelines. 2 Similar studies on ESI epidemiology are not available, but we hypothesise that a similar downtrend in Gram-positive infections is likely to have occurred.
Our findings showed that locally, Gram-positive infection only accounts for 46% of ESI infections (44% of peritonitis cases), meaning current empiric antibiotic therapy offers effective treatment for less than half of all ESI. We propose that broader first-line therapy (or dual therapy with Gram-negative/anti-Pseudomonal cover) for ESI should be considered. Bernardini and colleagues’ study highlighted the anti-pseudomonal benefits of gentamicin cream 16 but gentamicin cream is not universally available in the United Kingdom, so standard practice here is mupiricin. 2
We found sex had no difference in clinical outcomes between males and females. This may be reflective of the low incidence of ESI in our cohort. Furthermore, we would be keen to know whether menopausal/ hormonal status influences ESI incidence. Unfortunately the number of young females in our cohort was very small, limiting our ability to undertake this analysis, but future work exploring hormonal status in larger datasets would be very valuable.
Limitations of this study are that it is a single-centre study, with a 5-month period missing. Culture negative swabs are not recorded at our centre, so we were unable to retrospectively identify patients with purulent ES and culture negative infections. We were also unable to reliably identify from the casenotes whether PD was family-assisted or not. Contact contamination could have contributed to ESI and future work should ensure this data is collected. Future studies could also explores sex differences in microbiota profiles in ESI.
Given the small number of patients included despite a 12-year follow-up period, we suggest that larger studies to explore subtle sex differences are needed, and importantly, national registries should encourage recording of epidemiological data on exit site associated infections, as these are major infections for people treated with PD.
Footnotes
Author contributions
HB, RC and EAB participated in study conception and design. HB, LC, SP, AG, GT, RC and EAB participated in data acquisition. HB and EAB undertook data analysis/interpretation. HB drafted the article and all authors undertook critical revision of the manuscript to its final form. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H.B, L.C, A.G, and G.L report no conflicts of interest. S.P: Nursing Committee-International Society for Peritoneal Dialysis. Speaker - Baxter Healthcare, Fresenius Medical Care. Consultancy fees –Baxter Healthcare. R.C: Speaker - Baxter Healthcare. E.B: Advisory board - Fresenius Medical Care. Speaker - Baxter Healthcare, Fresenius Medical Care.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Infrastructure support for this research was provided by the NIHR Imperial Biomedical Research Centre (BRC).