
Abstract
Background
Peritoneal dialysis (PD)—associated peritonitis is a major complication in PD and may require abdominal imaging to identify the intra-abdominal pathology, though its clinical utility remains unclear.
Methods
This retrospective, single-center study included all episodes of PD-associated peritonitis that occurred between January 2013 and July 2024. The primary objective was to identify factors predicting the use of abdominal imaging during peritonitis episodes.
Results
A total of 691 episodes of peritonitis occurred in 376 PD patients during the study period. Of these, 354 episodes (51%) were subjected to abdominal imaging, which revealed 102 episodes (29%) suggestive of enteric or other secondary peritonitis. The most common abnormal imaging findings were colitis or enteritis, followed by ileus or intestinal obstruction. Imaging findings indicating the need for urgent medical or surgical attention were observed in 27 episodes of peritonitis (7.6%). Imaging was more frequently performed in peritonitis episodes caused by polymicrobial enteric bacteria (adjusted odds ratio [AOR]: 4.49; 95% CI [2.13–9.48]), single enteric bacteria (AOR: 2.02; 95% CI [1.31–3.13]), and fungi (AOR: 7.77; 95% CI [2.48–24.29]), compared to nonenteric bacteria. Hypotension (AOR: 6.19; 95% CI [2.81–13.66]), cloudy effluent (AOR: 1.91; 95% CI [1.30–2.80]), and higher PD effluent cell counts at presentation (AOR: 1.03; 95% CI [1.01–1.05]) were all significantly associated with imaging. Only polymicrobial infection involving enteric bacteria (AOR: 2.65; 95% CI [1.28–5.50]) was significantly associated with abnormal imaging findings suggestive of secondary or enteric peritonitis. Furthermore, polymicrobial infections with enteric bacteria (AOR: 9.17; 95% CI [3.29–25.50]), fungal infections (AOR: 5.25; 95% CI [1.26–21.96]), and hypotension (AOR: 2.77; 95% CI [1.08–7.07]; p = .03) were significantly associated with critical imaging findings.
Conclusion
Imaging in PD peritonitis was primarily performed based on causative organisms or clinical features. Only polymicrobial enteric peritonitis, fungal infections, and hypotension were significantly associated with critical imaging findings. Future prospective studies are required to improve diagnostic accuracy and guide imaging decisions in PD-related peritonitis.
Keywords
Introduction
Peritoneal dialysis (PD) is a widely utilized renal replacement therapy for patients with end-stage kidney disease. Despite its benefits, PD-associated peritonitis is a common and serious complication that contributes significantly to morbidity and mortality in PD patients.1–3 Prompt diagnosis and appropriate treatment are essential to prevent adverse outcomes, including catheter loss, intra-abdominal complications, and transition to hemodialysis (HD).4,5
Diagnosis of PD-associated peritonitis is primarily based on clinical features such as abdominal pain, cloudy PD effluent, along with laboratory confirmation of elevated peritoneal dialysate white cell count (predominantly polymorphonuclear) and positive microbiological cultures.3,6,7 While most peritonitis cases are attributed to touch contamination or breaks in sterile technique during PD procedures,7,8 the underlying cause often remains unknown in many cases. Enteric peritonitis or other intra-abdominal pathology can also contribute to these clinical presentations, and abdominal imaging may help identify such conditions, which may require additional therapeutic approaches such as surgical intervention.
Imaging modalities, such as computed tomography (CT) and ultrasound abdomen, are valuable tools for detecting intra-abdominal pathology, including bowel obstruction or perforation, intra-abdominal abscesses, and other intra-abdominal infections. 9 Despite its potential utility, the role of imaging in PD peritonitis remains poorly defined. The 2022 update of the International Society for PD (ISPD) Peritonitis Guidelines highlights the importance of imaging in cases where secondary causes of peritonitis are suspected. 7 However, the ISPD guidelines do not specify which clinical features should prompt the use of abdominal imaging to detect secondary peritonitis in these patients. Additionally, there is a lack of evidence to guide both the need for and predictors of such imaging.
The indiscriminate use of contrast imaging exposes patients to radiation and may potentially compromise residual kidney function.10–12 However, data on the prevalence of intra-abdominal causes detected in peritonitis patients undergoing imaging remain limited. Studies in this area are scarce, and the frequency and diagnostic yield of imaging for identifying intra-abdominal pathology in this population are unclear. A previous study by Trinh and Bargman et al. reported the prevalence of imaging use and associated abnormalities; however, the number of peritonitis episodes was small, and most patients were Caucasian. 13 There is a lack of data on the prevalence of imaging use and the proportion of cases in which imaging detects intra-abdominal pathology as the cause of peritonitis among the Asian PD population. Our study aimed to address this knowledge gap.
Methods
Study design and population
This was a single-center retrospective cohort study conducted at Singapore General Hospital. The study included all episodes of PD peritonitis from January 2013 to July 2024. The study was conducted as a clinical audit and was exempted from the ethical review by the SingHealth Centralized Institutional Review Board (CRIB).
Data collection
The study collected the demographic and clinical data of patients, including age, gender, race, the primary cause of kidney failure, comorbidities, modality of PD, and receiving financial support from a Voluntary Welfare Organization (VWO). VWO refers to community-based or nongovernmental groups that provide financial or social support services to patients in need, particularly those with limited socioeconomic resources. Detailed information regarding each episode of peritonitis including the date of peritonitis, clinical presentation such as the presence of fever, abdominal pain, hypotension (defined as either systolic blood pressure below 100 mmHg, a mean arterial pressure of < 65 mmHg, or the need for vasopressor support), cloudy PD effluent on presentation (patients who were aware of cloudy effluent or were reported to have cloudy effluent at presentation), laboratory results such as PD effluent cell count on initial presentation, and causative organisms—subcategorized into five groups: nonenteric bacteria, enteric bacteria (single organisms), enteric bacteria (polymicrobial), fungi, and culture-negative peritonitis—were collected. The date and type of abdominal imaging and findings reported by radiologists were also recorded. Imaging findings were classified as (1) no significant abnormalities detected, (2) abnormal findings suggestive of enteric or other intra-abdominal pathology as a cause of peritonitis, and (3) abnormal findings unrelated to the etiology of peritonitis. Relapsing peritonitis was defined as an episode that occurs within four weeks of completion of therapy of a prior episode with the same organism and recurrent peritonitis was defined as an episode occurring within four weeks of completion of therapy of a prior episode with a different organism. 7
Study outcomes
The primary outcome of the study was to evaluate the factors influencing the use of abdominal imaging in PD patients with peritonitis. The secondary outcomes included assessing the prevalence, types, and findings of imaging, particularly those indicating intra-abdominal pathology as a cause of peritonitis or requiring urgent medical or surgical attention. In addition, the study examined factors predicting enteric or other intra-abdominal causes of peritonitis and factors predicting critical imaging findings. Enteric peritonitis was defined as peritonitis originating from an intestinal source, including inflammation, perforation, or ischemia of intraabdominal organs. 7 Critical imaging findings referred to intra-abdominal pathologies requiring urgent medical or surgical intervention, such as appendectomy for appendicitis or bowel resection for ischemic bowel.
Statistical analysis
The categorical variables of baseline demographics data and clinical characteristics were presented as frequencies (percentage), and continuous variables were presented as mean ± standard deviation or median (interquartile range) as per data distribution. Categorical variables were compared using the chi-square test or Fisher's exact test as appropriate. Continuous variables were analyzed using the nonindependent t-test. The primary outcome was analyzed using logistic regression. Variables with p-value < .2 in the univariate analysis were included in the multivariable analysis. The same model was used for the secondary outcome analysis. For the outcome of critical imaging findings, given the limited number of events, only variables with a p-value of < .2 in the univariate analysis were included in the final model. A p-value < .05 was considered statistically significant. Statistical analysis was performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA).
Results
There was a total of 691 episodes of peritonitis that occurred in 376 PD patients between January 2013 and July 2024. Of these, 354 (51%) episodes had abdominal imaging (Supplemental Figure S1). The commonest type of imaging used was contrasted CT of abdomen and pelvic (AP) scan (n = 343, 96.9%), followed by noncontrasted CT AP scan (n = 6, 1.7%), and ultrasound abdomen (n = 5, 1.4%). Baseline characteristics of patients who had undergone imaging during at least one peritonitis episode and those who had never undergone imaging for peritonitis were presented in Table 1.
Demographics of patients with and without abdominal imaging performed.
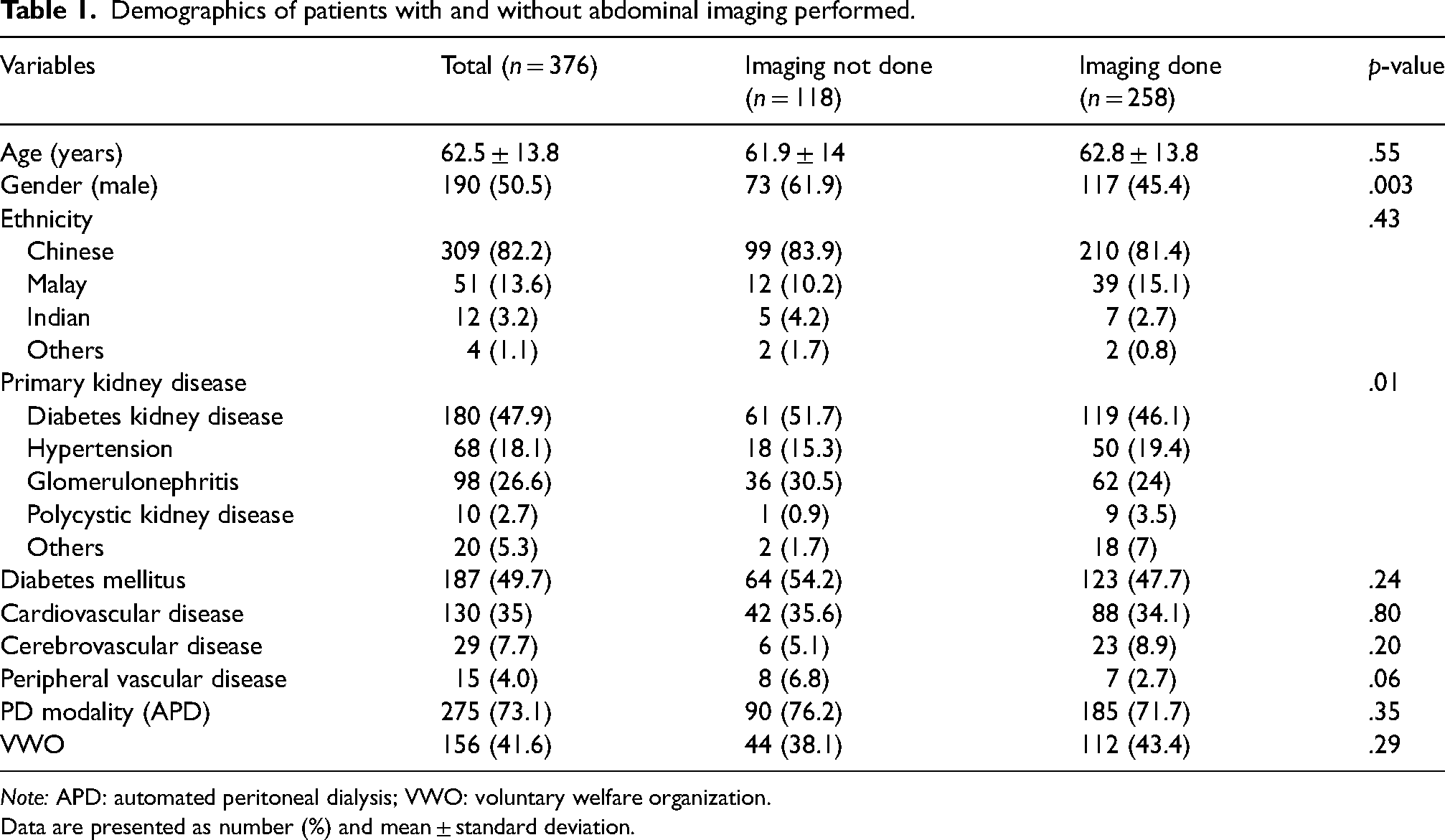
Note: APD: automated peritoneal dialysis; VWO: voluntary welfare organization.
Data are presented as number (%) and mean ± standard deviation.
All imaging was conducted during inpatient admissions. Median time to imaging from peritonitis was 2 days (Interquartile range 1–3). Approximately 16.1% of imaging episodes were conducted on the same day of presentation, 42.4% performed between day 1 and day 2, 41.5% conducted on day 3 onwards, when microbiological data and early clinical response would likely have been accessible to guide decision-making.
Factors associated with imaging use in PD peritonitis
Compared to nonenteric organisms, polymicrobial enteric organisms (adjusted odds ratio [AOR]: 4.49: 95% CI [2.13–9.48]; p < .001), single enteric organisms (AOR: 2.02; 95% CI [1.31–3.13]; p = .002), and fungal organisms (AOR: 7.77; 95% CI [2.48–24.29]; p < .001; Table 2) were significantly associated with higher odds of imaging. Clinical features including hypotension (AOR: 6.19; 95% CI [2.81–13.66]; p < .001), cloudy effluent (AOR: 1.91; 95% CI [1.30–2.80]; p = .001), and higher PD effluent cell counts at presentation (AOR: 1.03; 95% CI [1.01–1.05]; p = .01) were also independently associated with higher odds of imaging. Relapsing or recurrent peritonitis, fever, and abdominal pain were not significantly associated with performing imaging.
Multivariable logistic regression of factors predicting imaging in PD-related peritonitis.
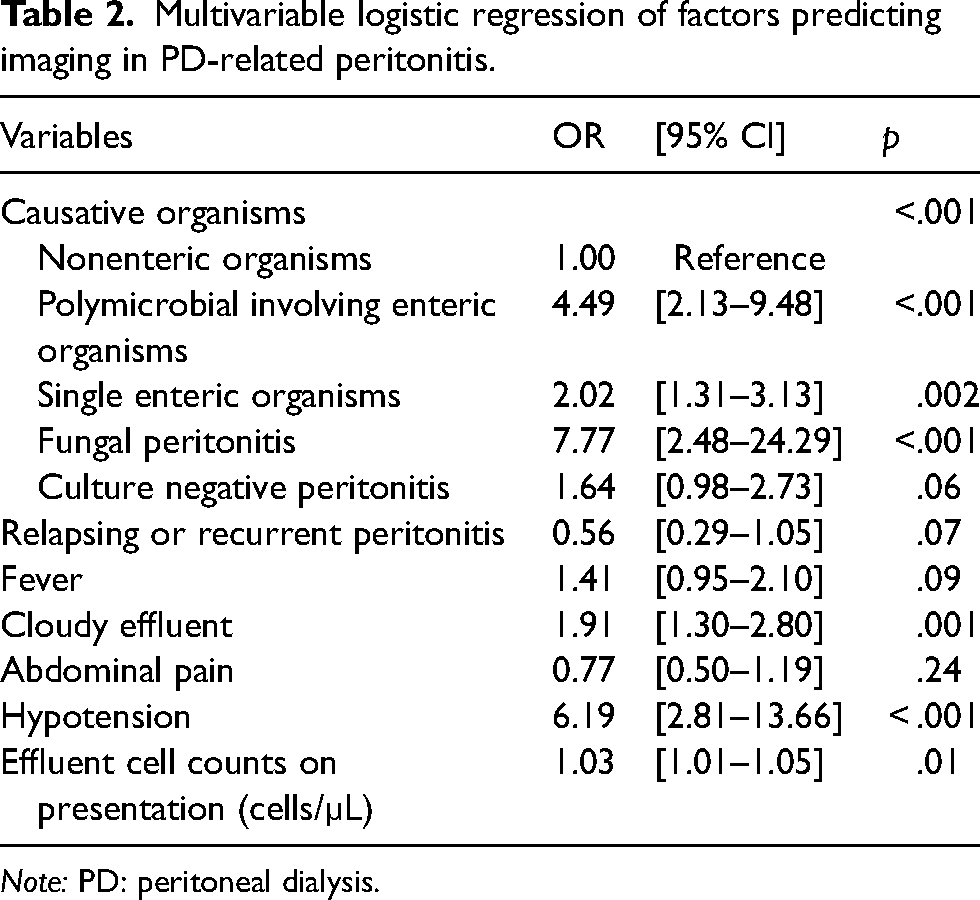
Note: PD: peritoneal dialysis.
Imaging findings in peritonitis
Out of 354 episodes of peritonitis that underwent imaging, approximately half (n = 185, 52%) showed no significant abnormalities. The remaining 169 episodes (48%) were reported as having abnormal findings, with 67 (19%) of them had abnormal findings that were not related to peritonitis, and only 102 (29%) were reported to have pathologies for enteric or other secondary peritonitis (Figure 1). The most common abnormal imaging findings were colitis or enteritis (n = 29) and ileus or intestinal obstruction (n = 16) (Supplemental Table S1). The critical imaging findings that required urgent medical or surgical attention were observed in 27 (7.6%) cases, including appendicitis (n = 6), cholecystitis (n = 6), and bowel ischemia or perforation (n = 4) (Supplemental Table S2). Other abnormal findings, such as diverticulosis (n = 28) and gallstones (n = 24), were also reported (Supplemental Table S3).
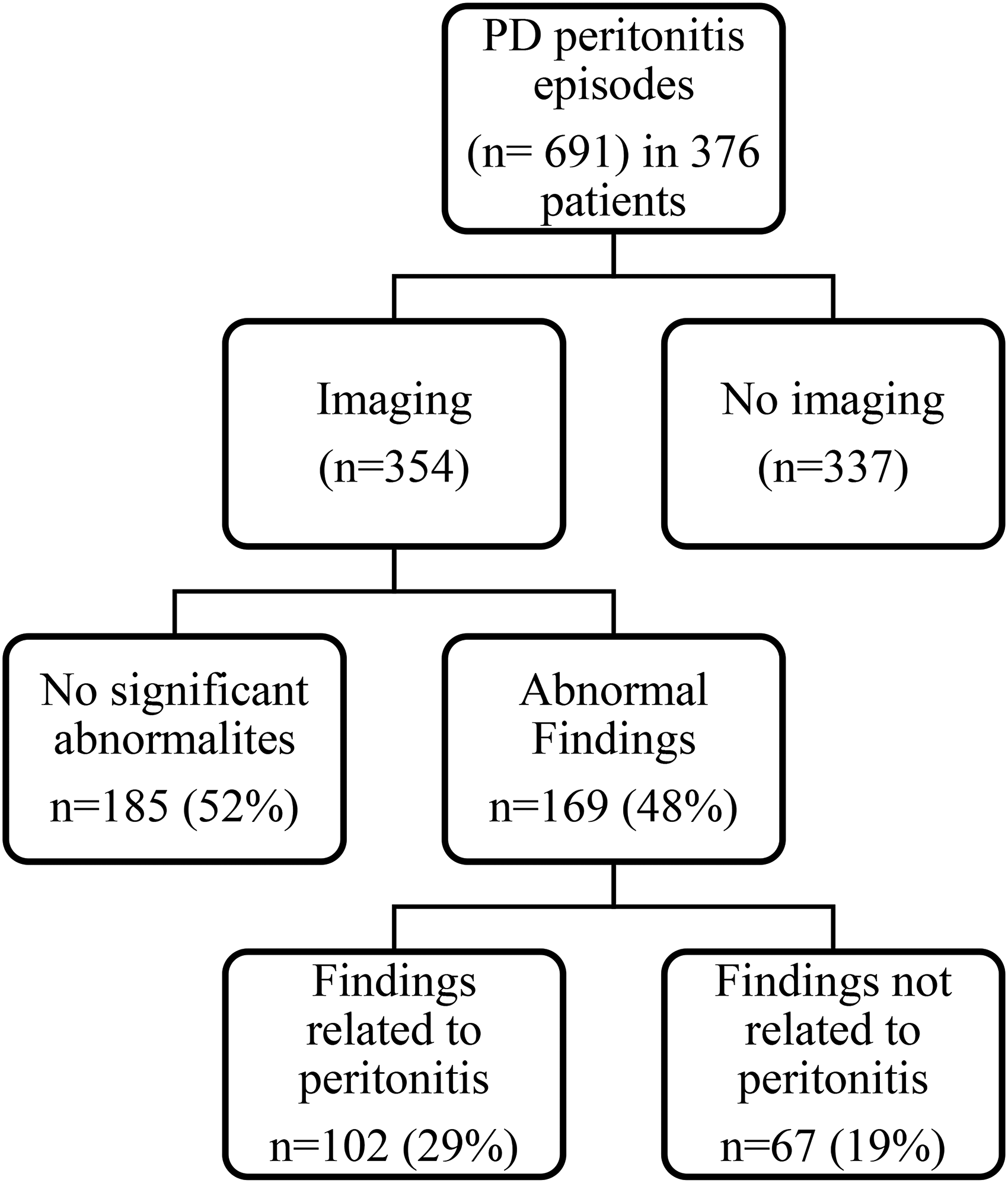
Flow diagram of imaging utilization and findings in peritoneal dialysis-related peritonitis.
Factors predicting enteric or other intra-abdominal pathology causing peritonitis
The type of causative organism was significantly associated with the likelihood of imaging findings suggestive of enteric or secondary peritonitis, whereas clinical features such as fever, abdominal pain, and hypotension were not (Table 3). Among all causative organisms, only polymicrobial infections involving enteric bacteria were significantly associated with increased odds of such imaging findings (AOR: 2.65; 95% CI [1.28–5.50]; p = .01), compared to nonenteric infections. In contrast, single enteric organisms (AOR: 1.78; 95% CI [0.98–3.22]; p = .06), fungal infections (AOR: 1.51; 95% CI [0.55–4.16]; p = .42), and culture-negative episodes (AOR: 0.87; 95% CI [0.40–1.93]; p = .74) were not significantly associated with positive imaging findings. Among patients with imaging findings suggestive of enteric or secondary peritonitis, 39% required catheter removal during their hospitalization.
Multivariable logistic regression of imaging positive finding in enteric or other causes of PD-related peritonitis.
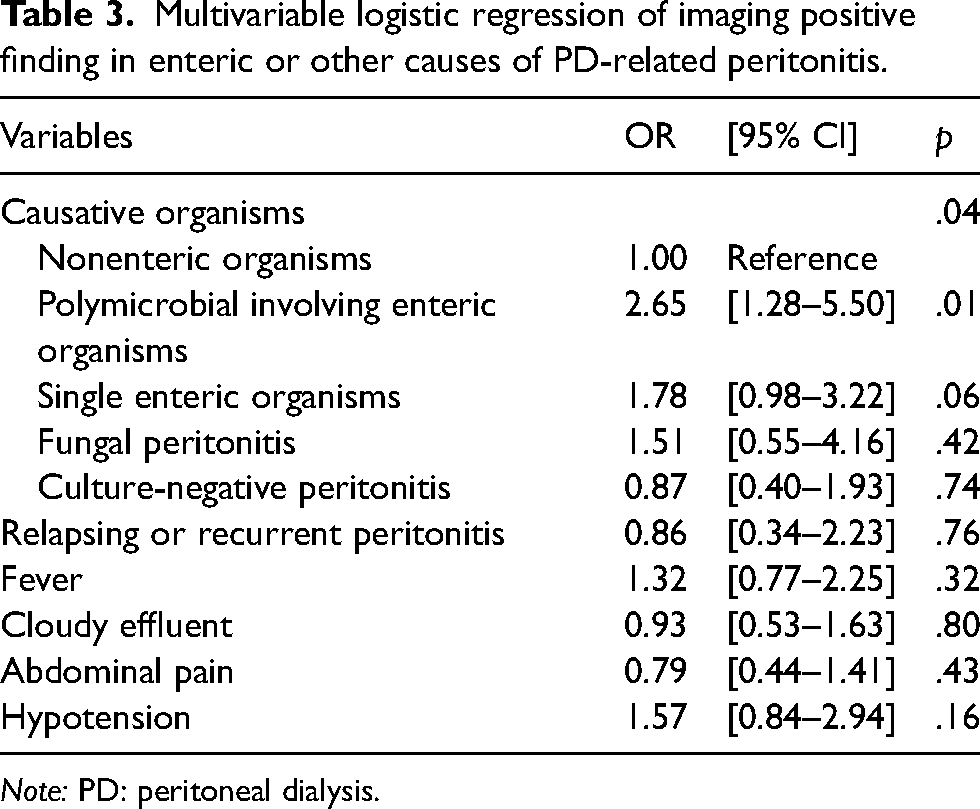
Note: PD: peritoneal dialysis.
Factors predicting critical imaging findings
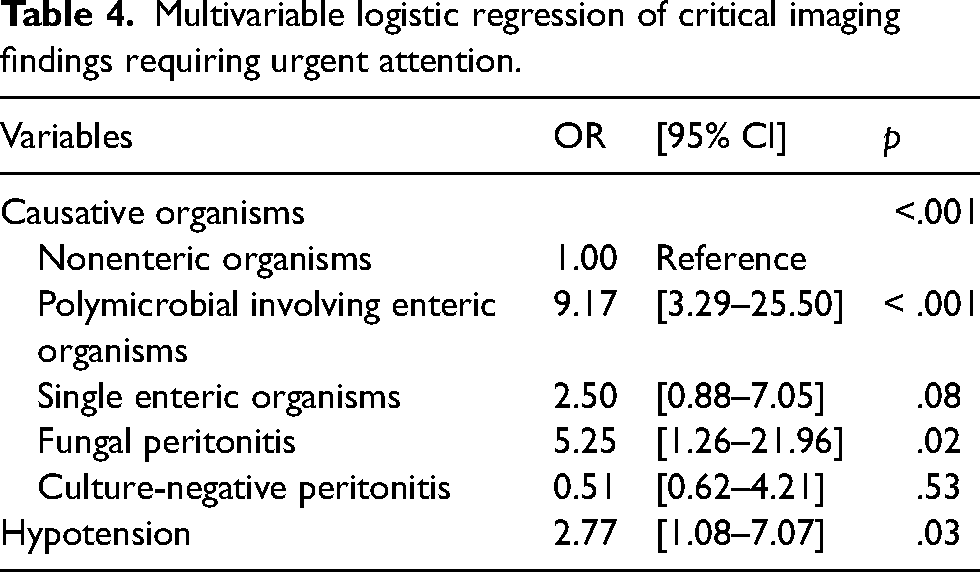
Enteric polymicrobial infections (AOR: 9.17; 95% CI [3.29–25.50]; p < .001), fungal infections (AOR: 5.25; 95% CI [1.26–21.96]; p = .02), and hypotension (AOR: 2.77; 95% CI [1.08–7.07]; p = .03) were significantly associated with critical imaging findings requiring urgent medical or surgical intervention (Table 4).
Multivariable logistic regression of critical imaging findings requiring urgent attention.
Discussion
Our study demonstrated that half of the peritonitis episodes underwent imaging. Imaging was significantly more common in peritonitis episodes caused by enteric (polymicrobial or single) organisms, and fungal organisms compared to nonenteric organisms. Additionally, clinical features such as hypotension, cloudy effluent at presentation, and laboratory findings of a higher effluent white cell count were significantly associated with a higher likelihood of undergoing imaging during peritonitis. Approximately half of the imaging studies showed no significant findings, while less than one-third of imaging revealed abnormalities. Among abnormal findings, colitis or enteritis was the most common. Critical findings requiring urgent medical or surgical attention were identified in 7.6% of imaging studies. Among the causative organisms, only polymicrobial enteric peritonitis showed a significant association with positive imaging findings suggestive of enteric or other secondary causes of peritonitis. When focusing specifically on critical imaging findings, a narrower and more severe subset (e.g. ischemic bowel, perforation, excluding colitis and enteritis), polymicrobial enteric infections, fungal peritonitis, and hypotension were all significantly associated.
Our study demonstrated that imaging was frequently overutilized in the evaluation of peritonitis in our cohort. The decision to order imaging was primarily influenced by the type of causative organism, particularly polymicrobial enteric (77.1%), single enteric organisms (60.9%) and fungal peritonitis (69.7%), driven by concerns regarding enteric or other intrabdominal pathology causing peritonitis and the need to identify a potential source. However, the present study demonstrated that only polymicrobial enteric organisms and fungal infections were significantly associated with enteric peritonitis or critical imaging findings. Therefore, routine use of imaging based solely on the presence of Gram-negative single organisms, nonenteric organisms, or polymicrobial infections—without distinguishing between enteric and nonenteric bacteria and without clinical judgment—should be avoided, as it may delay appropriate treatment and lead to unnecessary healthcare costs. Similarly, relying on clinical features such as fever, cloudy effluent at presentation, or rising effluent cell counts, which were not predictive of critical imaging findings in this study, is not recommended as the sole basis for imaging. Instead, features such as hemodynamic instability or physical examination findings suggestive of an acute abdomen, rather than abdominal pain alone, should prompt further investigations, including imaging.14,15
Our findings highlight polymicrobial including enteric organisms as a significant and independent predictor of positive imaging findings suggestive of secondary intra-abdominal pathology. This supports its role as a marker of complicated peritonitis and aligns with the 2022 ISPD Peritonitis Guidelines, which recommend a low threshold for imaging in patients with polymicrobial or enteric infections, especially when secondary causes are suspected. In contrast, peritonitis due to enteric single organisms, culture negative, or nonenteric organisms was not significantly linked to abnormal imaging findings. These findings suggest that not all enteric organisms carry equal risk for secondary pathology, and peritonitis episodes due to polymicrobial including enteric organisms may warrant greater diagnostic attention than single-organism enteric infections. 16
Our findings differ from those of Trinh and Bargman, who reported that polymicrobial or fungal infections did not predict the presence of radiologic abnormalities. 13 Our study builds on and extends their work by emphasizing the importance of more detailed microbial classification in predicting abnormal imaging findings. While Trinh et al. grouped all polymicrobial infections together, we differentiated between enteric and nonenteric sources. This approach revealed that only polymicrobial infections involving enteric organisms were significantly associated with imaging findings suggestive of enteric or secondary peritonitis. The difference in classification likely explains the differing results. In line with the study by Ribera Sánchez et al., which showed worse clinical outcomes such as higher rates of hospitalization, surgical intervention, treatment failure, and mortality in patients with polymicrobial enteric peritonitis compared with single organism enteric peritonitis, 16 our study also found that only polymicrobial enteric infections were significantly associated with abnormal imaging findings, whereas single organism enteric infections were not.
In our study, fungal peritonitis was significantly associated with critical imaging findings. Imaging should be considered in PD patients with fungal peritonitis when clinically appropriate, particularly in the presence of features suggestive of a surgical abdomen. The ISPD Peritonitis Guidelines recommend prompt catheter removal in cases of fungal peritonitis due to its high morbidity and mortality. 7 While imaging may assist the surgical team in determining the need for additional intervention alongside catheter removal, it should not delay the initiation of timely treatment.
Our study found that relapsing and/or recurrent peritonitis episodes were not significantly associated with the likelihood of undergoing imaging. This contrasts with the findings of Trinh and Bargman, who reported higher imaging rates in relapsing, recurrent, and refractory episodes. 13 The discrepancy may be attributed to differences in episode classification: their analysis grouped refractory, relapsing, and recurrent episodes together, while our study examined relapsing and recurrent episodes separately. Refractory peritonitis, by contrast, often raises concern for ongoing intra-abdominal pathology, prompting more frequent use of imaging. These differences in clinical context and classification may account for the lower imaging rates observed in relapsing and/or recurrent peritonitis in our study.
In the study by Trinh et al., hypotension was not found to be associated with abnormal imaging findings, although ICU admission was associated with abnormal results. 13 In contrast, our study showed that hypotension predicted critical imaging findings, with the majority of patients with hypotension (86%) undergoing abdominal imaging. The differing results between the two studies may attributed to differences in patient selection, classification of hypotension severity, or timing of imaging in relation to the onset of hypotension. Hypotension in peritonitis can result from septic shock due to an acute surgical abdomen or from hypovolemia related to poor oral intake, ongoing ultrafiltration from dialysis, or antihypertensive use. Therefore, the decision to perform imaging should be guided by a thorough clinical assessment, including history-taking, a review of PD records, and physical examination, rather than relying solely on the presence of hypotension.
Our results highlight the need for a more selective approach to imaging in PD peritonitis. While imaging is essential for detecting intra-abdominal complications, the high proportion of negative imaging findings suggests that clinical judgment should guide its use rather than routine imaging. Focusing on severe clinical presentations, hemodynamic instability, or clinical suspicion of intra-abdominal pathology will prompt clinicians to evaluate for intraabdominal pathology.14,15 Unnecessary imaging in PD patients presenting with symptoms of suspected peritonitis not only exposes them to radiation, intravenous contrast agents, and additional costs but also delays the initiation of appropriate treatment.17,18 Treatment of peritonitis should begin promptly once it is suspected, and the administration of antibiotics should not be postponed for imaging studies. Delays in initiating antibiotics have been associated with poor outcomes, including treatment failure, transfer to HD, and even mortality. A study by Muthucumarana et al. further reported that imaging performed within 24 h of presentation increased the median time to starting antibiotics, underscoring the importance of prioritizing timely treatment over unnecessary imaging. 19
This is one of the very few studies that examine the role of imaging of the abdomen during peritonitis in PD patients. Strengths of our study include a relatively large sample size and a comprehensive analysis of imaging findings, microbiological patterns, and clinical predictors in PD peritonitis. In particular, the study provides valuable insights into enteric and critical PD peritonitis, which are clinically important but underreported in the literature. However, this study has several limitations. First, it was a single-center, retrospective observational study, which may be subject to recall bias. Second, the study lacked granular information on key clinical details, including: who ordered the imaging (nephrologists versus emergency physicians), the specific reasons for imaging, the exact timing of imaging, the patients’ location at the time of presentation and imaging (emergency department vs inpatient wards), detailed findings from abdominal physical examinations, and whether patients required intensive care unit admission during their episode of peritonitis. Third, serum lactate levels, which may have influenced decisions regarding imaging as reported in previous study were not available in our study. Fourth, detailed information on antibiotic treatment regimens and the antimicrobial sensitivity of the causative organisms was not available. Finally, abnormal findings such as colitis or ileus may not clearly distinguish whether they are the cause or the consequence of peritonitis. Therefore, these abnormal findings may have limited utility in guiding patient management.
Based on the findings from the present study, we propose a clinical decision-making framework to guide the use of abdominal imaging in PD peritonitis. Imaging should be considered in patients with clinical features suggestive of secondary or intra-abdominal pathology, such as hemodynamic instability (e.g. hypotension), or peritonitis caused by polymicrobial involving enteric bacteria or fungi. In contrast, routine imaging is not recommended for peritonitis episodes caused by single-organism enteric bacteria, nonenteric bacteria (including polymicrobial nonenteric infections), or culture negative episodes. This approach aims to help clinicians balance benefits and risks, minimize unnecessary treatment delays, and reduce patients’ exposure to radiation and contrast agents, as well as healthcare costs.
In conclusion, diagnostic abdominal imaging was commonly performed in patients with PD peritonitis. Importantly, our study found that polymicrobial involving enteric organisms were predictive of enteric or intra-abdominal imaging findings. Polymicrobial infection involving enteric bacteria, fungi, and presence of hypotension were significantly associated with critical imaging findings. Further research is needed to refine clinical and laboratory criteria that can guide imaging decisions more effectively. Additionally, prospective studies evaluating the impact of imaging on patient outcomes, including treatment modifications and prognosis, would be valuable in optimizing PD peritonitis management.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608251383992 - Supplemental material for Factors influencing diagnostic imaging in peritoneal dialysis-associated peritonitis
Supplemental material, sj-docx-1-ptd-10.1177_08968608251383992 for Factors influencing diagnostic imaging in peritoneal dialysis-associated peritonitis by Khin Zar Li Lwin, Marjorie Wai Yin Foo, Mathini Jayaballa, Elizabeth Ley Oei, Chieh Suai Tan, Angela Yee Moon Wang and Htay Htay in Peritoneal Dialysis International
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions of clinicians and PD nurses from the PD unit at Singapore General Hospital.
Author contributions
K.Z.L. Lwin, M.W.Y. Foo, M.J., E.L. Oei, C.S. Tan, A.Y.M. Wang, and H. Htay contributed to the concept of the study; H. Htay and K.Z.L. Lwin analyzed and interpreted the data; K.Z.L. Lwin drafted the manuscript, with critical input and review by H. Htay; M.W.Y. Foo, A.Y.M.Wang, and C.S. Tan reviewed the manuscript for important intellectual content. All authors reviewed and approved the version to be published.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted as a clinical audit and was exempted from the ethical review by the SingHealth CRIB.
Funding
Htay Htay has received consultancy fees, speaker's honoraria and travel sponsorships from Baxter Healthcare and consultancy fees and travel sponsorships from AWAK Technologies, speaker's honoraria from Fresenius Medical Care, grants from Johnson & Johnson Company, grants from Singhealth NIG, outside the submitted work. Marjorie WY Foo has received grants from National Medical Research Council for the study; consultancy fees and speaker's honoraria and travel sponsorships from Baxter Healthcare, and consultancy fees and travel sponsorships from AWAK Technologies. Angela Yee-Moon Wang has received speaker's honoraria from Fresenius Kabi, Astra Zeneca, and Bayer and also consultancy fees from Fresenius Kabi, and has received grants from National Medical Research Council. The other authors have nothing to disclose.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.