
Abstract
Background and objectives
Iron plays a critical role beyond erythropoiesis, yet the prognostic significance of iron deficiency (ID) independent of anemia remains poorly defined in the peritoneal dialysis (PD) population. This study aimed to evaluate the association between iron status, specifically transferrin saturation (TSAT), and mortality in PD patients, independent of hemoglobin levels.
Design, setting, participants, and measurements
We conducted a retrospective cohort study of 11,013 adults who initiated PD at a large US dialysis network between December 2004 and January 2011. Patients had at least 180 days on PD and baseline data on TSAT, ferritin, hemoglobin, albumin, and white blood cell count. The primary outcome was all-cause mortality. Broadly adjusted associations between iron parameters and mortality were assessed using Cox proportional hazards models and restricted cubic splines, with adjustments for demographic, clinical, treatment-related, and laboratory variables including hemoglobin and ESA use.
Results
Iron deficiency, defined as TSAT ≤20%, was present in 10% of patients at PD initiation. The cohort was 54% male and 70% Caucasian, with a mean age of 55 years; 39% had diabetes. While 91% received erythropoiesis-stimulating agents, only 34% received IV iron. After comprehensive adjustment, TSAT ≤20% remained independently associated with increased mortality (adjusted HR: 1.26; 95% CI: 1.12–1.42). Spline analyses showed a sharp rise in mortality risk at TSAT levels below 25%. Ferritin was inconsistently associated with mortality risk. During follow-up, 2704 deaths occurred (24.6% of the cohort) over a median 440-day follow-up.
Conclusions
Iron deficiency is common in incident PD patients and is associated with increased mortality risk, independent of anemia. These findings challenge current anemia-centric treatment paradigms and suggest that iron status, particularly TSAT, should be routinely assessed in PD patients regardless of hemoglobin levels. A prospective, randomized trial is warranted to evaluate whether proactive iron management improves outcomes in this population.
Introduction
Beyond its established role in erythropoiesis, iron is essential for a wide array of physiological processes, including mitochondrial function, oxidative metabolism, immune response, and cardiovascular health.1–3 While prior studies have demonstrated that low iron stores are associated with adverse outcomes in non-dialysis CKD and hemodialysis populations even in the absence of anemia,3–5 evidence in the peritoneal dialysis (PD) population remains sparse and underdeveloped.
PD patients face unique challenges in anemia and iron management. Reduced clinical contact limits opportunities for routine monitoring and administration of intravenous (IV) iron, making oral iron a more common but often less effective alternative. Current treatment guidelines remain largely anchored in hemoglobin thresholds, potentially overlooking patients with iron deficiency who are not anemic and leading to reliance on oral iron, which is often less effective.3,8 Furthermore, prior studies in PD populations have been constrained by small sample sizes, limited statistical power, and inadequate adjustment for confounding factors such as ESA use, comorbidities, and laboratory markers including hemoglobin levels.6,7
Treatment benefits have been demonstrated in heart failure and hemodialysis populations and extend beyond erythropoiesis alone. However, the clinical significance of iron deficiency in peritoneal dialysis remains largely undefined.1,2
This study offers a novel perspective by disentangling the effects of iron deficiency from anemia in a large, contemporary cohort of incident PD patients. It aims to fill a critical gap by evaluating the prognostic significance of iron deficiency, independent of anemia, during the early and vulnerable phase of PD initiation. We hypothesize that low TSAT, a key marker of iron status, is associated with increased mortality risk regardless of hemoglobin levels. In doing so, we seek to challenge the prevailing anemia-centric paradigm of iron therapy and provide evidence that iron deficiency in PD warrants clinical attention even when hemoglobin levels appear adequate.
Methods
Patient sample
Our study used real-world data from adult kidney failure patients who received PD at a dialysis provider network (Fresenius Medical Care, Waltham, MA) between 01 Dec 2004 and 31 Jan 2011. We included incident peritoneal dialysis patients who remained on PD for at least 180 days with at least one measurement for TSAT, ferritin, and hemoglobin during this period.
Ethical considerations
Data captured during routine dialysis care at a clinic network in the United States was de-identified for research purposes. Analysis was performed under a protocol approved by New England Independent Review Board (Needham Heights, MA; NEIRB# 17-1334030-1). A waiver of informed consent was provided, and analysis was conducted in accordance with title 45 of the United States Code of Federal Regulations part 46.116(f), and the Declaration of Helsinki.
Outcome
Our primary outcome for this study was all-cause mortality. The cohort included incident PD patients, and the time-at-risk for mortality events was defined as any death that occurred after the first 6 months (180 days) of PD initiation. Patients were censored when any of the following events occurred after baseline: PD technique failure or loss to follow-up.
Exposure
TSAT was defined as the primary exposure variable and was assessed during the first 180 days following PD initiation. If multiple TSAT values were available during this period, values were averaged to estimate iron stores during early PD. Patients were categorized into five TSAT groups: ≤20%, >20% to ≤30% (reference group), >30% to ≤40%, >40% to ≤50% and >50%. Covariates for model adjustment were selected a priori and included demographics, comorbidities, laboratory values, and medication use. Consistent with TSAT values, other laboratory parameters with more than one measurement within the first 3 months were averaged. Non-iron laboratory covariates were averaged over 90 days to reduce the likelihood of adjusting for mediator pathways. TSAT and ferritin, the primary exposures, were averaged over the full 180-day window to improve measurement reliability.
TSAT categories were chosen based on clinical practice patterns and prior studies of iron deficiency in CKD and dialysis populations. 8 While KDIGO anemia guidelines 7 do not define discrete TSAT categories, they support iron supplementation when TSAT is <30%, which informed the selection of the reference and deficiency thresholds used in this analysis.
Ferritin values and IV iron administration in the form of iron sucrose (IV Venofer) were both captured during the 6-month baseline period. However, the timing of laboratory measurement relative to iron dosing was not standardized and may have varied across patients.
A sub-analysis was conducted on the overall cohort to explore the relationship between IV iron administration and iron biomarkers. TSAT and ferritin were treated as continuous variables, using the average values from the first 180 days of PD, and IV iron exposure was defined as cumulative dose received during the same period. To visualize and analyze potential non-linear associations between iron biomarkers and IV iron dosing, we employed restricted cubic splines.
Statistical analysis
Descriptive statistics were computed to describe patient characteristics for the overall cohort, as well as by TSAT level. Categorical data were shown in numbers and proportions, and continuous data were tabulated showing mean and standard deviations.
To estimate the association between iron deficiency and all-cause mortality, we used a series of Cox proportional hazard models adjusted in a cumulative stepwise manner for multiple confounders. The first model (Model A) was not adjusted for any covariates. Model B adjusted for demographic parameters: age at dialysis initiation, sex, race (Caucasian vs. non-Caucasian), dialysis vintage, and history of hemodialysis prior to PD initiation. Model C added comorbidities to Model B: gastrointestinal bleeding, peripheral vascular disease, hypertension, cardiovascular disease, cerebrovascular disease, heart failure, acute myocardial infarction, diabetes mellitus, and cancer. Model D adjusted for medications: ESA and IV iron dosing. ESA dose is shown in epoetin alpha equivalents, with any darbepoetin doses being converted using 1:200 darbepoetin to epoetin ratio. 10 Iron medications were limited to those given via intravenous formulations. Model E further adjusted for laboratory values including albumin, ferritin, and white blood cell (WBC) count. The final model (F) adjusted for hemoglobin in addition to all covariates from the preceding models.
PD-specific variables such as residual kidney function, peritoneal Kt/V, urine volume, dialysate characteristics, and peritoneal membrane transport status were not available for most patients and were not included due to substantial missingness.
We conducted a comprehensive analysis of iron parameters in peritoneal dialysis patients using Cox proportional hazards models with splines to investigate the associations between both TSAT and ferritin levels with mortality risk. We modeled TSAT as a continuous variable using restricted cubic splines with 4 degrees of freedom. Knots were placed at 20% and 30%, with boundary knots at 0% and 50%. These values were chosen based on clinical relevance and confirmed to fall within the core distribution of observed TSAT values. Ferritin was modeled as a continuous variable using restricted cubic splines with 4 degrees of freedom. Knots were placed at 100, 200, and 500 ng/mL, consistent with clinical thresholds used in the management of iron deficiency in dialysis populations. 11 Boundary knots were set at 0 and 2000 ng/mL to capture the majority of the observed distribution while reducing the influence of extreme values. This method allowed for a more flexible assessment of potential non-linear associations between iron biomarkers and mortality risk, without assuming a strictly linear effect or relying on pre-specified categories. Ferritin spline estimates at very low levels should be interpreted with caution due to sparse observations and boundary-knot behavior. Both models adjusted for a wide range of demographic and clinical covariates, including age, sex, race, dialysis modality, comorbidities, and other laboratory values. We generated predictions across the respective ranges of TSAT (4–50%) and ferritin (0–2000 ng/mL) values, while holding other variables constant at their median or most frequent values. The results were visualized using plots of the predicted hazard ratios with 95% confidence intervals, to highlight how mortality risk changes with TSAT and ferritin levels independently, capturing potential non-linear relationships without imposing predetermined functional forms.
Analyses were conducted using SAS software, version 9.4 (SAS Institute, Cary, NC). Kaplan-Meier plots were created using the survival package (v3.2-7; Therneau, 2020). Forest plots were generated with R version 4.2.2 and ggplot2 package (v3.3.3; Wickham, 2016).
Time-to-event modeling
We used cause-specific Cox proportional hazards models to estimate the association between TSAT categories and all-cause mortality. Death was the event of interest. Patients were censored at the time of kidney transplantation, permanent transfer to hemodialysis, whichever occurred first. Although competing events were not modeled explicitly, they were examined descriptively, and their frequencies were similar across TSAT strata, reducing concern for informative censoring.
Results
Patient characteristics
Among 16,495 adults who initiated PD in the network, 30% (n = 4913) were not included since they discontinued PD in the initial 180 days of treatment (e.g., transplant, died, left the clinic network), and 3% (n = 569) were excluded due to missing laboratory data during the initial observation period. The final study cohort included 11,013 patients.
Patients were 54% male and 70% Caucasian, with a mean age of 55 years at dialysis initiation. PD was the first dialysis modality in 54% of patients. During the first 180 days of PD, mean hemoglobin was 12.1 g/dL, TSAT was 31%, ferritin was 445.7 ng/mL, and albumin was 3.6 g/dL. ESA was administered to 91% of patients during the initial 180-day period, while 34% received IV iron. Among those who received these therapies, the mean weekly epoetin and IV iron doses were 3488 IU/week and 61.6 mg/week, respectively. Nearly all patients who received an ESA were prescribed epoetin; <1% (n = 31) received darbepoetin alfa.
Table 1 displays baseline characteristics by TSAT level and Table 2 by IV iron dosing status. Patients who received IV iron had lower mean TSAT (28.6% vs. 32.5%) and ferritin (392 ng/mL vs. 473 ng/mL) levels compared to those who did not receive IV iron. The prevalence of comorbid conditions such as diabetes, cardiovascular disease, and hypertension was slightly higher among those who received IV iron. The overall mortality rate in the cohort was 24.6% and was lower in the IV iron group (21.7%) compared to the non–IV iron group (26.0%).
Patient characteristics overall and by TSAT achievement in the first 180 days of PD.
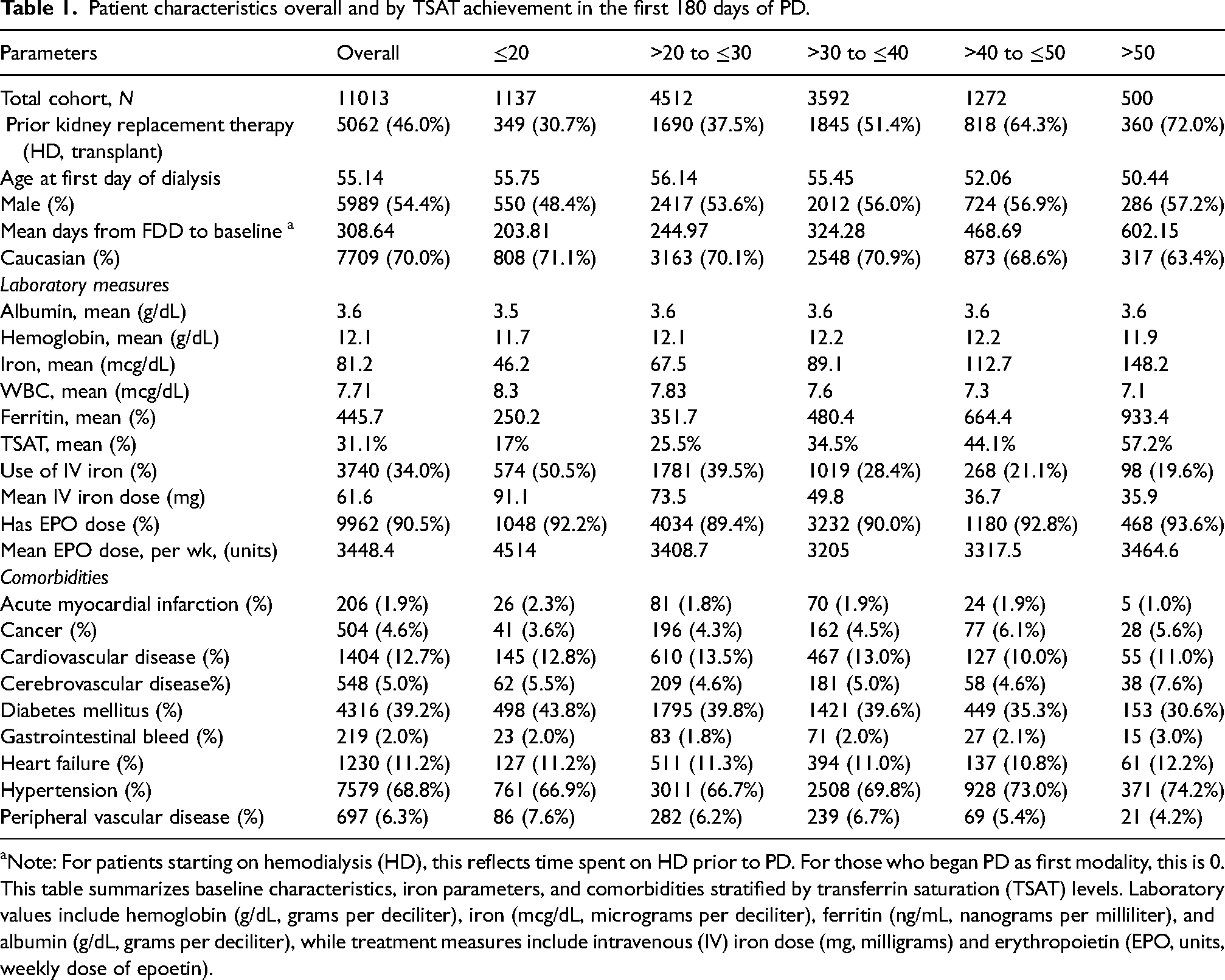
Note: For patients starting on hemodialysis (HD), this reflects time spent on HD prior to PD. For those who began PD as first modality, this is 0.
This table summarizes baseline characteristics, iron parameters, and comorbidities stratified by transferrin saturation (TSAT) levels. Laboratory values include hemoglobin (g/dL, grams per deciliter), iron (mcg/dL, micrograms per deciliter), ferritin (ng/mL, nanograms per milliliter), and albumin (g/dL, grams per deciliter), while treatment measures include intravenous (IV) iron dose (mg, milligrams) and erythropoietin (EPO, units, weekly dose of epoetin).
Crude mortality rate by TSAT achievement in the first 180 days of PD.

Crude mortality rate and survival time by baseline iron stores
During follow-up, 2704 deaths occurred, yielding an overall mortality rate of 24.6%. Table 3 shows crude mortality rates by baseline TSAT levels among 11,013 peritoneal dialysis (PD) patients, following the initial 180-day period. The cohort is divided into five TSAT categories: ≤20% (n = 1137), >20% to ≤30% (n = 4512), >30% to ≤40% (n = 3592), >40% to ≤50% (n = 1272), and >50% (n = 500). The highest mortality was observed in those having TSAT values of ≤20% (31.2% died, n = 355), with a death rate of 195.8 per 1000 Patient-Year (PY).
Crude mortality rate by IV iron dose in the first 180 days of PD.
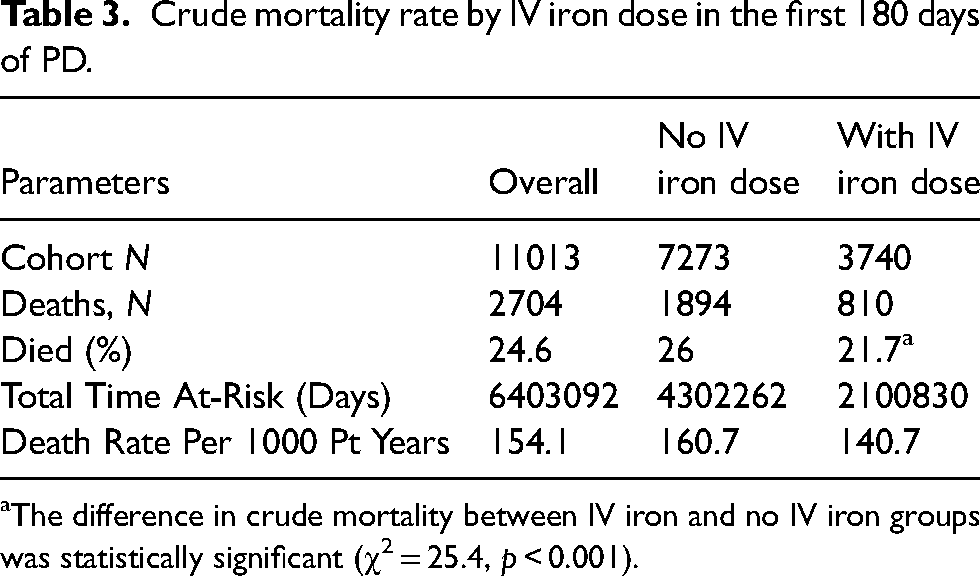
The difference in crude mortality between IV iron and no IV iron groups was statistically significant (χ2 = 25.4, p < 0.001).
Those achieving TSAT levels in the >40% to ≤50% range had a 21.3% crude mortality (n = 271), with an adjusted death rate of 142.3 per 1000 PY. The median follow-up time was 440 days (IQR: 184–865), with a total of 403,092 person-days at risk, distributed across TSAT categories.
For time-to-event analyses, follow-up began immediately after the 180-day exposure assessment window. During this analytic period, 354 deaths were observed. All remaining patients were censored because of kidney transplantation (n = 416), permanent transfer to hemodialysis (n = 2722), or administrative end of study (n = 7521). Descriptive competing-risk counts by TSAT category are provided in Supplemental Table 2.
Crude mortality rate and survival time IV iron dosing
Among patients who did not receive IV iron, the mortality rate was higher at 26.0% (death rate: 160.7 per 1000 PY) after the 180-day baseline period. While crude mortality was lower among patients who received IV iron (21.7% vs. 26.0%), this unadjusted difference should be interpreted with caution given the potential for confounding (death rate: 140.7 per 1000 PY). The total time at risk was 6,403,092 days for the entire cohort, with 4,302,262 days for those not receiving IV iron and 2,100,830 days for those who did (Table 4).
Kaplan–Meier survival curves based on achieved TSAT levels
Patients with TSAT between 40% and 50% exhibited the greatest median survival probability, reaching approximately 1900 days. Individuals in the >20% to ≤30%, >30% to ≤40%, and >50% TSAT groups had a 50% survival probability between 1600 and 1700 days. Notably, those with TSAT ≤20% had a significantly shorter survival, dying on average about 500 days earlier than the rest of the cohort. Figure 1 shows the Kaplan–Meier survival curves for the different TSAT categories. Of the 11,013 patients, 1137 (10.3%) had TSAT ≤20%, meeting criteria for iron deficiency.
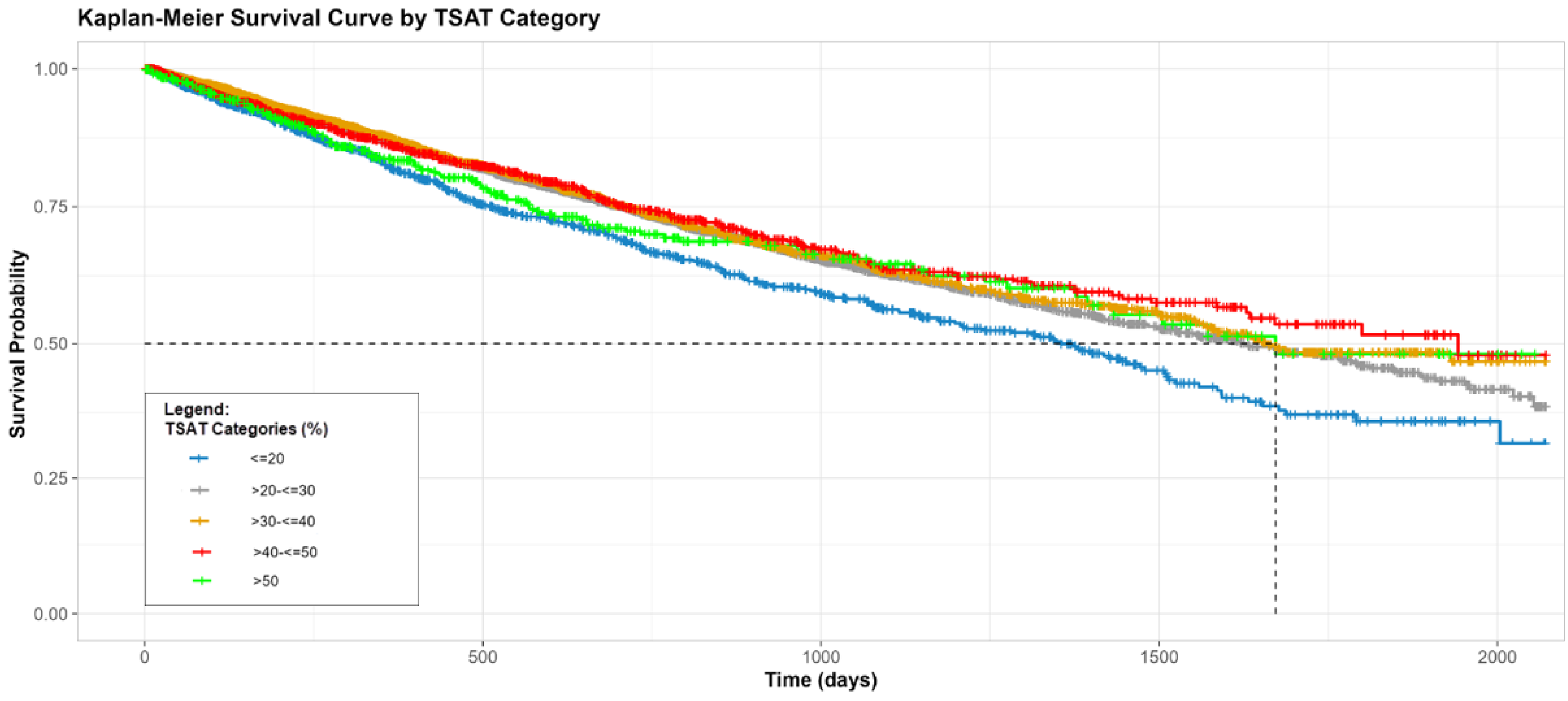
Survival in PD by TSAT level at PD start.
Mortality risk by baseline iron stores in the first 180 days of PD
Stepwise assessment of mortality risk was evaluated and is shown in Figure 2. TSAT ≤20% was consistently associated with higher mortality across all models, including after adjustment for hemoglobin (Model F: HR 1.22, 95% CI: 1.08–1.37, p = 0.0015). The persistence of this association despite adjustment for hemoglobin supports the hypothesis that iron deficiency confers mortality risk independent of anemia. Notably, the >30% to ≤40% TSAT group showed a potential protective association in some models (e.g., Model E), though this association was slightly reduced and no longer statistically significant after adjustment for hemoglobin in Model F (Table 5). Overall, patients with a TSAT ≤20% consistently had an increased risk of death after adjusting for all covariates.
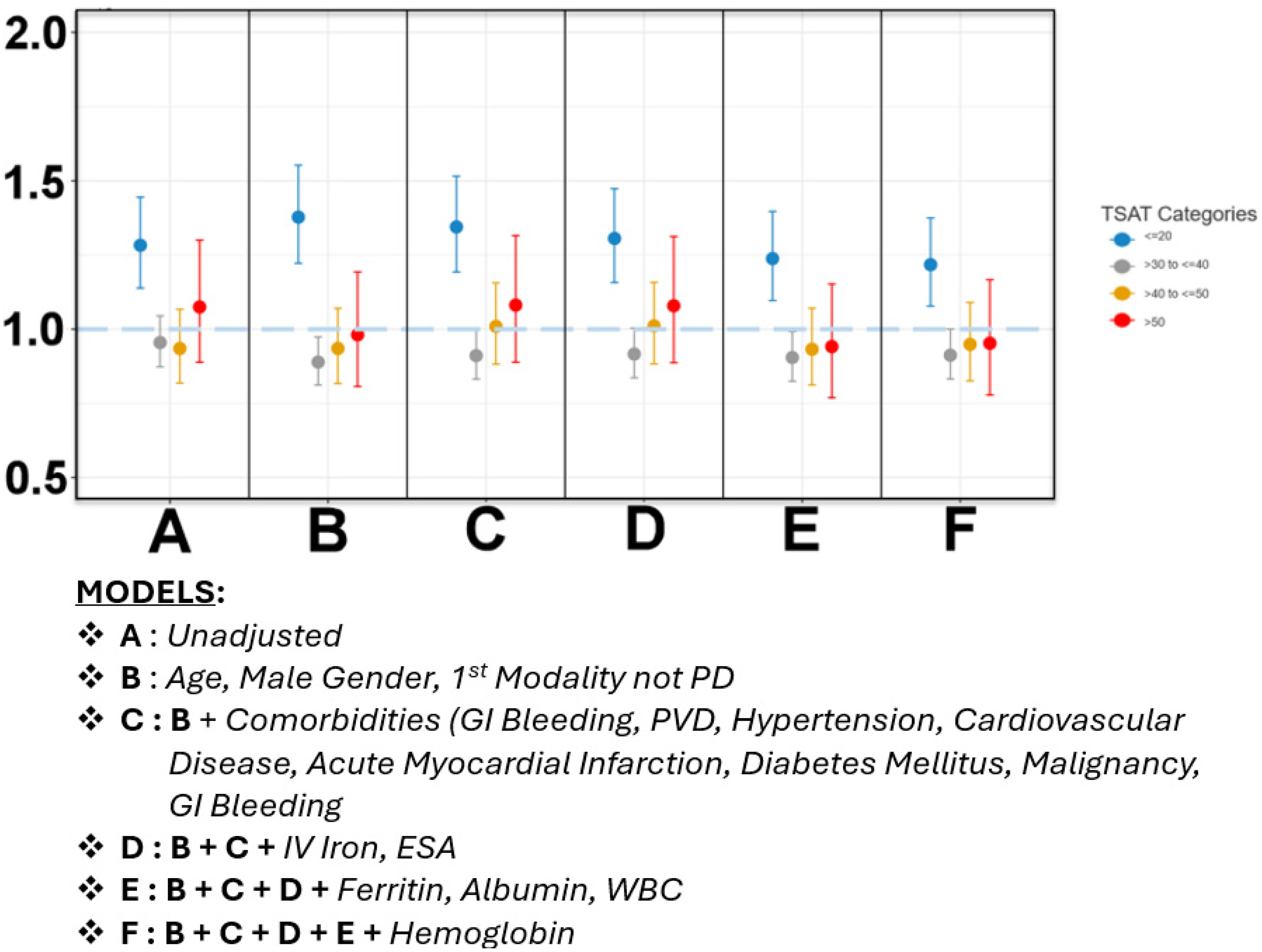
Mortality risk by TSAT level at PD start.
Spline-Adjusted mortality risk across continuous TSAT levels
We analyzed TSAT as a continuous variable using restricted cubic splines (Figure 3). The confidence intervals show an increasing risk of death at lower TSAT levels, particularly below 25%. In the subgroup of patients who did not receive IV iron, a similar pattern was observed, with higher mortality risk associated with TSAT levels <26% (Figure 4). Among those who received IV iron, the spline curve did not show a clear inflection point, and confidence intervals were wide, limiting the ability to draw definitive conclusions in this subgroup (Figure 5).
Spline-adjusted mortality risk across continuous ferritin levels
Ferritin exhibits a dynamic relationship with death, where higher levels are associated with increased mortality risk (Figure 6). Stratifying by IV iron treatment, we found that higher ferritin levels correlate with an elevated risk of death in the overall cohort (Figure 7). While spline modeling suggested lower predicted risk at ferritin values near zero, this represents model behavior at the boundary rather than a clinically meaningful inflection.
Among patients who received IV iron, there was no increase in mortality risk associated with higher ferritin levels during the baseline period (Figure 8). While this may suggest a potential modifying effect of IV iron, interpretation is limited by the lack of standardized timing between iron administration and ferritin measurement.
Discussion
In this large, contemporary cohort of incident PD patients, we demonstrate that low TSAT(≤20%) is a strong and independent predictor of all-cause mortality. This association persisted even after adjusting for hemoglobin and other key covariates, reinforcing the hypothesis that iron deficiency has prognostic implications beyond its role in facilitating erythropoiesis. These findings add to a growing body of literature suggesting that iron deficiency may affect patient outcomes via mechanisms unrelated to anemia, such as impaired mitochondrial function, reduced oxidative metabolism, immune dysregulation, and cardiac and muscle function.1–3,9,13–15
Our study makes several unique contributions. First, we address a major gap in PD literature by evaluating iron status independent of anemia in a well-characterized cohort, by far the largest cohort addressing this topic. Most prior studies in PD have either focused exclusively on anemia management or were constrained by limited sample sizes and insufficient adjustment for confounders.4,5,8 Second, by concentrating on TSAT, a dynamic and functionally relevant biomarker of circulating iron; we offer a more clinically actionable perspective than studies relying solely on ferritin, which is often confounded by inflammation.17–19 Third, we evaluate iron status during the early phase of PD. This period is a critical and underrepresented window of vulnerability where iron deficiency is highly prevalent, reinforcing the role of an early and proactive intervention with potential impact on improving outcomes.
Despite 91% of patients receiving erythropoiesis-stimulating agents (ESAs), only one-third received IV iron, and over 10% were iron-deficient at baseline. Notably, the average hemoglobin in the TSAT ≤20% group was 11.7 g/dL, which is above guideline-based anemia thresholds. This indicates that many iron-deficient patients were not anemic and therefore unlikely to be recognized under hemoglobin-centered treatment protocols. These findings support the need to consider iron status independently of hemoglobin in PD management.
This finding further suggests that iron-deficient PD patients may be systematically overlooked and undertreated using current protocols that prioritize hemoglobin levels over iron status. Our results support a reevaluation of this paradigm and argue for broader consideration of iron supplementation strategies in PD patients regardless of anemia.
The prognostic value of TSAT independent of hemoglobin echoes findings in non-dialysis CKD and heart failure populations, where iron deficiency has been associated with reduced quality of life, increased hospitalizations, and higher mortality—even in the absence of anemia.1,2,12,13,14 Taken together with prior studies in nondialysis CKD and heart failure, these findings reinforce the broader systemic implications of iron deficiency. These parallels highlight a broader physiological role for iron that extends beyond red blood cell production, reinforcing the need to reassess iron management strategies in PD through a more systemic lens.
To our knowledge, this is the largest study to date evaluating iron status in incident PD patients with rigorous adjustment for confounding, including hemoglobin and ESA use. While previous PD studies such as AIM-PD 4 and the work by Luo et al. 5 have identified associations between abnormal iron markers and outcomes, they lacked sufficient power, comprehensive adjustment, and a focus on iron deficiency independent of anemia. Moreover, none have explored these relationships with the granularity afforded by spline modeling, which revealed a clear inflection in mortality risk below TSAT 25%, further validating the prognostic threshold used in our categorical analysis.
Our observational findings may complement those of the PIVOTAL trial in hemodialysis, 12 which demonstrated improved outcomes with proactive IV iron therapy, even among patients with ferritin and TSAT levels traditionally considered adequate. Although PD patients were not included in PIVOTAL, our results suggest that similar benefits may extend to this population, supporting the need to explore proactive iron management in PD, particularly for patients who do not meet conventional anemia criteria. Confirming this hypothesis will require a prospective, randomized trial specifically designed for the PD setting. Translating proactive iron management into PD practice, however, presents unique challenges. Addressing these barriers may also yield economic benefits by reducing ESA use, preventable hospital encounters, and the broader costs of undertreated iron deficiency.
Beyond clinical implications, our findings are biologically plausible. Iron is indispensable for mitochondrial ATP generation, muscle function, and tissue oxygen utilization. Preclinical and clinical data across various chronic disease states, such as heart failure, inflammatory bowel disease, and CKD, support these mechanisms and show benefit from iron repletion independent of changes in hemoglobin.14–16,18,19 In PD, where logistical barriers to IV iron administration persist, newer oral agents and HIF-PHIs may provide feasible alternatives that warrant further investigation.
Interestingly, we also observed a lower crude mortality rate in patients who received IV iron during the first 180 days of PD, despite their greater comorbidity burden and lower baseline TSAT. Although limited by confounding, the lower crude mortality observed among IV iron recipients, despite greater comorbidity burden, raises the hypothesis that early iron repletion may offer clinical benefit in PD. Future prospective studies should evaluate whether proactively delivered iron supplementation, independent of hemoglobin levels, can improve outcomes in PD.
Because technique failure and transplant may occur non-randomly with respect to illness severity, misclassification is possible if patients experienced a clinical decline prompting modality switch before death. However, competing events were distributed similarly across TSAT categories (Supplemental Table 2), making substantial differential bias unlikely.
Our study has several limitations. The retrospective design precludes definitive causal inference, and residual confounding remains possible. The study timeframe investigated was dated, but was selected to capture anemia management in times before ESA targets were lowered, and IV iron use may have been increased. We lacked data on oral iron use and the precise timing of ferritin or TSAT measurements relative to IV iron administration. These factors may have influenced iron status classification. Additionally, approximately one-third of the original PD cohort was excluded due to early technique failure or missing data. While necessary for ensuring reliable exposure assessment and time-at-risk, this exclusion may have introduced selection bias. Patients who died within the 180-day baseline window were excluded because TSAT and ferritin could not be reliably assessed during this period. This design choice was necessary to avoid misclassifying early deaths due to incomplete or absent iron measurements. However, because cohort entry required surviving to the end of the 180-day baseline window, this approach may preferentially exclude the sickest patients and introduce the possibility of survivor bias.
We were unable to adjust for several PD-specific factors: residual kidney function, dialysate characteristics, and peritoneal membrane transport status. These variables were not consistently captured in the dataset. Residual kidney function, in particular, is a strong prognostic factor in PD, and its absence represents an important limitation of our analysis. Information on oral iron use, inflammatory markers such as CRP, and broader nutritional indicators was incomplete. Residual confounding is possible, therefore, and should be addressed in future prospective studies.
We did not perform hemoglobin-stratified or time-varying analyses because hemoglobin lies on the causal pathway between iron status and outcomes, and treatment exposures (ESA and IV iron) were recorded at the prescription level rather than at the level of actual administration timing, making time-dependent modeling unreliable.
Our study reflects practice patterns from 2004 to 2011, an era characterized by higher ESA dosing targets, more variable IV iron use, and continued use of acidic lactate-based dialysate in some regions. These differences may influence absolute treatment patterns; however, the underlying pathophysiology of iron deficiency and its relevance to mortality risk have remained consistent over time. Importantly, variation in anemia and iron management continues to persist in modern PD care, making these historical data still informative for understanding the clinical implications of iron deficiency in this population.
Nonetheless, the large sample size of this study, its focus on incident PD patients, comprehensive covariate adjustment, and rigorous analytic approach all enhance the validity and relevance of our findings. The clear and consistent association between iron deficiency and mortality, independent of anemia, highlights a missed opportunity in current PD management.
Conclusion
Iron deficiency is both common and prognostically significant in PD patients, even without anemia. Our findings challenge traditional anemia-focused treatment strategies and support broader iron monitoring and supplementation approaches tailored to the unique context of PD. These results highlight the need to reconsider when and how iron deficiency is managed in this population and lay the groundwork for future interventional trials. They also underscore the need for updated guidelines that recognize iron status as an independent treatment target in PD.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608251412935 - Supplemental material for Anemia-independent prognostic value of iron deficiency in incident peritoneal dialysis patients
Supplemental material, sj-docx-1-ptd-10.1177_08968608251412935 for Anemia-independent prognostic value of iron deficiency in incident peritoneal dialysis patients by Vladimir Rigodon, Murilo Guedes, Peter G Pecoits, Brianna Hartley, Yue Jiao, Len A Usvyat, Dinesh K Chatoth, Jeffrey L Hymes, Franklin W Maddux, Jeroen Kooman, Thyago P Moraes, Jochen G Raimann, Peter Kotanko, John W Larkin, Roberto Pecoits-Filho and On behalf of the MONDO Investigators in Peritoneal Dialysis International
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DC is an employee of Fresenius Medical Care and owns stock in the company. DC's spouse owns shares in Amgen. DC is a member of the ASN Peritoneal Dialysis (PD) Workgroup and the US Advisory Panel for PDOPPS.
FWM is an employee of Fresenius Medical Care and owns stock in the company.
JR is an employee of Fresenius Medical Care and holds shares of stock in the company. JR also serves on the Board of Directors of Easy Water for Everyone, a 501(c) 3 organization.
JWL is an employee of the Renal Research Institute LLC, a wholly owned subsidiary of Fresenius Medical Care Holdings Inc. JWL holds share options/ownership in Fresenius Medical Care and is an inventor on patents in the field of dialysis. JWL serves as Chairperson of the MONitoring Dialysis Outcomes (MONDO) Initiative Data Management Group and as a member of the MONDO Steering Committee.
LAU is a full-time employee of the Renal Research Institute LLC, a wholly owned subsidiary of Fresenius Medical Care Holdings Inc. LAU holds share options/ownership in Fresenius Medical Care and is an inventor on patents in the field of dialysis. LAU serves as an Executive Advisory Board Member for Privacy Analytics Inc., a Steering Committee Member of the MONDO initiative, and a Steering Committee Member of the American Society of Nephrology Partnership for Responsible Augmented Intelligence in Kidney Health.
MG is affiliated with the Division of Nephrology, Stanford University School of Medicine.
PK is a former employee of the Renal Research Institute LLC, a wholly owned subsidiary of Fresenius Medical Care. PK holds stock in Fresenius Medical Care and is an inventor on multiple patents in the field of kidney care.
PP, BH, and VR are students affiliated with the Pontifical Catholic University of Paraná. VR and YJ are also employees of the Renal Research Institute LLC, a wholly owned subsidiary of Fresenius Medical Care.
RPF is employed by the Arbor Research Collaborative for Health, which runs the DOPPS studies. RPF reports non-financial support from Fresenius Medical Care, Bayer, AstraZeneca, Novo Nordisk, FibroGen, Akebia, and Boehringer Ingelheim; and personal fees from George Clinical, all outside the submitted work.
TP is affiliated with the Pontifical Catholic University of Paraná. TP has served as a consultant for AstraZeneca, Baxter Healthcare, Bayer, Boehringer Ingelheim, Lilly, and Novo Nordisk; received research funding from Baxter Healthcare; and received honoraria from AstraZeneca, Baxter Healthcare, Bayer, Boehringer Ingelheim, Lilly, and Novo Nordisk. TP holds advisory or leadership roles as a member of the Peritoneal Dialysis International Editorial Board, Co-Editor in Chief of the Brazilian Journal of Nephrology, Coordinator of the ISPD International Studies Committee, and Coordinator of the Peritoneal Dialysis Committee for the Latin American Society of Nephrology and Hypertension (SLANH).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability
The dataset used in the presented analyses is not publicly available. The dataset was captured from a private electronic medical record system that is restricted to use by only authorized employees of Fresenius Medical Care. The dataset can be made available upon reasonable request to access the dataset, which would require an agreement to be established between Fresenius Medical Care and an external institution of any applicable requestor.
Sources of support
There was no external funding for the work presented in this manuscript. The author's institutions internally supported the conduct of the analysis and manuscript, which included employee salaries and company infrastructure.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.