
Abstract
Background
Patients receiving peritoneal dialysis (PD) often report problems with constipation. Constipation in PD is associated with increased risks of mechanical and infectious complications, such as poor drainage and fluid removal, catheter migration and peritonitis. A natural fibre supplement, psyllium husk, has been identified as a potential alternative therapy to minimise the risk of constipation for patients receiving PD.
Methods
FIBRE-PD is a prospective parallel-arm open-label feasibility study in which patients on PD were 1:1 randomly assigned to receive either psyllium husk (intervention group) or continue routine Movicol® (control group) for four weeks (28 days). The primary outcome was feasibility, defined as successful recruitment of 60 patients, representing 70% of eligible PD patients. Secondary outcomes included adherence, retention, safety, bowel frequency and patient-reported outcomes (e.g., gastrointestinal symptom burden, quality of life).
Results
Overall, 96 patients were screened for eligibility. Sixty-six (69%) were deemed not eligible, mainly due to non-adherence to prescribed regular Movicol (n = 41, 62%). Among 30 eligible patients, 20 patients (67% of eligible population) were successfully recruited into the study. The intervention group demonstrated high retention (77%), adherence rates (78%) and significant improvement in gastrointestinal symptoms and quality of life compared to patients in the control group. No adverse outcomes were reported.
Conclusion
The FIBRE-PD did not meet its original recruitment target due to an unexpectedly high number of ineligible patients. The recruited proportion almost reached the pre-specified target of 70% of eligible patients, and participants in the intervention group demonstrated high retention and adherence rates with observed benefits in gastrointestinal symptom burden and quality of life.
This is a visual representation of the abstract.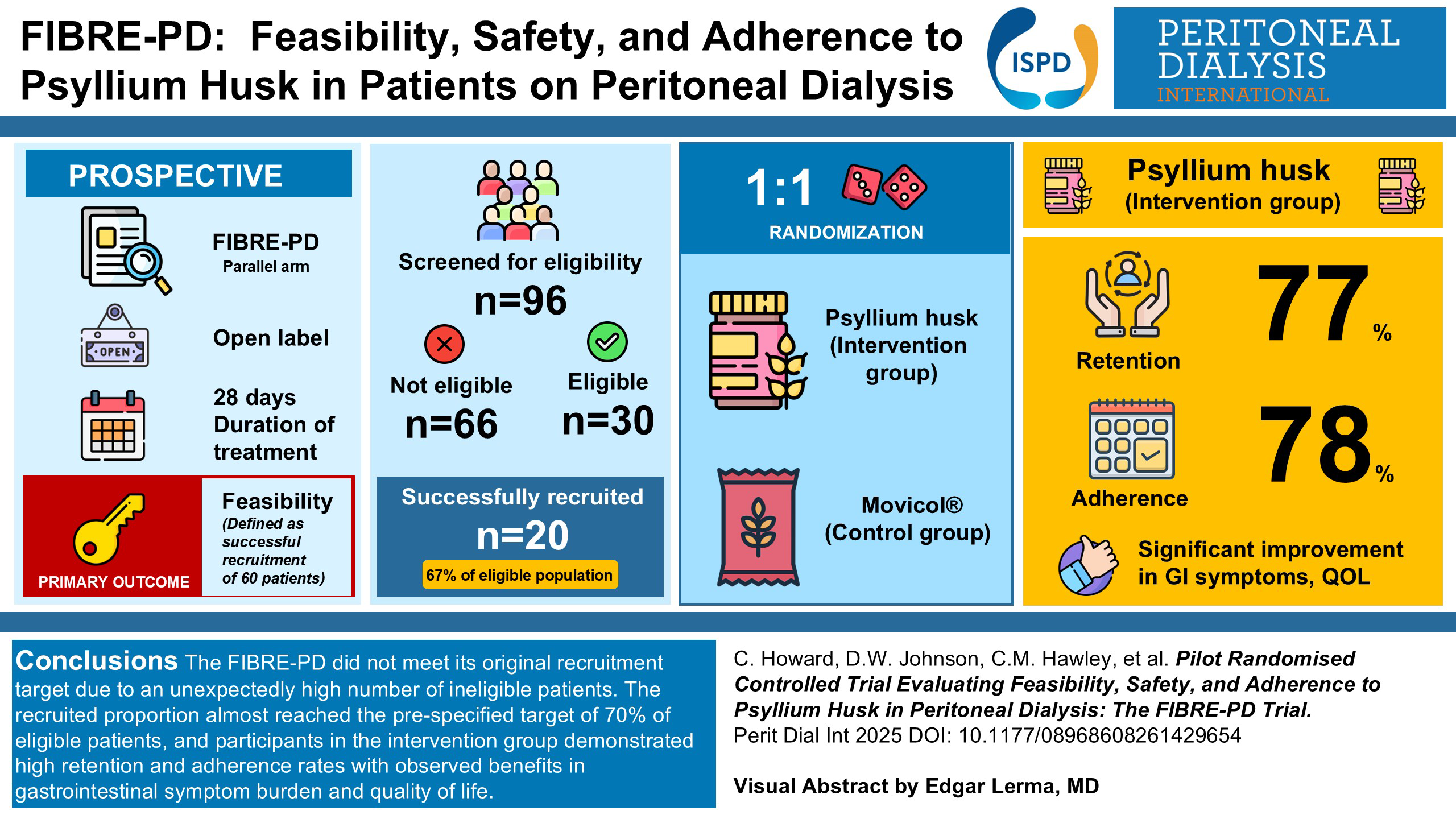
Introduction
Peritoneal dialysis (PD) is the most common type of home dialysis modality used to treat patients suffering from kidney failure in Australia. 1 Many patients receiving PD report problems with gut motility, mostly from constipation. The causes of constipation in PD are multifactorial, including fluid restrictions, low dietary fibre intake, comorbidities (e.g., diabetes) and medications (e.g., phosphate binders, diuretics, calcium channel blockers). Constipation in PD is associated with increased risks of mechanical and infectious complications, 2 such as drainage obstruction and poor fluid removal, catheter migration and peritonitis. Su et al. observed that the only symptom directly associated with peritonitis was constipation in their study involving 158 patients.2,3 The burden of symptoms associated with constipation and psychological impacts can negatively affect quality of life and compromise both physical and emotional well-being, 4 whilst posing additional economic burden to patients. Unsurprisingly, gastrointestinal problems have been identified as one of the important outcomes that matter to key stakeholders in PD, including patients receiving PD, as identified in the global Standardised Outcomes in Nephrology-PD (SONG-PD) Initiative. 5
Patients on PD are advised to consume regular bowel aperients to minimise the risk of constipation, which include a plethora of laxative compounds (such as bulk forming, osmotic, stimulant, pro-kinetic). However, these are poorly tolerated, costly, add to pill burden and not always effective. One of the most common forms of laxatives used is Movicol® (macrogol-3350 + sodium chloride + bicarbonate + potassium chloride, Norgine), a type of osmotic laxative. Patients are often advised to take multiple sachets of this agent daily, even though they are also often poorly tolerated thereby resulting in sub-optimal adherence. In addition, patients may need to consume up to eight sachets a day (daily out-of-pocket cost of A$5.33/day with weekly cost reaching A$37.31) to maintain bowel regularity, which is both burdensome and expensive.
Psyllium husk is a natural, bulk forming, cost-effective laxative ((recommended daily dose 8 g, equating to AUD$0.23/day or AUD$1.61 per week, and AUD$6.79 per month)), which works to regulate bowel motion by increasing the size and weight of the stool, thereby stimulating bowel activity, and making the stool easier to pass. 6 A recently completed meta-analysis by McRorie et al. showed that soluble fibre in the form of psyllium was 3.4 times more effective than insoluble fibre at increasing stool output in people with chronic idiopathic constipation. 7 In another study by Noureddin et al., it was shown that psyllium supplementation not only improved constipation but also improved glycaemic and lipid control as well as weight in patients with type 2 diabetes mellitus and chronic constipation. 8 Psyllium husk can also be mixed with soft foods rather than water, which may provide additional benefit for patients on PD with a fluid restriction. Although these data from general populations are encouraging, the benefits of psyllium husk have not been examined in patients on PD. The FIBRE–PD trial was developed to explore feasibility of recruitment, adherence, efficacy and safety of implementing psyllium husk to patients receiving PD compared to standard care. This feasibility trial was conducted to confirm recruitment, adherence, and safety, ensuring that a larger efficacy study would be practical and well-designed for this population.
Methods
Study design
FIBRE-PD is a single-centre, parallel group, open-label, randomised controlled trial (ACTRN12622000895785). The study protocol was reviewed by the Metro South Human Research Ethics Committee (HREC/2021/QMS/76238). Informed consent was obtained from all participants. The study was conducted according to International Committee for Harmonisation (ICH) Good Clinical Practice (GCP) guidelines and reported according to CONSORT guidelines. The study was conducted in the Peritoneal Dialysis Unit of the Princess Alexandra Hospital from 11 October 2022 to 11 October 2023.
Participants
Eligible participants were aged 18 years or older, had received PD for ≥3months, were currently taking Movicol® to regulate their bowel motions as prescribed by the treating team (defined as taking more than one sachet per week) and were able to provide informed consent. Non-adherence was defined as taking less than one sachet per week despite being prescribed regular Movicol®, consistent with unit policy to recommend routine aperient use to prevent catheter-related complications. Additionally, patients were excluded from the study if they met any of the following criteria: (1) had received radiation to the bowel or had a large bowel resection, (2) had medically diagnosed and active inflammatory bowel disease, (3) were unwilling or unable to meet the requirements of the protocol, (4) had a physical, medical or psychological condition that may have interfered with study participation and (5) had no plans for commencing or recently commenced any new dietary therapy during the trial duration.
Study procedures
Participants meeting the inclusion criteria were randomly assigned in a 1:1 ratio to receive either psyllium husk or continue Movicol®. Random allocation was concealed by using a centralised spreadsheet accessed by research nurses not connected to the study located external to the peritoneal dialysis unit. Participants in the psyllium husk group (intervention group) received a 1-kg bag of natural psyllium husk fibre and a 20-ml measuring scoop. Initial dose was 1 scoop per day (8 g of psyllium husk), with the dose to be up titrated (up to three scoops/day) if needed throughout the study period. They were instructed to completely cease their regular Movicol® during the study duration. Participants in the standard treatment arm (control group) were instructed to continue their regular dose of Movicol® as usual during the study period. A baseline dose of Movicol was recorded at enrolment and weekly during the study period. There were no study-specific guidelines for dose adjustment for Movicol; dosing remained at the discretion of the patient, consistent with usual clinical practice (between one to six sachets/day). Both arms were given a daily checklist to record actual usage of product, as patients were given flexibility to adjust the number of psyllium husk scoops or number of Movicol® sachets per day based on their bowel motion frequency (aiming for one bowel motion/day) and Bristol stool score (aiming for Type IV). During weekly telephone calls initiated by nurses, their progress was reviewed and the doses of Movicol® or psyllium husk were modified as necessary, for control and intervention group, respectively. Data were collected at baseline (day 0) and then weekly for 28 days. Data collection at days 0, 3, 7, 14, 21, and 28 was chosen to enable early safety monitoring, assess adherence patterns and evaluate short-term symptom changes during the initial treatment period. Safety outcomes included measurement of serum potassium at day 14. Data collection schedule for the trial is outlined in the Supplementary Table 1.
Outcomes
The primary outcome was feasibility, specifically whether 60 eligible PD patients (representing 70% of patients in the unit) could be recruited to the study (i.e., a proxy indication that they were willing to take psyllium husk). Secondary outcomes included adherence, retention, patient-reported and clinical outcomes. Adherence was defined as taking more than 80% of the prescribed study therapy at day 28 (original weight-final weight of bag/number of days). Retention was assessed by the proportion of patients who remained in the study for the entire study period and completed all the study requirements without withdrawing their consent. Patient-reported outcomes included changes in quality of life and changes in gastrointestinal symptom burden (measured using the Edmonton Symptom Assessment and Gastrointestinal Symptom Rating Scale). Clinical outcomes assessed were bowel motion frequency (total number of motions over three days), catheter malfunctions requiring intervention (including poor flow, catheter malposition requiring surgical repositioning, etc.) and episodes of volume overload requiring hospitalisation. Safety outcomes included any adverse or serious adverse events (such as death or unplanned hospital admissions) and biochemistry parameters (proportion of patients with hyperkalaemia >6 mmol/L requiring treatment).
FIBRE-PD's main objective was to provide precise estimates of feasibility and tolerability, that will help in the planning of a larger, sufficiently powered trial. The target sample size was 60, representing 70% recruitment rate out of those eligible with 80% adherence rate. The 95% confidence intervals were estimated to be (58%, 82%) and (66%, 94%), respectively. Recruitment feasibility, adherence and retention were estimated as proportions.
Statistical analysis
Descriptive statistics were used for patient characteristics. Continuous data were described using mean ± standard deviation or median (interquartile range) and compared between groups using t-test or Mann‒Whitney U-test, as appropriate. Categorical data were reported as frequency (%) and compared between groups using Chi-squared test. The proportion of patients with optimal Bristol Stool Score (Score 3 or 4) between each treatment group was assessed using chi-squared test. The overall linear trends in repeated measures continuous data (e.g., daily bowel frequency) over the follow-up period were analysed by fitting a multilevel linear regression model. Continuous data were transformed (e.g., logarithmic transformation) if required and continuous time was included as a fixed-effect. Random intercepts and slopes were added to allow for repeated measurements over time. To evaluate the differences between the two treatment groups on these outcomes, treatment (psyllium husk vs. Movicol®) group and time were subsequently added to the model as fixed effects. If the interaction term was not statistically significant, it was dropped from the model and the unconditional effect of treatment was assessed. Data were analysed using the software package Stata/SE14.0 (College Station, TX, USA). P < 0.05 was considered to represent a statistically significant difference.
Results
Participant characteristics
Patients were approached to participate in the study at clinics from 11 October 2022 to 11 October 2023. In total, 20 patients consented to participate in the study and 11 were randomised to the intervention group (55%). Baseline demographic characteristics were comparable between the two groups (Table 1) other than higher proportions of females (55% vs. 22%), diabetes mellitus (27% vs. 11%) and automated PD utilisation (64% vs. 44%) in the intervention group. A significantly higher proportion of patients randomly allocated to psyllium husk reported more optimal Bristol Stool Score (64% vs. 22%). Two participants in the intervention group (2 of 11) did not complete the study as they received kidney transplants.
Baseline demographics of study participants.
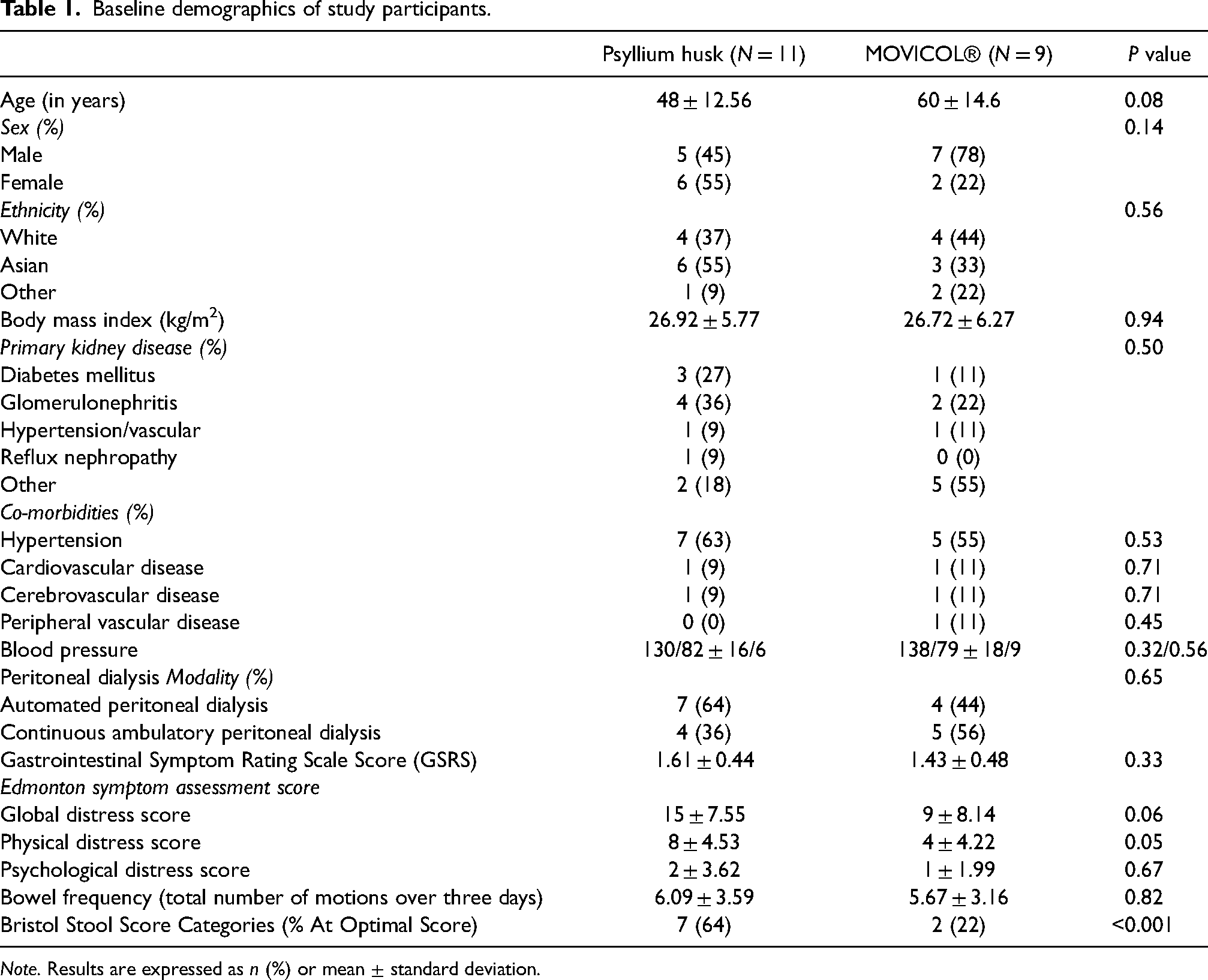
Note. Results are expressed as n (%) or mean ± standard deviation.
Feasibility, adherence and retention
Among 96 patients who were screened, 30 patients met the eligibility criteria (31%) and 20 consented to participate (representing 67% of eligible patients; Figure 1). Those who were deemed ineligible for participation were mostly due to non-adherence to regular Movicol® prescribed by their treating team (defined as taking at least one sachet per week) (self-disclosed; n = 41; 62% of ineligible patients).
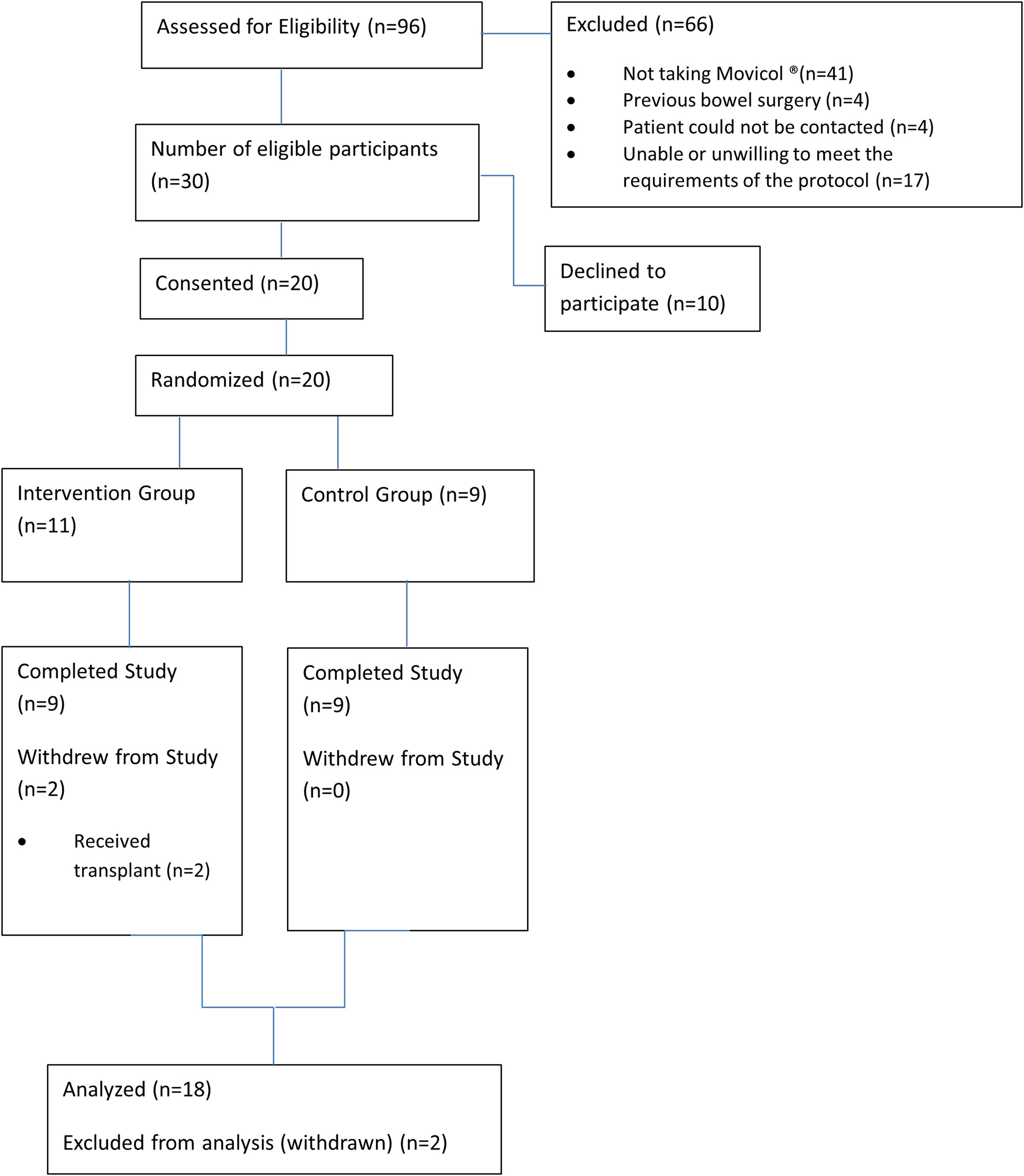
FIBRE-PD study flow diagram.
Adherence in the intervention group was assessed as the proportion of patients who consumed more than 80% of the prescribed study therapy at week four. Of the participants, 78% (7 of 9) consumed more than 80% of the prescribed psyllium husk during the study period. The two participants who did not meet adherence criteria were due to consuming only a half scoop (4 g) per day instead of recommended 8 g (full scoop) due to desired effect obtained with a lowered dose. Once corrected for this modification, the average adherence rate (defined as taking >80% of the dose) was 100%. All participants in the control group reported adherence in taking Movicol® as prescribed throughout the study period.
Retention was defined as completion of a four-week study period without withdrawing consent. Other than two patients who received kidney transplants (intervention group), all participants completed the study in both groups.
Bowel frequency and bristol stool score
During the study, total bowel frequency over three days remained largely unchanged (coefficient −0.004, 95% CI −0.01 to 0.003, p = 0.3; median at baseline 6 [3‒6.5] to day 28 5.5 [3‒6]). There was a significant interaction between treatment type and time (p = 0.001), whereby patients receiving psyllium husk experienced a decrease in bowel frequency over time (coefficient −0.01, 95% CI −0.02 to 0.005, p = 0.002), which was not observed with Movicol® (coefficient 0.007, 95% CI −0.002 to 0.02, p = 0.12; Figure 2). The proportion of patients with an ideal Bristol Stool Score was greater for both groups (p < 0.001; supplementary Table 2). However, there were no significant differences in the proportions of patients with an ideal Bristol Stool Score between the two treatment groups at baseline (p = 0.09) and at day 28 (p = 0.66; Figure 3).
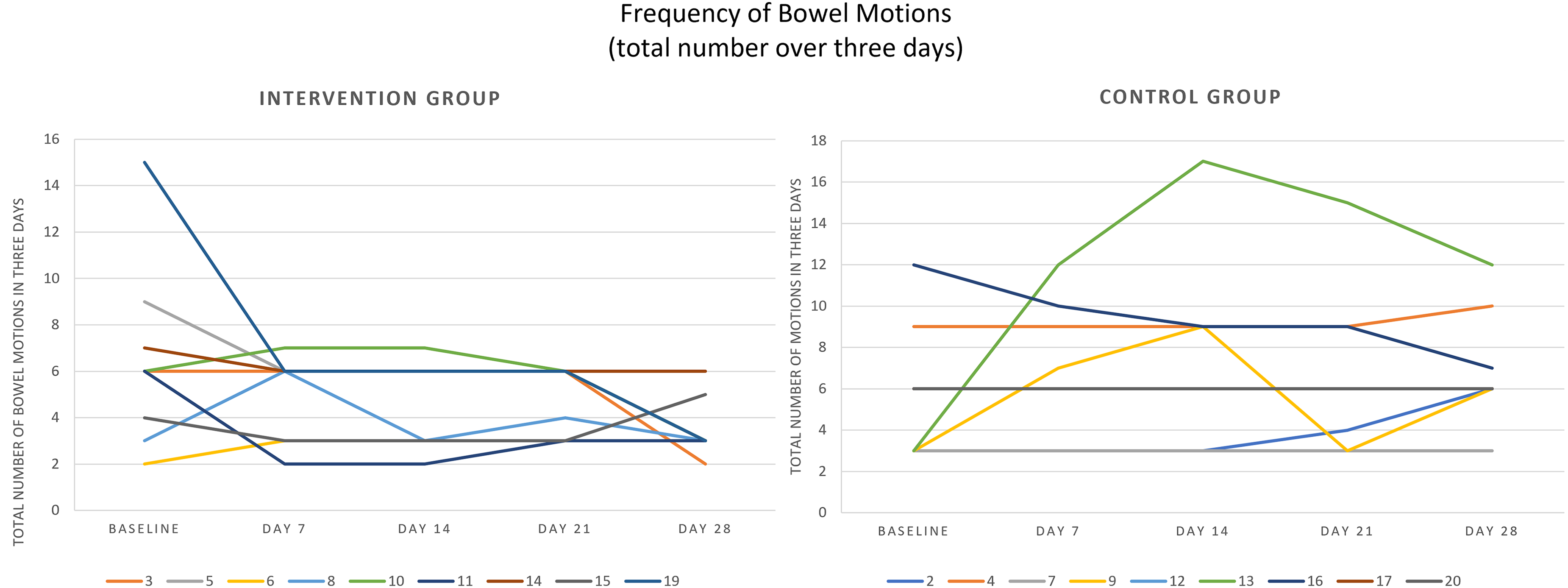
Frequency of bowel motions (total count over three days) for intervention and control groups.
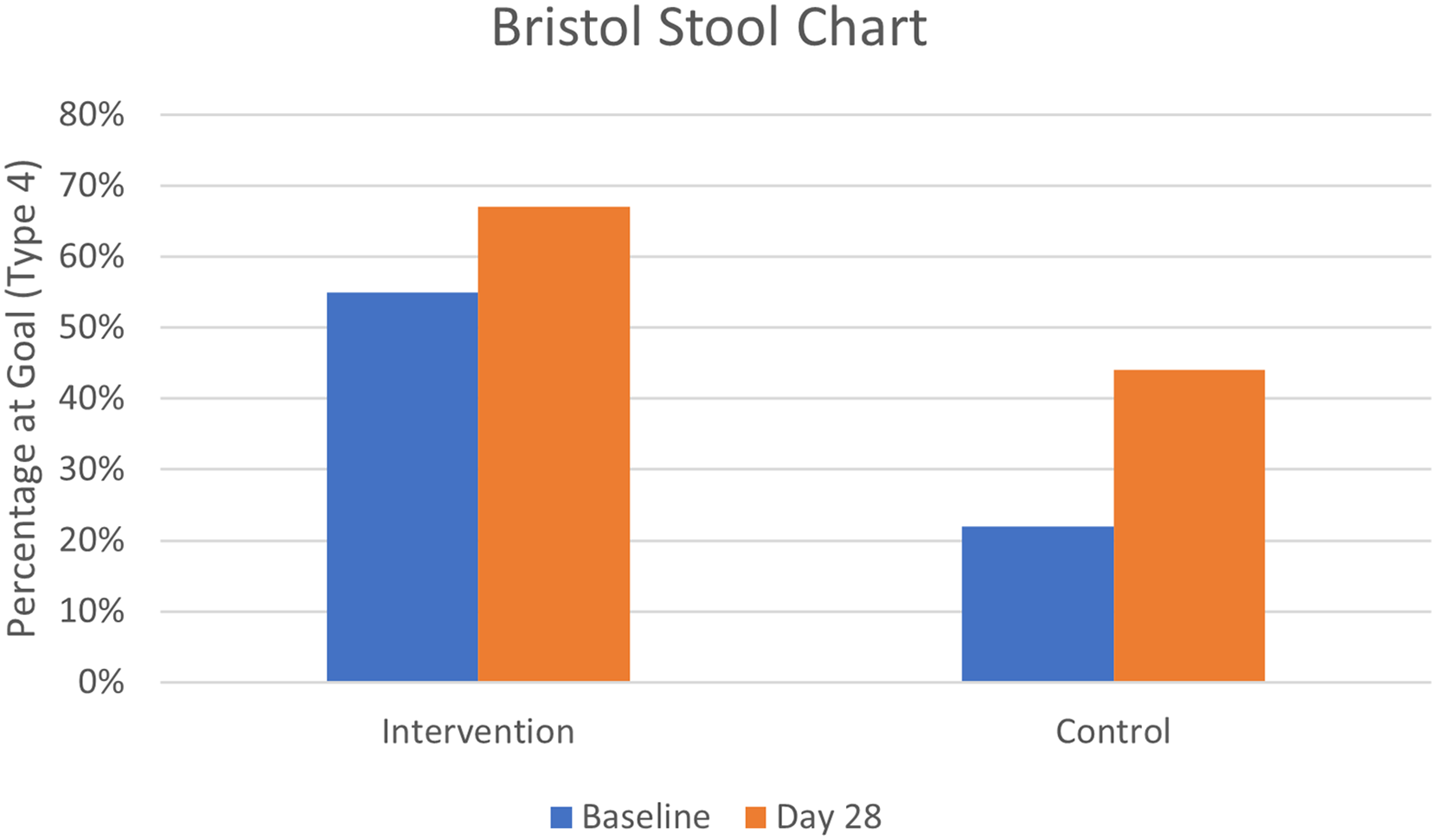
Proportion of patients for intervention and control groups with ‘ideal’ Bristol Stool Score at baseline (p = 0.09) and day 28 (p = 0.66).
Gastrointestinal symptom rating scale and Edmonton symptom assessment
The median GSRS decreased over time in the psyllium husk group (from 1.6 [1.2‒1.8] to 1.3 [1.2‒1.3]), whereas it was relatively stable in the Movicol® group (from 1.3 [1‒1.6] to 1.4 [1.1‒2.1]; Figure 4(a)). The difference in trend of log transformed GSRS over time was not statistically significant between the two groups (coefficient −0.02, 95% CI −0.25‒0.20, p = 0.83). The global distress component of the Edmonton Symptom Assessment decreased for those who received psyllium husk (from 14 [8‒18] to 4 [2‒9]) which was not seen in the Movicol® group (from 6 [4‒11] to 7 [5‒16]; Figure 4(b)). The difference in these results over time was statistically significant when examined as the first-order interaction term between treatment group and time (p = 0.008). Similar results were observed for the physical distress component of the Edmonton Symptom Assessment whereby the distress score decreased in the psyllium husk group from 8 [5‒10] to 1.5 [0‒4] but increased in the Movicol® group from 3 [2‒6] to 6 ([2‒9]; p = 0.003). The psychological distress component of the Edmonton Symptom Assessment was comparable over time for both groups.
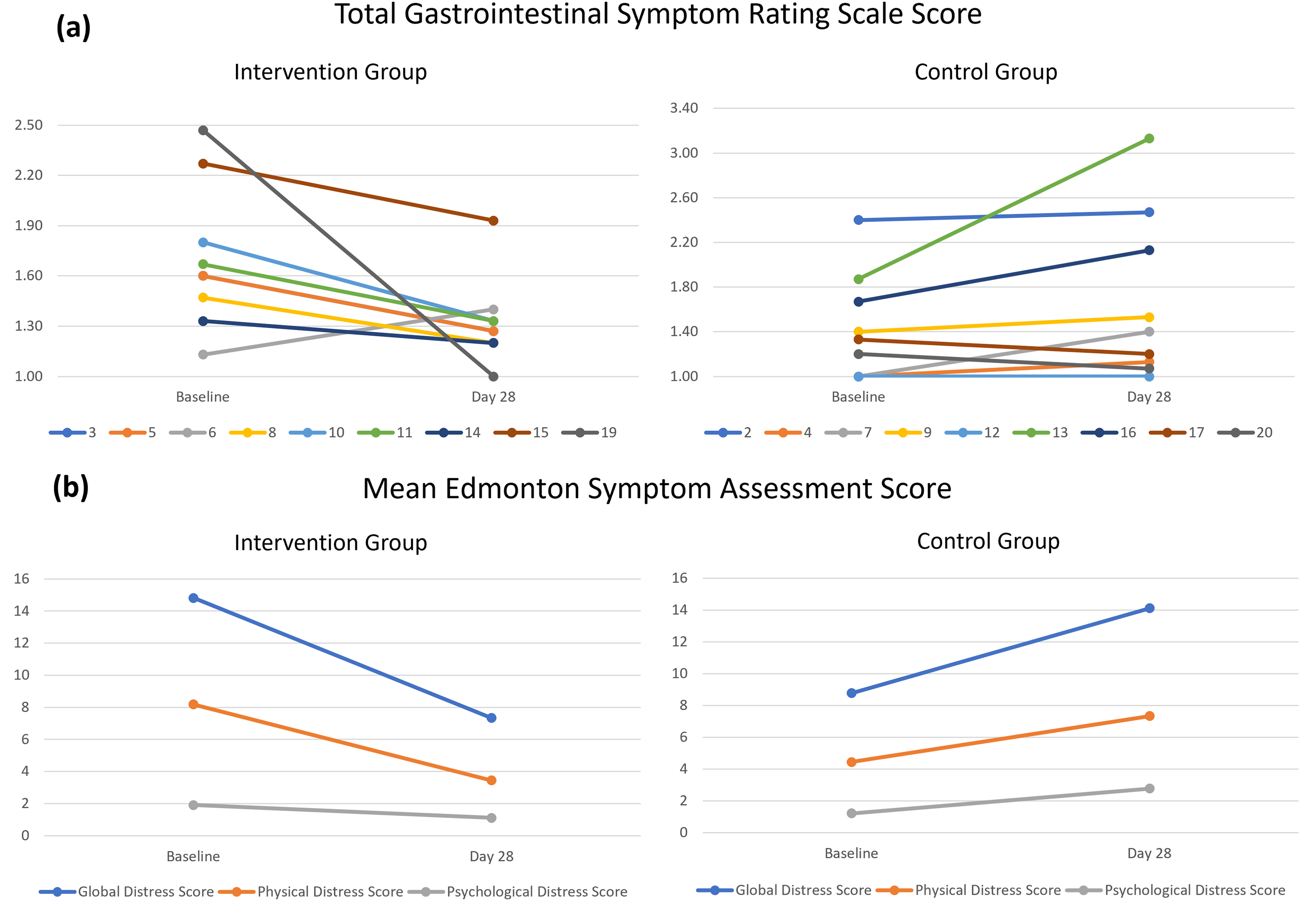
(a) Trends in gastrointestinal symptom burden measured by Gastrointestinal Symptom Rating Scale. (b) Trends in quality of life measured by Edmonton Symptom Assessment.
Safety
There were no adverse events or serious adverse events in either group, including no documented episodes of hyperkalaemia, episodes of volume overload requiring hospitalisation or catheter malfunctions requiring intervention.
Discussion
In this feasibility RCT, psyllium husk in patients receiving PD was demonstrated to be as effective and safe as Movicol® in supporting regular bowel motions. The study did not reach the feasibility criteria defined by the recruitment target. However, this was mainly due to an unexpectedly large number of patients (n=41) who were ineligible due to non-adherence to regularly prescribed Movicol® as per their treating team. Although the recruitment number was lower than the initial target, the FIBRE-PD trial was able to enrol more than two-thirds of eligible patients and demonstrated high adherence and retention rates in the intervention group. Patients who received psyllium husk also reported a significantly lower symptom burden compared to those who were allocated to receiving Movicol®.
Psyllium husk was well tolerated and compared with Movicol®, it was associated with a reduction in gastrointestinal symptom burden, an improvement in stool consistency, and a decrease in stool frequency, especially among those with higher baseline values. These changes were accompanied by improvement in quality-of-life scores in both physical and mental distress components among patients who received psyllium husk. These results are in keeping with published experiences of psyllium husk in the general population where the agent has been shown to relieve both constipation and diarrhoea. 9 The observed reduction in bowel frequency without significant changes in Bristol Stool Score may reflect that most patients in the psyllium husk group already achieved optimal stool consistency at baseline (64%), leaving limited scope for further improvement, while psyllium's water-absorbing and gel-forming properties likely moderated stool frequency without compromising form. In fact, psyllium husk has been identified as one of the most effective types of fibre in treatment of irritable bowel syndrome because it is soluble and has high water-holding, gel-forming capacity, which facilitates smooth transit of stool through the gastrointestinal tract. Moreover, psyllium husk is mostly non-fermenting or mildly fermenting, which enhances its water-holding capacity whilst reducing gas production thereby mitigating the bloating and abdominal discomfort exerted by other bowel aperients. 10
High adherence to psyllium husk was achieved without an increase in adverse effects compared to the use of Movicol® in the FIBRE-PD study. In addition, the lower cost of psyllium husk is likely to make this more desirable compared to Movicol® from the patient's perspective. For example, one month's supply of Movicol® (30 sachets) costed AUD $11.88 on average, whilst one month's supply of psyllium husk (250 g) costed AUD $6.79 on average. This means that if patients are prescribed psyllium husk instead of Movicol®, this switch will result in 43% lower out-of-pocket expenses for patients.
A surprising finding in this study was the unexpectedly high proportion of patients who were assessed as being ineligible due to non-adherence to Movicol® prescribed by the treating team for regular administration. Although the reasons for non-adherence were not specifically explored as part of this study, prior studies have reported reduced adherence to Movicol® due to its taste and gastrointestinal side effects, including bloating, cramping and loose stools. 11 Additionally, while Movicol® increases stool frequency, it does not necessarily improve stool consistency or composition. Patients starting PD have reported an increase in symptom burden from increased stool frequency, resulting in poorer quality of life and at times limited functional capacity. 12 This highlights a huge gap in current practice, whereby existing bowel management strategies are not meeting patient needs. It is quite plausible that this disparity is responsible for significantly high rates of transfer to haemodialysis within the first year of starting PD due to mechanical reasons, which is often closely related to constipation. Despite the critical importance of bowel function to the success of PD, gastrointestinal symptoms experienced by patients receiving PD are poorly understood. In a recently published systematic review of all RCTs involving patients on PD, gastrointestinal symptoms were only reported in 61 (19%) of 324 PD trials. Most (90%) of the gastrointestinal outcomes were patient-reported adverse effects with no defined metrics, with the most common outcomes being nausea (n = 27, 43%), followed by diarrhoea (n = 26, 43%), vomiting (n = 22, 36%) and constipation (n = 21, 34%).13,14 The findings from this review are consistent with the recent report from the Kidney Disease – Improving Global Outcomes (KDIGO) initiative, which described decreased appetite, diarrhoea, nausea, vomiting and constipation as common and serious patient-identified symptoms that are poorly managed with modern treatment. 15
This study has several strengths including its randomised, feasibility trial design together with detailed data collected to verify safety, tolerance and adherence. However, these need to be weighed against the limitations of the study. It was a single-centre trial with a small sample size, thereby limiting its generalisability. The study was not powered to evaluate hard clinical endpoints, such as transfer to haemodialysis from mechanical complications like catheter dysfunction, which are critical outcomes for PD patients. Additionally, the open-label design may have introduced bias, particularly with respect to patient-reported outcomes. The high ineligibility rate further limited the applicability of the findings to the broader PD population. In the future, if a similar study is to be repeated, study design should consider the risk of non-adherence to Movicol® prescribed by the treating team. The short follow-up period also limited evaluation of long-term outcomes.
In conclusion, FIBRE-PD presents psyllium husk as an alternative to Movicol® for managing constipation in PD patients. Its tolerability, cost-effectiveness and efficacy in reducing symptom burden and improving quality of life make it a viable option for addressing a critical gap in PD care. The results of the FIBRE-PD trial will help to inform the design of a future large-scale, multi-centre study, which is necessary to confirm the results observed and assess long-term clinical and patient-centred outcomes.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608261429654 - Supplemental material for Pilot randomised controlled trial evaluating feasibility, safety and adherence to psyllium husk in peritoneal dialysis: The FIBRE-PD trial
Supplemental material, sj-docx-1-ptd-10.1177_08968608261429654 for Pilot randomised controlled trial evaluating feasibility, safety and adherence to psyllium husk in peritoneal dialysis: The FIBRE-PD trial by Chloe Howard, David W Johnson, Carmel M Hawley, Kylie Pegg, Hannah Mayr, Diana Leary, Rachael Hale, Andrea K Viecelli, Janette Hamilton, Vicki Thomas, Irish Dela-Pena and Yeoungjee Cho in Peritoneal Dialysis International
Footnotes
Acknowledgements
The authors acknowledge the Princess Alexandra Hospital Peritoneal Dialysis Unit Nurses and Patients.
Author contributions
Study conception: C. Howard and J. Hamilton. Study design: C. Howard, D.W. Johnson, C.M. Hawley, K. Pegg, H. Mayr, D. Leary, R. Hale, A. K. Viecelli, J. Hamilton, V. Thomas, I. Dela-Pena and Y. Cho. Conduct of the trial related activities: C. Howard K. Pegg, H. Mayr, J. Hamilton, V. Thomas, I. Dela-Pena and Y. Cho.
Data analysis: C. Howard, Y. Cho. Manuscript draft and review: C. Howard, D.W. Johnson, C.M. Hawley, K. Pegg, H. Mayr, D. Leary, R. Hale, A. K. Viecelli, J. Hamilton, V. Thomas, I. Dela-Pena and Y. Cho.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by Metro South Human Research Ethics Committee (HREC/2021/QMS/76238).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This study was received funding support from Queensland Health – Clinical Research Fellowship (mid-career; Chief Investigator – Yeoungjee Cho).
Informed consent to participate
Written informed consent was obtained from all subjects before the study.
Informed consent to publish
Written informed consent was obtained from the patients for their anonymised information to be published in this article
Trial registration
Australian New Zealand Clinical Trial Registry: ACTRN12622000895785.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.