
Abstract
Background
Chronic kidney disease (CKD) represents a growing public health challenge worldwide, particularly in countries with a medium sociodemographic index such as the Dominican Republic (DR), where both the incidence and prevalence of CKD have shown a sustained increase. In response, the DR government launched a national peritoneal dialysis (PD) program in 2013 to expand access to kidney replacement therapy (KRT).
Methods
A retrospective analysis was conducted on the development and implementation of the national continuous ambulatory peritoneal dialysis (CAPD) program over ten years. The model was structured around three pillars: (1) a multidisciplinary team comprising nephrology, nursing, nutrition, psychology, and social work; (2) dedicated infrastructure for PD delivery; and (3) a management system driven by standardized processes and protocols, aligned with ISO certification standards. Patient care involved comprehensive baseline assessments, structured training, monthly follow-up, routine retraining, and home evaluations. Program performance was monitored through predefined clinical indicators.
Results
Since the implementation of the program, the PD penetration in DR increased from 2.7% to 22.4%, reaching 1118 patients by the end of 2024. This growth reflects the program's ability to improve access to KRT through a centralized and standardized care model. This model not only facilitated consistency in care delivery across participating centers but also enhanced the growth of PD.
Conclusions
The 10-year experience of the national PD program in the DR provides evidence for the feasibility and effectiveness of a standardized, patient-centered, and multidisciplinary PD program. The implementation of this program has significantly increased access to kidney replacement therapies and driven the sustained growth of KRT in the DR and provides a scalable model for the implementation of national PD initiatives in similar contexts.
Introduction
Over the past three decades, we have witnessed significant changes in the behavior of the world's population. Life expectancy has increased, accompanied by population aging and a rising prevalence of chronic non-communicable diseases such as diabetes mellitus (DM).1,2 Likewise, chronic kidney disease (CKD), a condition associated with DM, hypertension (HTN), and aging, has gained relevance, not only because of the increase in its frequency (around 10% of the world's population) 3 but also due to the growth observed over the last 30 years in the number of related deaths (98% increase, 1.1 million) and the impact on disability-adjusted life years, DALYs (62% increase, 35 million). 4 This trend is particularly evident in countries with a medium sociodemographic index, where CKD rose nine places on the scale of diseases that cause the most DALYs in the population. 2
The Dominican Republic (DR) is a middle-income country. According to 2023 data, the population was 11.3 million inhabitants, and its gross domestic product (GDP) was $121.4 billion. In 2021, 4.92% of the GDP was allocated to health spending. Its life expectancy is 73 years. The population growth rate is 1.1% per year, and the crude mortality rate in 2021 was seven deaths per thousand inhabitants. 5 CKD is the seventh leading cause of death in the country, 6 with DM and HTN being its main causes. The prevalence of CKD in 2017 was 8394 cases per 100,000 inhabitants, and the associated mortality was 25 cases per 100,000 inhabitants, 7 representing a growing burden for the Dominican Health System. 8
The current structure of the Dominican Health System (DHS) dates back to 2001. An overview of the coverage and financing mechanisms under the Dominican Social Security system is provided in Supplemental Figure S1. Within this framework, the DHS ensures full coverage of dialysis therapies, including both hemodialysis (HD) and peritoneal dialysis (PD).9–11
PD in the DR has evolved through several key stages over the past decades. Early PD procedures were first performed in 1966, followed by the establishment of an intermittent PD program in 1976. Universal coverage for dialysis therapies was implemented in 2001; however, despite this policy, PD uptake remained low, with only 2.7% of patients receiving PD in 2012.12–14 In response to this limited uptake and the growing burden of CKD, a major structural transformation occurred in 2011 when the Dominican government launched a national public tender for PD services. 15 This initiative included the creation of seven dedicated PD centers nationwide, the development of a comprehensive care program, and the implementation of home delivery systems for dialysis supplies. The first patients were incorporated into the national PD program in 2013. Subsequent innovations included the incorporation of icodextrin into routine PD management in 2017 and the introduction of automated PD with remote monitoring in 2021.
This national strategy was designed to address the historically low utilization of PD and expand access to kidney replacement therapy (KRT) in a standardized and coordinated manner.
This study describes the structure, implementation model, and clinical outcomes of the national PD program in the DR over its first decade.
Methods
Study design
A retrospective evaluation of the DR's national PD program was conducted for the period from January 1, 2013, to December 31, 2024. The analysis focused on the program's structure, implementation model, and clinical outcomes over the 12-year span. Data were collected prospectively and analyzed retrospectively.
Structure of the care model
The program is built on a multidisciplinary and patient-centered care model, supported by three essential pillars: a team of highly trained healthcare professionals including nephrologists, nurses, dietitians, psychologists, and social workers; dedicated infrastructure designed specifically for the provision of PD; and a management system based on standardized processes, aligned with international quality standards and certified under ISO regulations.
Patient flow and clinical management
Modality selection is initially made at the patient's hospital after all KRT options are explained. If the patient is deemed suitable for PD, they are referred to the nearest PD center. Although they are referred specifically for PD, all candidates undergo a structured evaluation to confirm suitability, and KRT options are reviewed again to ensure an informed choice before catheter placement is scheduled. After catheter insertion, patients and/or caregivers receive standardized training and certification before discharge to home-based therapy.
The multidisciplinary team conducts baseline assessments and encompasses a detailed evaluation of the patient's body composition, cognitive function, and peritoneal catheter exit site. Comprehensive blood tests, a thorough review of clinical history, and a physical examination complement these.
A personalized dialysis prescription and short-term care plan is defined. Monthly in-person follow-ups are held, during which dialysis parameters, pharmacological treatment, dietary plans, and psychosocial needs are adjusted. Regular retraining and home visits are protocolized, including additional visits following hospitalizations or infectious complications.
Human resources
Each PD center is staffed by a fixed team including nephrologists, nurses, psychologists, dietitians, and social workers trained specifically in PD (see supplemental table S1). The team-to-patient ratio is standardized across centers. Staffing ratios are regulated by the PD program provider and monitored through internal routine audits.
Infrastructure
Seven PD centers were specifically designed to support the operational needs of the comprehensive care model. Each facility includes consultation rooms assigned to each specialty, dedicated spaces for patient training and post-training recovery, as well as areas designated for clinical procedures, educational activities, and storage of medical supplies. A schematic representation of the standard layout is provided in Supplemental Figure S2.
Management system
The program is structured around a standardized management system, certified under ISO-9001 and ISO-14001, and supported by clinical protocols grounded in international best practices. Key performance indicators, such as peritonitis rates, are monitored regularly and discussed in monthly review meetings. When any deviations from expected standards are identified, targeted quality improvement actions are implemented to strengthen the consistency and safety of care.
Clinical indicators and outcomes
Program performance was evaluated using three core indicators: the annual peritonitis rate, expressed as episodes per patient-year and calculated as the total number of peritonitis episodes divided by the total time at risk of all patients in the period; the rate of transfer to hemodialysis due to peritonitis-related complications; and the total number of active PD patients over time. 16 The percentage of transfers to hemodialysis related to infection was defined as the number of PD patients transferred to HD due to peritonitis divided by the total number of active PD patients for the corresponding year. 17 Staffing ratios were established during the design of the national PD program to ensure patient safety and workload balance. Compliance with these ratios and adherence to clinical protocols are verified through periodic ISO-9001:2015 certification audits, coordinated through both internal quality assessments and external evaluations by the National Health Service.
Results
PD patients
To contextualize program expansion, Supplemental Table S2 summarizes the annual national distribution of hemodialysis and PD based on the available datasets for the study period. Although transplant numbers are not systematically recorded at the national level, these data allow PD growth to be interpreted within the broader trends of dialysis activity in the country.
Since implementation, the proportion of prevalent patients treated with PD in the DR has increased from 2.7% in 2013 to 21.6% in 2023. Figure 1 demonstrates the program's improved ability to broaden access to KRT through a standardized and centralized care model.
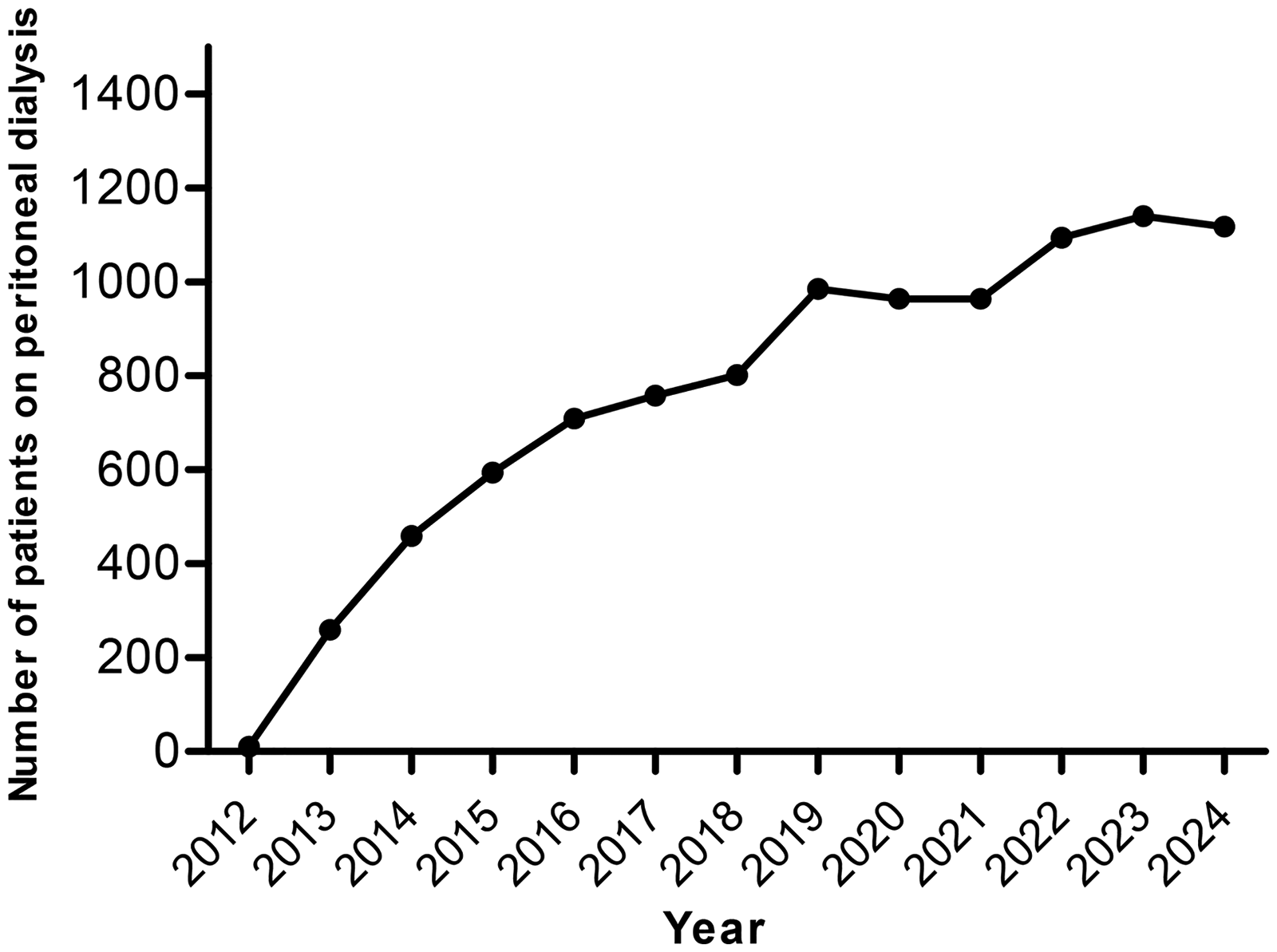
Number of active patients in the program as of 31 December 2024. Growth of the national peritoneal dialysis (PD) program in the Dominican Republic from 2012 to 2024. The number of active patients receiving PD increased progressively following the implementation of the national program, reaching 1118 patients by December 2024.
Table 1 summarizes the demographic and clinical characteristics of the cohort as of December 31, 2024. The cohort consisted of 1118 active patients with a mean age of 54.6 ± 17.8 years and a male predominance of 58.6%. Most patients had a primary level of education, followed by secondary education, with a smaller proportion having no formal or university education. Diabetes mellitus, with or without hypertension, was the leading cause of kidney failure, followed by hypertension alone. The majority of patients were treated with CAPD, while a smaller proportion received automated PD (APD). These data describe the current demographic and clinical profile of the PD population in the DR.
Patients on KRT in the Dominican Republic (Dec 2024).
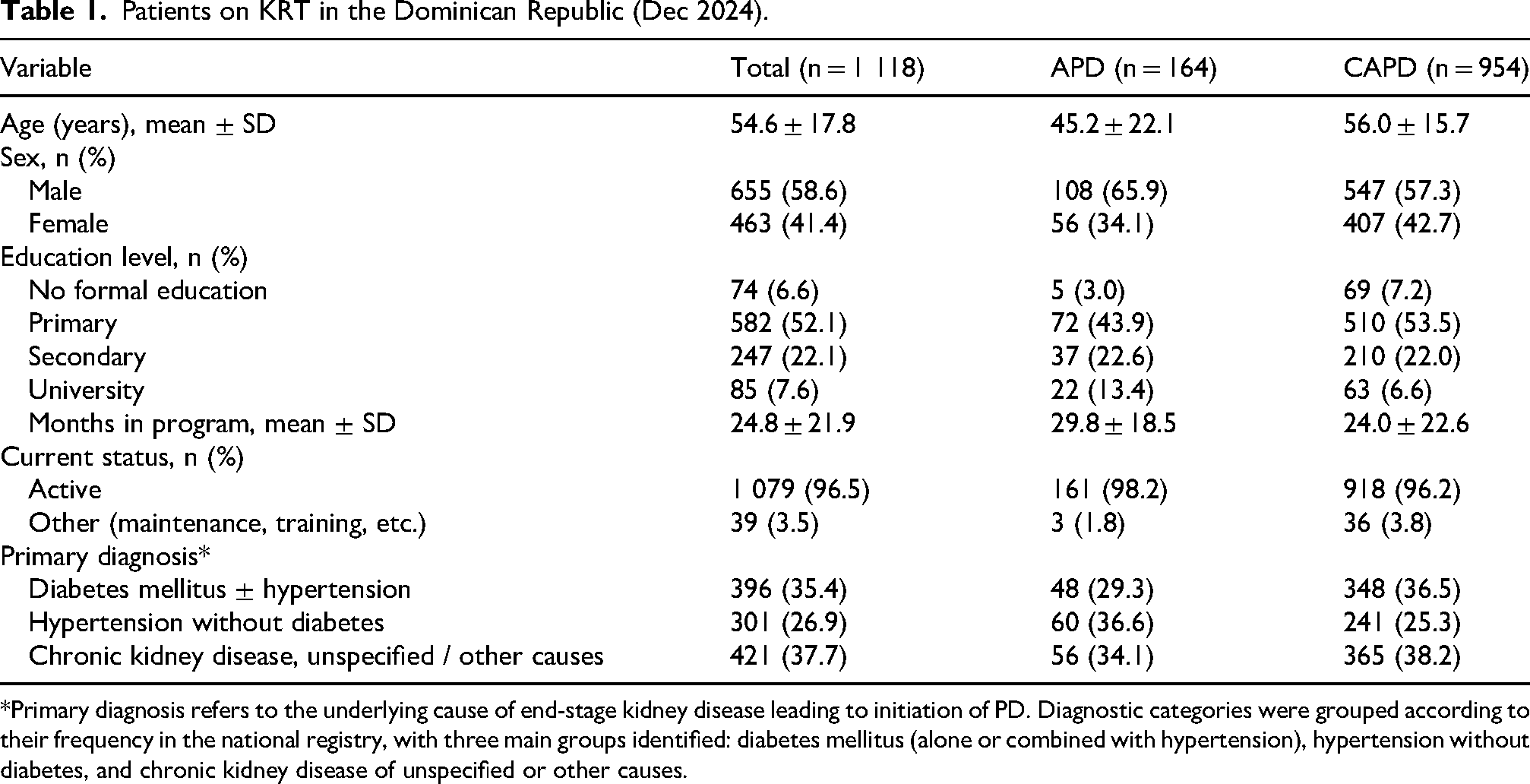
*Primary diagnosis refers to the underlying cause of end-stage kidney disease leading to initiation of PD. Diagnostic categories were grouped according to their frequency in the national registry, with three main groups identified: diabetes mellitus (alone or combined with hypertension), hypertension without diabetes, and chronic kidney disease of unspecified or other causes.
Over the past 3 years, PD numbers have remained stable. This plateau reflects a steady incidence of new dialysis starts, rather than a reduction in access to PD or limited use of available innovations. The stabilization in PD growth also coincides with the recent expansion of hemodialysis units in the country, which has increased overall HD availability and influenced modality distribution.
PD units
The program was implemented through a network of seven PD centers, each staffed by a multidisciplinary team comprising nephrologists, nurses, nutritionists, psychologists, and social workers. The care model and number of centers remained constant throughout the study period, based on three fundamental pillars: specialized equipment, dedicated infrastructure, and standardized ISO-certified processes.
All centers were designed under a standardized model with comparable infrastructure and organization to ensure uniform implementation of the national PD program. No substantial variation in infrastructure, staffing, or organization was observed across the seven centers.
Staff-to-patient ratios showed only minor variation across centers and consistently met the minimum standards of one nephrologist per 200 patients and one nurse per 40 patients, with similarly stable ratios across other disciplines, including social work, nutrition, and psychology. These ratios were consistently maintained across centers in accordance with predefined program standards (Figure 2).
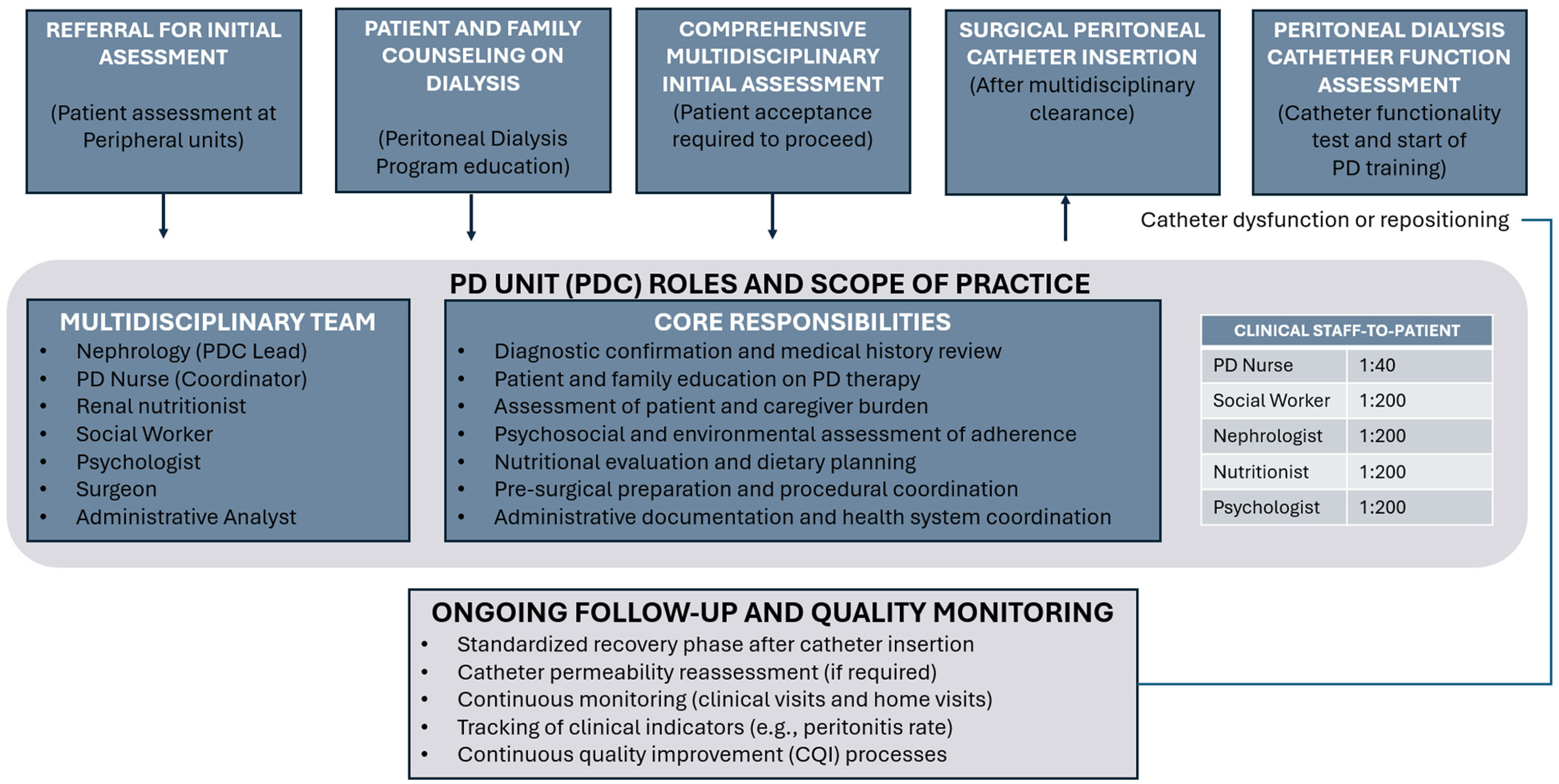
Complete patient admission & care model for peritoneal dialysis. *Standardized, Multidisciplinary, Health-System approved PD Care Model.
Outcomes
Infection outcomes also improved substantially. The annual peritonitis rate decreased from 0.8 episodes per patient-year in 2015 to an average of 0.19 during 2020–2022 and 0.13 in 2024, approaching the targets proposed by the 2022 ISPD guidelines (Figure 3(a)).
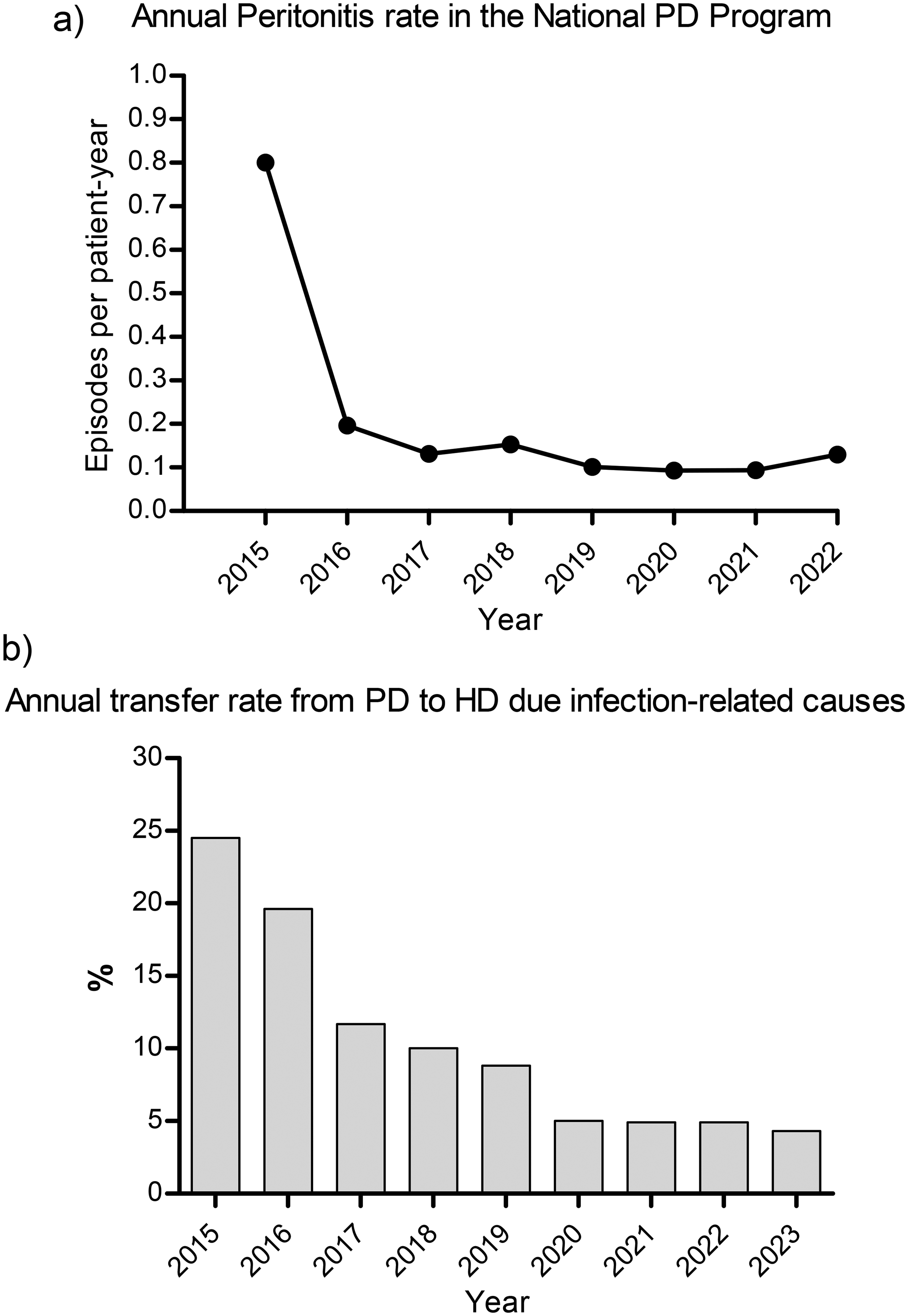
Annual PD-associated peritonitis rate (a) and transfer to hemodialysis due to infection-related causes (b). (a) Annual peritonitis rate associated with peritoneal dialysis, expressed as episodes per patient-year. (b) Annual proportion of patients transferred from peritoneal dialysis (PD) to hemodialysis (HD) due to infection-related causes. The figures show the progressive reduction in peritonitis rates and infection-related transfers over the study period within the national PD program.
However, microbiological documentation in the national registry was not standardized during the early years of the program, and culture-negative peritonitis episodes were not systematically recorded. Consequently, the reported peritonitis rates should be interpreted with caution, as the true incidence of PD-associated peritonitis may be underestimated.
The reduction in peritonitis rates was accompanied by a decline in transfers to hemodialysis due to infection-related complications (Figure 3(b)). Overall transfers to hemodialysis, irrespective of cause, were also recorded and are reported in the study dataset, showing a consistent pattern with the observed clinical outcomes. The consistent application of standardized clinical protocols, continuous quality improvement processes, and multidisciplinary monitoring were key factors in achieving and maintaining these outcomes.
Discussion
The growth of the national PD program is the result of a government decision to allocate resources and support the implementation of a comprehensive PD service. Key contributing factors include: (1) government funding and full coverage of supplies for PD patients; (2) the establishment of seven PD centers nationwide, with standardized training protocols for healthcare teams and patients; and (3) a strong referral network coordinated by hospital-based nephrologists.
Recent reports from the Dominican Society of Nephrology indicate that PD penetration reached approximately 21.6% of dialysis patients in 2023, equivalent to 91.1 patients per million population, supporting the expansion observed in the national PD program.18–23
A comprehensive approach to PD therapy has been achieved through interdisciplinary team involvement, ensuring proper PD catheter insertion, periodic follow-up and adherence to the recommendations made to the patient.
The promotion of quality driven culture has allowed the implementation of periodic audits, ensuring their standardization across the centers leading to standardized care processes and consistent clinical outcomes. The integration of a CQI program facilitates the development of effective data-based solutions to emerging clinical challenges, not only resolving them but also ensuring the sustainability of the changes over time.
The home-based PD program also demonstrated its effectiveness and resilience in the context of natural disasters and other contingencies, such as Hurricane Maria (2017) or the SARS-CoV-2 epidemic, where the uninterrupted provision of dialysis supplies guaranteed patient safety and continuity of their therapy despite widespread disruptions in the healthcare supply chain. 24
As in many countries around the world, the Dominican healthcare system faces an escalating burden due to the growing prevalence of chronic conditions such as DM, HTN, and CKD. Without a doubt, one of the greatest challenges for health systems will be securing resources to implement health care policies and models focused on preventing predisposing diseases for CKD as DM and HTN but also ensuring the coverage of the population already requiring dialysis. It will be necessary to identify the proportion of patients by dialysis modality (HD/PD), based on the cost of providing the therapy, outcomes, economic considerations (time on PD therapy, hospitalizations), as well as return to productive work and quality of life. Achieving universal access to KRT must remain a strategic priority.25,26
A parallel challenge involves the availability of adequately trained healthcare professionals, particularly in PD. Substantial gaps exist in nephrology training programs, where PD often receives limited emphasis. Most medical residency curricula do not offer robust training or access to specialized PD facilities, restricting hands-on experience to the in-patient setting. In the field of nursing, the gap is even more pronounced, as there are currently no postgraduate training programs or specialization tracks in nephrology nursing. Similarly, professionals in nutrition, psychology, and social work lack access to local training pathways focused on CKD management and dialysis therapies, limiting the development of interdisciplinary expertise critical for optimal patient care. Addressing these training gaps is essential to sustain program expansion and preserve quality standards. 27
Regarding CAPD program, the most important challenge is moving forward to ensure the systematic and uninterrupted application of processes and protocols to positively impact patients clinical outcomes. Although outcome indicators have shown a positive trend over time, there are still opportunities for improvement. The introduction of low-glucose solutions, the widespread use of APD (in pediatric and adult patients) with advanced remote monitoring, the integration of body composition analysis and volume control, and the implementation of continuing education programs are expected to further strengthen the PD program. These innovations have the potential to generate even better outcomes than those achieved during the past decade. 27
Over its first decade, the national PD program in the DR achieved consistent and measurable progress. PD coverage increased from 6.5% of dialysis patients in 2011 to 22.4% in 2024, supported by the consolidation of seven centers and standardized clinical protocols. The peritonitis rate declined from 0.8 to 0.13 episodes per patient-year, and transfers to hemodialysis due to infection decreased notably, reflecting the impact of multidisciplinary monitoring and continuous quality improvement. Broader data on technique survival are being collected through the national PD registry and will be analysed in future evaluations of long-term program outcomes.
Building upon these achievements, the next objectives include the nationwide implementation of low-glucose and biocompatible solutions, the expansion of APD with integrated remote monitoring systems, and the adoption of advanced tools for body composition analysis and volume management. The program also aims to strengthen continuous education and training for nephrology and nursing teams, ensuring the sustainability of these improvements and the continued delivery of equitable, patient-centered care.
This study has several limitations. Catheter-related infections and microbiological data, including culture-negative peritonitis, were not systematically documented in the national registry, particularly during the early phases of the program. As a result, the calculated peritonitis rate may underestimate the true incidence of PD-associated peritonitis, preventing reliable estimation of infection-related outcomes.
Information on the use of incremental and assisted PD was also not routinely captured. Although these modalities were used selectively according to clinical judgment and patient needs, the absence of uniform documentation limited the ability to analyze their frequency or clinical impact. Residual kidney function was evaluated when clinically indicated. Urine output was typically estimated on a monthly basis through patient self-report. However, the frequency of these measurements and the specific metrics used were not consistently recorded across centers, which prevented a reliable quantitative analysis.
Finally, despite the national scope and large cohort, the retrospective design and variation in documentation practices across centers restricted the possibility of performing more advanced analyses, including a detailed evaluation of technique survival. These limitations should be considered when interpreting the findings.
The 10-year evaluation of the national PD program in the DR demonstrates that a standardized, multidisciplinary and quality-oriented model of care can substantially expand access to KRT and improve clinical outcomes in a middle-income context.
These achievements highlight the effectiveness of integrating management systems, structured follow-up, and continuous quality improvement processes within a national framework. The Dominican experience provides a scalable reference model for the implementation of sustainable, home-based PD programs in comparable healthcare contexts.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608261452388 - Supplemental material for Ten-year implementation of a National Peritoneal Dialysis Program in the Dominican Republic: A retrospective study
Supplemental material, sj-docx-1-ptd-10.1177_08968608261452388 for Ten-year implementation of a National Peritoneal Dialysis Program in the Dominican Republic: A retrospective study by Sergio Óscar Hernández Ordóñez, Erwin Iván Campos Echavarría, Elianny Sarina Polanco Brazoban, Zulma Bolena Lara Mayorga, Miguel ángel Cuevas Budhart, José Carolino Divino-Filho, Janny Katherine, Alexandra Encarnación Ogando, Yocasta Lara Hernández and Alfonso Ramos-Sánchez in Peritoneal Dialysis International
Supplemental Material
sj-docx-2-ptd-10.1177_08968608261452388 - Supplemental material for Ten-year implementation of a National Peritoneal Dialysis Program in the Dominican Republic: A retrospective study
Supplemental material, sj-docx-2-ptd-10.1177_08968608261452388 for Ten-year implementation of a National Peritoneal Dialysis Program in the Dominican Republic: A retrospective study by Sergio Óscar Hernández Ordóñez, Erwin Iván Campos Echavarría, Elianny Sarina Polanco Brazoban, Zulma Bolena Lara Mayorga, Miguel ángel Cuevas Budhart, José Carolino Divino-Filho, Janny Katherine, Alexandra Encarnación Ogando, Yocasta Lara Hernández and Alfonso Ramos-Sánchez in Peritoneal Dialysis International
Footnotes
Acknowledgements
Margarita Flores, Patricia Mosqueda, Vanessa Duran, Yenifer Collado, Marcia Abreu. (Macrotech Renal Program). Luz Dalia Rodriguez (Assitant Coordinator of Nephrology SNS). Nairobi Madé (Coordinator of High-Complexity Hospitals SNS). Ankia Mora, Franklin Mena, (PDC Robert Reid Cabral Hospital). Solangel Ramirez, Ada Rodriguez, Hector Martinez, Celso Campusano (PDC Moscoso Puello Hospital). Yenni Peguero Baez, Jancarlos Duran y Cesar Esquea (PDC Padre Billini Hospital). Maximo Suero, Elisenit Romero, (PDCTaiwan Hospital). Giovanni Damaso, Sandra Rodriguez (PDC Musa Hospital). Rosa Castillo, Lorayne Tejada, Bianka Samuel Peralta, Jaqueline Zorrilla, (PDC Cabral y Baez Hospital). Dra. Aquilidis Then, Arlette Toribio. (PDC San Vicente de Paul Hospital)
ORCID iDs
Ethical considerations
Not applicable. This is a programmatic report based on aggregated, identified data and does not involve human subjects or require ethics committee approval.
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contributions
Conception (AR, SH, EC), drafting (all authors), critical review (AR, SH, EC, JD, MC), and final approval of the manuscript (AR, SH, EC, MC). ZL and EP additionally contributed to data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Macrotech Farmacéutica.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ARS, SOH, EIC, ZBL, ESP: Employees of Macrotech. In addition, SOH reports funding for academic activities, and ARS declares ownership of Baxter shares.
AEO, YLH, MACB, JCD: Declare no conflicts of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.