
Abstract
Background
The aim of this study was to clarify the current status of assisted peritoneal dialysis (PD) implementation in Japan.
Methods
A nationwide, cross-sectional, questionnaire survey was conducted by the Working Group of the Academic Committee of the Japanese Society for Peritoneal Dialysis. A paper-based questionnaire of 22 items was developed based on a literature review and clinical experience. The questionnaires were sent to all 310 facilities that were members of the Japanese Society for Peritoneal Dialysis (JSPD).
Results
Responses were received from 209 facilities (response rate 67.4%). It was found that assisted PD is already being implemented in approximately two-thirds of PD facilities, accounting for 15.9% of all PD patients. Cognitive decline and muscle weakness were the leading reasons for starting assisted PD. Family members, particularly spouses and adult children, were the main caregivers in this cohort, either alone or in collaboration with visiting nurses; cooperation with general practitioners was relatively limited. Facilities with a large number of PD patients made use of collaboration with visiting nurses and respite care facilities, remote monitoring, and medical care-specific social networking sites.
Conclusion
This nationwide survey demonstrates that assisted PD is widely practiced in Japan and plays a critical role in sustaining PD therapy for elderly and functionally impaired patients. However, substantial heterogeneity in implementation and insufficient integration with broader medical and social care systems remain major challenges. Addressing these issues through standardization, multidisciplinary collaboration, and policy reform will be essential to meet the needs of Japan's rapidly aging dialysis population.
Introduction
In Japan, while nearly 340,000 patients receive hemodialysis (HD), only about 10,000 undergo peritoneal dialysis (PD), representing a markedly lower prevalence (approximately 3% of all dialysis patients) compared with Western countries. 1 Although there is no difference in patient costs among dialysis modalities, the low utilization of PD relative to HD is likely attributable to a healthcare system that favors in-center HD, insufficient provision of information by healthcare professionals, and limitations in home care support systems. The widespread availability of HD facilities, along with transportation services, also contributes to this situation.
The rapid aging of the population has led to a notable increase in the ageing of both patients starting dialysis and the overall dialysis patient population. According to the annual survey of the Japanese Society for Dialysis Therapy Renal Data Registry at the end of 2022, the average age of new dialysis patients is increasing every year, and the proportion of elderly dialysis patients aged 70 years or older is also steadily increasing. 1 This trend is observed not only among HD patients but also among those receiving PD. Elderly dialysis patients may have difficulty managing their own dialysis therapy due to factors such as declining physical function, cognitive impairment, visual impairment, and impaired manual dexterity.
PD is an important option for home dialysis therapy, both in terms of maintaining patients’ quality of life (QOL) and making effective use of medical resources. However, because patients must perform routine procedures such as bag exchanges and exit site care, it has been pointed out that this can be a major barrier to continuing PD in elderly patients with reduced self-care abilities. 2 Given this background, “assisted PD,” in which medical professionals, caregivers, and family members assist with PD procedures on behalf of the patient, has become common, particularly in Europe and Canada.3–6
Meanwhile, in Japan, the idea that PD is “home medical care performed by the patients themselves” has historically been emphasized, and bag exchanges by third parties have not been publicly permitted. As a result, the institutionalization and standardization of assisted PD have not progressed sufficiently, and actual implementation is currently left to the discretion and ingenuity of each facility. In recent years, there has been discussion about the need for limited assistance by family members, and related academic societies are working to establish legal frameworks and operational guidelines, but the actual situation on a national scale is far from clear.
In particular, there have been very few reports that systematically summarized the extent to which assisted PD is practiced in Japan, the patient background characteristics that lead to its selection, the breakdown of caregivers, the type of assistance provided, and operational issues. 7 With an expected increase in elderly dialysis patients in the future, clarifying the current state and issues of assisted PD will provide important basic information for expanding PD therapy options and achieving patient-centered kidney replacement therapy.
In this study, therefore, with the aim of clarifying the status of assisted PD implementation in Japan, a questionnaire survey targeting medical institutions involved in PD care was conducted, and the current situation of assisted PD patients, details of treatment methods, support systems, and medical collaboration were examined.
Materials and methods
Study design and setting
This nationwide, cross-sectional, questionnaire survey was conducted by the Working Group of the Academic Committee of the Japanese Society for Peritoneal Dialysis (JSPD) to clarify the current status of assisted PD in Japan. The purpose of JSPD is to promote medical care, academic culture, and the welfare of the nation by carrying out activities related to the advancement, development, and dissemination of medical treatment and research related to kidney failure and PD therapy. The survey period was from April 1 to June 30, 2025. The questionnaires were sent to all 310 facilities employing physicians affiliated with JSPD. Responses were submitted by mail, returning the questionnaire by mail was considered consent to participate in the study, and no financial incentives were offered to respondents. Each facility was instructed to submit one response, and completion by a chief nephrologist was preferred. Individual patient-level information and personal identifiers were not collected.
Questionnaire
Members of the JSPD Research Working Group developed the questionnaire based on a literature review and clinical experience and conducted the survey. The paper-based questionnaire consisted of 22 items (total number of PD patients, number of PD patients aged 65 years or older, number of PD patients aged 75 years or older, number of assisted PD patients, the person assisting, the family member assisting, reason for assisting, dialysis modality, dialysis prescription and treatment frequency, utilization of long-term care insurance, collaboration with general practitioners and visiting nurses, use of respite facilities, application of remote monitoring, and use of medical care-specific social networking sites [SNSs]). The detailed content of the questionnaire is shown in Table 1. Responses were requested by entering a numerical value or checking a checkbox. If discrepancies were found in the number of responses or if the numbers were difficult to read, the facility was contacted, and the data were corrected.
Content of the questionnaire.
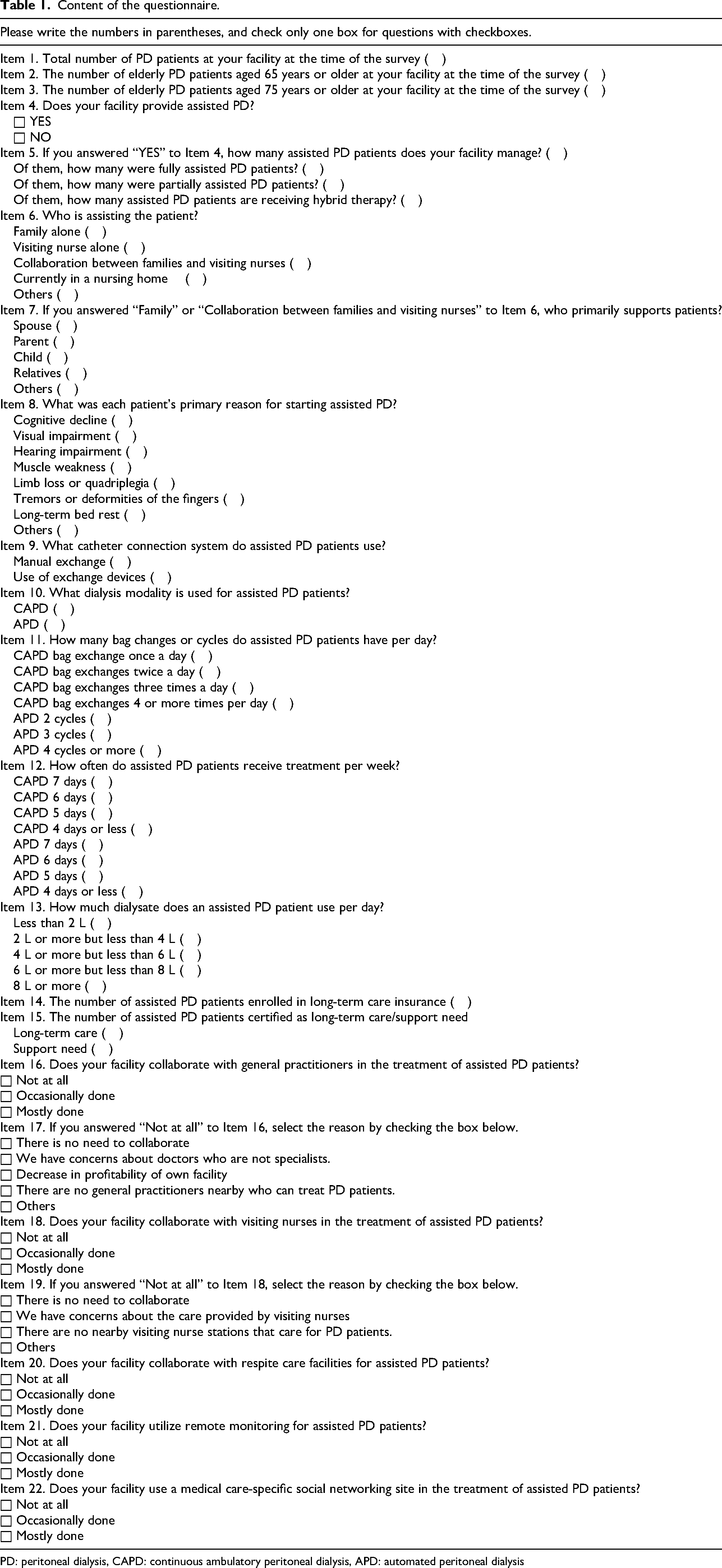
PD: peritoneal dialysis, CAPD: continuous ambulatory peritoneal dialysis, APD: automated peritoneal dialysis
Ethical issues
This study was conducted in accordance with the Declaration of Helsinki. The survey collected respondents’ names, affiliations, and email addresses. Therefore, ethical approval was obtained from the JSPD Ethics Committee (Reference number: JSPD2025-1). The JSPD Ethics Committee is registered with the Ministry of Health, Labor and Welfare's Research Ethics Review Committee Reporting System (https://rinri.mhlw.go.jp/).
Statistical analysis
The data obtained are expressed as median and interquartile range (IQR) values or the number (n) and proportions (%). Facilities treating assisted PD patients were divided into two groups based on the median number of assisted PD patients, and trends in proportions for ordered categorical variables were tested using the Cochran–Armitage trend test. All analyses used SPSS Statistics (version 29.0.2.0; IBM Japan, Tokyo, Japan). A p-value <0.05 was considered significant.
Results
Responses were received from 209 facilities, with a response rate of 67.4% (nine of these facilities were not managing PD patients at the time of the survey). At the time of the survey, the total number of PD patients was 4854, of which 2743 (56.5%) were aged 65 years or older, and 1486 (30.6%) were aged 75 years or older. Of the 200 facilities managing PD patients, 132 (66.0%) provided assisted PD, with 771 patients receiving assisted PD, accounting for 15.9% of the total. The median number of PD patients at the 132 facilities was 20 (IQR 12, 42), and the median number of assisted PD patients per facility was 3 (IQR 1.0, 6.0). Furthermore, of the facilities managing assisted PD, 121 were hospitals, and 11 were clinics. The percentage of assisted PD patients among all PD patients varied greatly depending on the facility, with the lowest rate being 2.5% and the highest rate being 100% (the number of assisted PD patients per facility ranged from a minimum of 1 to a maximum of 70). Among these patients, 363 (47.1%) received fully assisted PD, 408 (52.9%) received partially assisted PD, and 161 (20.9%) underwent hybrid therapy combining PD with HD once or twice weekly.
Most primary caregivers were family members alone (326 patients), followed by 217 patients who worked in collaboration with family members and visiting nurses, and 148 patients who worked with visiting nurses alone (Figure 1). Of the family members assisting, the largest number were spouses (55.5%), followed by children (34.5%); the others (10%) were parents, siblings, and relatives.
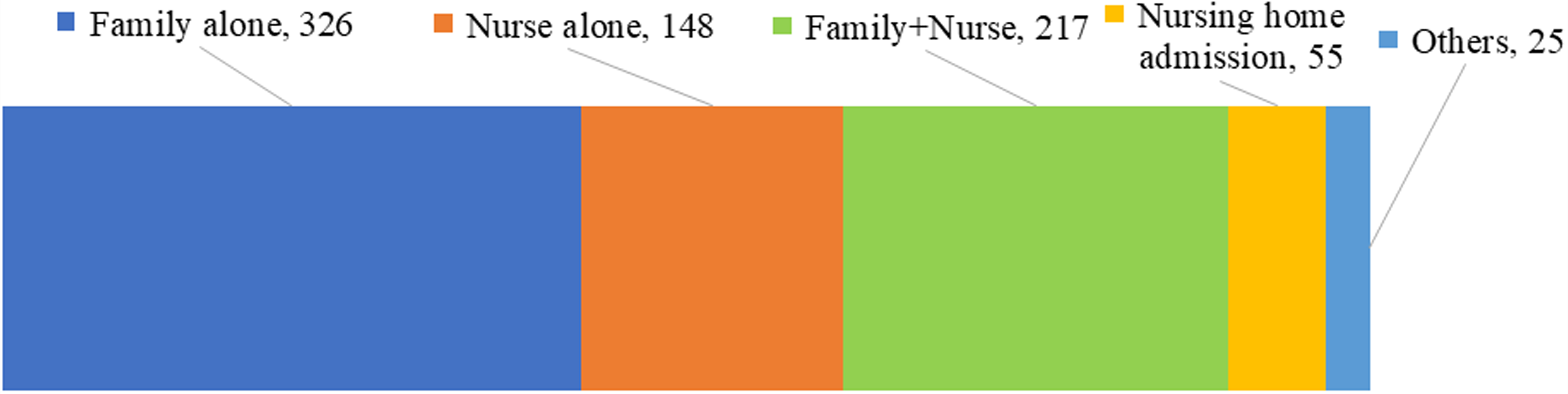
Breakdown of primary caregivers for 771 assisted PD patients.
The most common reason for starting assisted PD was cognitive decline (327 patients), followed by muscle weakness (202 patients) (Figure 2). Other factors included mental illnesses such as schizophrenia and panic disorder, the request of the family, or the discretion of medical professionals.
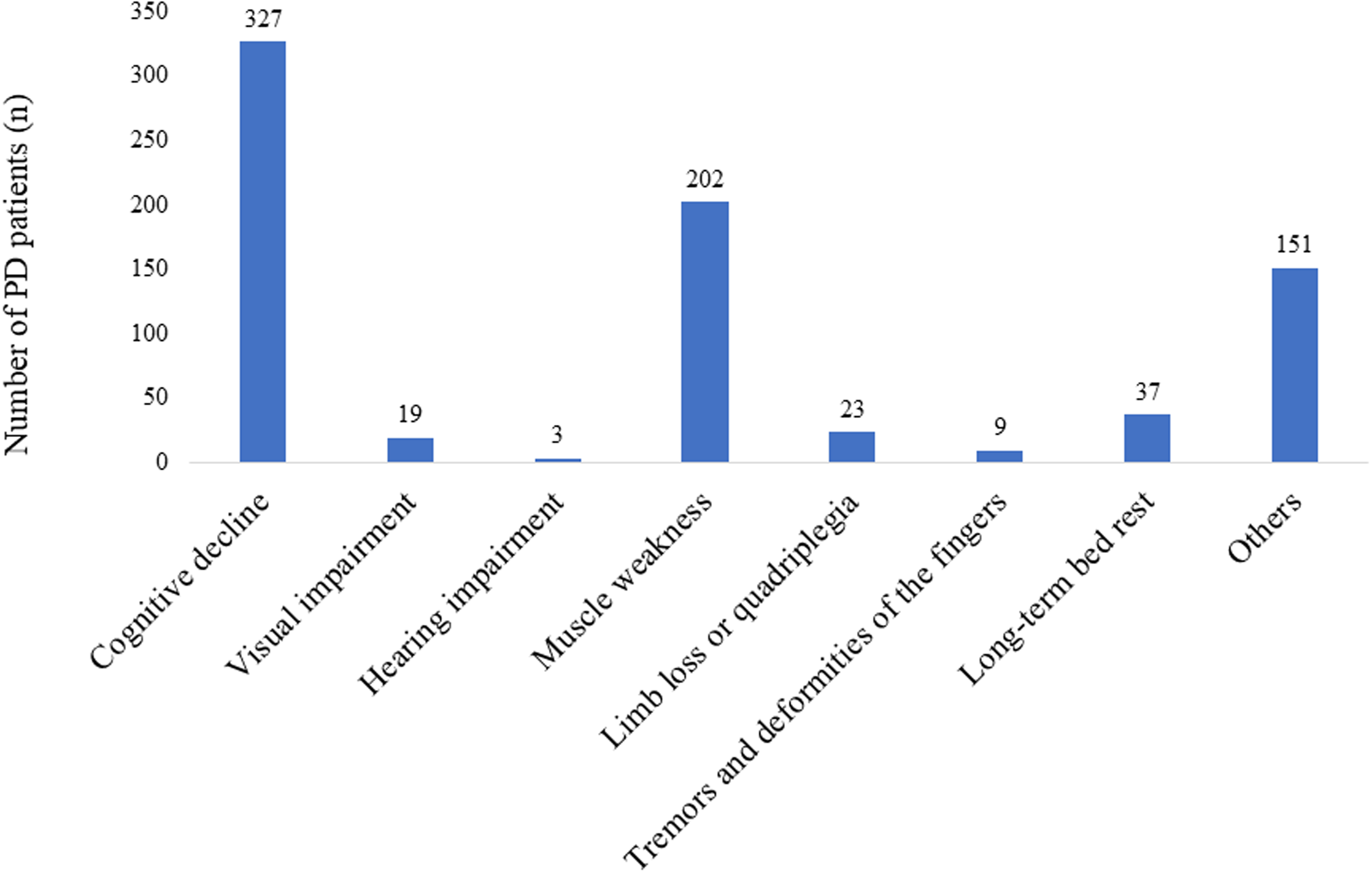
Reasons for assisted PD.
Of the 771 assisted PD patients, 547 (70.9%) chose continuous ambulatory peritoneal dialysis (CAPD), and 224 (29.1%) chose automated peritoneal dialysis (APD). In addition, 512 patients (66.4%) used exchange devices (sterile devices with ultraviolet irradiation or sterile devices with thermal bonding). The most common number of bag changes per day for CAPD was two or three (Supplemental Figure 1), whereas the most common number of cycles for APD was three or more than four (Supplemental Figure 2). The most common weekly treatment frequency was 7 days for both CAPD and APD (85.9%), and few patients had days off PD (Supplemental Figure 3). Daily dialysate usage was 2 L to less than 4 L in 243 patients, 4 L to less than 6 L in 224 patients, and 6 L to less than 8 L in 162 patients (Supplemental Figure 4).
A total of 427 (55.4%) assisted PD patients were enrolled in long-term care insurance, and most of them had been certified as requiring long-term care (79.8%); the number of assisted PD patients who were certified as having support need was low (83, 20.2%).
Compared with collaboration with visiting nurses (86.4%), collaboration with general practitioners (56.1%) was low. The most common reason given for not coordinating between visiting nurses and general practitioners was that there was no need for it. Furthermore, few facilities were using remote monitoring, respite care facilities, or medical care-specific SNSs when treating assisted PD patients.
Subsequently, the facilities were divided into two groups based on the median number of PD patients, and the relationships with collaboration and the use of information transmission tools were examined. It was found that facilities with a larger number of assisted PD patients were significantly more likely to collaborate with visiting nurses and respite care facilities and to use medical care-specific SNSs and remote monitoring (Table 2).
Collaborate with general practitioners.
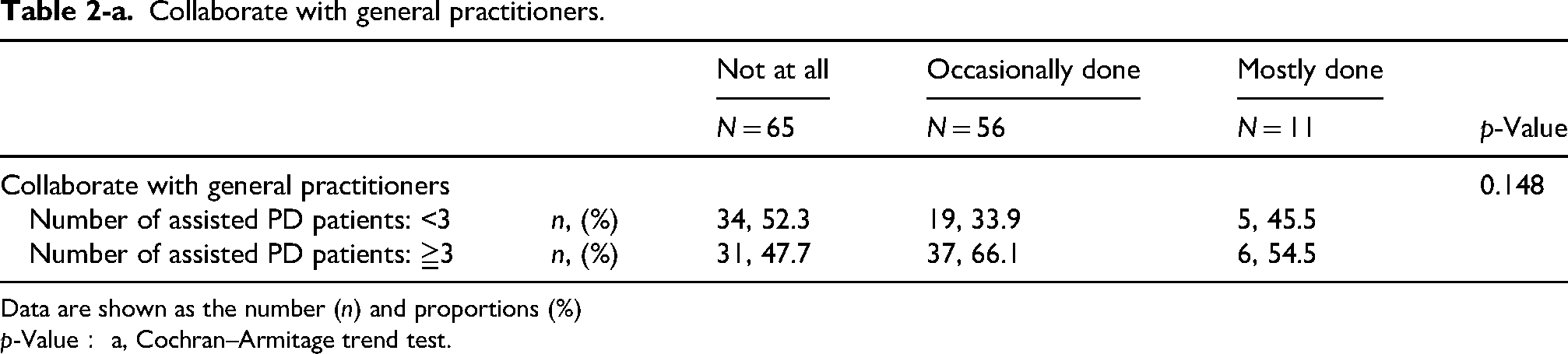
Data are shown as the number (n) and proportions (%)
p-Value: a, Cochran–Armitage trend test.
Collaborate with visiting nurses.
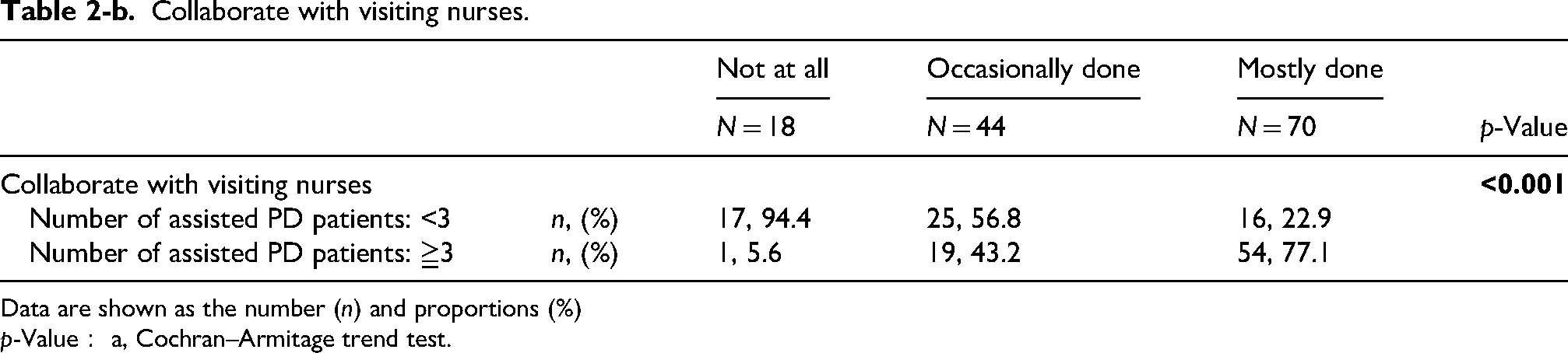
Data are shown as the number (n) and proportions (%)
p-Value: a, Cochran–Armitage trend test.
Collaborate with respite care facilities.
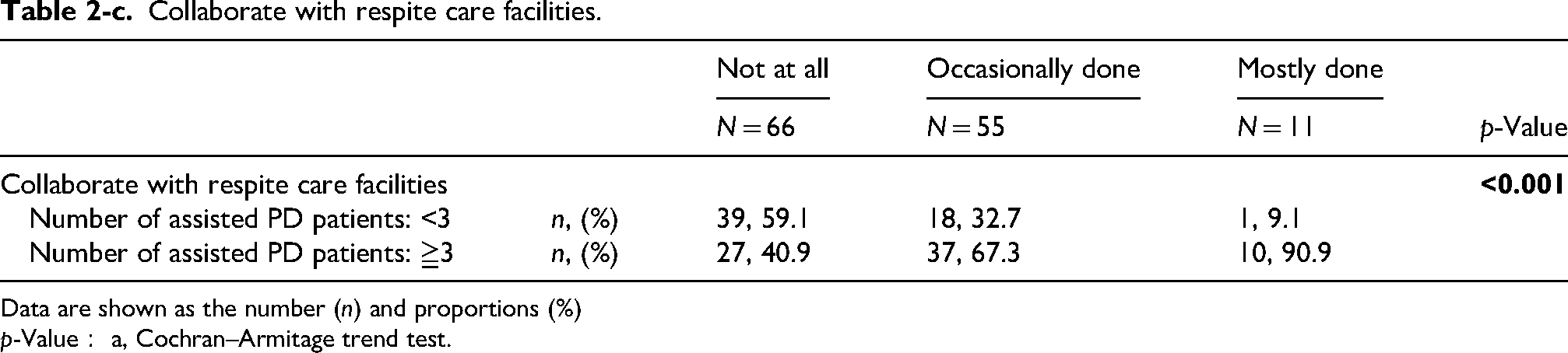
Data are shown as the number (n) and proportions (%)
p-Value: a, Cochran–Armitage trend test.
Utilize remote monitoring.
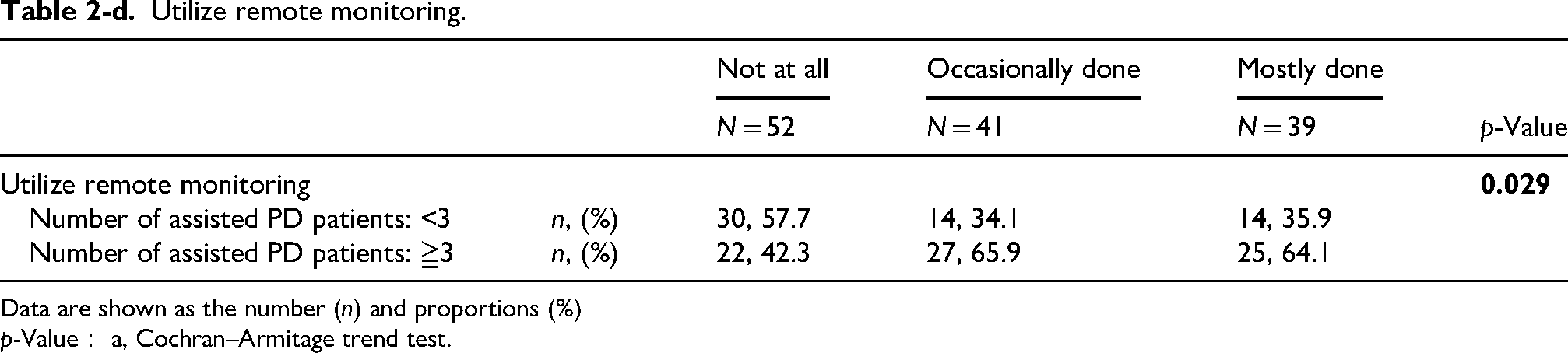
Data are shown as the number (n) and proportions (%)
p-Value: a, Cochran–Armitage trend test.
Utilize medical care-specific social networking sites.
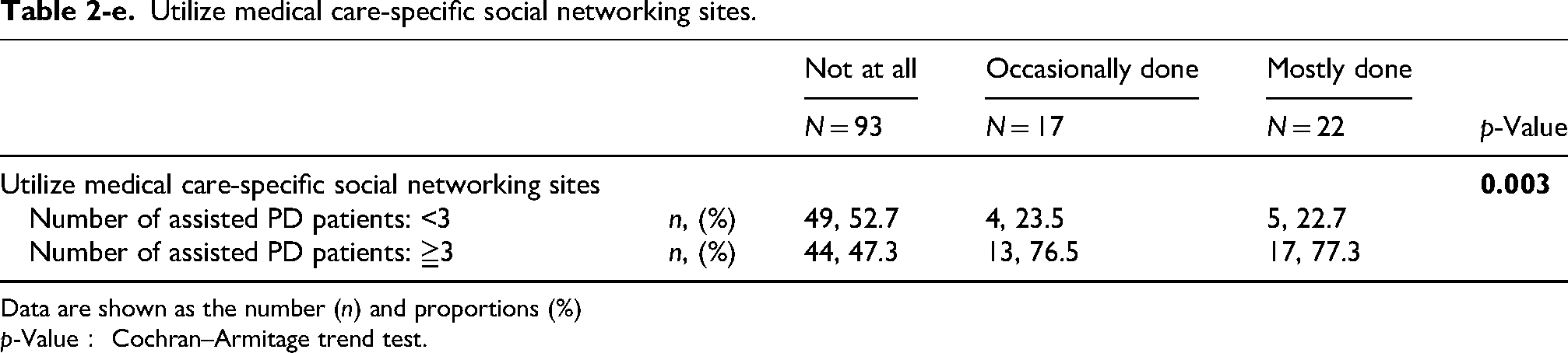
Data are shown as the number (n) and proportions (%)
p-Value: Cochran–Armitage trend test.
Discussion
In this nationwide questionnaire survey, the current status, characteristics, and challenges of assisted PD in Japan were clarified. It was found that assisted PD is already being implemented in approximately two-thirds of PD facilities, accounting for 15.9% of all PD patients, despite the lack of formal institutionalization and standardized operational frameworks. These results suggest that assisted PD has emerged as an essential modality to sustain PD therapy in the rapidly growing elderly dialysis population in Japan.
In 2013, a questionnaire survey was conducted regarding the current situation of assisted PD patients in Japan. 7 It found that 173 facilities managed assisted PD patients, and the number of assisted PD patients was 474, accounting for 9.7% of all PD patients (4889 patients). Considering that the current survey targeted roughly the same number of PD patients, the number of facilities managing assisted PD patients and the number of patients is clearly increasing; over the past 12 years, the number of facilities has increased by approximately 2.7 times, and the number of patients has increased by 1.6 times. According to the Position Paper for the International Society for Peritoneal Dialysis (ISPD) on assisted PD, the prevalence of assisted PD among all PD patients varies greatly by country, ranging from 8% (Sweden) to 45% (France). 8 Given that the aging of dialysis patients in Japan is significant compared with other countries where assisted PD is practiced, the current prevalence of assisted PD may be low. In addition, the wide inter-facility variation observed in this study suggests that assisted PD in Japan remains highly dependent on local practices rather than standardized national frameworks.
Consistent with prior reports,9,10 cognitive decline and muscle weakness were the leading reasons for starting assisted PD. These findings indicate that assisted PD functions primarily as a strategy to maintain PD in patients who would otherwise be forced to discontinue home dialysis due to declining self-care capacity. Notably, more than half of the patients received partial assistance, suggesting that assisted PD in Japan is often implemented as a flexible, stepwise support model rather than full substitution of self-care. This approach aligns with international recommendations emphasizing the preservation of patient autonomy whenever possible. 8 However, there were also cases in which assisted PD was started at the request of the family or the discretion of medical professionals. From the perspective of the appropriate allocation of medical resources in Japan, it is necessary to discuss which specific patients should be prioritized for assisted PD. Furthermore, the present questionnaire did not specifically collect data on whether assisted PD was initiated as the initial modality or after transition from HD. In clinical practice in Japan, assisted PD is often introduced when patients experience a decline in self-care ability, either during ongoing PD or at the time of PD initiation, whereas transition from HD to assisted PD is relatively uncommon. This issue is particularly relevant in relation to residual kidney function and the feasibility of less intensive PD regimens. Therefore, further studies are warranted to clarify the optimal timing of assisted PD initiation.
Family members, particularly spouses and adult children, were the main caregivers in this cohort, either alone or in collaboration with visiting nurses. This contrasts with reports from Europe and Canada, where visiting nurses or paid caregivers often serve as the primary providers of assistance. Unlike in some other Asian countries, assistance by domestic workers is not formally recognized within the Japanese healthcare system. High reliance on Japanese family caregivers reflects cultural norms, as well as structural constraints in home nursing resources and the medical reimbursement system. Though family involvement is a key facilitator of home dialysis, previous studies have highlighted the substantial physical and psychological burden placed on caregivers.11,12 The findings of the present study highlight the need to develop sustainable support systems for family caregivers.
In Japan, visiting nurse services are generally covered under the public health insurance and long-term care insurance systems, depending on patient eligibility (e.g., intractable disease status, activities of daily living, cognitive function, and level of care required). Their responsibilities include assistance with bag exchange procedures, exit-site care, and monitoring of patients’ clinical conditions. However, insurance coverage may not fully support the cost of daily bag exchanges. In such cases, family members may be required to assist. For example, in PD patients requiring the highest level of care, daily CAPD (two exchanges per day) or APD may exceed the scope of insurance coverage, thereby imposing out-of-pocket costs on patients.
Several challenges remain. There is currently no standardized training program for visiting nurses specifically focused on assisted PD care, and the level of experience may vary across facilities. In addition, coordination among visiting nurses, nephrologists, and general practitioners is not always well established. Reimbursement structures and workforce availability may also influence the extent to which healthcare professionals can be involved in assisted PD. Addressing these issues will be essential to ensure the safe and sustainable implementation of assisted PD.
More than half of the assisted PD patients in the present study were certified under the long-term care insurance system, reflecting significant care dependency. However, it has been suggested that assisted PD is less frequently implemented for patients who are certified as “requiring assistance” (a condition requiring a lower assistance level than long-term care). This suggests that the introduction of assisted PD is delayed. Timely implementation of assisted PD has been proposed as a strategy to prevent unplanned transition to in-center HD and reduce caregiver stress. 8
Although CAPD was chosen more frequently than APD in assisted PD patients, APD was used in approximately 30% of cases. APD may reduce the burden on caregivers and facilitate assisted PD, especially in elderly patients. 13 The relatively lower use of APD in Japan may reflect concerns regarding device management, alarm handling, or limited experience of caregivers and visiting nurses. The high prevalence of catheter connection systems is consistent with prior studies showing that assistive devices can improve feasibility and safety in elderly PD patients.14,15 Despite assisted PD, most patients underwent PD seven days per week, with few days off PD. These data suggest that, even in frail patients, dialysis adequacy has been prioritized. This is in contrast to new concepts such as incremental PD and palliative PD, which have been proposed in recent years to reduce the treatment burden in elderly, frail patients.16,17 The absence of standardized guidance on PD prescription adjustment for assisted PD patients or frail PD patients may partly explain this practice pattern. Future studies should explore whether more individualized, goal-directed PD prescriptions could further improve QOL in assisted PD patients.
Although collaboration with visiting nurses was common, cooperation with general practitioners was relatively limited in Japan. In their review, Saeed et al. stated that, to optimize outcomes for elderly dialysis patients, it is crucial for primary care clinicians and nephrologists to collaborate, promote shared decision-making, and provide patient-centered, coordinated care. 18 In September 2020, the JSPD collaborative certified physician system was launched to develop leaders in promoting PD through regional medical collaboration (https://www.jspd.jp/certified/), and many general practitioners have been certified. It is hoped that this initiative will benefit even more assisted PD patients.
This study showed limited use of remote monitoring, respite care services, and medical care-specific SNSs in the management of assisted PD patients. Furthermore, facilities with a large number of PD patients made use of collaboration with visiting nurses and respite care facilities, remote monitoring, and medical care-specific SNSs. There is growing evidence that telemedicine and respite care can enhance the safety and sustainability of home dialysis.19,20 Effective use of these services has the potential to ensure patient safety and reduce anxiety and burden for caregivers. Home care support has been reported to significantly increase the number of patients who can be offered PD, 21 which is consistent with the findings of the present study.
Taken together, the present findings suggest that assisted PD is already an indispensable component of PD care in Japan, but it remains insufficiently standardized. International guidelines and position papers increasingly recognize assisted PD as a legitimate and necessary modality for elderly and disabled patients.8,22 Furthermore, the cost of in-center HD has been demonstrated to remain higher than that of assisted PD, and its cost-effectiveness has also come under scrutiny. 23 Establishing clear operational guidelines, legal frameworks, and reimbursement policies, while strengthening integration with long-term care insurance and primary care, will be essential to promote equitable access and sustainable implementation of assisted PD in Japan. To address these challenges, national-level policy initiatives are needed to: (1) clarify the legal positioning of third-party assistance in PD; (2) establish standardized operational guidelines; (3) provide education for caregivers; (4) expand reimbursement for home nursing and respite services; and (5) promote the use of information and communication technology (ICT) and remote monitoring.
This study has several limitations. First, the data were collected at the facility level and were based on self-reported questionnaire responses, without external validation using objective data sources such as patient registries or medical records. Therefore, concerns remain regarding the reliability of the findings. Second, patient-level data, including outcomes such as survival rates, QOL, complications, or transitions to alternative dialysis modalities, were not available in the present study. Future research should prioritize the inclusion of outcome data to provide a more comprehensive understanding of this topic. Third, because this study included only facilities employing physicians affiliated with the JSPD, the generalizability of the survey results may be limited. In Japan, most facilities providing PD have physicians affiliated with JSPD; however, some facilities without such affiliation may exist, and comprehensive data on these facilities are lacking. Therefore, the findings of this study may not fully represent the overall status of PD practice in Japan.
To address these limitations, future studies incorporating patient-level data and linkage with national registries, such as the Japanese Society for Dialysis Therapy Renal Data Registry, would be valuable to provide more robust and generalizable evidence on assisted PD.
Conclusion
This nationwide survey demonstrates that assisted PD is widely practiced in Japan and plays a critical role in sustaining PD therapy for elderly and functionally impaired patients. However, substantial heterogeneity in its implementation and insufficient integration with broader medical and social care systems remain major challenges. Furthermore, there is no standardized, systematic training program for assisted PD at the national level, and each facility conducts its own education and training. Addressing these issues through standardization, multidisciplinary collaboration, and policy reform will be essential to meet the needs of Japan's rapidly aging dialysis population.
Supplemental Material
sj-pdf-1-ptd-10.1177_08968608261457525 - Supplemental material for Current status of assisted peritoneal dialysis in Japan: A nationwide questionnaire survey
Supplemental material, sj-pdf-1-ptd-10.1177_08968608261457525 for Current status of assisted peritoneal dialysis in Japan: A nationwide questionnaire survey by Tsutomu Sakurada, Harumi Kitamura, Kohkichi Morimoto, Kyoko Kataoka, Hiroka Owaki, Chiharu Kinoshita, Saya Imai, Hiroki Ohashi, Takuo Kusumoto, Masanobu Miyazaki, Masaaki Nakayama, Hideki Kawanishi, Jun Minakuchi and Tadashi Tomo in Peritoneal Dialysis International
Footnotes
Acknowledgments
We thank all facilities for responding to the questionnaire survey.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki. The survey collected respondents’ names, affiliations, and email addresses. Therefore, we obtained ethical approval from the JSPD Ethics Committee (Reference number: JSPD2025-1). The JSPD Ethics Committee is registered with the Ministry of Health, Labor and Welfare's Research Ethics Review Committee Reporting System (![]() ).
).
Consent to participate
The individual patient-level information and personal identifiers were not collected. The responses by study participants were submitted by mail, returning the questionnaire by mail was considered consent to participate in the study.
Author contributions
TS, HK, KM, KK, HOwa, CK, SI, HOha, TK, and MM made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data. MN, HK, JM, and TT drafted the article or revised it critically for important intellectual content. All authors accept direct responsibility for the manuscript.
Consent for publication
Not applicable.
Funding statement
This work did not receive any grants from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interest
The authors disclosed conflicts of interest with respect to the research, authorship, and/or publication of this article: We have read and understood Peritoneal Dialysis International's policy on conflicts of interest disclosures. TS has received speaker honorarium from Vantive Japan, and received research grant from Terumo Corporation. KM has received speaker honorarium from Vantive Japan, Terumo Corporation, and JMS Co., Ltd MN is a medical expert specializing in clinical trials at Terumo Corporation. TT has received speaker honorarium from NIPRO Corporation, Asahi Kasei Medical Co., Ltd, Nikkiso Co., Ltd, and Vantive Japan. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available, but restrictions apply to the availability of these data which were used for the current study, and so are not publicly available. However, the data underlying this article will be shared on reasonable request to the corresponding author.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.