
Abstract
Clinical context and findings
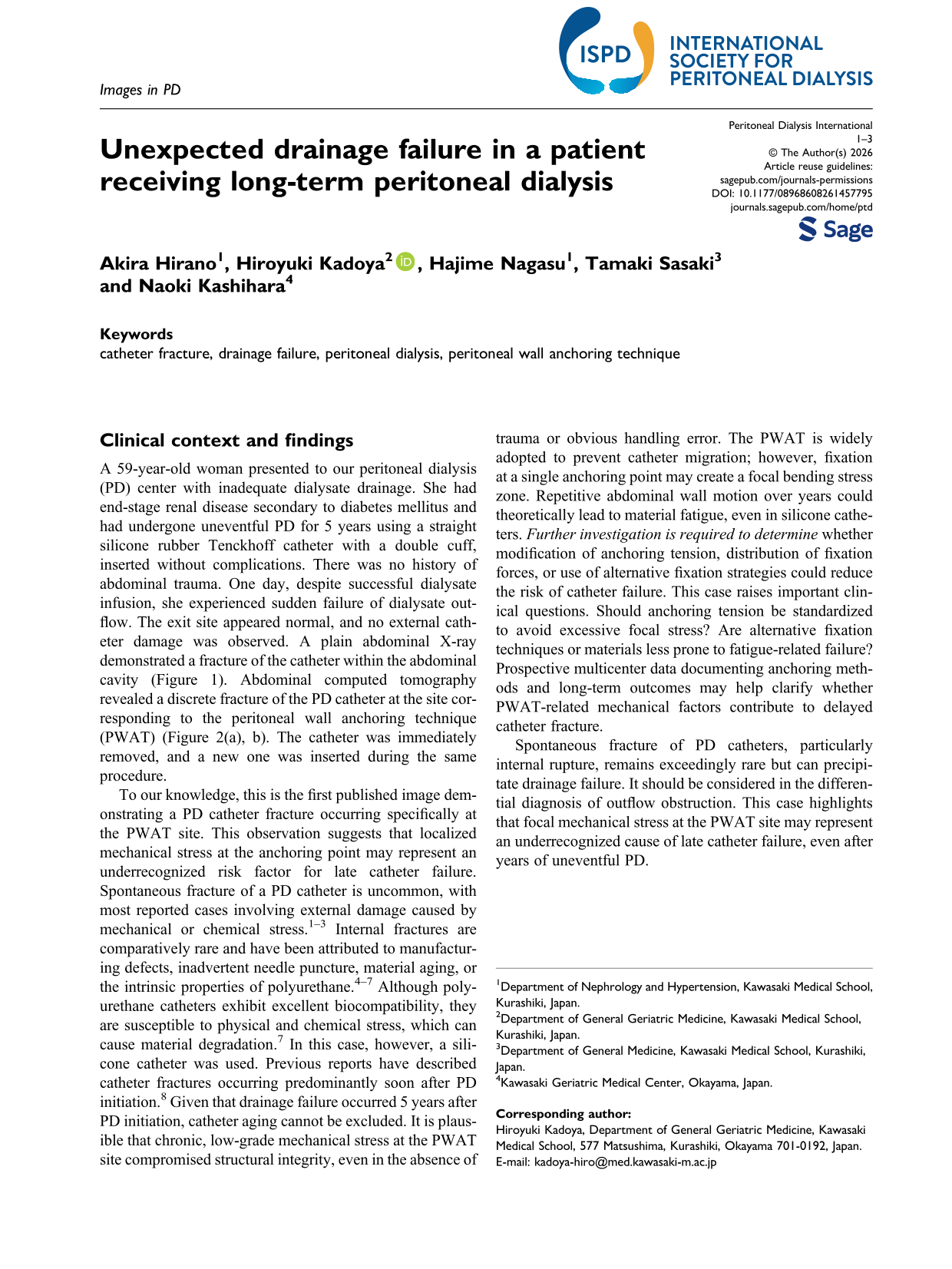
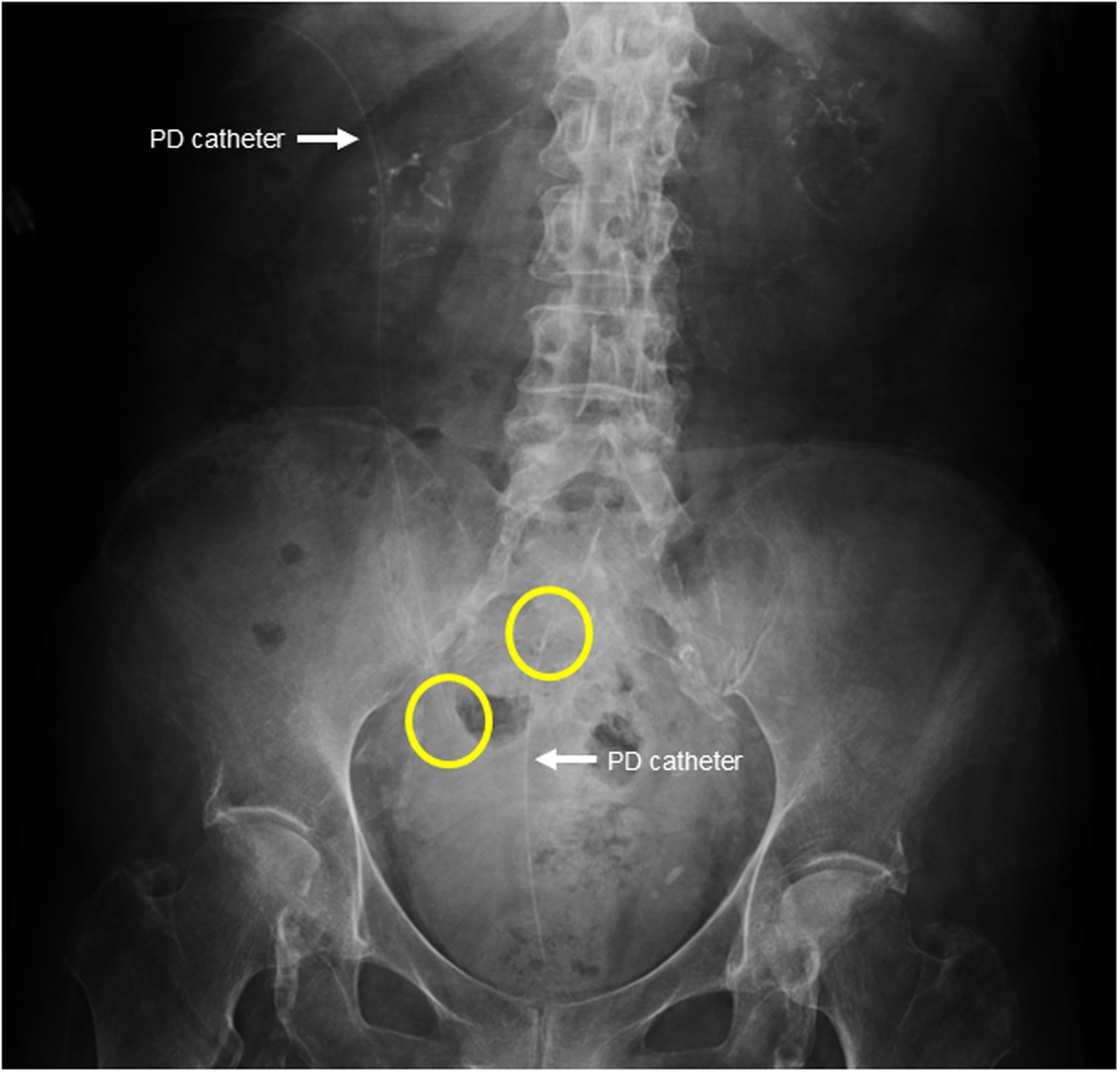
A 59-year-old woman presented to our peritoneal dialysis (PD) center with inadequate dialysate drainage. She had end-stage renal disease secondary to diabetes mellitus and had undergone uneventful PD for 5 years using a straight silicone rubber Tenckhoff catheter with a double cuff, inserted without complications. There was no history of abdominal trauma. One day, despite successful dialysate infusion, she experienced sudden failure of dialysate outflow. The exit site appeared normal, and no external catheter damage was observed. A plain abdominal X-ray demonstrated a fracture of the catheter within the abdominal cavity (Figure 1). Abdominal computed tomography revealed a discrete fracture of the PD catheter at the site corresponding to the peritoneal wall anchoring technique (PWAT) (Figure 2(a), b). The catheter was immediately removed, and a new one was inserted during the same procedure.
Abdominal plain radiograph (X-ray) demonstrating intraperitoneal disconnection of the peritoneal dialysis (PD) catheter. The arrow points to the PD catheter, and the circle highlights the catheter tip
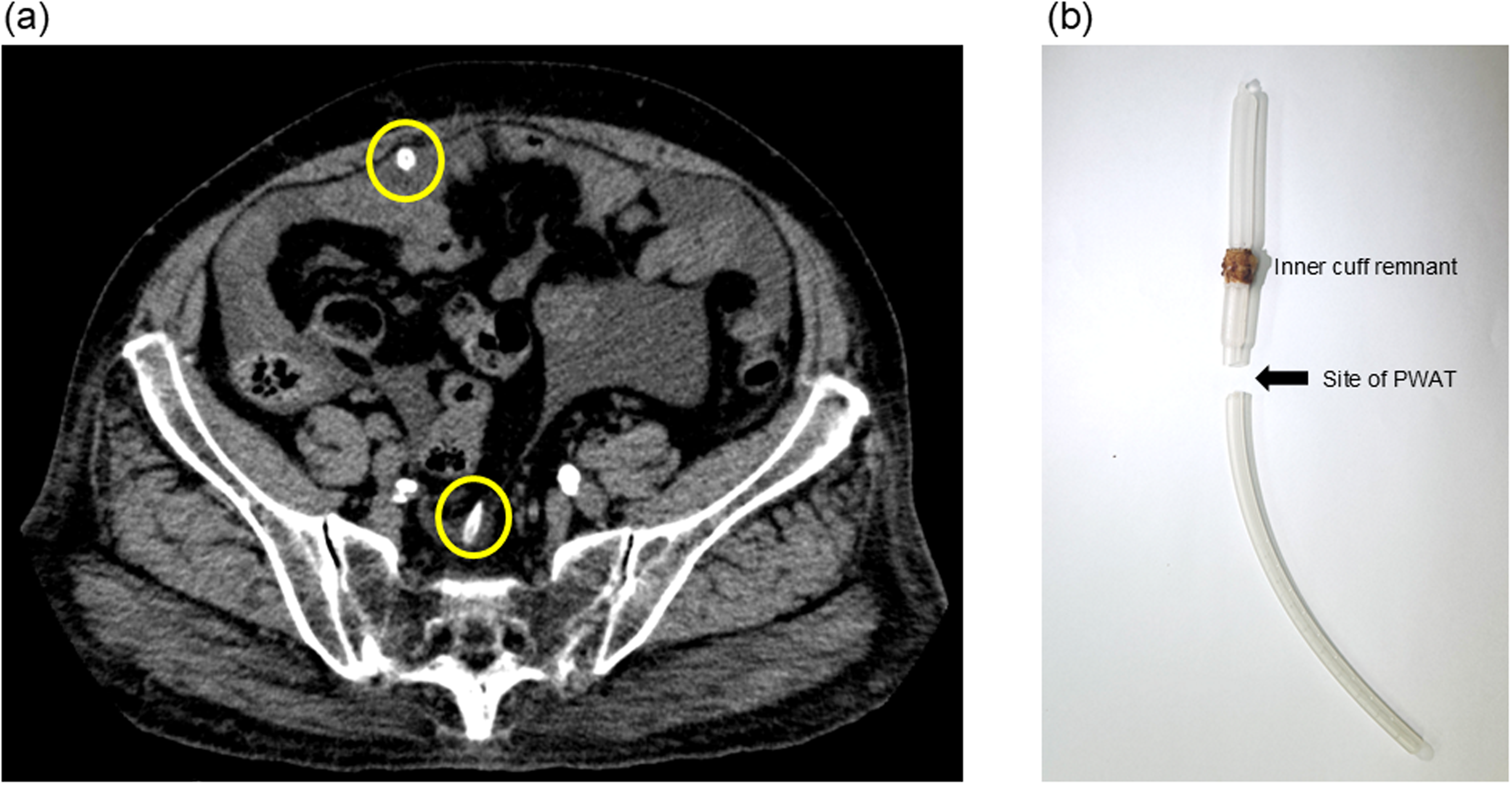
Abdominal computed tomography (CT) images demonstrating clear discontinuity of the peritoneal dialysis catheter at the peritoneal wall anchoring technique (PWAT) site. (a) Axial CT view showing separation of the proximal and distal catheter segments (circles). (b) Magnified view highlighting the fracture site adjacent to the inner cuff remnant at the PWAT anchoring point.
To our knowledge, this is the first published image demonstrating a PD catheter fracture occurring specifically at the PWAT site. This observation suggests that localized mechanical stress at the anchoring point may represent an underrecognized risk factor for late catheter failure. Spontaneous fracture of a PD catheter is uncommon, with most reported cases involving external damage caused by mechanical or chemical stress.1–3 Internal fractures are comparatively rare and have been attributed to manufacturing defects, inadvertent needle puncture, material aging, or the intrinsic properties of polyurethane.4–7 Although polyurethane catheters exhibit excellent biocompatibility, they are susceptible to physical and chemical stress, which can cause material degradation. 7 In this case, however, a silicone catheter was used. Previous reports have described catheter fractures occurring predominantly soon after PD initiation. 8 Given that drainage failure occurred 5 years after PD initiation, catheter aging cannot be excluded. It is plausible that chronic, low-grade mechanical stress at the PWAT site compromised structural integrity, even in the absence of trauma or obvious handling error. The PWAT is widely adopted to prevent catheter migration; however, fixation at a single anchoring point may create a focal bending stress zone. Repetitive abdominal wall motion over years could theoretically lead to material fatigue, even in silicone catheters. Further investigation is required to determine whether modification of anchoring tension, distribution of fixation forces, or use of alternative fixation strategies could reduce the risk of catheter failure. This case raises important clinical questions. Should anchoring tension be standardized to avoid excessive focal stress? Are alternative fixation techniques or materials less prone to fatigue-related failure? Prospective multicenter data documenting anchoring methods and long-term outcomes may help clarify whether PWAT-related mechanical factors contribute to delayed catheter fracture.
Spontaneous fracture of PD catheters, particularly internal rupture, remains exceedingly rare but can precipitate drainage failure. It should be considered in the differential diagnosis of outflow obstruction. This case highlights that focal mechanical stress at the PWAT site may represent an underrecognized cause of late catheter failure, even after years of uneventful PD.
Footnotes
Acknowledgements
The authors thank the patient and her family for their contribution to this study. The authors also thank Editage for English language editing. This study received no funding support.
Ethics approval and consent to participate
The case study was conducted in accordance with the principles of the Declaration of Helsinki.
Author contributions
HK drafted the manuscript. AH and HK managed PD-associated peritonitis. HN, TS, and NK conceived and designed the work, interpreted the data, and critically reviewed the manuscript. All authors read and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosure
All authors declare no competing interests.
Patient consent statement
Written informed consent was obtained from the patient for the publication of this case report. Ethical approval for publication was deemed unnecessary by Kawasaki Medical School.