
Abstract
Background
The Standardized Outcomes in Nephrology—Peritoneal Dialysis (SONG-PD) initiative identified core outcomes for patients receiving peritoneal dialysis (PD). However, this study included very few Japanese participants, raising concerns whether their findings applied to Japanese patients. This study aimed to identify important factors in the choice of dialysis modality from the SONG-PD list.
Methods
Participants comprised 199 patients receiving dialysis (mean age, 61 ± 12 years; male, 71.9%) who initiated PD between January 1, 2018, and September 30, 2024. Important factors in the choice of dialysis modality were investigated using a questionnaire and clinical data were obtained from medical records.
Results
Important factors with high voting percentages included “Flexibility with time (ability to schedule dialysis according to one's day)” “Life participation (ability to work, study, do home duties),” “Mobility/fitness (ability to move without assistance, and to train to achieve physical goals)” and “Ability to travel.” These findings, except for “Life participation,” differed from the core outcomes identified in the SONG-PD study. Subgroup analysis showed that “Death” had a higher voting percentage in patients with diabetic nephropathy. Additionally, important factors varied partly depending on age and employment status.
Conclusion
Important factors in the choice of dialysis modality among Japanese patients initiating PD, particularly regarding flexibility, daily activities, mobility, and travel, highlight specific needs that may not be fully captured by the internationally derived SONG-PD core outcomes, except for life participation itself. Important factors identified in this study may be included in clinical trials involving Japanese patients to support shared decision making.
Keywords
Background
The number of patients receiving chronic dialysis in Japan exceeds 300,000, the vast majority of whom undergo hemodialysis (HD), with only around 10,000 patients on peritoneal dialysis (PD). 1 PD allows for home-based treatment and requires fewer hospital visits, making this approach potentially more conducive to maintaining quality of life (QOL) compared to HD.2–5 However, because PD utilizes the peritoneum—a biological membrane—as a dialysis membrane, long-term continuation may become difficult in some cases.4–6
When considering PD as a modality for kidney replacement therapy (KRT), healthcare providers have traditionally emphasized clinical findings reflecting the removal efficiency of uremic toxins and fluid overload, as well as the early detection and treatment of dialysis-related complications. 7 In contrast, the aspects prioritized by patients when choosing a treatment modality may differ from those emphasized by medical professionals.8,9 Indeed, the International Society for Peritoneal Dialysis recommended that not only residual kidney function, volume status and dialytic solute removal, but also patient-oriented outcomes should be assessed for prescribing high-quality goal-directed PD. 10
The international Standardized Outcomes in Nephrology—Peritoneal Dialysis (SONG-PD) initiative aimed to bridge this gap between clinicians and patients by identifying outcomes that matter to all stakeholders. 11 The SONG-PD study was conducted to establish a core outcome set for PD to be measured in all clinical trials and considered of critical importance to patients, caregivers, and health professionals. This process included a systematic review, nominal group technique sessions with patients and caregivers, interviews with health professionals, and an international Delphi survey, followed by a consensus workshop. The Delphi is a validated technique which has been used across a variety of health disciplines including mechanical ventilation, 12 prostate cancer, 13 non-specific low back pain, 14 preterm birth, 15 and reconstructive breast surgery 16 to generate consensus on core outcomes for clinical trials. As a result, five outcomes were identified as critically important to all stakeholders: PD-related infection; cardiovascular disease; mortality; technique survival; and life participation (e.g., ability to work, study, do home duties, etc.). 17
However, only a small number of participants from Japan were involved in the SONG-PD study, raising concerns that the perspectives of Japanese patients receiving PD may not have been adequately reflected. 17 Therefore, whether the core outcomes identified in the SONG-PD align with the values and needs of Japanese patients receiving PD remains unclear.
The present study aimed to identify important factors in the choice of dialysis modality among Japanese patients initiating PD from among the 39 factors evaluated in the SONG-PD study. 11 Using a questionnaire survey, we sought to gain a deeper understanding of their needs and to contribute to the development of better support for shared decision making in KRT.
Methods
Study population
Participants in this study comprised 199 patients at the Jikei University Hospital (Tokyo, Japan), the Jikei University Katsushika Medical Center (Tokyo, Japan), the Jikei University Third Hospital (Tokyo, Japan), the Jikei University Kashiwa Hospital (Chiba, Japan), Saitama Red Cross Hospital (Saitama, Japan), and Kawaguchi Municipal Medical Center (Saitama, Japan). The inclusion criterion was starting PD as the first KRT for end-stage kidney disease (ESKD). Exclusion criteria were patients younger than 20 years and those with a history of kidney transplantation or HD, except for less than a month in duration, before the start of PD. This study was approved by the institutional review board (IRB) of the Jikei University Hospital (IRB no. 36-004(12103)), and was performed in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all patients.
Questionnaire investigations
We conducted questionnaire investigations asking for factors the patient considered most important in the choice of dialysis modality between HD and PD. We stated in the questionnaire that respondents should select up to five applicable items. Questionnaire form including response options and their definitions were shown in Supplementary Table 1. Listed options in this questionnaire were exactly the same as those in the SONG-PD study. 11 Then, we ranked the items purely based on the number of patients who selected each one. Additionally, we conducted a sensitivity analysis with adjustments based on the number of selected items (e.g., applying a weight of 2.5 times for each item when only two items were selected). We conducted subgroup analyses based on sex, age, presence or absence of diabetes, timing of referral to nephrologist, presence or absence of multidisciplinary care, and employment status. In this analysis, age was divided into categorical groups divided by median.
Clinical data
Clinical data, including age, sex, cause of ESKD, comorbidities, physical examination, laboratory findings at the start of PD, and employment status, were obtained from medical records. Regarding comorbidities, cardiovascular disease was defined as heart failure, acute myocardial infarction, arrhythmia or conductive disturbance, valvular disease, and other heart disease, whereas cerebrovascular disease was defined as subarachnoid hemorrhage, cerebral hemorrhage, cerebral infarction, or other cerebrovascular disease. Blood tests for hemoglobin, serum albumin, and creatinine were performed using standard laboratory techniques at each center. Estimated glomerular filtration rate (eGFR) was calculated using the simplified prediction equation derived from the modified version in the Modification of Diet in Renal Disease study as proposed by the Japanese Society of Nephrology. 18 The duration from nephrologist referral to PD initiation, presence or absence of multidisciplinary educational interventions before PD initiation and subjects performing PD manipulation at the start of PD were also investigated. Early referral was defined as the patient being referred to the nephrologist more than 1 year before PD initiation, whereas late referral was defined as the patient being referred to the nephrologist less than 1 year before PD initiation. Data are presented as mean and standard deviation or median and interquartile range (IQR), as appropriate.
Results
Patient data are shown inTable 1. Mean patient age was 60 ± 12 years and 71.9% of patients were male. Underlying causes of ESKD were chronic glomerulonephritis (20.2%), diabetes (35.7%), nephrosclerosis (27.6%), polycystic kidney disease (4.5%), and other or unknown causes (12.6%). Prevalences of cardiovascular disease, cerebrovascular disease and malignancy were 20.1%, 8.0%, and 15.6%, respectively. Serum creatinine and eGFR at PD initiation were 8.3 mg/dL (IQR, 7.3–9.4 mg/dL) and 5.8 mL/min/1.73 m2 (IQR, 4.8–6.5 mL/min/1.73 m2), respectively. One-hundred and fifty-six patients (78.4%) were referred to the nephrologist more than 1 year before PD initiation (i.e., early referral), and 170 patients (85.4%) received multidisciplinary educational intervention in advance. Regarding PD manipulation, 181 patients (91.0%) performed manipulations themselves.
Patient characteristics at PD initiation.
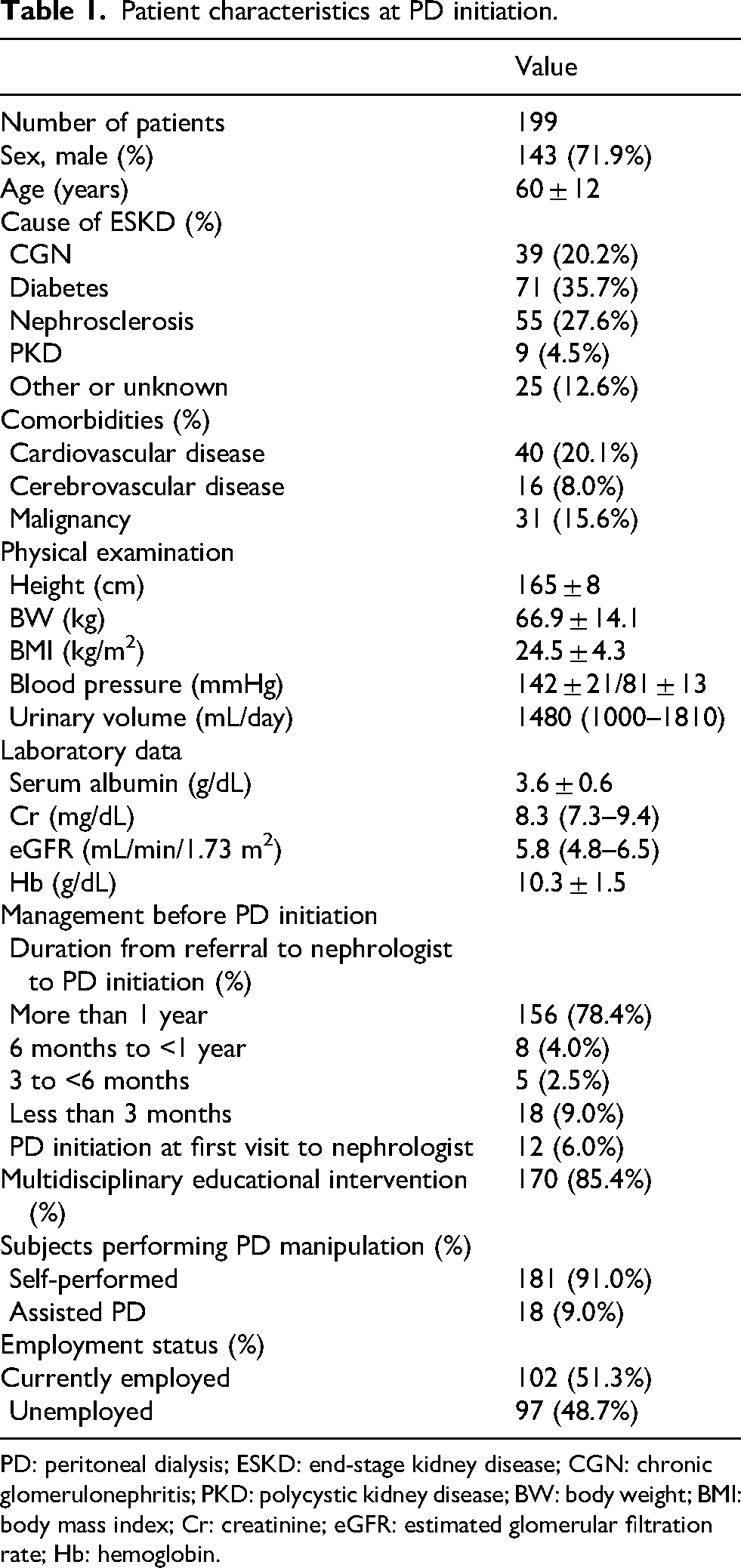
PD: peritoneal dialysis; ESKD: end-stage kidney disease; CGN: chronic glomerulonephritis; PKD: polycystic kidney disease; BW: body weight; BMI: body mass index; Cr: creatinine; eGFR: estimated glomerular filtration rate; Hb: hemoglobin.
Figure 1 shows the results of the questionnaire survey. The top 10 selected factors were as follows:
Flexibility with time (ability to schedule dialysis according to one's day); Life participation (ability to work, study, do home duties, etc.); Mobility/fitness (ability to move without assistance, and to train to achieve physical goals); Ability to travel (to go away for holidays, events, visiting family, work, etc.); PD failure (when the PD stops working and one needs to go on another type of treatment, e.g., HD; how long the PD lasts); Death (number of people who die, risk of death, how long one is likely to live); PD-related infection (avoidance of PD-related infections, including peritonitis, exit-site infection, and tunnel infection); Impact on family and friends (ongoing impact that living with a patient on PD has on family, caregivers, and friends); Fatigue (feeling tired or having no energy most of the day, for many days or weeks in a row); and Catheter complications (avoiding problems relating to access to the peritoneal cavity (including fluid leaks, obstruction, hernia, omental wrapping, hemoperitoneum).
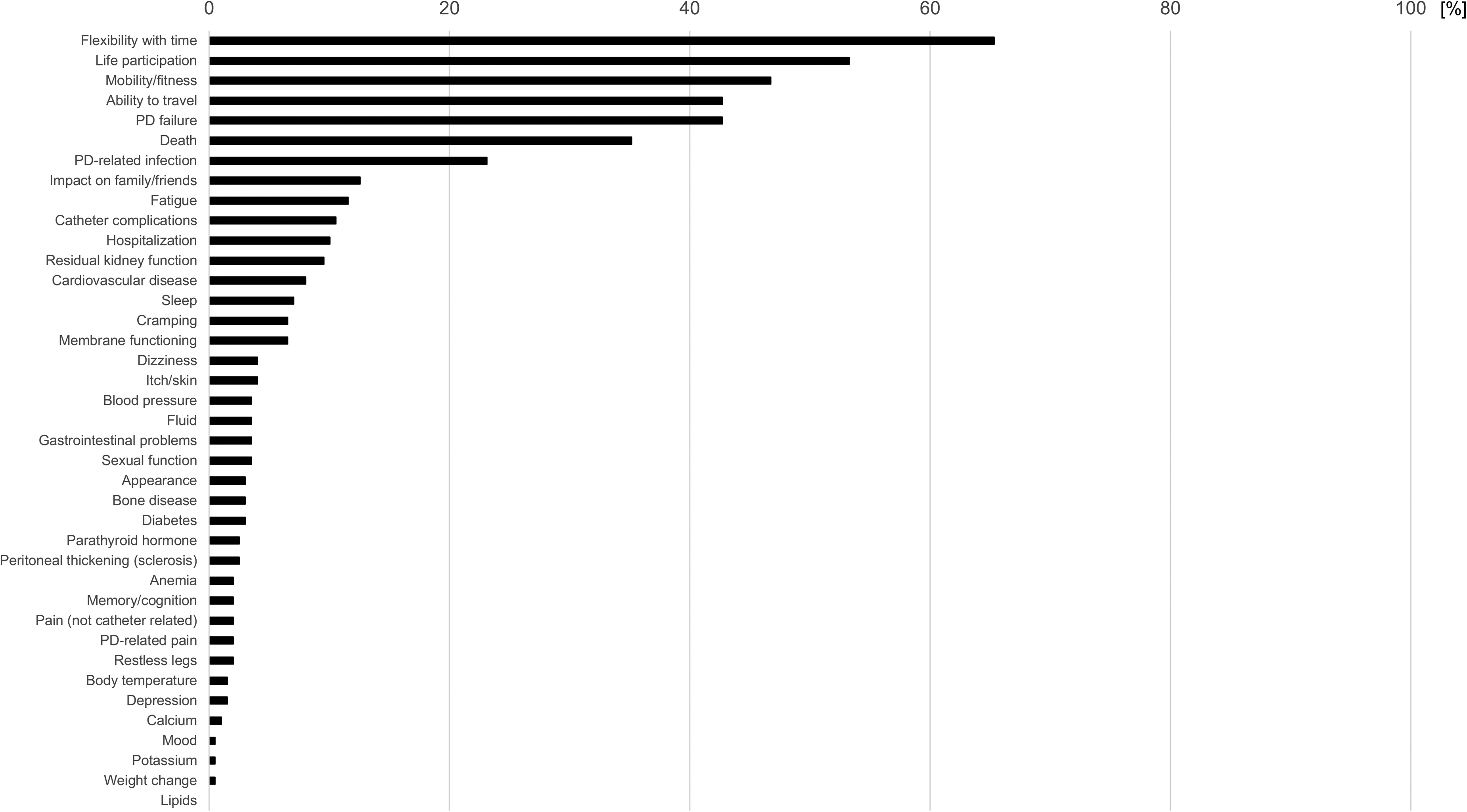
Results of the questionnaire survey in 199 patients.
The results of a sensitivity analysis with adjustments based on the number of selected items were almost similar to the main analysis (Supplementary Figure 1).
Figure 2 shows the top ten selected factors in each subgroup analysis. Younger patients tended to rate “Ability to work, study, do home duties, etc.” (Life participation) more highly, whereas elderly patients tended to rate “When the PD stops working and the patient needs to go on another type of treatment, e.g., HD; how long the PD lasts” (PD failure) more highly. Diabetic patients tended to rate “Number of people who die, risk of death, how long one is likely to live” (Death) more highly than nondiabetic patients. Currently employed patients tended to rate “Ability to work, study, do home duties, etc.” (Life participation), “Number of people who die, risk of death, how long one is likely to live” (Death), and “Ongoing impact that living with a patient on peritoneal dialysis has on family, caregivers, and friends” (Impact on family/friends), whereas unemployed patients tended to rate “To go away for holiday, event, visiting family, work, etc.” (Ability to travel) than their counterpart. In other subgroup analyses by sex, time from nephrology referral to PD initiation, and presence or absence of multidisciplinary educational interventions before PD initiation, we could not find any striking difference. Unfortunately, we could not conduct statistical analyses because of the limited number of patients and the large number of options included in the questionnaire survey.
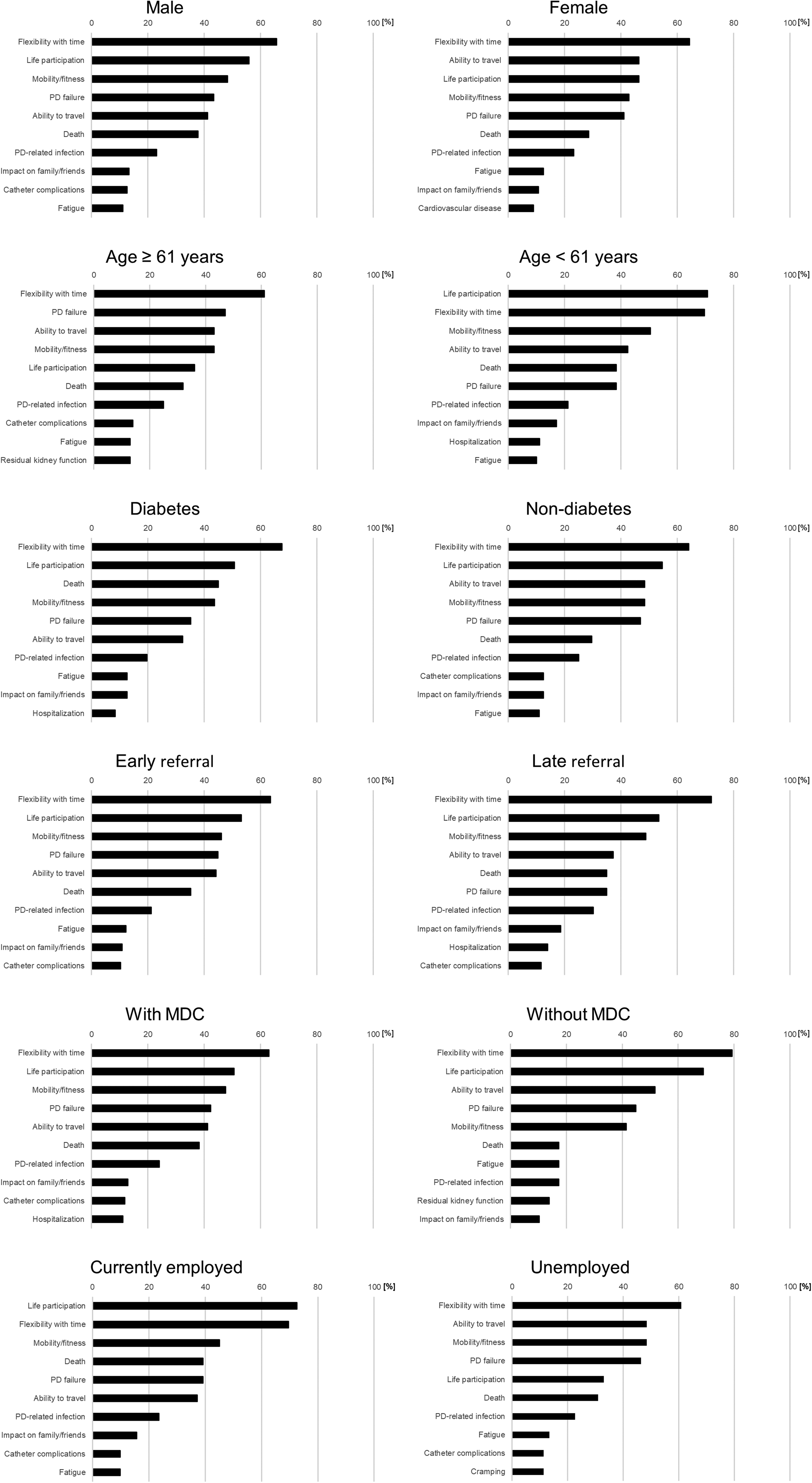
The top 10 important factors in the choice of dialysis modality in each subgroup. MDC: multidisciplinary care.
Discussion
This study revealed that important factors in the choice of dialysis modality among Japanese patients initiating PD were related to daily flexibility and activity—specifically, “flexibility with time,” “ability to work/study/do housework,” “ability to move freely,” and “ability to travel.” While “life participation” was selected in both this study and the international SONG-PD study, the greater emphasis on time flexibility and travel in our findings is particularly notable. 17 Of note, “life participation” should be interpreted broadly as participation in daily roles and activities, including family, social, and leisure activities, rather than necessary activities such as work or home duties. The rankings of the other core outcomes from the SONG-PD initiative than “life participation” were as follows: “PD failure” ranked fourth, “Death” sixth, “PD-related infection” seventh, and “cardiovascular disease” 13th. In a study that investigated the outcomes prioritized by patients receiving PD in Australia, the United States, and Hong Kong, when choosing PD, the top 10 outcomes were PD infection, mortality, fatigue, flexibility with time, blood pressure, PD failure, ability to travel, sleep disturbance, ability to work, and impact of family/friend. 9 The results of that study were almost similar to ours, but blood pressure and sleep disturbance were given greater emphasis. In a questionnaire survey conducted among 17 Japanese patients receiving PD, “self-ability/independence,” “decreased frequency of hospital visits,” and “time flexibility” were particular advantages, whereas “high frequency of dialysis in a day,” “catheter care,” and “troubling other people” were particular disadvantages of choosing PD, however, this finding should be interpreted cautiously because of the very small sample size. 19 Among them, “self-ability/independence” and “time flexibility” were included among top ten selected factors of the present study, whereas the item on “decreased frequency of hospital visits” was not included among the options in this questionnaire. It should be noted that the targets in this study differ from those in the SONG-PD study. This study was to identify important factors in the choice of dialysis modality among patients initiating PD, whereas the SONG-PD study was to identify core outcomes to be included and assessed in clinical trials. Therefore, it is difficult to directly compare the important outcomes between these studies.
These differences may reflect unique cultural and social aspects of dialysis care in Japan. Patients who opt for PD often seek greater autonomy and hope to maintain QOL through home-based treatment.8,9 Globally, PD remains underutilized in Japan. 20 Because only a limited number of patients receive PD, these wishes are considered to have been more pronounced. Furthermore, several other factors may explain these findings. First, Japanese dialysis patients are older than those in other country, therefore patients may place relatively less emphasis on mortality when choosing a modality. 21 Second, Japan has reported comparatively low rates of PD-related peritonitis, which may partly explain why PD-related infection ranked lower in our cohort than in international studies. 22
Our findings highlight the potential gap between patient priorities and the clinical metrics traditionally emphasized by healthcare providers.8,9 In the practice of shared decision making for KRT, it is crucial to understand and respect the values and goals of patients—such as the desire to travel, continue working, or manage their time freely—and to provide tailored information and dialogue accordingly.23,24 In addition, the shared decision-making approach, particularly by multidisciplinary education intervention, could enhance patient satisfaction and outcomes in PD.25,26 This study offers concrete insights into what Japanese patients receiving PD truly value, providing useful guidance for more patient-centered decision-making.
The presence of diabetes and age were thought to be important factors in shared decision making for KRT. Diabetic patients prioritized living a longer life, probably because of the serious prognostic implications.27,28 It is noteworthy that life prognosis has not been clearly shown to differ significantly between HD and PD in diabetic patients.29,30 Meanwhile, maintaining an active social life remains a priority even after the initiation of dialysis for younger patients, whereas long-term continuity of treatment is regarded as a key concern for elderly patients. Similarly, currently employed patients tend to prioritize contributing to society, such as ability to work, study, do home duties, impact on family or friends, or life prognosis.
This study had several limitations. In particular, the use of a questionnaire survey in this study allowed for only limited conclusions. The SONG-PD study was conducted using Delphi survey, a group facilitation technique including patients, caregivers, and health professionals with experience or expertise in PD.11,17 This group facilitation technique has been established as a useful decision-making process. 31 Additionally, as mentioned above, our questionnaire asked important factors in the choice of dialysis modality among patients initiating PD, whereas the SONG-PD study was to identify outcomes of importance to patients receiving PD. These questions are different. Therefore, it is difficult to directly compare the important outcomes between the SONG-PD study and our study. Nevertheless, this study is meaningful in that it identified factors prioritized by Japanese PD patients—a subject that has received limited attention to date. These findings are expected to contribute to more tailored and needs-based support for selecting KRT in Japan. Incorporating these important factors in the choice of dialysis modality into clinical research and routine practice could ultimately lead to improved outcomes for patients receiving PD in Japan.
Conclusion
Important factors in the choice of dialysis modality among Japanese patients initiating PD were patient-orientated outcomes such as flexibility with time, life participation, or mobility/fitness rather than mortality or dialysis-related complications. To support the outcomes of importance to Japanese patients receiving PD, factors identified in this study could be considered in Japanese clinical trials and clinical practice. This may enhance shared decision making.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608261460222 - Supplemental material for Important factors in the choice of dialysis modality among Japanese patients initiating peritoneal dialysis
Supplemental material, sj-docx-1-ptd-10.1177_08968608261460222 for Important factors in the choice of dialysis modality among Japanese patients initiating peritoneal dialysis by Yudo Tanno, Yukio Maruyama, Nanae Matsuo, Masato Ikeda and Takashi Yokoo in Peritoneal Dialysis International
Footnotes
Acknowledgments
The authors would like to thank all contributors, patients, and professionals involved in this study. Especially, we are grateful to the following professors who supervised the administration of the questionnaire survey: Dr Yuki Shina (the Jikei University Hospital), Dr Satoshi Kidoguchi, Dr Shohei Fukunaga, Dr Maiko Furuya and Dr Naohito Masuda (the Jikei University Katsushika Medical Center), Dr Keita Hirano, Dr Akimitsu Kobayashi and Dr Ai Katsuma (the Jikei University Third Hospital), Dr Yukiko Tsuchiya and Dr Ryumon Miyashita (the Jikei University Kashiwa Hospital), Dr Morimasa Amemiya, Dr Taro Hoshino and Dr Takahito Niikura (Saitama Red Cross Hospital), and Dr Shinya Yokote and Dr Yu Honda (Kawaguchi Municipal Medical Center).
Ethical approval
This study was approved by the IRB of the Jikei University Hospital (IRB no. 36-004(12103)) and was performed in accordance with the principles of the Declaration of Helsinki.
Informed consent to participate
Written informed consent was obtained from all patients.
Informed consent to publish
Written informed consent was obtained from all patients.
Author contributions
YT, YM, NM, MI, and TY researched literature and conceived the study. YT, YM, and NM were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. YT wrote the first draft of the manuscript. TY supervised the research. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
We have read and understood the policy of Peritoneal Dialysis International on disclosing conflicts of interest and declare the following interests: Y.T., Y.M., N.M. and M.I. received honoraria from Vantive International, Inc. and Terumo Corporation. No other authors have any conflicts of interest to declare.
Data availability statement
The data supporting the results of this study are available from the corresponding author on reasonable request.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.