
Abstract
Backgrounds
Unplanned initiation of peritoneal dialysis (PD) is linked to higher risks of complications and transfer to hemodialysis (HD). This study evaluates whether assisted PD was associated with the risk of transitioning to hemodialysis, for the individuals experiencing unplanned PD initiation.
Methods
This retrospective study analyzed data from the French Language Peritoneal Dialysis Registry (RDPLF), including 1009 patients with unplanned PD initiation, defined as a period of <30 days on HD before PD initiation, between January 1, 2002, and December 31, 2018. We compared assisted PD (nurse/family-assisted) versus self-care PD using cause-specific analyses. Time-dependent coefficient Cox regression addressed non-proportional hazards. Mediation analysis was conducted to explore the direct and indirect effects of assisted PD on the risk of transfer to HD, considering early peritonitis as a mediator.
Results
In unplanned starters, Assisted PD was associated with an increased early risk of transfer to HD within the first six months (cs-HR 2.00, 95% CI 1.30–3.30), but a reduced risk thereafter (cs-HR 0.70, 95% CI 0.50–0.90). Patients on assisted PD had a higher risk of death (cs-HR 2.39, 95% CI 1.77–3.24) and a lower likelihood of transplantation (cs-HR 0.23, 95% CI 0.12–0.42). Mediation analysis revealed no significant indirect effect of assisted PD on the risk of transfer to HD via early peritonitis.
Conclusion
Unplanned PD initiation presents significant early risks, with assisted PD showing delayed protective effects after six months. Targeted early support (psychological and social) and further research are crucial to optimize outcomes for this patient group.
Introduction
Approximately 30% of patients initiate dialysis in an unplanned manner,1,2 despite comprehensive guidelines on the management of patients with chronic kidney disease (CKD). 3 There remains a lack of consensus on what precisely defines an unplanned initiation,2,4 nevertheless it has been accepted that unplanned dialysis initiation often results in patients beginning dialysis via hemodialysis with a catheter which negatively affects the patients outcome. 5 The consequences of the unplanned initiation include higher rates of morbidity and mortality, increased rate and duration of hospitalization, and a reduced quality of life.5–9
In the PD context unplanned initiation is of particular concern as it is associated with a greater risk of transfer to hemodialysis which is a major concern for patients and the nephrology team.10,11 Indeed, Lobbedez et al. showed that, compared to a planned PD initiation, an unplanned PD initiation was associated with a higher risk of transfer to HD when accounting for competing risks (sd-HR 1.33; 95% CI 1.13–1.55). 10 Although this remains to be demonstrated, this higher risk of transfer to HD might be driven by early complications on PD, such as peritonitis, which may be exacerbated by the lack of preparation and support that is associated with an unplanned PD initiation. Furthermore, emotional distress linked to the unplanned PD start may affect the patient's ability to cope with home dialysis, which could lead to a transfer to HD.
One potential intervention that may improve PD duration in the unplanned PD starters is the provision of home assistance, such as home visits or assisted PD.10,12,13 Indeed, it can be hypothesized that providing home assistance may help patients and their relatives cope with home dialysis after discharge from hospital, thereby decreasing the likelihood of transfer to HD. In addition, assisted PD could decrease the risk of early complication of PD that jeopardize PD duration. 14
This study was carried out to evaluate whether assisted PD was associated with the risk of transitioning to hemodialysis, for the individuals experiencing unplanned PD initiation. The study was also conducted to determine whether the protective effect of assisted PD is mediated by its impact on the risk of early peritonitis.
Methods
Study population
This was a retrospective study using data from the French Language Peritoneal Dialysis Registry (RDPLF). Data from all patients older than 18 years of age incident on PD between January 1, 2002, and December 31, 2018, was extracted. The end of the study period was December 31, 2021.
Patients experiencing a period of less than 30 days on HD before PD initiation, which was considered as a proxy of an unplanned PD initiation, were included in the study. Indeed, in the context of PD, some studies have suggested that a period of less than 30 days on hemodialysis before PD is a proxy for an unplanned start,10,15 assuming that switching from HD to PD within the first month of renal replacement therapy was not the pathway chosen by the patients and by their nephrologists.
Patients who experienced primary PD failure, defined as those who were on PD for less than one day, were excluded from the analyses.
Definition of variables
Baseline characteristics, evaluated at PD initiation, were extracted from the RDPLF database including: age, sex, diabetic status, underlying kidney disease, previous kidney replacement therapy (KRT) before PD, PD modality at initiation (continuous ambulatory PD [CAPD] or automated PD [APD]), type of centre and assistance status. To assess comorbidities, the Charlson comorbidity index (CCI) was extracted from the database, and the modified CCI was calculated by subtracting the age subscore to assess the role of comorbidities independently of patient age. The centre size was estimated by the number of incident patients per year of participation over the study period. The total number of peritonitis and the date of first peritonitis were extracted from the registry.
Explanatory variables
The main explanatory variable was assisted PD, defined as either nurse-assisted PD or family-assisted PD. Self-care PD was used as a comparator. Sensitivity analyses were conducted according to the assistance modality (Eg nurse-assisted PD versus self-care PD and family-assisted PD versus self-care PD).
The a priori mediator was an early peritonitis episode defined by a peritoneal infection occurring within the first 6 months of PD.
Events of interest and competing events
The event of interest was a transfer to HD for more than 2 months, death on PD and kidney transplantation were considered as competing events. 16 Death occurring within two months of transferring to HD was considered to have occurred while on PD.
The time to event was calculated for the first of these events for each patient.
Statistical analysis
The required sample size to detect a significant difference in the risk of transfer to HD between assisted PD and self-care PD patients was calculated with the observed rates of transfer to HD of 28.8% in the assisted group and 41.7% in the self-care group. With a two-sided p value of less than 5%, a power -of 80%, and an estimated 20% lost to follow-up, the required sample size was 328 patients for each group.
A direct acyclic graph (DAG) was used to represent the relationship between the exposure variable (assisted PD), the mediator (early peritonitis), and the confounders (Supplemental Figure S1). Assumptions for potential confounders and mediators were defined based on the literature data.10,14,17 For the event of interest, we tested the interaction between the exposure and the mediator which was not significant. In addition, the interactions between assisted PD, age, and sex have been investigated and were not significant.
Kaplan-Meier survival curves were drawn for the event transfer to HD, according to the assistance status. To evaluate the association between assisted PD and the risk of transfer to HD, Cox regressions were used to estimate the cause-specific hazard ratios (cs-HRs) and their 95% confidence intervals (CIs). The association between the exposure and each variable was assessed with a bivariable analysis. Thereafter a multivariable analysis was performed with the exposure, the confounders and the mediator and subsequently without the mediator. All variables were included a priori in the multivariate analysis. A mediation analysis with a counterfactual approach was performed to explore the direct effect of assistance on the risk of transfer to HD and the indirect effect of assistance through the mediator.
A previous study from our team has demonstrated that the impact of assistance on the risk of transfer to HD was not constant over time, the protective effect of assisted PD appearing after the first 6 months on PD. 18 Consequently, a time-dependent coefficient Cox regression with a 6-month cutoff (based on the aspect of the regression spline estimating the baseline hazard of the effect of assisted PD on the risk of transfer to HD over time, Supplemental Figure S2) allowing to estimate adjusted hazard ratios for the first 6 months (<6 months cs-HR) and beyond (≥6 months cs-HR) was employed to assess the effect of assistance over the time. 19 Sensitivity analyses were conducted with a 12-month cutoff.
The use of assistance is influenced by the patient's characteristics; therefore, we conducted a sensitivity analysis using a propensity score (PS) matching method to reduce the effects of confounding. Indeed, the inspection of the PS distribution between the groups of patients allows to identify areas of nonoverlap. The covariates included in the PS calculation were selected a priori as being those more strongly associated with the use of assistance: age, sex, age, diabetes and primary renal disease. We used a nearest-neighbor matching method with a caliper of 0.25 standard deviation and a 1:1 ratio of participants. Cox models were performed on the matched dataset.
As the rate of missing data was of 2.6%, a complete case analysis was performed. Statistical analyses were performed with R version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria).
The RDPLF has the approval of the French National Ethics Committee (Commission Nationale de l’Informatique et des Libertés). This study took place within the framework of this authorization. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines (STROBE 2008).
Patient representation
Patients’ opinions and perspectives on research topics are important but often under-represented. 20 We asked two of our patients to participate in this research project by evaluating the topic and content of our study. We reported verbatim of their opinions on the relevance of our research.
Results
Patient characteristics
Of the 15675 incident PD patients on PD over the study period, 1049 (6.6%) had an unplanned PD initiation. Of those, 40 patients experienced primary PD failure and were excluded, thus 1009 patients were included in the analyses (Supplemental Figure S3). Patients characteristics according to the timing of PD initiation (Eg planned or unplanned) is provided in Supplementary Table S1.
Unplanned patient's characteristic according to the assistance status are provided in Table 1. Among the 1009 patients included in the study, 560 (56%) were treated by assisted-PD. Compared to self-care PD patients, assisted PD patients were older (median age: 78.6 vs. 54.5 years) and included a higher proportion of female patients (242/560 females - 43.2% vs. 125/449 females 27.7%). Comorbidity burden was markedly higher in the assisted PD group (CCI≥5: 272/560–46% vs. 86/449–19%). Diabetes was also more prevalent among assisted patients (Diabetic patients: 256/506–46% vs. 84/449–19%).
Patient's characteristics at PD initiation according to the assistance status.
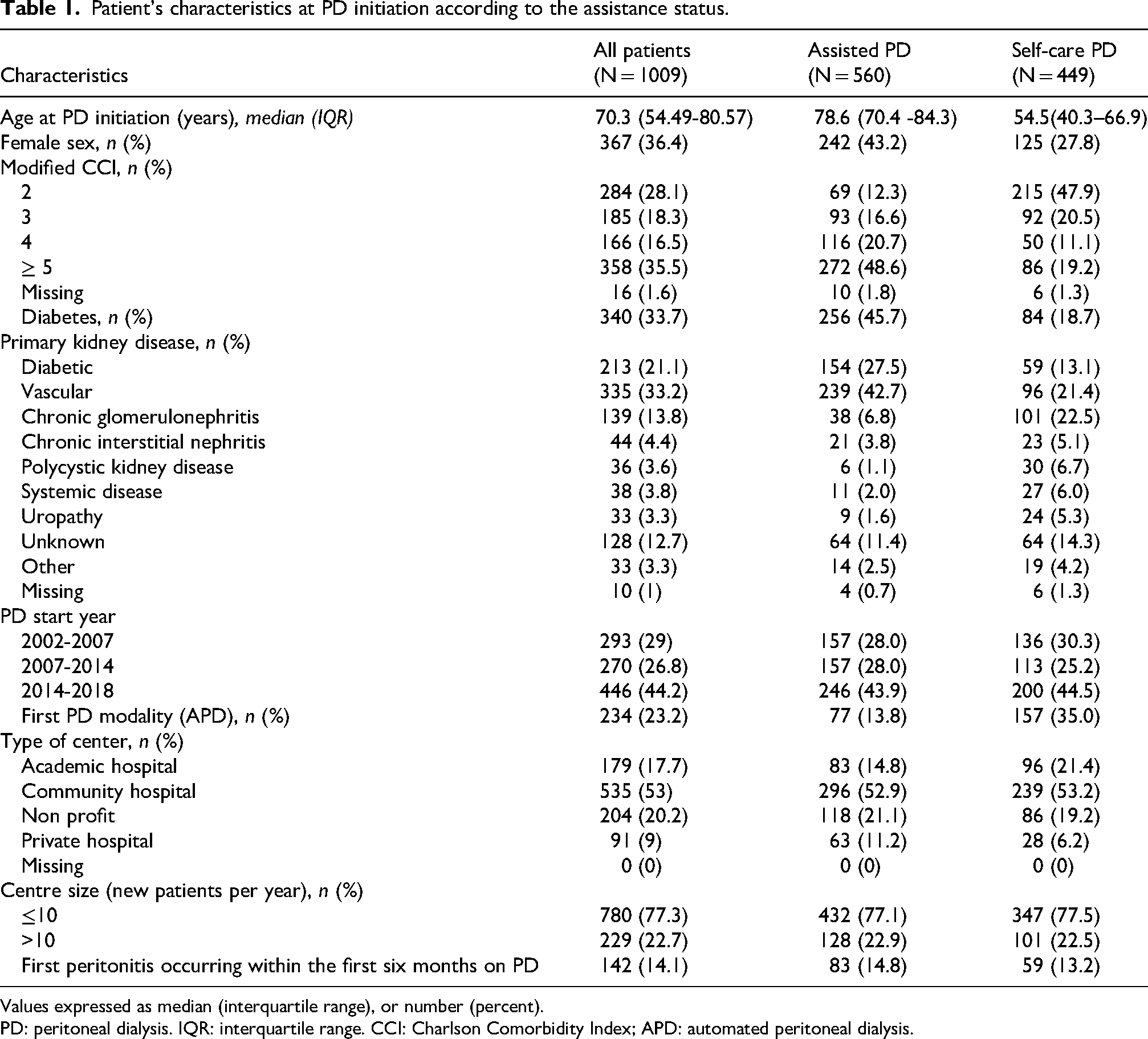
Values expressed as median (interquartile range), or number (percent).
PD: peritoneal dialysis. IQR: interquartile range. CCI: Charlson Comorbidity Index; APD: automated peritoneal dialysis.
Outcomes on PD
Over the study period, there were 410 (41%) death, 348 (34%) transfer to HD and 161 (16%) kidney transplantation. In the assisted-PD group, 337 patients (60%) died, 161 (29%) transferred to HD, and 13 (2%) underwent kidney transplantation. In contrast, among self-care PD patients, 72 (16%) died, 187 (42%) transferred to HD, and 148 (33%) underwent transplantation. The median time on PD was 16 months overall, with 15 months in the assisted-PD and 17 months in the self-care PD group respectively. Figure 1 displays Kaplan-Meier survival curves for event transfer to HD according to assistance status.
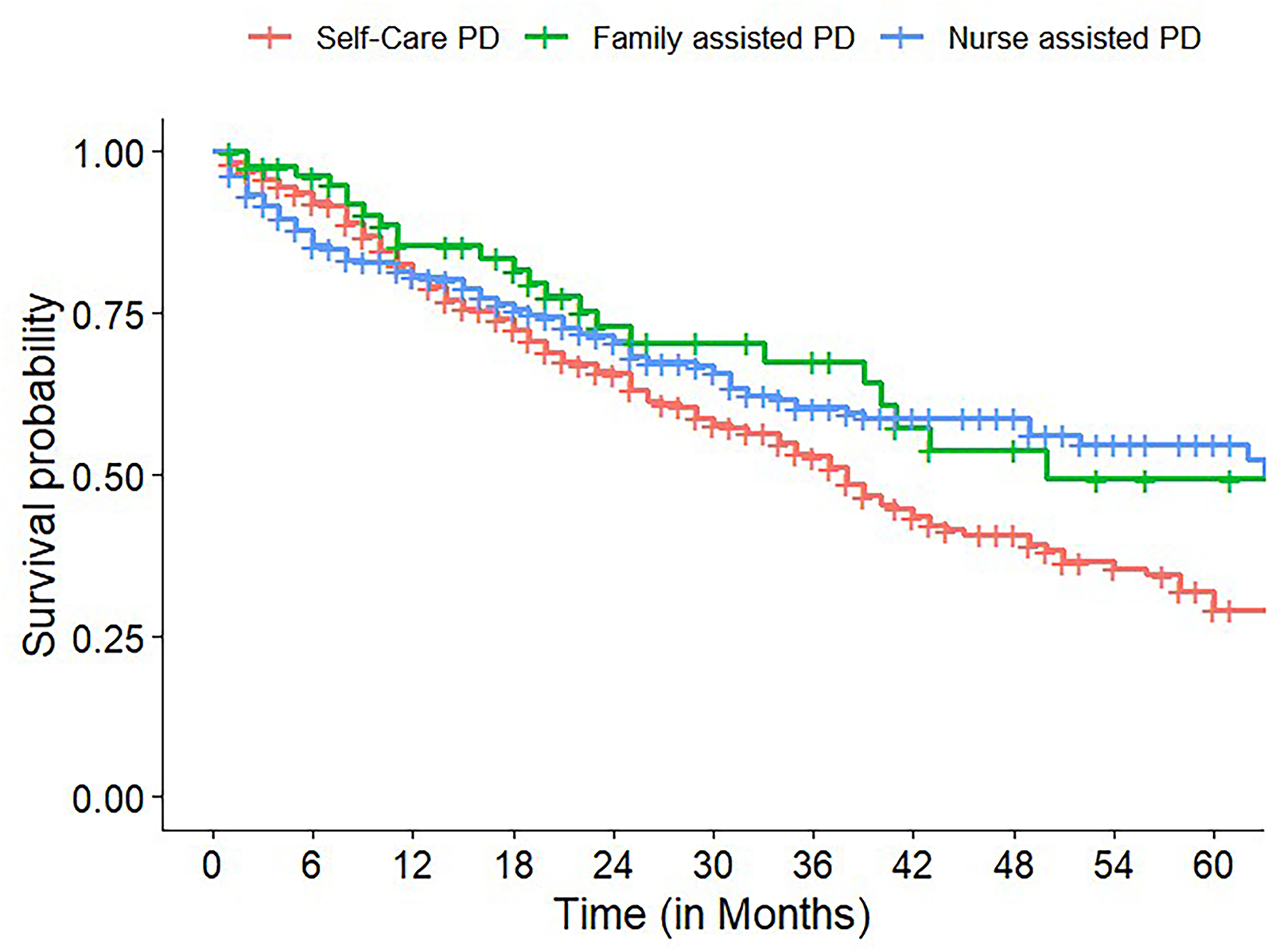
Kaplan-Meier survival curves by assistance status for the event transfer to HD HD: hemodialysis, PD: peritoneal dialysis.
The causes of transfer to HD, according to the assistance status, are provided in Supplemental Table S2.
Association between assisted PD and the risk of transfer to HD
In the multivariate Cox regression, there was no significant association between assisted PD and the risk of transfer to HD (cs-HR 0.91, 95% CI 0.70–1.20) (Figure 2). Whereas, using a time-dependent coefficient analysis, assisted PD was associated with a greater risk of transfer to HD within the first six months of PD (<6 months cs-HR 2.00, 95% CI 1.30–3.30), but a lower risk thereafter (≥6 months cs-HR 0.70, 95% CI 0.50–0.90) (Figure 2).
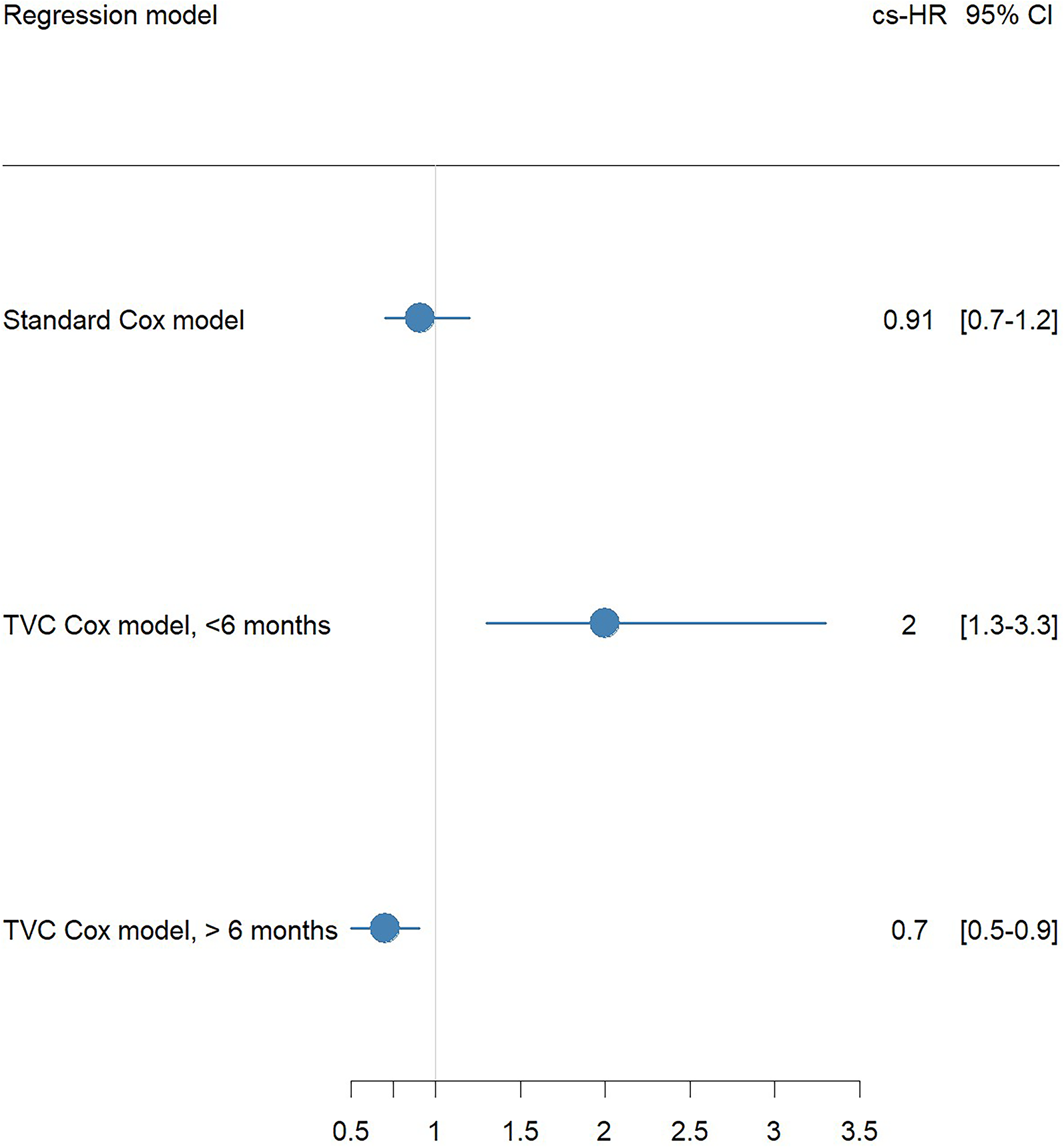
Forest plot representing the effect of assisted PD on the risk of transfer to HD in the adjusted Cox regression and adjusted Cox regression with time varying coefficient with a cutoff period at 6 months. PD: peritoneal dialysis; HD: hemodialysis; TVC: time varying coefficient; cs-HR: cause-specific hazard ratio. On the basis of the aspect of the regression spline, a cutoff period at 6 months after PD initiation was selected, enabling us to estimate the adjusted hazard ratios of the effect of assistance on the different outcomes for the first 6 months of PD (<6 months cs-HR) and for those above 6 months after PD initiation (≥6 months cs-HR). Cs-HR are adjusted on age, sex, diabetes, causal nephropathy, modified CCI, PD start year, PD modality, administrative center type and center size.
Sensitivity analyses with a 12-month cutoff yielded similar results, showing no association within the first 12 months (<12 months cs-HR 1.30, 95% CI 0.90–1.90) but a lower likelihood afterward (≥12 months cs-HR 0.70, 95% CI 0.50–0.96) (Supplemental Figure S4).
When the mediator early peritonitis was included in the multivariable analysis the association between assisted-PD and the risk of transfer to HD did not change significantly. Mediation analysis indicated no overall direct or indirect effect of assisted PD on the risk of transfer to HD through peritonitis. There was a protective direct effect of assisted PD on the risk of transfer to HD after six months on PD (HR 0.7, CI 0.5–0.9), which was not mediated by a lower risk of early peritonitis (indirect effect: HR 0.99, CI 0.96–1.02) (Supplemental Table S3 and S4).
Association between assisted PD and the competing risks of death and transplantation
In the multivariate analysis, assisted PD was associated with an increased risk of death (cs-HR 2.39, 95% CI 1.77–3.24). According to the adjusted Cox regression with time-dependent coefficients, assisted PD was associated with a greater risk of death regardless of the timing (Supplemental Figure S5). The sensitivity analyses performed defining the cut-off period at 12 months provided similar results (Supplemental Figure S4).
In the multivariate analysis, assisted PD was associated with a decreased chance of transplantation (cs-HR 0.23, 95% CI 0.12–0.42). Using time-dependent coefficient analysis, assisted PD was not associated with the risk of transplantation in the first six months (<6 months cs-HR 0.17, 95% CI 0.02–1.30), but showed a lower likelihood thereafter (≥6 months cs-HR 0.23, 95% CI 0.12–0.44) (Supplemental Figure S5). Sensitivity analyses with a 12-month cutoff yielded similar results (Supplemental Figure 4).
Patient representation and verbatim discussion
The patient's representation and verbatim discussion are displayed in Table 2.
Patients’ representation and verbatim discussion.
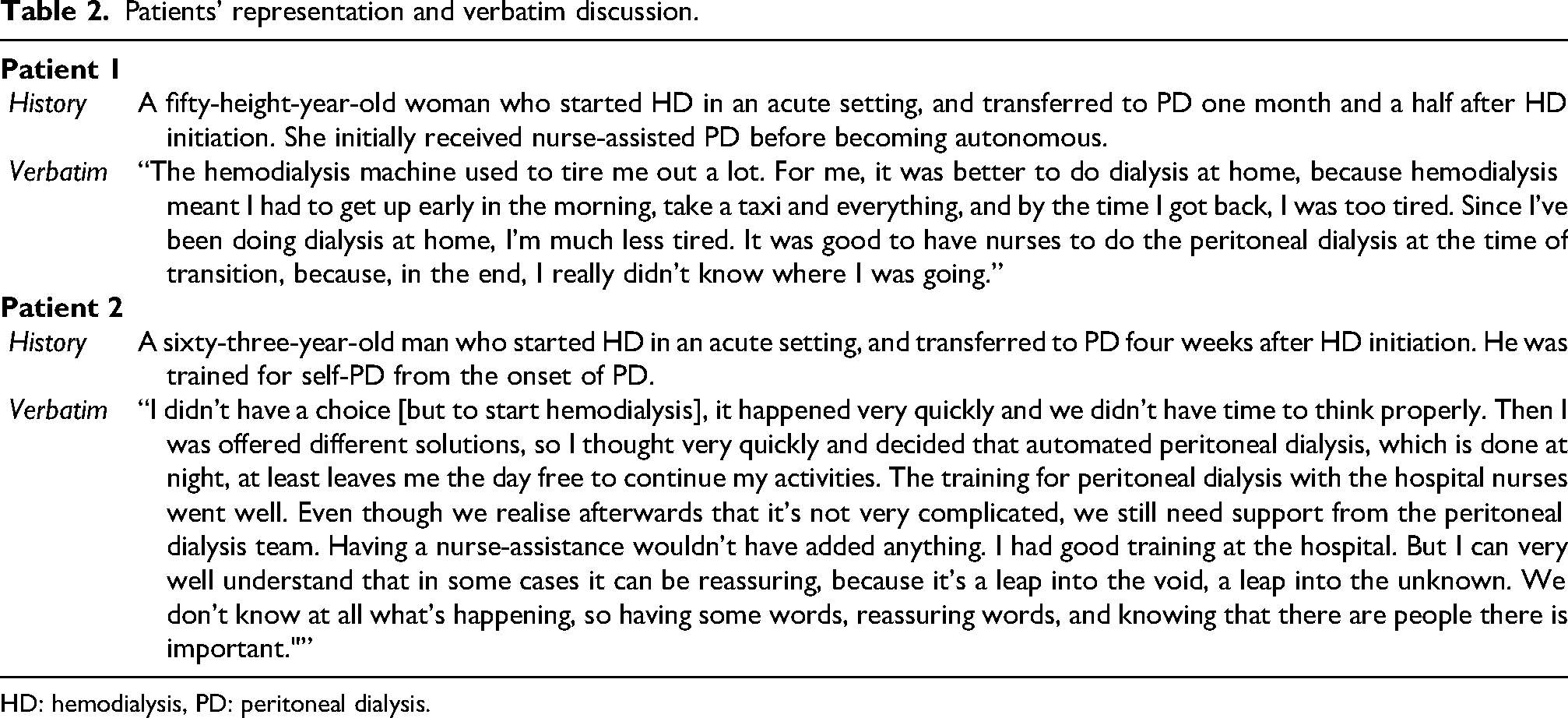
HD: hemodialysis, PD: peritoneal dialysis.
Sensitivity analyses according to assistance modality
Sensitivity analyses comparing nurse-assisted PD versus self-care PD and family-assisted PD versus self-care PD provided similar results. According to the usual adjusted Cox regressions, compared with self-care PD patients, nurse assistance was not associated with the risk of transfer to HD (mean cs-HR, 1.02; 95% CI 0.76–1.36). In the first 6 months after PD initiation, patients on nurse assisted PD had a greater risk of transfer to HD (<6 months cs-HR, 2.55; 95% CI 1.59–4.09) but a lower likelihood afterward (>6 months cs-HR, 0.69; 95% CI 0.49–0.697). In both models, the usual adjusted regression and adjusted Cox regressions with time-dependent coefficients, family-assisted PD was not associated with the risk of transfer to hemodialysis (Supplemental Figure S6). Regardless of the modality and timing, assisted PD was associated with a greater risk of death, and a lower risk of kidney transplantation except in the first 6 months after PD initiation when the association was not significant (Supplemental Figure S6).
In the PS-matched patient cohort, reduced to 420 patients, there was no significant association between assisted PD and the risk of transfer to HD (cs-HR 0.92, 95% CI 0.66–1.28).
Discussion
Our findings suggest that assisted PD, independently of the assistance modality, in the context of an unplanned PD initiation situation is not associated with the overall risk of transfer to HD. During the first 6 months of PD, patients treated by assisted PD had a higher risk of transfer to HD, followed by a reduced risk thereafter. Mediation analysis found no significant indirect effect of assisted PD on the risk of transfer to HD through early peritonitis, indicating that infection pathways do not influence this association. Assisted PD was consistently linked to an increased risk of death and a lower likelihood of kidney transplantation, highlighting the complex dynamics and the need for targeted early support in these patients, including the need for additional psychological and social support.
Our study included a sufficient sample size to detect meaningful differences in the risk of transfer to HD between assisted PD and self-care PD groups. The non-significant effect likely reflects the fact that assisted PD was associated with a greater risk of transfer to HD during the first 6 months after the dialysis initiation. This finding could lead to the conclusion that patients who needed to be assisted were also those with the greater risk of an early PD cessation. It also suggests that the initial six months are a critical adjustment period and that home assistance is not the only factor that can decrease the risk of early PD cessation. Our results suggests that additional measures may be necessary during this period, as assistance alone does not reduce the risk of transferring to HD. In our study assisted PD had a protective effect on the risk of transfer to HD after six months on PD which is consistent with existing literature. 18 This initial increase in risk may be related to the indication for assisted PD itself, as patients requiring assistance are likely to be frailer, with greater comorbidities or functional limitations, which could contribute to early complications or difficulties in adapting to PD. In the group of PD patients who did not experience early PD cessation, assisted PD may lead to more stable and sustainable dialysis management, suggesting that assisted PD could help unplanned dialysis patient to stay on PD after the initial 6 months period. 21
It is important to notice that the effect of assistance was not mediated by a lower risk of early peritonitis. This is of importance as in response to the challenges associated with unplanned PD initiation; educational programs have been developed to empower patients by providing them with the necessary knowledge and skills to manage their treatment effectively and to make a choice between HD and PD despite the unplanned initiation.22,23 In addition to educational programs, transitional care units have emerged as a vital component in the dialysis care continuum. These units are designed to provide temporary, intensive support to patients newly initiated on dialysis, with a strong emphasis on facilitating a smoother transition to home-based therapies. By focusing on patient activation and self-management, transitional care units help patients gain confidence and competence in managing their dialysis treatment independently. These units not only support patients during the critical early stages of dialysis but also play a pivotal role in promoting long-term adherence to home dialysis modalities.24–26
The observed transfer rate to HD was notably high, particularly in the autonomous group. This highlights the substantial morbidity and mortality associated with unplanned dialysis initiation, which has been previously demonstrated in the literature.5,10,11 Unplanned starts are often linked to acute clinical decompensation, resulting in higher complication rates and a greater likelihood of early treatment modality changes.
We observed a higher rate of transfer to HD due to social reasons in the assisted patient group compared to the self-care group. This finding aligns with previous data. 27 Surprisingly, one might expect that assistance would reduce the risk of transfer for social reasons. However, our results underscore that, in the context of unplanned initiation of PD, assistance alone is insufficient to mitigate the risk of transfer. This suggests the critical need for additional psychological and social support alongside practical assistance. It is plausible that the stress and challenges associated with unplanned PD initiation contribute to patient or caregiver burnout. This finding warrants further validation, as providing enhanced psychosocial support in case of an unplanned PD initiation could prove to be a valuable approach in improving outcomes and reducing transfer rates.
Finally, in our findings, elderly patients with multiple comorbidities who initiate PD in an unplanned manner exhibit a poor prognosis with a significant risk of mortality. This underscores the critical need to carefully consider the indication for urgent initiation of PD in elderly, comorbid patients. It also highlights the importance of considering conservative management as a viable alternative in this situation.28,29
Our study has several limitations. The observational design precludes conclusions about causality, and the retrospective nature may introduce classification bias. The reliance on declarative data in the registry about the causes of PD cessation and transfer to HD could lead to declaration bias. Focusing on a specific population within the French healthcare system may limit the generalizability of our findings. Although we attempted to control for confounding, we observed a large age difference between the assisted PD group and the comparator self-care PD group. The small sample size might reduce statistical power and not all potential confounding variables, such as socioeconomic factors or clinical practices, were accounted for. However, our findings are robust, as indicated by consistent results across numerous sensitivity analyses.
In conclusion, this study highlights the complex dynamics and challenges of unplanned PD initiation. While assisted PD may offer benefits over time, the initial six months are critical and require additional support beyond mere assistance. The higher rate of transfer to HD for social reasons among assisted patients underscores the need for comprehensive psychosocial support. Integrating educational programs and transitional care units could address these complexities and improve patient-centered care. The poor prognosis in certain subgroups, particularly elderly and comorbid patients, emphasizes the need for careful consideration of PD initiation in urgent settings and the potential for conservative management.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608261460228 - Supplemental material for What is the effect of the assistance on the risk of transfer to HD after an unplanned peritoneal dialysis initiation? A cohort study with data from the RDPLF
Supplemental material, sj-docx-1-ptd-10.1177_08968608261460228 for What is the effect of the assistance on the risk of transfer to HD after an unplanned peritoneal dialysis initiation? A cohort study with data from the RDPLF by Ivan Fred Djomkam, Clémence Béchade, Antoine Lanot, Maxence Ficheux, Thierry Lobbedez and Annabel Boyer in Peritoneal Dialysis International
Footnotes
Acknowledgements
We would like to thank Denis Crousle and Laurence Bougault for their contributions to this work, in evaluating the topic and content of the study. We would like to express our gratitude to all patients, nurses, and nephrologists in the renal units who provided data to the RDPLF.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author contributions
I.F.D. designed the study, analysed and interpreted the data, and drafted the manuscript. C.B., A.L., M.F., and T.L. interpreted the data and provided intellectual content of critical importance. A.B. designed the study, interpreted the data, and corrected the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The data presented in this study were provided by the RDPLF which has the approval of the French National Ethics Committee (Commission Nationale de l'Informatique et des Libertés– Number 542668). The study was approved by the data provider. Additional written informed consent from participants was not required for the study presented in this article in accordance with national guidelines. We have received written and informed consent for the publication of the clinical data of the 2 patients who contributed to the study by their verbatim. Written consent was not required as this is an ob servational study analysing data from a national registry, the RDPLF, which has the approval of the French National Ethics Committee (Commission Nationale de l'Informatique et des Libertés– Number 542668). Patients are informed at the inclusion in the registry that their data are collected and might be analysed/published. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines (STROBE 2008).
Informed consent
None was needed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.