
Abstract
Background
Peritoneal dialysis (PD)—associated peritonitis remains a leading cause of hospitalization, technique failure, and transfer to in-center hemodialysis, with touch contamination during connections accounting for many episodes. Although shrouded connectors and “flush before fill” mechanisms reduce contamination risk, most automated peritoneal dialysis (APD) systems incorporate recessed fluid paths on only one side of the tubing–bag interface, potentially allowing bacterial transfer. We evaluated whether bilateral shrouded connectors with recessed fluid paths reduce bacterial contamination during simulated APD therapy.
Methods
In vitro microbiological testing was performed using three APD systems: Vantive/Baxter Claria™ (System A), Fresenius Liberty™ (System C), and Simergent Archimedes™ (System B). Connectors were deliberately contaminated with Staphylococcus aureus to simulate touch contamination, followed by a simulated APD treatment. Bacterial growth was quantified from pre-therapy flush fluid and the first patient fill (“mock peritoneum”). Agar imprinting was used to assess bacterial distribution relative to connector geometry.
Results
Bacterial growth adjacent to the fluid path was observed with contaminated System A connectors but not with System B or System C, where growth was confined to the shroud. Quantitative cultures demonstrated markedly higher bacterial transfer with System A compared with System B and System C across both flush and mock peritoneal samples. Systems B and C employing bilateral shrouded, recessed connectors showed bacterial counts several orders of magnitude lower. All aseptic controls were sterile.
Conclusion
Bilateral shrouded connectors with recessed fluid paths substantially reduce transfer of touch contaminants during simulated APD therapy. This design may mitigate a major mechanism of PD-related peritonitis, warranting clinical evaluation.
Keywords
Introduction
Peritoneal dialysis-associated peritonitis remains a leading cause of both hospitalization and peritoneal dialysis (PD) discontinuation or transfer to in-center hemodialysis (ICHD), and continues to be a major contributor to mortality among patients treated with PD.1–7 In addition to its substantial clinical impact, peritonitis exacts a heavy fiscal burden due to emergency department visits, hospitalizations,8,9 and transition to higher-cost kidney replacement therapies. 10 Fear of developing peritonitis remains a significant patient-related obstacle to broader PD uptake. 11
Most PD-associated peritonitis episodes result from touch contamination during consumables setup, in which inadvertent breaks in sterile technique allow bacteria to enter the peritoneal cavity.1,12,13 Coagulase-negative staphylococcal species and Staphylococcus aureus, common components of normal skin flora, account for approximately half of all cases. 2 To mitigate this risk, PD delivery systems underwent major design modifications in the 1990s and early 2000s, including twin-bag Y-set systems,14,15 incorporation of “flush before fill” mechanisms,16,17 and the transition from spike to shrouded (protective outer sleeve) ¼ turn Luer-type connectors on the automated peritoneal dialysis (APD) solution bag. 18 Recessing the fluid path into the shroud, rather than having it extend beyond the outer shroud surface, further reduces the risk of touch contamination (Figure 1).
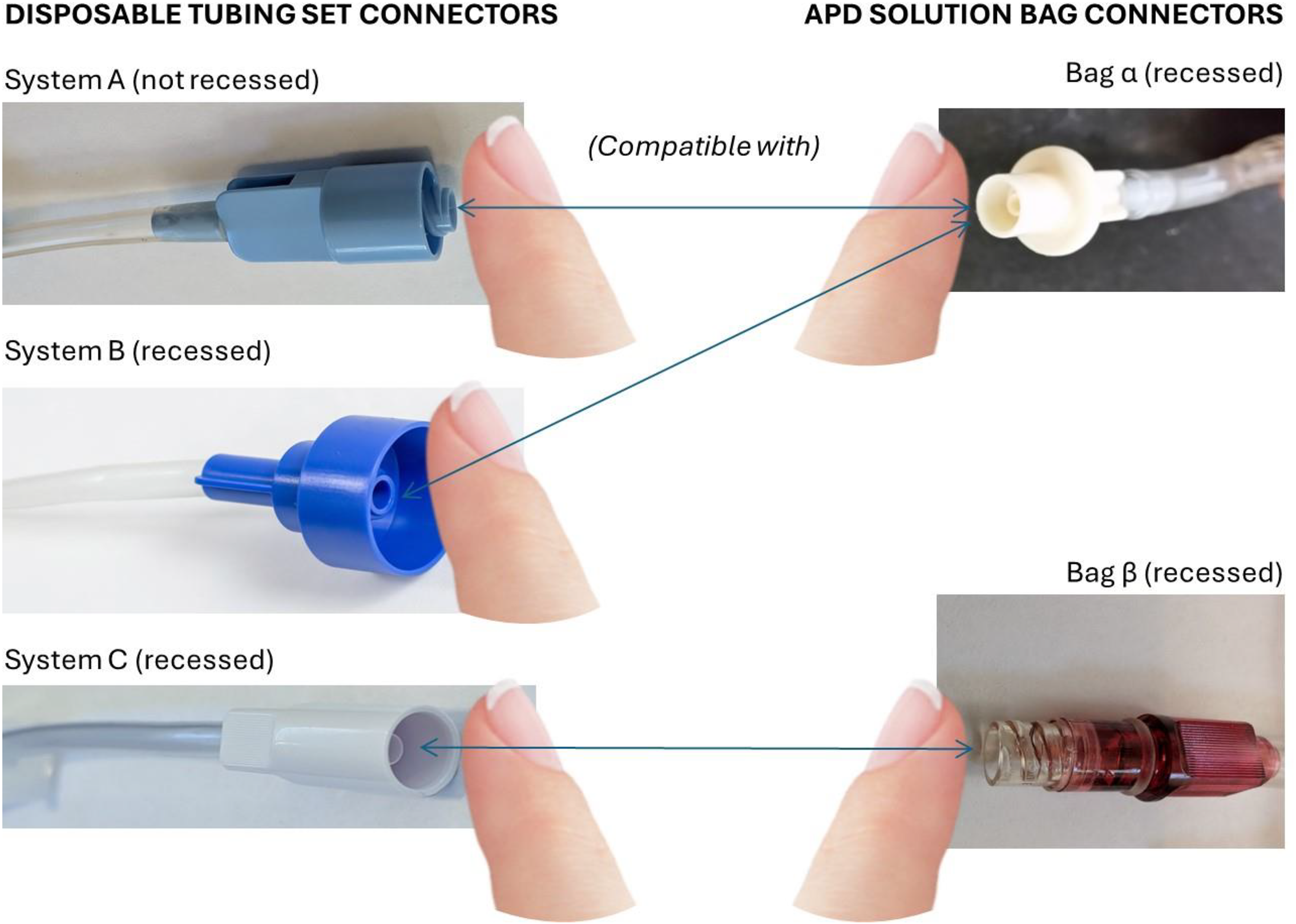
Tubing set and APD solution bag connectors.
Despite these advances, many currently available APD systems incorporate recessed, shrouded fluid paths on only one side of the bag/tubing connection, leaving the opposing connector susceptible to contamination. Given that a single nightly APD therapy requires multiple bag connections using multiple tubing set lines (e.g., one for the heater bag, supply bag, and optional last fill bag), these vulnerabilities represent repeated opportunities for inadvertent contamination.
Infection prevention has been identified as a core outcome by the Standardized Outcomes in Nephrology (SONG) PD Initiative. 19 In response to this and other patient-prioritized unmet needs, a novel APD cycler (Archimedes™, Simergent) with a tubing set enabling bilaterally shrouded connectors and recessed fluid paths was developed and recently cleared by the US Food and Drug Administration. 20
We evaluated the ability of this bilateral, recessed, shrouded tubing set connector system to prevent transfer of touch contaminants into the fluid path using in vitro microbiology testing, and compared its performance with the two most widely used commercial APD cycler systems in North America, one of which is also commercially available globally.
Materials and methods
Automated peritoneal dialysis systems
Three APD systems and their associated tubing set connectors were included in this evaluation: Vantive/Baxter's globally available Claria™ system (System A, which shares the same bag connectology as their Amia™ system), Fresenius’ Liberty™ system (System C), and the Simergent Archimedes™ system (System B).
The female connector of both System A and System B APD tubing sets was each coupled to the shrouded male connector of 2.5% dextrose monohydrate Baxter Dianeal™ APD solution bags (Bag α). The System B tubing set shrouded recessed female connector was designed with matched threading to be mated with the shrouded recessed male Bag α APD solution connector.
Both System A and System B female tubing set connectors have shrouds, but the latter has a recessed fluid path, whereas the fluid path on the former is not recessed, extending beyond the end of the shroud (Figure 1). Unlike Systems A and B, the shrouded connector of the System C tubing sets is male in orientation but also contains a recessed fluid path. System C tubing sets were coupled with the female connectors of 2.5% dextrose monohydrate Fresenius Delflex™ APD solution bags (Bag β) (Figure 1).
While Bag α used with Systems A and B contains a recessed shrouded connector configuration, Bag β contains an internal septum that is punctured during connection to the System C tubing set connector. All APD solution bags and tubing sets were fresh, intact, and within expiry dates when used for experiments.
Preparation of bacterial challenge suspensions and contaminated agar surfaces
All experiments were conducted at the Lawson Research Institute, St Joseph's Health Care, London, Ontario, CA.
S. aureus was the organism chosen for the touch contamination experiments, given its common culpability in touch contamination. Bacterial cultures were prepared by inoculating 10 mL tryptone soy broth with a colony of bacteria and growing at 37
Touch contamination procedure
Tubing set connectors—either male or female—from each APD system or PD solution bag connectors were pressed against either the S. aureus covered agar plate or an aseptic TSA plate (control) with the goal of simulating touch contamination on one side of the connection per experiment (Figure 2). Following the tubing set or bag connectors being pressed to the bottom of either agar plate, mating connections of contaminated or uncontaminated male with female connectors were then made after one intentional misaligned connection, whereby the bag distal end was touched to the distal end of the tubing set connector before making an axially-centered connection. Nine different experimental scenarios were tested, each repeated in an identical fashion 3–5 times, each with a new set of respective sterile PD supplies and associated connectors (Table 1). A simulated APD treatment was then run using each of the respective APD cyclers. The first 50 mL of the drain line fluid was collected in a sterile tube—this was the flush fluid before the fill (Sample 1)—and the first patient fill cycle was then collected in another sterile tube (Sample 2). The latter was considered the “mock peritoneum.” Each collection tube was centrifuged to collect bacterial cells, resuspended in 1 mL PBS, and 100 µL from each was spread on a fresh TSA plate, with colony counts determined from each collection plate. Concurrently, an aliquot of the 1 mL suspension was serially diluted and spot-plated in order to enumerate any samples that contained too many colonies for the directly plated aliquot. PD supplies were discarded after each simulated therapy completion (single use).
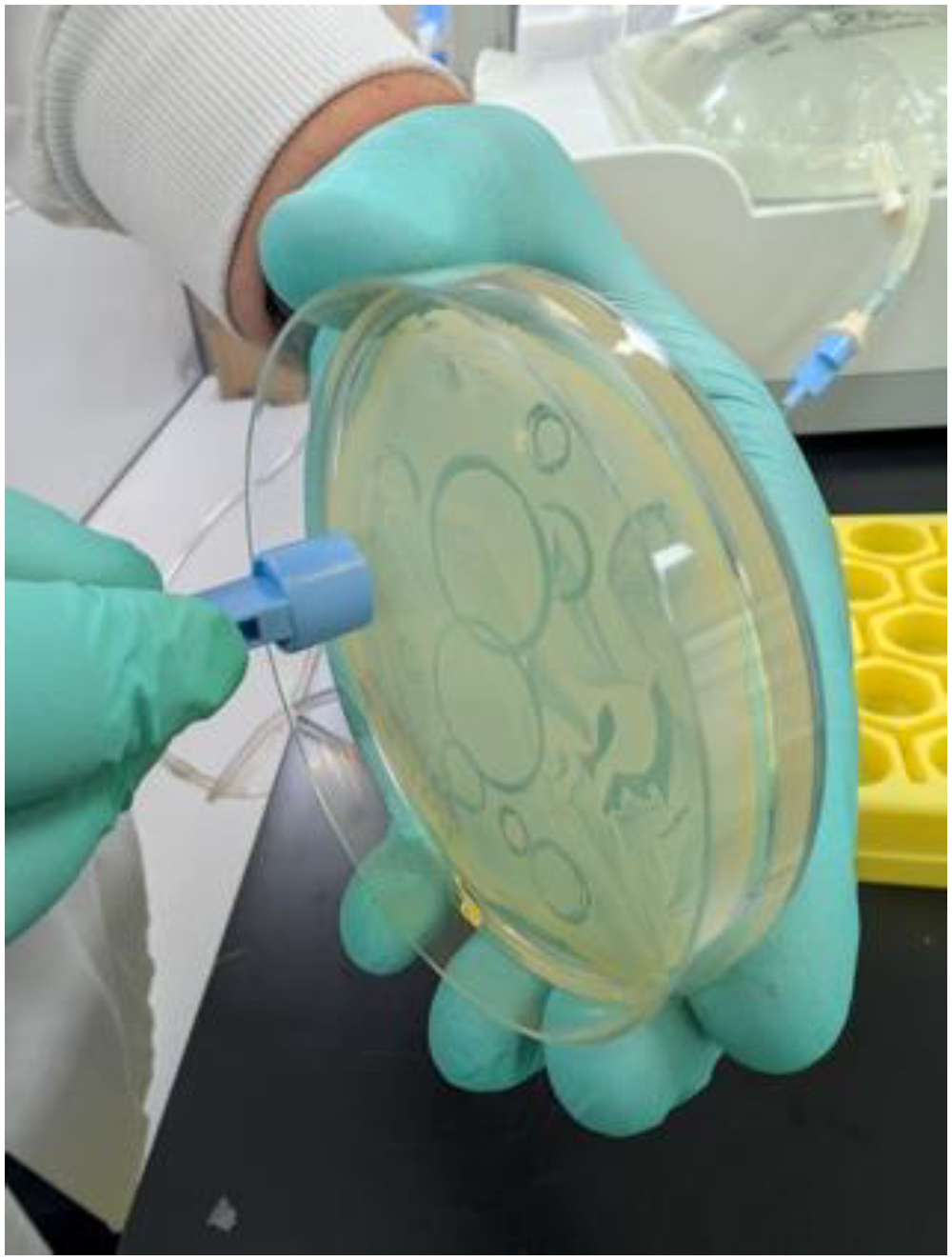
Contaminating connectors with S. aureus.
Simulated touch contamination experimental scenarios.
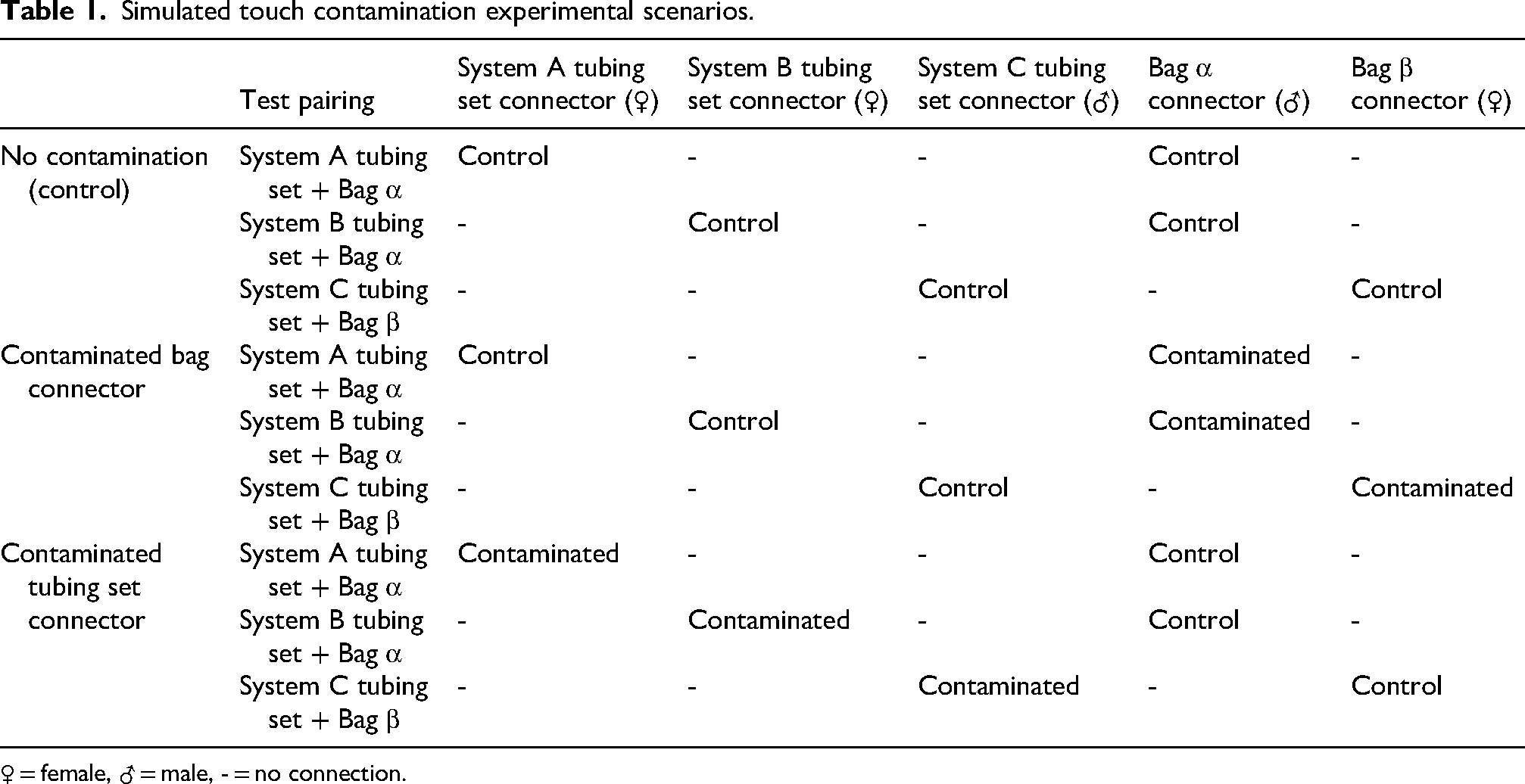
♀ = female, ♂ = male, - = no connection.
In associated but separate experiments with a new set of PD supplies, following both new tubing set and PD solution bag connectors’ contamination with S. aureus covered plates using the same method described above, the connectors were then pressed against clean TSA plates and cultured overnight at 37°C. The pattern of bacterial growth was examined qualitatively, with specific attention to evidence of bacterial growth in the area of the connector fluid path.
Results
Contaminated tubing set connectors pressed onto aseptic agar plates revealed a specific bacterial growth pattern (Figure 3A) wherein S. aureus growth was seen only in the vicinity of the shroud for System B and C tubing set connectors, with no apparent growth around the area of the fluid path. Conversely, bacterial growth patterns were seen in the vicinity of the fluid path for System A tubing set connectors. Contaminated PD bag connectors pressed onto aseptic agar plates demonstrated S. aureus growth only in the vicinity of the shroud for both PD bag connectors tested (Bag α and Bag β), as shown in Figure 3B.
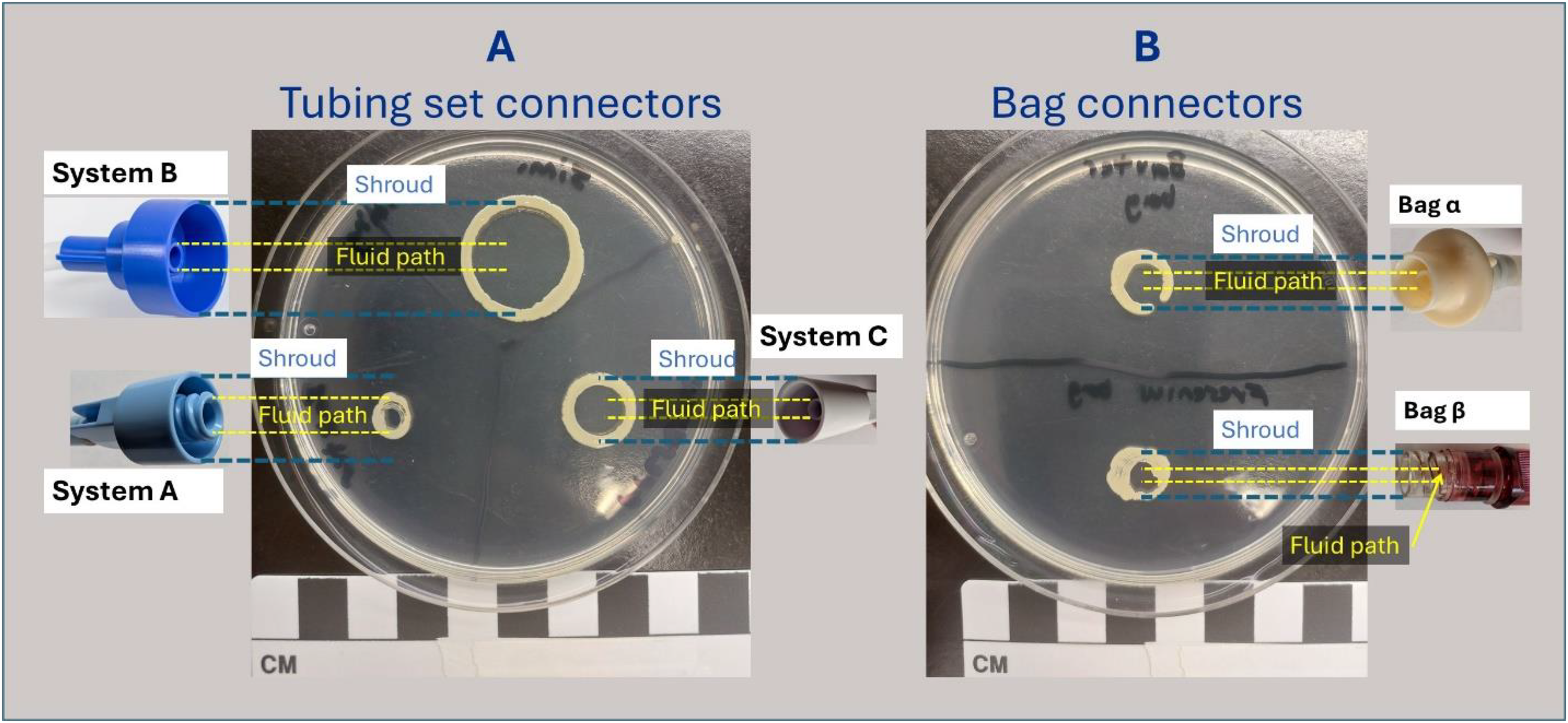
Qualitative growth patterns for contaminated tubing set (A) and APD bag connectors (B). Shrouded area (blue) and fluid path area (yellow) projected onto the agar plate are demonstrated with their respective bacterial growth sites.
Bacterial growth from Sample 1 aliquots (pre-therapy fluid flushed to the drain line) through the contaminated tubing set connector-PD bag connector following a simulated therapy for each respective APD system consistently demonstrated the greatest amount of S. aureus growth by several orders of magnitude with System A (Supplemental Figure 1). Mean cfu/mL was 650, 1.19 × 106, and 0 for System B, System A, and System C, respectively, for tubing set contamination; mean cfu/mL was 12, 3.15 × 104, and 0 for PD bag connector contamination. Similar findings were seen with Sample 2 aliquots (patient line/mock peritoneum) following contamination of either the PD bag connectors or tubing set connectors (Figure 4). The mean viable microbial growth in System B, System A, and System C for tubing set contamination was 284, 4.36 × 105, and 0 cfu/mL, respectively. For PD bag connector contamination, the mean viable microbial growth was 238, 3.44 × 103, and 0 cfu/mL, respectively. The full set of Sample 1 and Sample 2 test results is available in Supplemental Table 1.
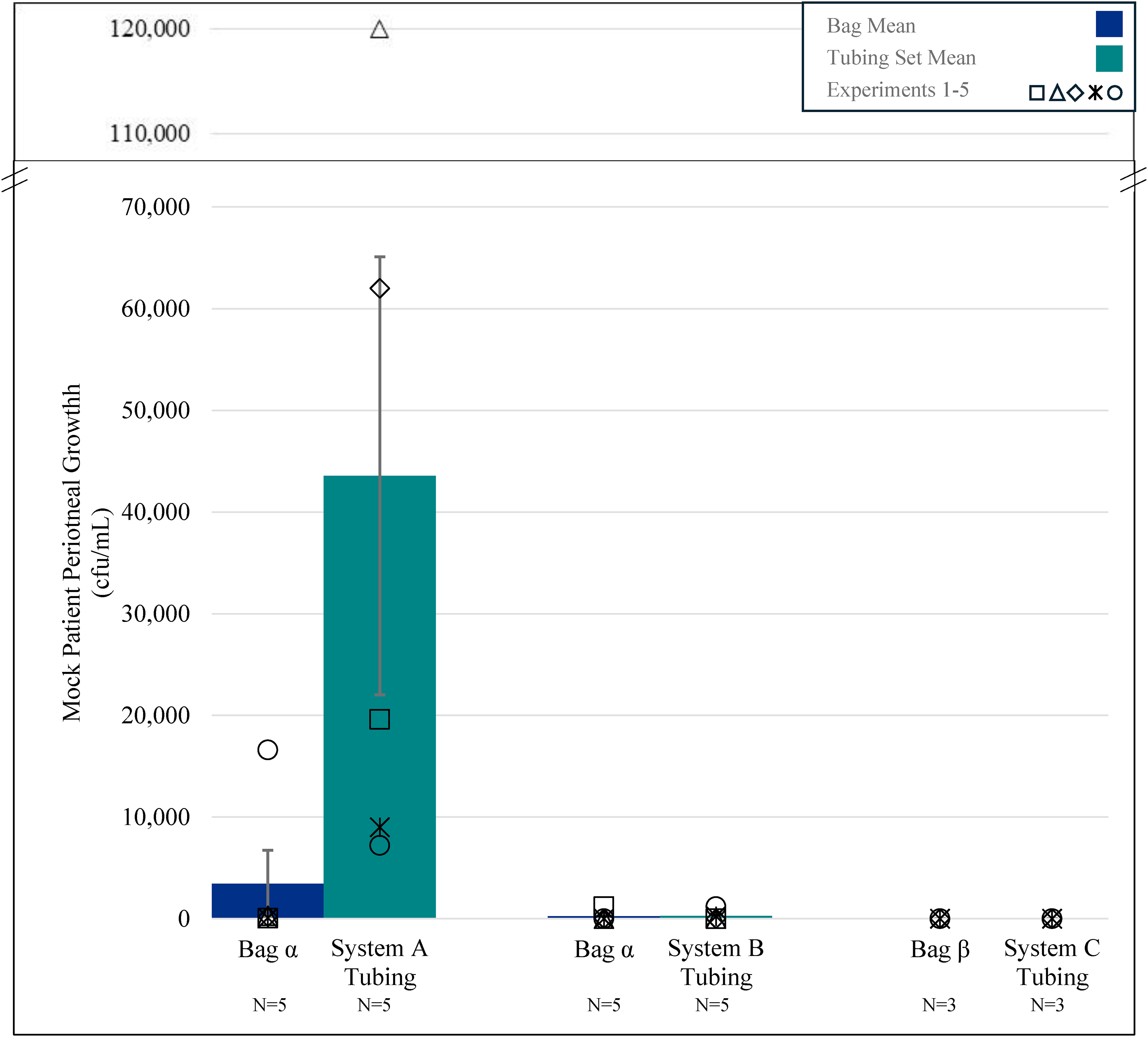
Mock patient peritoneal growth with designated connector contamination for sample 2 aliquots (individual experiments are indicated by plot symbols).
All of the control experiments (aseptic tubing set paired with aseptic bag connection) showed 0 cfu/mL growth in the mock peritoneum.
For System A, when contaminating the tubing set connector, the mock peritoneum showed one order of magnitude lower mean colony growth (4.36 × 105 cfu/mL) than the pre-therapy flushed fluid (1.19 × 106 cfu/mL). Similarly, when contaminating the Bag α connector and pairing it with the aseptic System A tubing set, the mock peritoneum showed one order of magnitude lower mean colony growth (3.44 × 103) than the flushed fluid (3.45 × 104 cfu/mL).
For System B, when contaminating the tubing set, the mock peritoneum showed less than ½ of the colony growth compared to the flushed fluid (284 vs. 650 cfu/mL). Also, when contaminating the Bag α connector and pairing it with the aseptic System B tubing set, one order of magnitude reduction of colony growth was seen (12 vs. 238 cfu/mL).
For System C, no growth was seen in either the mock peritoneum or the flushed fluid, and thus, no reduction in growth was seen for the three replicates performed when contaminating either the tubing set or bag connectors.
Discussion
This in vitro microbiological study demonstrates that bilateral shrouded tubing set connectors with recessed fluid paths on both sides of the tubing-set–PD solution bag interface effectively prevent transfer of S. aureus touch contaminants into the sterile fluid path during simulated PD therapy. In contrast, systems in which the recessed fluid path is present on only one side of the tubing set–bag interface were significantly more susceptible to bacterial transfer, despite the presence of “flush before fill” mechanisms. These findings suggest that fully shrouded, dual-recessed connection systems may substantially mitigate the risk of touch contamination—a leading cause of PD-associated peritonitis.
In both Sample 1 (flush) and Sample 2 (mock peritoneum) aliquots, there was a markedly elevated level of bacterial growth following contamination of the System A tubing set connectors. Alternatively, the novel System B cycler tubing set with shrouded solution line connectors and a recessed fluid path showed several orders of magnitude less growth compared to the System A tubing set connectors using the same Bag α. Contaminated System C tubing and PD solution bag connectors performed comparably to the System B connectors mated with shrouded Bag α connectors (containing a recessed fluid path). The absence of bacterial growth with System C may have been due to the smaller sample size of N = 3, as the first three replicates for System B also showed no growth. Alternatively, it may be due to the fact that the Bag β has a septum that is punctured in the process of making a connection to the tubing set connector and thus may wipe away some contamination in the process, while the Bag α used for both System A and System B does not have this septum.
Variability in cfu/mL counts was apparent within single connector systems across the multiple experiments. The differing numbers of visible colonies between experiments are not unexpected, even with an identical technique applied across experiments, given uneven transfer of bacteria to the connectors related to imperceptible differences in how hard (pressure) or how long (time) the connectors were pressed into the S. aureus-covered agar plate.
While the reduction in mean colony-forming units in the mock patient's peritoneal fluid compared to the pre-therapy flushed fluid clearly demonstrates the advantages of the “flush before fill” technology, it also demonstrates the need for further precautions in a system with a recessed fluid path on only one side of the tubing set/bag connection.
To prevent peritonitis, minimizing the amount of contamination reaching the peritoneum is imperative. System B and System C showed three to five orders of magnitude lower growth in the mock peritoneum than System A when contaminating respective tubing set connectors (284 vs. 0 vs. 4.36 × 105 cfu/mL). Similarly, both System B and C showed one to three orders of magnitude lower growth than did System A when contaminating the Bag α connectors (aseptic System A and System B tubing) or the Bag β connectors (238 vs. 0 vs. 3.44 × 103 cfu/mL, respectively).
A high bacterial inoculum (106 cfu/mL) was deliberately used to challenge the connection systems and ensure reliable transfer of organisms to the connectors, allowing proof of concept. Although this concentration may seem greater than what patients performing PD at home might encounter, microbiologic data demonstrate that a substantial bacterial burden can be present on the hands, particularly beneath the fingernails. Studies have demonstrated mean subungual bacterial densities of approximately 106 cfu before handwashing and about 105 cfu even after repeated washing. 21 This is similar to the bacterial load used in our experiments and is consistent with concentrations used in prior studies examining touch contamination during PD. 16 Additionally, cfus for Escherichia coli, fecal coliforms, and S. aureus have reached levels as high as 1 × 106, 1 × 108, and 1 × 106, respectively, in published studies of hand cultures of global populations. 22
Although appropriate handwashing can reduce bacterial burden, adherence may decline over time. One study reported that approximately 51% of patients who were initially taught proper handwashing technique were no longer consistently using it after six months of therapy. 23 Thus, while reinforcement of effective hand hygiene remains essential for reducing contamination and peritonitis risk, these observations highlight the importance of incorporating mechanical safeguards in addition to behavioral measures.
Peritonitis remains the principal infectious complication of PD and is a major contributor to technique failure, hospitalization, and mortality.1–7 Although improvements in training and connection technology have reduced incidence rates over the past two decades, “touch contamination” continues to account for nearly half of all peritonitis episodes, most often due to skin organisms such as S. epidermidis and S. aureus.1,2,12,13 Prior connector innovations, such as the adoption of shrouded or Luer-lock systems and “flush before fill” mechanisms, have reduced but not eliminated contamination risk. However, the current results indicate that partial design improvements—specifically, shrouding and recessing the fluid path on only one side of the connection—leave the system vulnerable to contamination of the unprotected component. This vulnerability becomes especially relevant during typical APD operation, where up to three separate bag-set connections occur nightly, multiplying opportunities for touch contamination.
The marked reduction in bacterial growth observed with the mating of connectors incorporating a recessed fluid path on both mating components highlights the functional benefit of a bilateral protective interface. By physically shielding the mating components from inadvertent contact and maintaining a recessed sterile fluid path on both sides, this design minimizes bacterial transfer even under deliberate contamination conditions. Furthermore, comparable results between Systems B and C—both employing shrouded, recessed connectors—underscore the importance of complete enclosure and fluid path separation rather than reliance on one-sided protective features. The “flush before fill” step remains a valuable secondary safeguard, but these findings suggest that optimal infection prevention requires a holistic approach integrating both mechanical (connector geometry) and procedural (flush) controls.
Beyond infection prevention, improvements in connection safety have implications for patient confidence and PD uptake. Fear of peritonitis is among the most frequently cited barriers to initiating or continuing PD therapy. 11 Enhancing connection design to minimize touch contamination risk may thus contribute not only to clinical safety but also to patient empowerment and acceptance of home-based therapies. System B, designed with patient-preferred usability and safety as central priorities, 24 aligns closely with the SONG-PD initiative, which identified infection prevention as a top outcome of importance to patients and clinicians. 19
This study has several limitations. First, it was performed in vitro under controlled laboratory conditions, which do not fully replicate the complexity of real-world patient environments where factors such as varying hand hygiene, ambient contamination, and connector handling behaviors may influence infection risk. Second, only S. aureus was used as the challenge organism; while it represents a major clinical pathogen, testing with additional species such as coagulase-negative staphylococci or Pseudomonas species could broaden applicability. While all experiments were performed by staff of the independent Lawson Research Institute, potential bias in the duration or pressure applied to bacteria-containing agar plates cannot be excluded. However, blinding would have been impossible given the distinct shapes of the different connectors and the commercial packaging of sterilized supplies.
Finally, the experiments simulated single contamination events; cumulative effects of contaminating multiple bag connections for the same therapy were not evaluated. Given the potential for three (3) PD solution bag connections with each therapy (e.g., heater bag, supply bag, optional last fill bag), there are up to three opportunities for touch contamination with each nightly treatment. Nevertheless, the consistency of the results across multiple replicates and APD systems provides compelling preliminary proof of concept evidence of the protective efficacy of the dual-shrouded, recessed fluid path connector design. Definitive superiority of this design will require randomized controlled trials or collection of registry data comparing clinical outcomes between differing connectology systems.
In conclusion
Supplemental Material
sj-docx-1-ptd-10.1177_08968608261461078 - Supplemental material for An in vitro comparison of bacterial touch contamination prevention between a novel APD cycler connector and existing APD connectors
Supplemental material, sj-docx-1-ptd-10.1177_08968608261461078 for An in vitro comparison of bacterial touch contamination prevention between a novel APD cycler connector and existing APD connectors by James A Sloand, Jeremy P Burton, Chris I Munday, Arsh K Jain, Osama El Shamy, Rick Pendergraft and Steve J Lindo in Peritoneal Dialysis International
Footnotes
Ethical considerations
Ethical approval was not required for this in vitro study.
Consent for publication
Human subjects were not involved in this in vitro study.
Author contributions
J.A.S. and S.J.L. conceived the project and wrote the first draft of the manuscript. J.P.B., C.I.M., and S.J.L. conducted all research and collated the data. All authors analyzed the data, reviewed, and edited the manuscript, and approved the final version.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ownership interests in Simergent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All supplies (tubing sets, PD solution bags, cyclers) for the research were funded by Simergent LLC. Lawson Research Institute graciously provided all necessary microbiological equipment and conducted all experiments at no cost to the investigation.
Data availability
The datasets generated and analyzed in the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.