
Abstract
There is a paucity of information regarding QTc prolongation in critically ill patients. A prospective observational study was conducted to assess the incidence and predictors of QTc prolongation associated with medications in intensive care unit (ICU) patients. Consecutive adult patients prescribed prespecified QTc-prolonging medications were assessed for development of the combined incidence of QTc >500 ms at anytime and QTc increase >60 ms above baseline. Over 3 months, 200 consecutive patients (63 ± 18 years; 52% female; 73% Caucasian; baseline QTc 447.3 ± 51.5 ms) were evaluated. The primary end point occurred in 48% of the patients (QTc >500 ms 40%, QTc increase >60 ms 29%). The majority of patients experienced a QTc >470 or 450 ms (60.5%). Mean increase in QTc at 48 hours was 20 ± 35 ms. Upon multivariate analysis, length of stay [odds ratio 1.30, 95% confidence interval (1.15, 1.47)] and baseline QTc [1.01 (1.01, 1.02)] were associated with an increased risk for the primary end point, while beta-blockers [0.41 (0.20, 0.81)] were associated with a risk reduction. In conclusion, increased risk of proarrhythmia, as assessed by QTc prolongation, occurs in the majority of ICU patients when prescribed medications with electrophysiologic properties. Increased vigilance is warranted. The possible protective effect of beta-blockers requires confirmation.
Ventricular repolarization is monitored by examining the QT-interval (QT; or the corrected QT-interval [QTc]) on an electrocardiogram (ECG). The QTc standardizes the QT interval duration for heart rate and allows for interpretation when obtained at different times. Delayed repolarization most often manifests as prolongation of the QTc. 1 The corrected QT-interval prolongation carries the risk of developing Torsade de Pointes (TdP), a potentially life-threatening polymorphic ventricular arrhythmia. Torsade de Pointes is associated with a poor prognosis and risk of sudden death. 1,2 The exact incidence of TdP is poorly characterized; however, the risk of developing TdP increases proportionately with QTc duration. 1,3-5
Drug therapy is the most common etiology associated with QTc prolongation. 2 Drugs capable of prolonging repolarization by affecting sodium and potassium ion currents are associated with increased risk of proarrhythmia. These include most antiarrhythmics, fluoroquinolones, phenothiazine antipsychotics (chlorpromazine, thioridazine), butyrophenones (haloperidol, droperidol), macrolides (erythromycin, clarithromycin), and pentamidine. In addition, interactions involving these drugs also have the potential to amplify their electrophysiologic effects. The risk of developing drug-induced TdP is also increased by other predisposing factors including older age, female gender, cardiac disease, preexisting bradycardias, electrolyte imbalances, and congenital long QT (LQT) syndrome. 1,2,6
The risk associated with QTc prolongation has received much more attention in recent years, resulting in the US Food and Drug Administration implementing more rigorous guidelines for assessing the proarrhythmic potential of new drugs during the approval process. However, medications known to cause prolongation of the QTc are still commonly prescribed without increased vigilance. In a recent survey of health care practitioners, including cardiology specialists, it was shown that less than two thirds of practitioners could accurately identify medications and/or medication regimens that may cause QTc prolongation. 7 Issues related to monitoring and adjusting medications with proarrhythmic potential are usually conducted after a patient has already experienced QTc prolongation and hence are needlessly exposed to increased risk of adverse events.
Currently, there is a paucity of information regarding the incidence and predictors of QTc prolongation in critically ill patients admitted to an intensive care unit (ICU) setting. Due to the large number of drugs patients receive in the ICU, the inherent aberrations in electrolytes, and the presence of preexisting risk factors, it is reasonable to expect a high incidence of QTc prolongation and ventricular ectopy in this patient population. The purpose of this study was to prospectively evaluate the incidence and predictors of significant QTc prolongation in adult medical and surgical ICU patients who were prescribed a medication known to affect ventricular repolarization and thus prolong the QTc.
Materials and Methods
Study Design
In a prospective, observational study, data regarding QTc prolongation was collected on consecutive medical–surgical ICU patients at The Nebraska Medical Center from December 1, 2003, to February 2, 2004. Any adult patient (19 years of age or older) prescribed prespecified high-risk drugs for QTc prolongation were included. Drugs included in the protocol were antiarrhythmics (amiodarone, sotalol, dofetilide, quinidine, disopyramide, procainamide), fluoroquinolones (moxifloxacin, levofloxacin, ciprofloxacin, gatifloxacin), erythromycin, and haloperidol. Nonhospital formulary medications known to affect ventricular repolarization were excluded. Patients were excluded if the prescribed QTc protocol drug was discontinued within 24 hours for a nonarrhythmogenic therapeutic reason or no follow-up ECG was ordered. Patients with pacemakers and paced rhythms were also excluded.
Patients in all hospital ICUs (56 total beds) were monitored daily for initiation of a QTc-prolonging drug identified in the protocol. Electrocardiograms were routinely ordered upon admission to the ICU. Upon initiation of a QTc-prolonging drug, the following information was collected: baseline demographics, past medical history, current medical diagnoses, concomitant oral and intravenous medications, laboratory data (serum chemistries, serum creatinine, liver function tests), social history (alcohol and smoking), detailed Acute Physiologic and Chronic Health Evaluation (APACHE II) score, heart rate, and QTc interval. Patients prescribed a prespecified QTc-prolonging drug were followed daily for the resulting effect on QTc duration and incidence of new onset ventricular ectopy. The corrected QT-interval duration was determined by measurement of the QT interval from a 12-lead ECG and correction for heart rate using Bazett’s formula [QTc = QT/(square root RR′)]. The QT interval was uniformly assessed manually using calipers in limb lead II on the first ECG obtained in the morning by one investigator (same investigator was responsible for measuring all QT intervals). The QT interval was averaged over 3 beats in patients with normal sinus rhythm and averaged over 10 beats in patients with an irregular rhythm. Obvious U waves were not included in the measurement of QT interval. Patients with a bundle branch block were included in the overall analysis. The study was approved by the University of Nebraska Medical Center Institutional Review Board.
Statistical Analyses
Descriptive statistics were calculated for the entire study population. The cutoffs for significant effect on QTc interval were derived from recommendations in the US Food and Drug Administration Center for Drug Evaluation and Research document, Clinical Evaluation of QT/QTc Interval Prolongation, and Proarrhythmic Potential for Non-Antiarrhythmic Drugs. 8 The primary end point was the incidence of an electrophysiologic adverse event potentially requiring discontinuation of the medication. An electrophysiologic adverse event was defined as a prolonged QTc interval >500 milliseconds at any time or QTc increase >60 milliseconds over baseline. Secondary end points included incidence of QTc >470 milliseconds in women or >450 milliseconds in men, mean increase in QTc at 48 hours, number of drug discontinuations for prolonged QTc interval (must have been verified with physician as primary reason for discontinuation of medication), and episodes of TdP or new onset ventricular ectopy (>3 beat run of premature ventricular beats, non-sustained ventricular tachycardia [VT] episode lasting at least 5 seconds, sustained VT or ventricular fibrillation [VF]). Two subgroup analyses were also performed, one excluding patients who received amiodarone, and one excluding patients with bundle branch blocks and baseline QTc >500 milliseconds. Amiodarone data were excluded for one subgroup analysis as it can be argued that QTc prolongation with amiodarone does not equate to increased risk of TdP. 9
The relationship between the primary outcome and predictors was examined using logistic regression models. Univariate relationships were first examined and if a predictor was significant at the .2 level, it was retained for further model building. Fisher’s exact test was used for categorical variables and a univariate logistic regression was used for continuous variables. The variables selected for further monitoring were entered into a multivariate logistic regression and a backward selection procedure was used to select those variables significant at the .05 level. All analysis was performed using the SAS System for Windows, version 9.1 (SAS Institute, Cary, North Carolina).
Results
Patient Population
Data were collected on 244 consecutive patients admitted to the ICUs. Forty-four patients were excluded due to the QTc-prolonging drug being discontinued within 24 hours (N = 2) or no follow-up ECG (N = 42). The analyses were conducted on the remaining 200 patients. The mean age of patients included was 63 ± 18 years. There was an approximate equal distribution between genders (female 52%), and the majority of patients were Caucasian (73%). The mean APACHE II score was 14.5 ± 6.2. The most common comorbid illnesses were hypertension (53%), diabetes (28%), coronary artery disease (28%), asthma or chronic obstructive pulmonary disease (24.5%), and history of atrial fibrillation (23.5%). Half of the patients were previous or current smokers (51%) and 18% reported some alcohol consumption. Patients were also receiving a variety of cardiovascular medications including beta-blockers (35%), diuretics (23%), statins (18%), angiotensin II antagonists (18%), and calcium channel blockers (14%). Specific demographic information is outlined in Table 1 .
Baseline Characteristics of Study Population
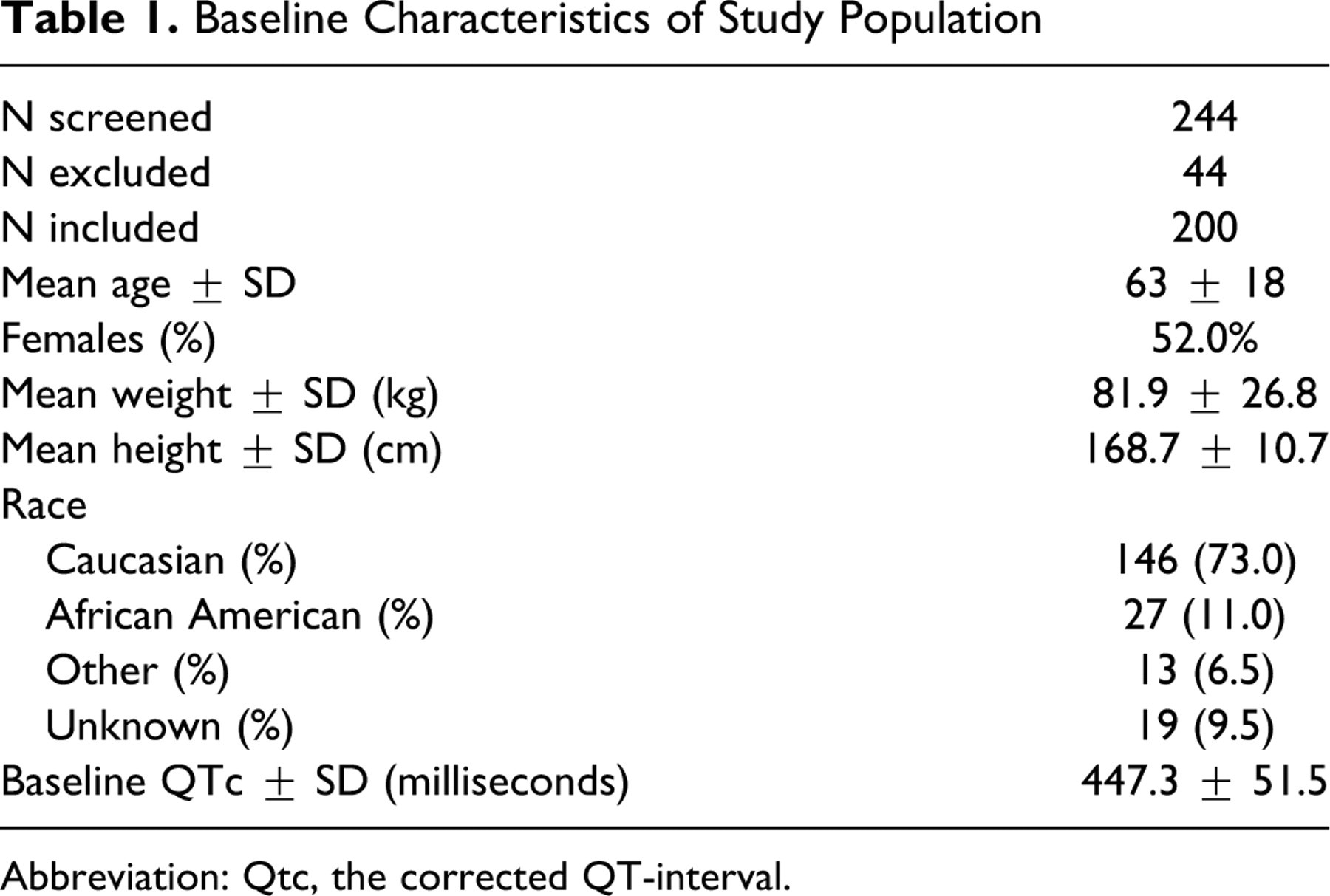
Abbreviation: Qtc, the corrected QT-interval.
There was a high rate of patients who experienced an electrophysiologic adverse event. The primary end point occurred in 48% of patients prescribed a QTc-prolonging medication. The incidence of patients experiencing each component of the primary end point was 40% for a QTc >500 milliseconds, and 29% exhibiting an increase in QTc >60 milliseconds over baseline. The secondary end point of QTc >470 milliseconds (females) or >450 milliseconds (males) occurred in 61% of patients. Despite these electrophysiologic findings, the medication causing the QTc prolongation was discontinued in only 13 patients (7.0%). Elimination of patients receiving amiodarone or those with existing bundle branch block only minimally decreased the incidence of the primary end point. Table 2 summarizes the distribution of the drugs, the mean increase in QTc, and incidence of the primary end point for each drug. Table 3 summarizes the incidence of the various electrophysiologic end points for the entire study population, as well as for subgroup analyses excluding patients who received amiodarone, and excluding patients with a bundle branch block.
Distribution and Effects on QTc of Protocol Specified Medications
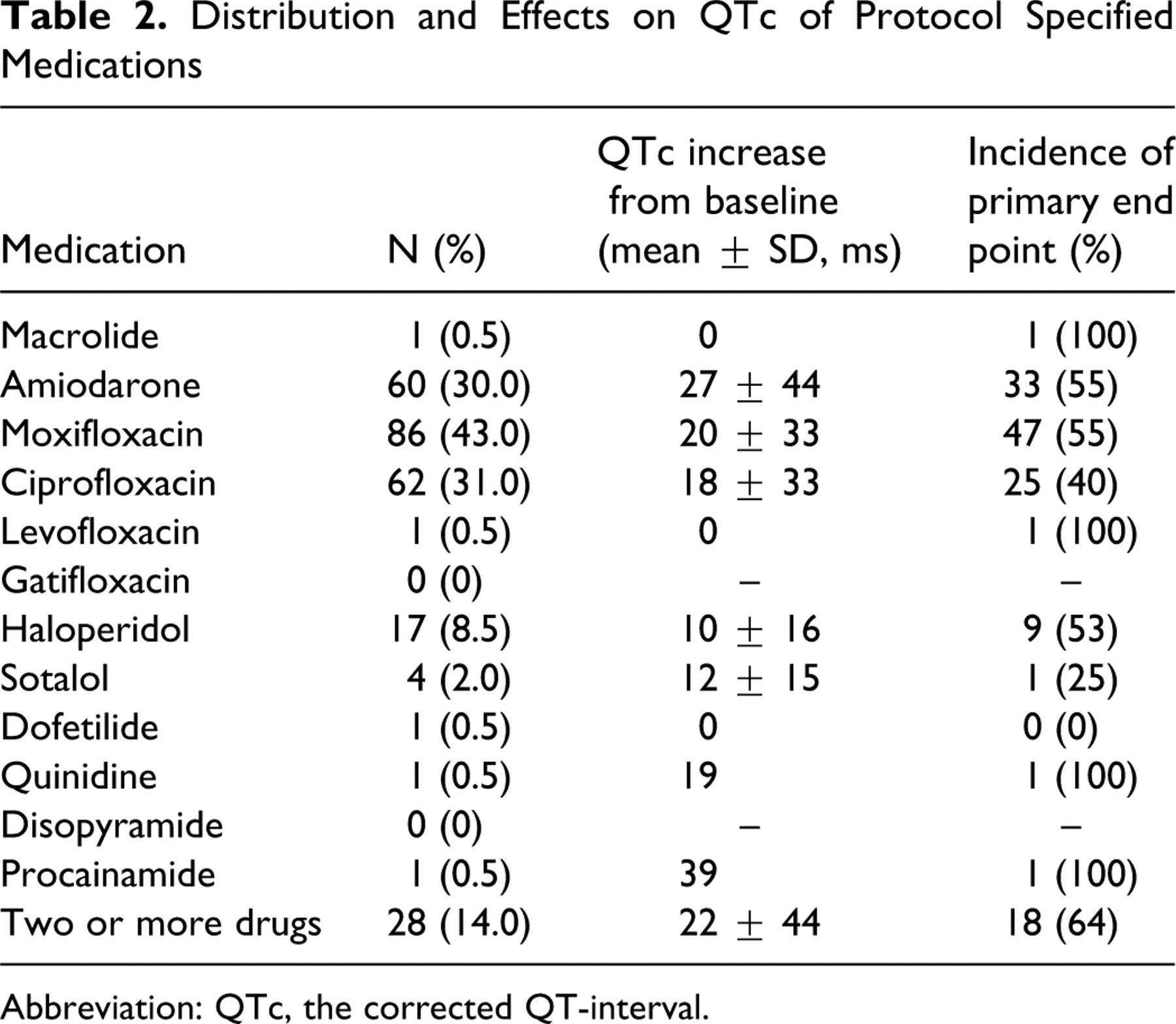
Abbreviation: QTc, the corrected QT-interval.
Electrophysiologic and Clinical End Points
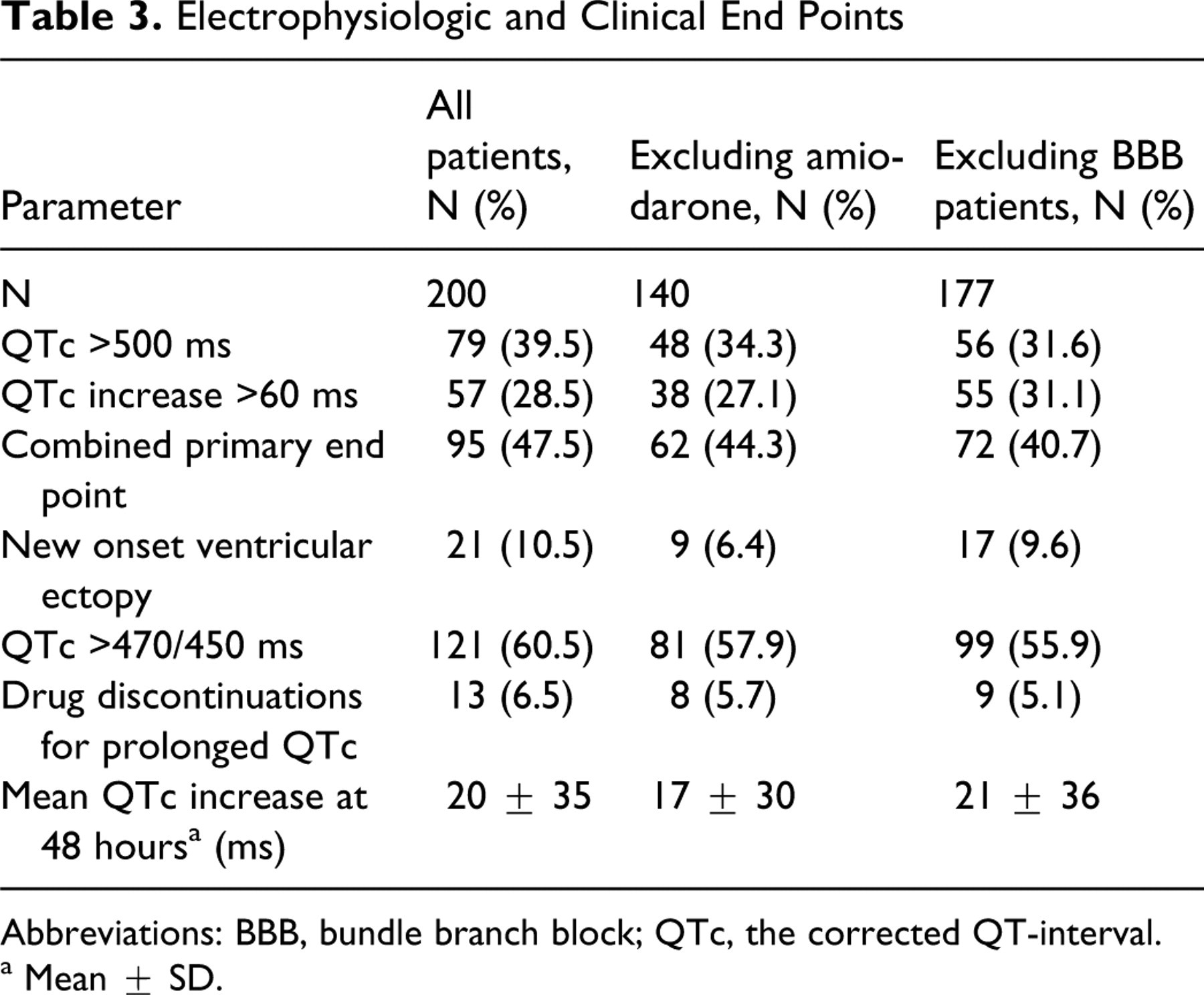
Abbreviations: BBB, bundle branch block; QTc, the corrected QT-interval.
a Mean ± SD.
Univariate and Multivariate Analyses
Baseline characteristics (race, gender, age), medical history (coronary artery disease, chronic heart failure, diabetes, thyroid disease, low serum potassium or magnesium, infection), medications (beta-blocker, calcium channel blocker, vasopressor, or inotrope), disease severity indicator (APACHE II), and specific QTc-prolonging medications (amiodarone, moxifloxacin, ciprofloxacin, haloperidol, combination of QTc-prolonging drugs) were included in the univariate analysis to determine possible predictors of the combined primary end point of QTc >500 milliseconds at any time and/or QTc increase of >60 milliseconds over baseline. Variables included in the analysis and their statistical significance are listed in Table 4.
Univariate Analyses for Predictors of the Primary End Point
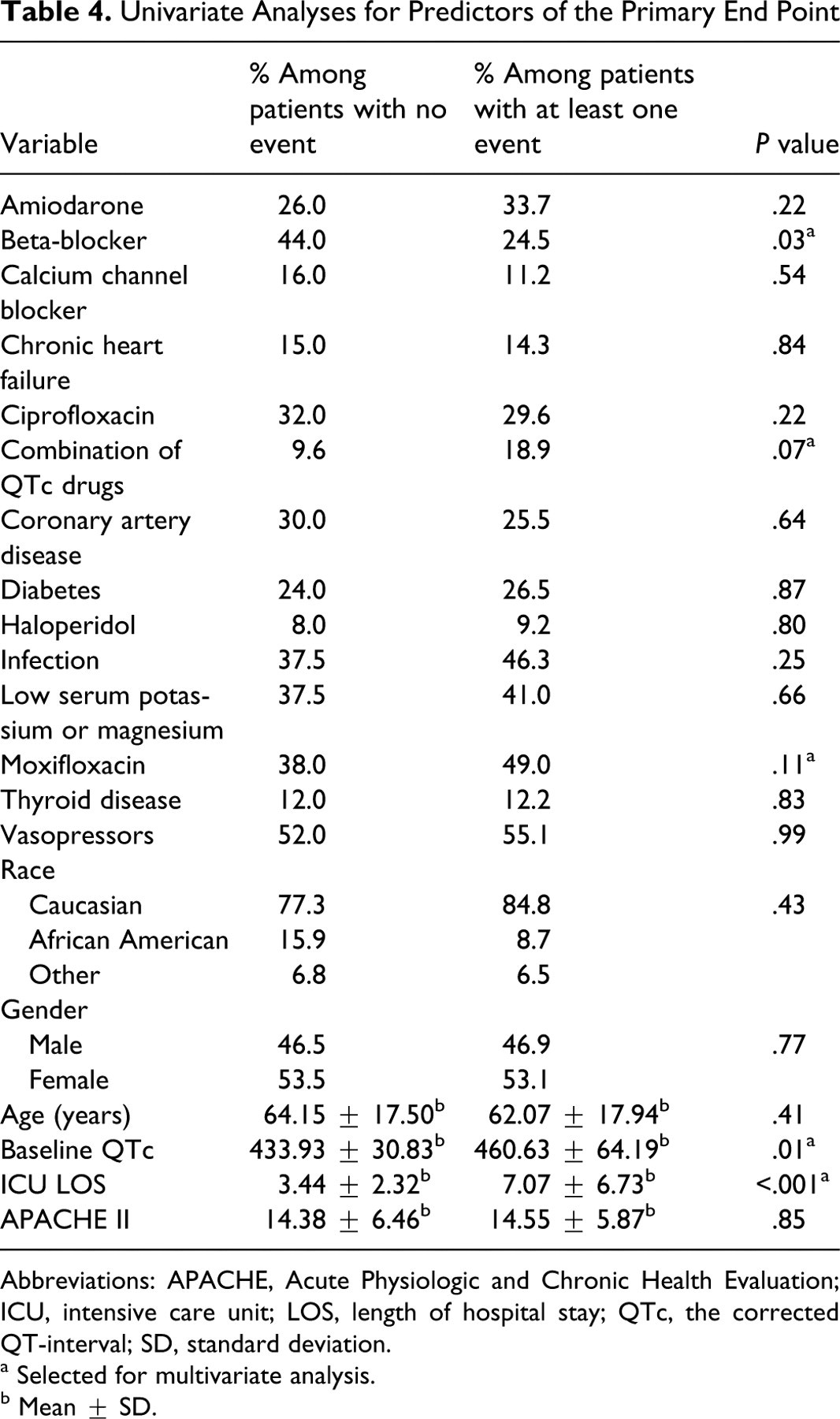
Abbreviations: APACHE, Acute Physiologic and Chronic Health Evaluation; ICU, intensive care unit; LOS, length of hospital stay; QTc, the corrected QT-interval; SD, standard deviation.
a Selected for multivariate analysis.
b Mean ± SD.
From the univariate analysis, the variables entered into the multivariate model were beta-blocker, moxifloxacin, combination of QTc-prolonging drugs, ICU length of stay, and baseline QTc. The variables retained (significant at the .05 level using a backward selection method) for the final model were beta-blocker, ICU length of stay, and baseline QTc. Table 5 gives odds ratios (OR) and 95% confidence intervals (CI) for the final model. Controlling for the other variables in the model, the odds of experiencing the primary end point for a patient taking beta-blockers is 0.41 times the odds for a patient not taking beta-blockers. The odds of experiencing the primary end point are 1.30 times greater for each additional day in the ICU. The odds of experiencing the primary end point are 1.01 times greater for each millisecond increase in baseline QTc. Beta-blockers (OR 0.47, 95% CI [0.23, 0.97], P = .04) and ICU length of stay (OR 1.31, 95% CI [1.16, 1.48], P < .001) retained significance in multivariate analysis excluding patients with a bundle branch block.
Multivariate Predictors of the Primary End Point
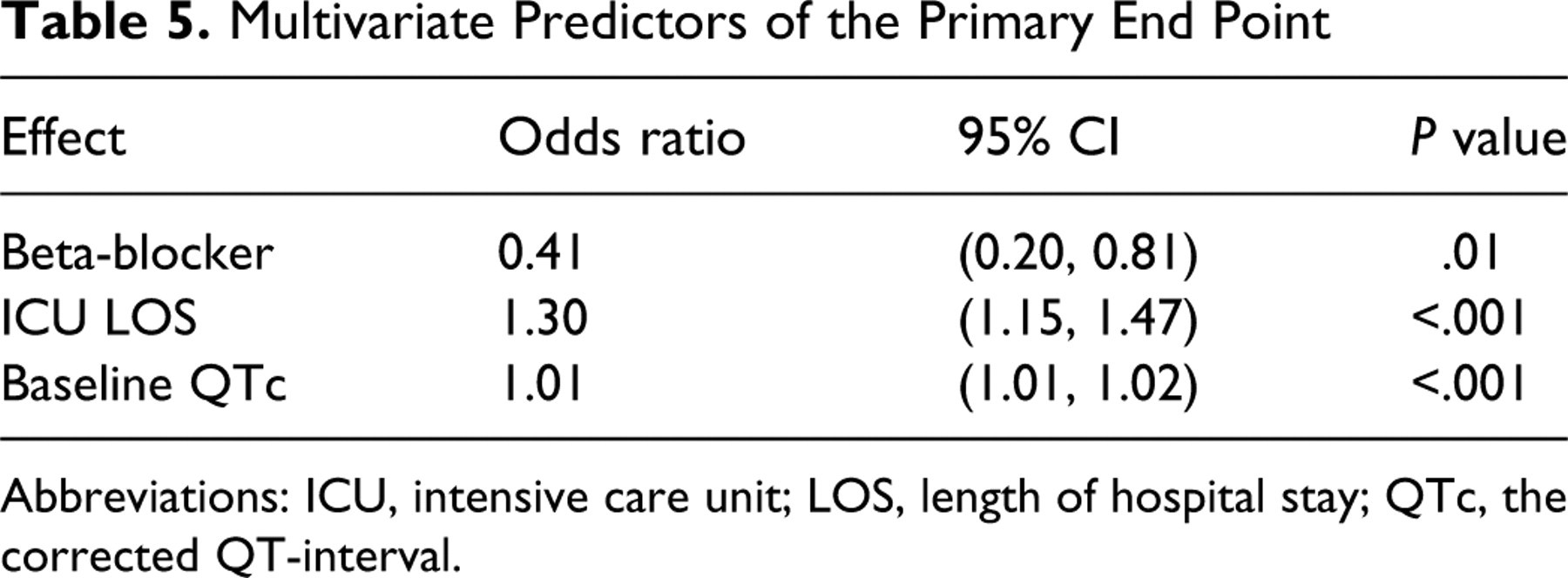
Abbreviations: ICU, intensive care unit; LOS, length of hospital stay; QTc, the corrected QT-interval.
Discussion
To the best of our knowledge, this is the first study to evaluate the incidence of drug-induced QTc prolongation in the medical–surgical ICU setting. The results of our prospective observational study suggest that medical–surgical ICU patients are exposed to a high incidence of significant QTc prolongation when prescribed medications with known electrophysiologic effects on ventricular repolarization. Despite over half of the patients experiencing significant QTc prolongation of greater than 470 milliseconds and 450 milliseconds, for females and males, respectively, medications were discontinued in a minority of patients. Interestingly, the incidence of an electrophysiologic adverse event was not predicted by any demographic characteristic, past medical history, or underlying disease severity as determined by APACHE II score. Exclusion of patients prescribed amiodarone or those with bundle branch blocks only mildly reduced the overall incidence of the primary end point, with no difference in mean increase in the QTc interval.
The multivariate modeling revealed only 3 predictive variables, with patients prescribed a beta-blocker exhibiting a reduced risk. Beta-blockers have long been known to reduce the incidence of ventricular arrhythmias and sudden cardiac death; however, their influence over QT prolongation and risk of TdP remains controversial. The antiarrhythmic properties of beta-blockers are attributed to both blockade of sympathetic stimulation and modulation of repolarization. Beta-blockers have been shown to reduce QTc prolongation, dynamicity and dispersion induced by pharmacologic agents, and diseases such as heart failure, myocardial infarction, and hypoglycaemia. 10-14 Beta-blockers are also generally regarded as first-line therapy for prevention of sudden cardiac death in congenital LQT syndrome. 15 However, this recommendation has been questioned as beta-blockers may not be protective in all forms of the disease, with recent evidence suggesting lack of efficacy in LQT2 and LQT3. 16 Therefore, our results support the notion that concomitant therapy with beta-blockers may reduce the QTc-prolonging effects of some medications, but whether this effect reduces proarrhythmic potential remains to be determined.
The risk of developing an electrophysiologic event also increased as a function of length of stay in the ICU and baseline QTc. Baseline QTc duration has previously been shown to be a predictor of subsequent QTc prolongation. 3-5,17 Interpreting the associations with length of ICU stay is less clear. Our study is unable to determine whether the presence of QTc prolongation resulted in longer lengths of stay in the ICU or if the duration of ICU stay predisposed the patients to electrophysiologic abnormalities.
There is a paucity of literature related to proarrhythmic risk in critically ill medical–surgical patient populations. There are no published studies on the incidence of QTc prolongation in critical care patients, or on whether these patients are at an increased risk compared to the general population. Evidence of drug-induced TdP in medical ICU patients receiving drugs included in our study are limited to case reports. 18-22 The incidence of all types of arrhythmias in medical ICU patients has only been reported by 2 groups in the last two decades. 23,24 In both studies, the incidence of QTc prolongation was not assessed.
The results suggest the need for expanded surveillance when selecting and monitoring these drugs in critically ill patients. Although our study was unable to evaluate whether the observed incidence of significant QTc prolongation resulted in detrimental patient outcomes, it may provide the impetus for routine QTc interval surveillance in other units of hospitals, evaluation of the incidence of QTc prolongation in other medical institutions, and the establishment of formal QTc monitoring programs. A prospective study is needed to evaluate the clinical implications of QTc prolongation and the effect of heightened surveillance.
Limitations
Our study has several limitations. First, the results reflect the practice and prescribing patterns at a single academic medical institution and thus may have limited generalizability to other medical ICUs. The actual incidence of electrophysiologic effects in different medical ICU patients may also vary based on the utilization patterns of known QTc-prolonging medications. However, the mean increase in QTc interval duration with moxifloxacin (20 ± 33 milliseconds) was longer in our study than reported in the general population (6 ± 26 milliseconds). 25 It may be hypothesized that this is a reflection of a predisposition of critically ill patients to electrophysiologic effects of drugs, an effect likely to occur at other medical institutions. A preliminary study comparing moxifloxacin to ciprofloxacin in ICU patients demonstrated mean QTc increases of 87 and 47 milliseconds, respectively. 26
Our statistical analysis identified 3 variables associated with either increased or decreased risk of developing an electrophysiologic event; however, predictive value does not equate to cause and effect. As discussed, the covariates identified as significantly associated with an increased or decreased risk of QTc prolongation inherently can be explained by previous literature or logic. However, their relative clinical importance requires confirmation. A prospective randomized study to confirm the protective electrophysiologic effects of beta-blockers when used concomitantly with QTc-prolonging medications is warranted.
We recognize that there is no consensus as to the optimal method for evaluation of QT intervals and proarrhythmic potential. It remains unclear as to whether absolute QT or QTc should be monitored to assess proarrhythmic risk. There are also limitations to methods used for heart rate correction, including over and under correction with Bazett’s formula at fast and slow heart rates, respectively. We also recognize that the exact importance or clinical relevance of QTc prolongation to the development of TdP is debatable as QTc prolongation alone does not predict proarrhythmic potential. 27 Other assessments such as alterations in QT dispersion may carry more predictive power. 28 However, these methods require specialized training or computer programs, and their reliability has also been questioned. 29 Our study utilized the QTc interval (correcting for heart rate with Bazett’s formula) to assess proarrhythmic potential, a readily available parameter that can be evaluated on a routine basis without special equipment or skills. Considering that the QTc interval can be easily calculated using this methodology by physicians, nurses, and pharmacists, and significant QTc prolongation is a recognized risk for drug-induced proarrhythmia, 1 we believe the results of our study remain thought provoking.
Finally, the aim of the study was to perform exploratory and hypothesis-generating analyses for a concept that has not been reported previously. As such, there was no control group to compare whether the incidence of electrophysiologic adverse events was higher in this medical–surgical ICU population than patients treated on other wards within the same hospital. Thus, the study demonstrates a high incidence of QTc prolongation but is unable to determine if the incidence is higher than in other patient populations. We also did not evaluate clinical end points such as incidence of TdP or mortality but instead focused on surrogate end points that have been identified for increased risk of poor outcome. The absolute incidence of TdP remains extremely low, and thus it would not have been reasonable to expect its occurrence. A prospective, multicenter study would be required to ensure adequate power to evaluate morbidity and mortality and confirm the findings on length of stay.
Footnotes
Acknowledgments
The authors would like to thank Shaina Pearson (Walker) for her help with data entry and Linda Schirmbeck for her editorial assistance.
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article. Dr. Olsen has received funding for research from Takeda, Carmel Pharma, AstraZeneca, and Astellas.
The authors received no financial support for the research and/or authorship of this article.