
Abstract
Purpose: This article will summarize the current evidence on the effects of omega-3 fatty acids on prevention and treatment of mental illness. Background: Omega-3 fatty acids are involved in many physiologic processes. Since they cannot be made de novo in the body, they are considered essential nutrients. As the Western diet evolved, dietary intake of fatty acids has shifted to increased omega-6 fatty acids and decreased omega-3 fatty acids intake. These changes have been correlated with numerous differences in prevalence and course of mental illnesses. Methods: A MEDLINE search from 1966 to December 2010 was completed to identify studies comparing changes in symptoms, functioning, other outcomes, and/or side effects in patients treated with omega-3 fatty acids for mental illness. The studies were reviewed and reported by specific psychiatric disorder studied. Conclusions: Omega-3 fatty acids play a role in many biologic functions. Epidemiologic data implicate omega-3 fatty acid deficiencies in many mental illnesses. Data are most robust for omega-3 fatty acids' role in affective disorders. However, data are conflicting, negative, or absent for most mental illnesses.
Introduction
Fatty acids can be divided into 2 categories, based on chemical properties (1) saturated fatty acids, which are usually solid at room temperature and (2) unsaturated fatty acids, which are liquid at room temperature. Carbon atoms in saturated fats are bound to 4 other atoms and cannot bind with other atoms. Unsaturated fatty acids can bind with other atoms due to double bonds linking at least 1 pair of carbon.
Based on the number of double bonds present, unsaturated fatty acids are either monounsaturated (contains 1 double bond) or polyunsaturated (containing >1 double bond). Plant oils such as olive and canola oils are made up of monounsaturated fatty acids. Vegetable-, nut-, and seed-based oils such as corn, sunflower, walnut, and flax seed oils consist of polyunsaturated fatty acids (PUFAs). Polyunsaturated fats are further defined by the location of the first double bond. Omega-6 fatty acids' double bonds begin at the sixth carbon atom, while omega-3 fatty acids' double bonds begin with the third carbon atom. Examples of omega-6 fatty acids are the short chain linoleic acid (LA) and the longer chain gamma linoleic (GLA) and arachidonic (AA) acids. Omega-3 fatty acids include alpha-linolenic acid (ALA), a short chain omega-3 fatty acid, and long chain omega-3 fatty acids eicosapentaenoic (EPA), docosapentaenoic acid (DPA), and docosahexaenoic (DHA).
The human body cannot make the short chain ALA and LA fatty acids, and so they are considered essential nutrients. The long chain omega-6 (GLA and AA) and omega-3 fatty acids (EPA, DPA, and DHA) can be formed in the body from LA and ALA. However, only 10% to 15% of ALA can be converted into EPA, DPA, or DHA in vivo. 1 Therefore, the majority of long-chain fatty acids are derived from dietary sources. 1–4,7–9 When a person is deficient in omega-3 fatty acids, there is increased incorporation of omega-6 fatty acids in cell membranes leading to stiffer, less flexible cell membranes. 1–3,7–10 Thus, the ratio of omega-6 fatty acids to omega-3 fatty acids is essential for normal neuronal functioning.
PUFAs are precursors of eicosanoids, a group of bioactive mediators involved in inflammation, immunity, and coagulation (Figure 1 ). 2 Series 1 prostaglandins and thromboxanes and series 4 leukotrienes are derived from AA. AA-derived eicosanoids respond to stress or injury producing an array of effects on clotting, muscle contractility, and cellular influx/efflux of substances such as calcium. These effects are modulated by the EPA-derived series 3 prostaglandins and thromboxanes and series 5 leukotrienes. EPA-derived eicosanoids have less potent effects or prevent the effects of AA-derived eicosanoids. Thus, adequate production of EPA-derived eicosanoids is necessary for proper functioning of AA-derived eicosanoids. 1–7
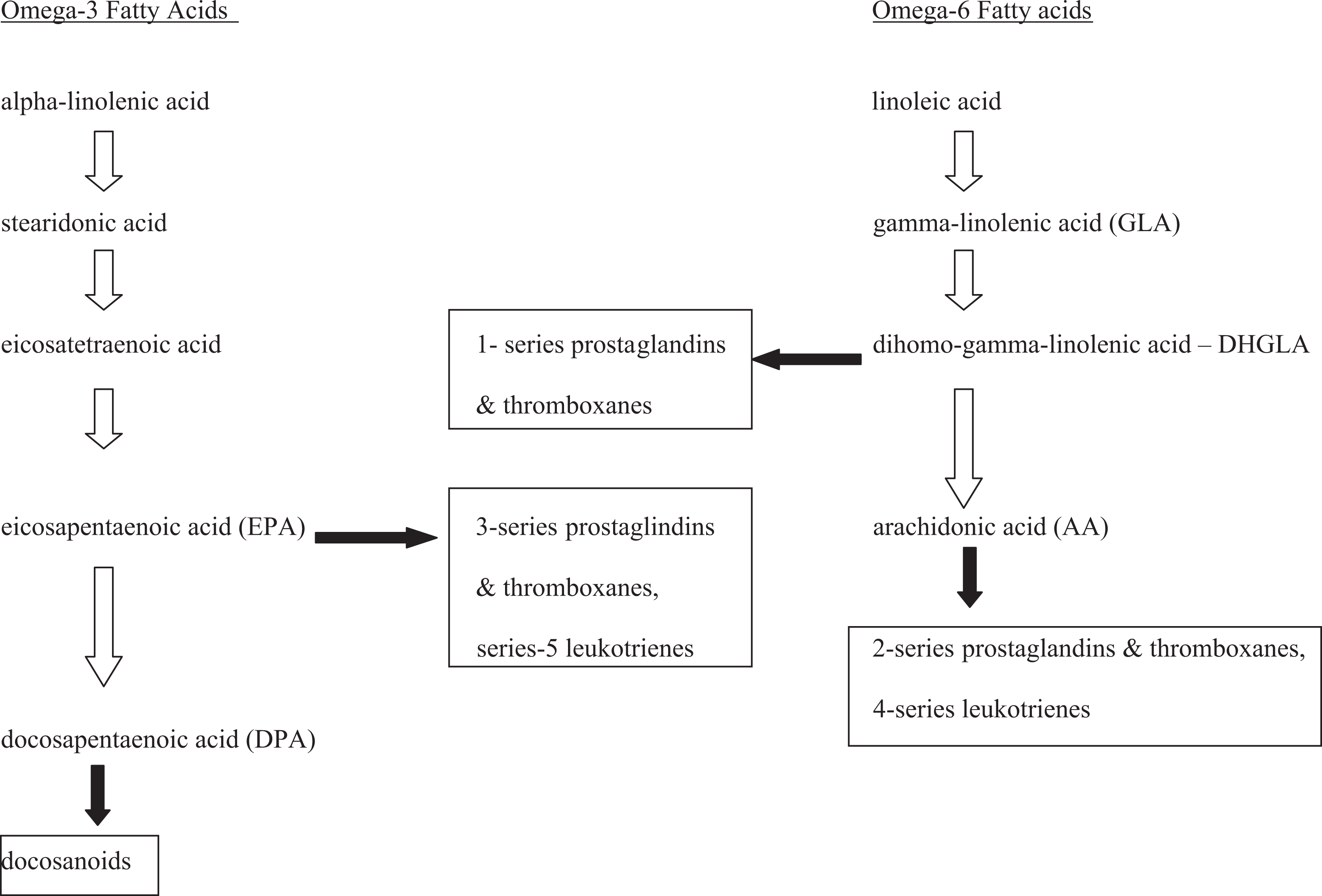
Polyunsaturated fatty acids.
DHA is converted into the docosanoids, a group of bioactive molecules possessing anti-inflammatory and neuroprotective properties. Resolvins, one type of docosanoids, are important in counteracting proinflammatory responses to omega-6 fatty acids. 4–7 Consequently this cytoprotective function is also heavily dependent on the omega-6 to omega-3 ratio. 1,3
DHA is an integral component of neuronal development and maturation. 1,2,8 Consequently, DHA is an important fatty acid for learning and neuronal growth and development during the fetal and infant stages. 3 Maternal DHA deficiency during pregnancy and lactation may lead to lower cognitive performance later in childhood.
Neuronal membrane fluidity is dependent on the type of fatty acid incorporated into the cell membrane. DHA and EPA are incorporated into neuronal cell membranes and allow the membrane to be fluid or “flexible.” Such membrane fluidity is necessary for proper functioning of lipid messengers which signal cascades leading to changes in neuronal flexibility and function. This is important in psychiatric illnesses because serotonin and catecholamine receptors, ion channels, transporters, and G-coupled proteins are dependent on fluid or flexible cell membranes.
Omega-3 fatty acids are also involved in many physiologic processes outside the central nervous system. EPA and DHA enhance nitric oxide production, which may be responsible for improved endothelial function and arterial compliance. 11,12 Alterations in the metabolism of adhesion molecules by DHA and EPA may inhibit new arterial plaque development. 13,14 Inhibition of voltage-gated sodium channels may account for reductions in arrhythmias with omega-3 fatty acid supplementation. 15 While omega-3 fatty acids influence platelet aggregation, recent studies have failed to find a correlation between omega-3 fatty acids and coagulation factors. 16 Although earlier studies have reported omega-3 fatty acids affect platelet aggregation through reductions in thromboxane, a proaggregatory eicosanoid and inhibition of cyclooxygenase enzymes associated with thrombosis. 17 However, the US Food and Drug Administration (FDA) has designated omega-3 fatty acids as “generally recognized as safe” when taken at normal doses. 18 Taken together, omega-3 fatty acid appears to be safe and beneficial in cardiac disease. 18
The source of omega-3 fatty acids is important. Epidemiologic data indicate both plant- (ALA) and marine (DHA and EPA)-derived omega-3 fatty acids are important for physiologic processes. 19 However, the preponderance of data indicate fish-derived omega-3 fatty acids are preferable to plant-derived omega-3 fatty acids. This is reflected in the American Psychiatric Association’s recommendations that (1) all adults eat a variety of fish (preferably oily fish) 2 or more times weekly; (2) patients with mood, impulse-control, and psychotic disorders consume 1 g of EPA + DHA daily; and (3) a supplement may be useful in patients with mood disorders. 19
Since omega-3 fatty acids are essential nutrients, changes in diet can have profound effects on omega-3 fatty acid concentrations. The ratio of omega-6 to omega-3 fatty acid intake has shifted dramatically in the Western diet over several decades. Currently in many Western countries the omega-6 to omega-3 intake ratio is 10:1, while a ratio of 1:1 may be more appropriate. 16 Given omega-3 fatty acids' beneficial effects on multiple neuronal and cardiovascular targets, it is not surprising that dietary changes are implicated in both psychiatric and cardiovascular disorders.
Methods
In order to determine whether omega fatty acids are a reasonable treatment option for psychiatric disorder, we conducted a systematic review of the medical literature. In January 2011, we conducted a MEDLINE search from 1966 to December 2010 to identify studies of omega-3 fatty acids as treatment or prevention of psychiatric illnesses. The following search terms were used: omega-3 fatty acid, eicosapentaenoic (EPA), docosahexaenoic (DHA), mental illness, psychiatry, affective and mood disorders, psychosis, schizophrenia, anxiety, substance abuse, attention-deficit hyperactivity disorder (ADHD), autism, Asperger’s, bipolar disorder, depression, perinatal and postpartum depression, and personality disorder. The reference section of these articles and previous reviews were searched for articles not identified in the original search. Articles were restricted to the English language. Data on study design, PUFA treatment, and side effects were abstracted and reported.
We examined studies within strata reflecting the rigor of their study design: randomized controlled trials (RCTs), nonrandomized controlled studies, and noncontrolled observational studies. Because of the robust number of studies with one of these designs, we excluded case reports and series without statistical analyses. Major limitations of each study are noted in the evidence tables; these include small sample sizes in some studies, limited matching characteristics, and short periods before follow-up assessment. Unless otherwise noted, all comparisons reported were statistically significant.
Unipolar Depression
Most epidemiologic data support the link between fish consumption and a lowered risk of depression. 20–28 Consumption of seafood at least twice a week may be associated with a lower risk of depression and suicidal ideation. 23,24 Severity of depressive symptoms has been linked to the omega-6 to omega-3 ratio. 25,26 Many studies suggest a link between depression and reduced omega-3 fatty acid concentrations in plasma, serum phospholipids, and red blood cells. 21–28 The one large trial that failed to replicate these findings may have been confounded by the high average daily intake of omega-3 fatty acids across the population. 29 Studies report mixed outcomes for the interaction of gender and omega-3 fatty acid concentrations on depression. One study reported increased fish intake was associated with less depression in women but not men, 20 while another study found depression was inversely related to omega-3 intake in boys aged 12 to 15 years. 28
Antidepressant response has been postulated to be associated with omega-3 fatty acid concentrations, although results from clinical trials have been mixed (Table 1 ). 30 –45 Of the 7 augmentation studies in adults, 4 found no benefit with the addition of omega-3 fatty acids. 30,31,32,35 However, 2 of these studies were in patients with comorbid diabetes or coronary heart disease and may not be applicable for depressed patients without these comorbidities. 30,31 The 2 positive placebo-controlled studies reported a 7.2- to 10.8-point improvement on the Hamilton Depression Rating scale (HAMD) compared with placebo. 33,36 The 1-dose finding trial reported significant benefit only in the low-dose (1 g) group. 34
Randomized Omega-3 Fatty Acid Trials in Unipolar Depression
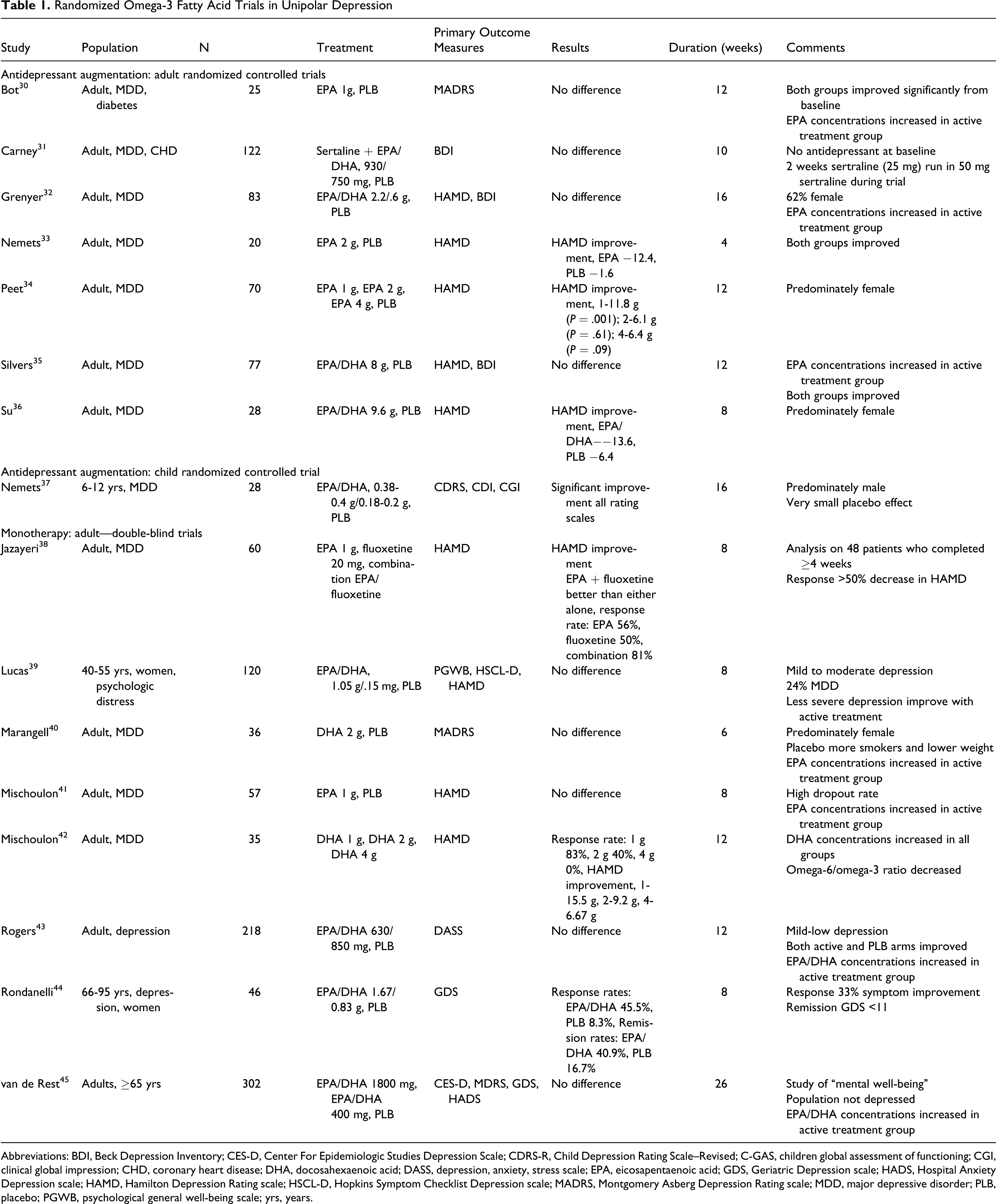
Abbreviations: BDI, Beck Depression Inventory; CES-D, Center For Epidemiologic Studies Depression Scale; CDRS-R, Child Depression Rating Scale–Revised; C-GAS, children global assessment of functioning; CGI, clinical global impression; CHD, coronary heart disease; DHA, docosahexaenoic acid; DASS, depression, anxiety, stress scale; EPA, eicosapentaenoic acid; GDS, Geriatric Depression scale; HADS, Hospital Anxiety Depression scale; HAMD, Hamilton Depression Rating scale; HSCL-D, Hopkins Symptom Checklist Depression scale; MADRS, Montgomery Asberg Depression Rating scale; MDD, major depressive disorder; PLB, placebo; PGWB, psychological general well-being scale; yrs, years.
Of the 8 double-blind trials of omega-3 fatty acids as monotherapy for depression, 6 were placebo controlled. 39–41,43–45 One randomized, double-blind trial compared omega-3 fatty acids, fluoxetine and the combination. 38 The remaining randomized trial was a dose finding trial and did not include a placebo group.
Five of the trials, including the largest study, reported no benefit of omega-3 fatty acids in depression. 39–41,43,45 However, one of the negative trials studied “mental well-being” in those ≥65 years and another studied psychological distress. 39,45 Both may not adequately address the use of omega-3 fatty acids in patients with major depression. The remaining trials differed significantly in terms of specific omega-3 fatty acids and dose studied, making generalization problematic. One trial included fluoxetine as an active comparator. 38 The authors reported 1 g of EPA and 20 mg fluoxetine had similar effects, while the combination was superior to either alone.
The final controlled study of omega-3 fatty acids was a dose finding study of DHA in adults with depression. 42 Doses included were 1, 2, and 4 g daily. All 3 doses were beneficial but the most improvement was seen on the 1-g dose, suggesting there may be a ceiling effect of DHA supplementation.
The only RCT in children was omega-3 fatty acid augmentation of ongoing antidepressant treatment. 37 The population was predominately male. The study found significant benefit on all outcome measures. The authors point out that the study had an unexpectedly low placebo response rate which may have affected the results.
The role of omega-3 fatty acids in unipolar depression is promising. Epidemiologic data support the theory that omega-3 fatty acid deficiency is associated with increased rates of depression. However, clinical trials report varied outcomes. This may be due to the heterogeneity of trials reported in the literature. Studies differed in which omega-3 fatty acid or combinations of fatty acids were used. Augmentation trials typically enrolled patients regardless of their baseline antidepressant. Doses studied varied widely, with total daily doses up to 9.6 g. A wide variety of depressive disorders were studied including major depressive disorder, less severe forms of depression, and depression with comorbid medical illnesses. Although most studies were in adult patients, age groups studied ranged from pediatric to geriatric populations. In addition, trials reported on outcomes of omega-3 fatty acid monotherapy, omega-3 fatty acid augmentation of specific antidepressant, and combinations of any pre-study antidepressant and omega-3 fatty acids. While doses ranged widely, all studies reported the use of EPA, DHA, or their combination, so fish-derived omega-3 fatty acids would seem to be preferable to plant-derived ALA.
While it is difficult to draw any firm conclusions about omega-3 fatty acids in unipolar depression, given the safety, cardioprotective effects, and suggestion that there may be some benefits with omega-3 fatty acid augmentation or monotherapy in depression, it seems reasonable to consider omega-3 fatty acids as a treatment option for patients with depression. They have a potential role as antidepressant augmentation or monotherapy for adults in whom antidepressants are not acceptable. Given the disparity of data, it is difficult to recommend specific doses or combinations of fatty acids. It has been suggested that EPA may be the effective component in depression treatment. 46 But, animal models suggest that DHA-deficient diets are associated with abnormal dopaminergic and serotonergic function. 47 Clinical trial data suggest that higher doses may not confer additional benefits and a daily total of omega-3 fatty acids (EPA/DHA) of 1 to 2 g is reasonable in unipolar depressive illnesses. While the one trial of omega-3 fatty acids in children was positive, it is premature to recommend its use as a therapeutic option in pediatric depression. However, since omega-3 fatty acids have been proven safe in many other pediatric conditions, it is unlikely their use in pediatric populations would be harmful.
Perinatal Depression
Normal neurodevelopment in utero is dependent on adequate supply of DHA. 1,2,8 Hibbeln and Davis suggest that during pregnancy, as DHA is transferred to the fetus, women with low-DHA intake will become depleted and more vulnerable to depression. 48 This is supported by epidemiologic data indicating higher intake of fish during pregnancy is associated with decreased risk of postpartum depression. 49,50 Countries with low fish intake have a 50-fold increased risk of postpartum depression compared with countries with high seafood intake. 49 Single women with low seafood intake who smoke may be more likely to have depressive symptoms during pregnancy. 51 Still other studies report lower concentrations of DHA in women who develop postpartum depression than those who do not. 50 Some studies have failed to find an association of omega-3 fatty acid intake and perinatal depression. One study of 80 women was probably underpowered to find a relationship, while another study had relatively high-baseline rates of seafood consumption. 51,52 The largest study, a prospective cohort study of 54 202 Danish women, did not support the inverse relationship of fish or omega-3 fatty acid intake and postpartum depression. 53
Potential risk of low DHA intake extends beyond mothers to their offspring. Lower verbal intelligence quotient (IQ), increased risk of fine motor deficits, and behavioral problems have been reported in children born to women with low seafood intake during pregnancy. 54,55 Hibbeln and Davis calculated 900 mg/d per 2000 calories from seafood is likely sufficient to provide optimal neurodevelopment in the offspring and decrease the risk of postpartum depression. 48 They also report that there is no evidence indicating an upper limit of intake for omega-3 fatty acids as there are no data indicating an excess of omega-3 fatty acids contribute to neurodevelopment or psychiatric risks.
Interventional trials of omega-3 fatty acid supplementation during pregnancy have reported mixed outcomes (Table 2 ). 56–62 Six randomized studies were placebo controlled and 1 was a randomized dose ranging study.
Randomized, Double-Blind Studies of Omega-3 Fatty Acid Trials in Perinatal Depression
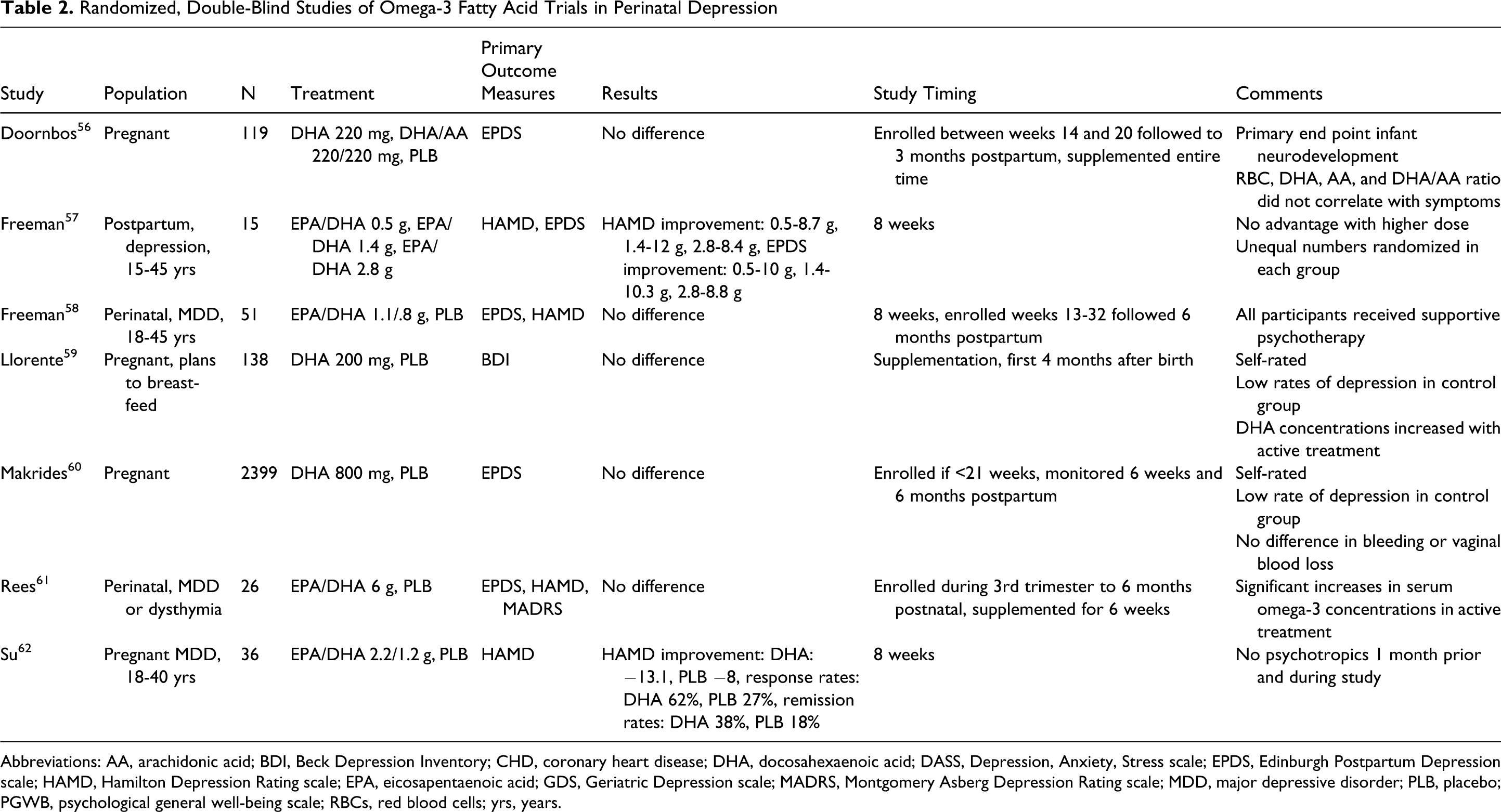
Abbreviations: AA, arachidonic acid; BDI, Beck Depression Inventory; CHD, coronary heart disease; DHA, docosahexaenoic acid; DASS, Depression, Anxiety, Stress scale; EPDS, Edinburgh Postpartum Depression scale; HAMD, Hamilton Depression Rating scale; EPA, eicosapentaenoic acid; GDS, Geriatric Depression scale; MADRS, Montgomery Asberg Depression Rating scale; MDD, major depressive disorder; PLB, placebo; PGWB, psychological general well-being scale; RBCs, red blood cells; yrs, years.
Freeman et al reported significant benefit of omega-3 fatty acid supplementation in women randomized to 1 of 3 doses of EPA and DHA. 57 However, the study lacked a placebo group and was not confirmed in more rigorous trials. Llorente and colleagues found 16 weeks of 200 mg was not associated with changes in rates of postpartum depression. 59 However, the study had a low baseline level of depression in both groups and of those with depressive symptoms at baseline, the majority reported only mild symptoms. Four other RCTs also failed to find the benefits of omega-3 fatty acid supplementation on depressive symptoms, 56,58,60,61 while 1 small trial reported benefit with DHA supplementation. 62
The largest randomized, double-blind, placebo-controlled trial found supplementation with 900 mg/d of omega-3 fatty acids did not prevent postpartum depression in 2399 women. 60 During the trial, women were supplemented with omega-3 fatty acids during the second half of pregnancy. Adherence was confirmed by increased concentrations of DHA in the cord blood of women in the active treatment arm compared with controls (7.2% vs 6.09%; P < .001). The results may have been confounded by an unusually low rate of maternal depression in the control group. The authors did report a nonsignificant trend toward decreased depression in women who had been previous medically diagnosed with depression.
While the role of omega-3 fatty acids in perinatal depression is supported by epidemiologic data, this has not been born out in interventional trials. The largest study of omega-3 fatty acid supplementation in pregnancy failed to find an effect of omega-3 fatty acids in perinatal depression. This study utilized a dose consistent with the 900 mg/d per 2000 calories suggested by researchers as likely to meet the nutritional requirements for 97.5% of pregnant women. 48 These findings are in direct contrast to some groups recommending routine omega-3 fatty acid supplementation for pregnant women. However, it is important to remember the risk to the fetus and some data indicate poor cognitive outcomes in children born to women with low omega-3 fatty acid intake. Overall, while the benefit of omega-3 fatty acids in perinatal depression, primarily DHA, is not supported by controlled trials, it is likely that normal neurocognitive development is dependent upon adequate maternal DHA concentrations. Given the safety of omega-3 fatty acids, effects in fetal development and general medical benefits such as improved cardiovascular health, DHA supplementation during pregnancy is reasonable. While there are no clear guidelines as to dose, Hibbeln and Davis' work support the use of 900 mg/d per 2000 calories of DHA during pregnancy. 48
Bipolar Disorder
Abnormalities in the omega-6 fatty acid, AA, are thought to play a role in the pathogenesis of bipolar disorder. 63,64 This has been demonstrated in several studies finding products of AA are increased in the blood, saliva, and cerebrospinal fluid of patients with bipolar disorder. 63 While omega-3 and omega-6 fatty acids both increase the proinflammatory eicosanoids, those derived from omega-6 fatty acids result in more inflammation than those derived from omega-3 fatty acids. So, in people with high omega-6:omega-3 fatty acid ratios, one would expect increased inflammation and possibly increased neuronal cell death. 63,64 Ideally, a shift in dietary intake to increased omega-3 fatty acids would decrease inflammation associated with omega-6 fatty acids.
This is supported by commonly used treatments for bipolar disorder which have a similar effect as omega-6 and omega-3 fatty acids (eg, lithium, carbamazepine, and valproate). In animal models it has been found that these medications decrease the turnover of the omega-6 fatty acid, AA, and may improve symptoms of bipolar disorder through secondary decreases in proinflammatory by-products of AA. 63,64
Epidemiologic studies also support the link of omega-6:omega-3 fatty acid ratios in bipolar disorder. In one cross-national study, seafood consumption was inversely related to rates of bipolar I, bipolar II, and bipolar spectrum disorders. 65 The relationship seemed strongest with bipolar II disorder. The authors reported a minimum consumption of 50 pounds of fish per year, which they estimate is equal to 3 g of EPA/DHA daily, was associated with decreased rates of bipolar disorders. Some studies have reported lower concentrations of omega-3 fatty acids in patients being treated for bipolar disorder, although other studies have not replicated these findings. 66–68 Clayton et al found no differences in omega-3 fatty acid concentrations in pediatric bipolar disorder when controlling for the intake of omega-3 fatty acids. 69 Rather, the authors suggest that the high cost of fresh fish and low socioeconomic status often associated with bipolar disorder may account for the lower concentrations of omega-3 fatty.
Omega-3 fatty acid concentrations have been correlated with symptom severity in bipolar disorder. Clayton reported that in pediatric bipolar disorder, DHA concentrations were associated with depression severity; while EPA concentrations were more closely associated with manic symptoms. 70 These results were replicated in a study of adults with bipolar disorder that reported omega-3 fatty acid concentrations and omega-6:omega-3 ratio were associated with severity of manic symptoms. 71
Three open-label trials have found adjunctive omega-3 fatty acid supplementation to be effective in bipolar disorder (Table 3 ). 72–80 The two studies in pediatric patients with bipolar disorder both reported improvement in manic symptoms, one of which reported improvements in depression when omega-3 fatty acids were added to ongoing treatment. 70,79 The one open-label adult trial reported significant improvement in depressive symptoms when omega-3 fatty acids were added to ongoing treatment. 75
Clinical Trials of Omega-3 Fatty Acids in Bipolar Disorder
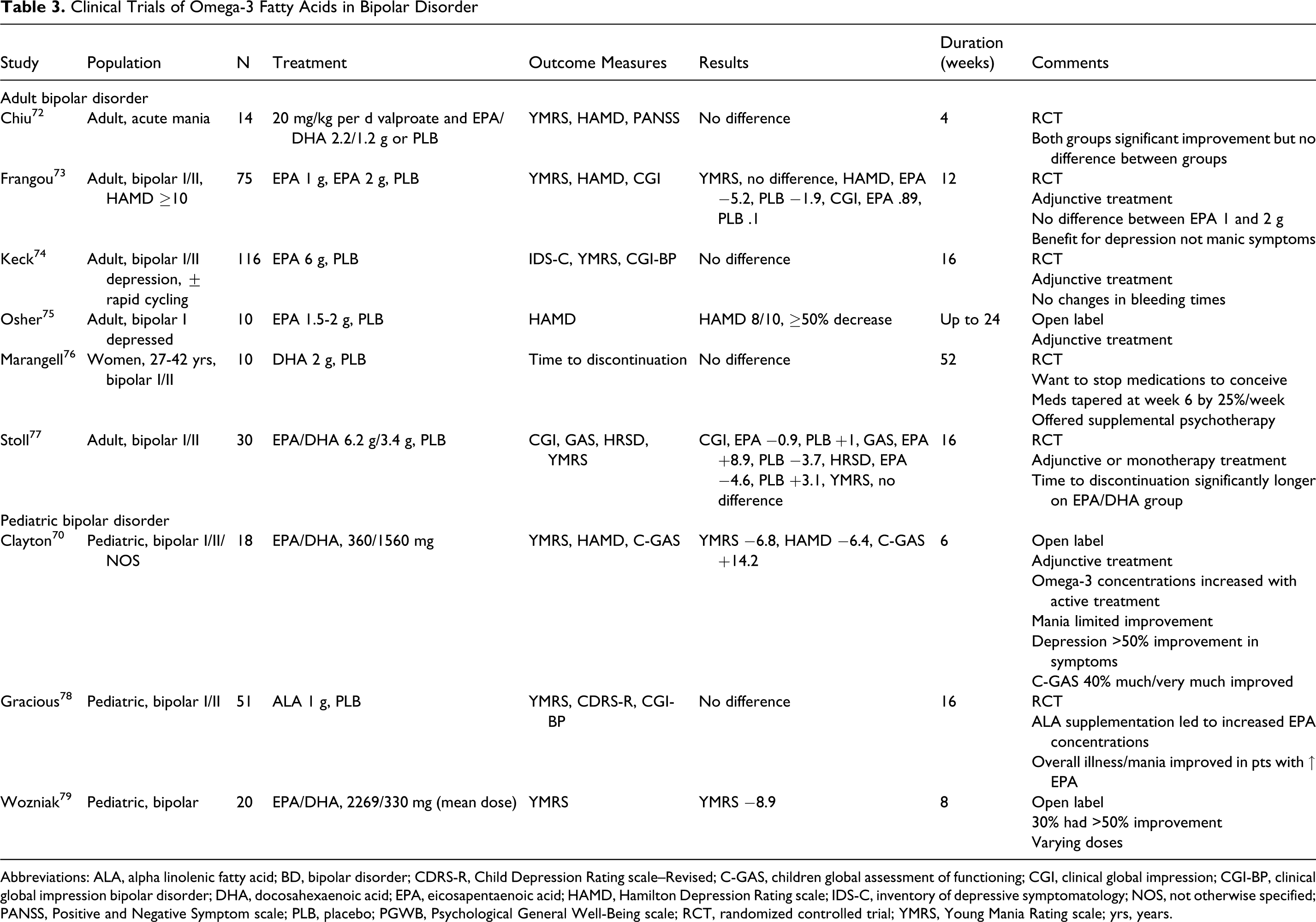
Abbreviations: ALA, alpha linolenic fatty acid; BD, bipolar disorder; CDRS-R, Child Depression Rating scale–Revised; C-GAS, children global assessment of functioning; CGI, clinical global impression; CGI-BP, clinical global impression bipolar disorder; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; HAMD, Hamilton Depression Rating scale; IDS-C, inventory of depressive symptomatology; NOS, not otherwise specified; PANSS, Positive and Negative Symptom scale; PLB, placebo; PGWB, Psychological General Well-Being scale; RCT, randomized controlled trial; YMRS, Young Mania Rating scale; yrs, years.
Results from more rigorous studies have been mixed (Table 3). Three RCTs reported no benefit, while 2 reported improvements with omega-3 fatty acid augmentation in adults with bipolar disorder. 72–74,76,77 Two negative trials studied omega-3 fatty acid supplementation in subpopulations (acute mania, women discontinuing mood stabilizers prior to becoming pregnant), making it difficult to generalize the findings. 72,76 Both positive trials reported significant improvement in depressive symptoms but no benefit for mania, suggesting omega-3 fatty acids may play a limited role in adult bipolar disorder. 73,77
The one randomized controlled trial on pediatric bipolar disorder reported no benefit with ALA supplementation. However, overall illness and manic symptoms improved in patients with significant increases in EPA concentrations. 78
Given the disparity in methods, populations studied, and outcomes, it is difficult to draw any firm conclusions about the relationship of omega-6:omega-3 fatty acids and bipolar disorder. While epidemiologic data indicate that there is a relationship, other studies controlling for omega-3 fatty acid intake do not find a similar association. In positive studies, data indicate either 2 to 4 g daily intake of EPA alone or in combination with DHA are beneficial in adults in the depressive phase of the illness.
Schizophrenia
Alterations in neuronal membranes and fatty acid metabolism have been implicated in the pathogenesis of schizophrenia. 80,81 Omega-3 fatty acids are known to effect membrane fluidity, dopaminergic and serotonergic systems, and modulate AA release, all of which are proposed to be altered in patients with schizophrenia. In addition, through modulation of glutathione, omega-3 fatty acids are also thought to be involved in neuronal protection from excitotoxic and oxidative stress. 82–85
Such theorized deficiencies have been supported by clinical data. Deficiencies in AA, an omega-6 fatty acid, and the omega-3 fatty acids such as EPA and DHA have been reported in drug-naive and medicated patients with schizophrenia when compared with matched controls and patients with bipolar disorder. 86–88 Patients with schizophrenia and tardive dyskinesia have also been shown to have decreased concentrations of erythrocyte omega-6 fatty acids. 89
These findings are supported by studies which report that lowered dietary intake of fatty acids is associated with psychotic symptoms and the course of schizophrenia. 90,91 One study of 33 000 women with a low intake of omega-3 fatty acids were found to have an increased risk of psychotic symptoms. 92 Another study reported significant deficiencies in a woman’s diet during pregnancy may increase the risk of schizophrenia in her children. 93 Omega-3 fatty acid supplementation may prevent or delay the onset of schizophrenia (Table 4 ). 94,95 In patients at high risk of psychosis, Amminger and colleagues reported 4.9% of EPA/DHA-treated patients and 27.5% of placebo-treated patients developed psychotic symptoms during 40 weeks. 94 Peet reported 57% and 100% of EPA- and placebo-treated patients required an antipsychotic at the end of 12 weeks. 95
Clinical Trials of Omega-3 Fatty Acids in Schizophrenia
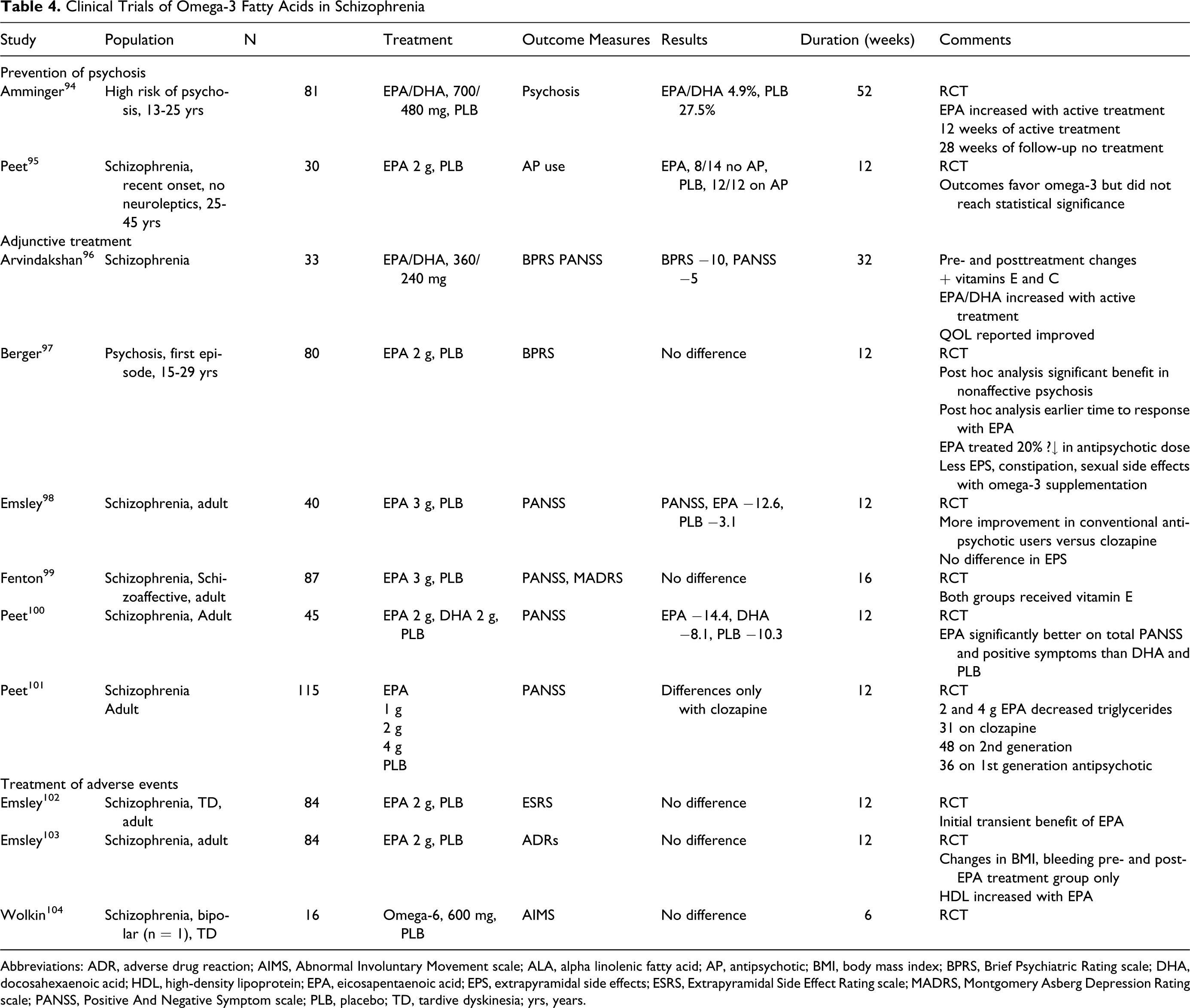
Abbreviations: ADR, adverse drug reaction; AIMS, Abnormal Involuntary Movement scale; ALA, alpha linolenic fatty acid; AP, antipsychotic; BMI, body mass index; BPRS, Brief Psychiatric Rating scale; DHA, docosahexaenoic acid; HDL, high-density lipoprotein; EPA, eicosapentaenoic acid; EPS, extrapyramidal side effects; ESRS, Extrapyramidal Side Effect Rating scale; MADRS, Montgomery Asberg Depression Rating scale; PANSS, Positive And Negative Symptom scale; PLB, placebo; TD, tardive dyskinesia; yrs, years.
Six studies have been reported assessing the role of adjunctive omega-3 fatty acids for the treatment of psychosis (Table 4). 96–101 One open-label study reported significant improvements in general psychopathology with omega-3 fatty acid supplementation. 96 Of the 5 RCTs, 2 were negative, 97,99 2 were positive, 98,100 and 1 found benefits only when omega-3 fatty acids were added to clozapine. 101 Post hoc analyses of one of the negative studies did report omega-3 supplementation was beneficial in nonaffective psychosis and associated with a 20% decrease in total antipsychotic dose. 97 Other studies report differential effects by concomitant antipsychotics with one reporting benefit only in patients treated with clozapine and another reporting increased benefits in augmentation of conventional antipsychotics. 98,101 The one study of both EPA and DHA found EPA significantly better than DHA. 100
The role of omega-3 and omega-6 fatty acid supplementation on side effects in patients with schizophrenia has been assessed in 3 RCTs. 102–104 These trials found no difference in side effects, extrapyramidal side effects, and tardive dyskinesia with active treatment and placebo. However, all of these trials were small and of short duration. Emsley et al did find increased bleeding time, body mass index, and decreased high-density lipoprotein (HDL) concentrations in patients pre- and post-EPA supplementation. 103
Studies assessing prevention of psychosis with omega-3 fatty acid supplementation are promising. Although far from conclusive, data suggest omega-3 fatty acids are more beneficial for nonaffective psychoses. Studies of omega-3 fatty acid treatment of schizophrenia are mixed. Data suggest EPA is more effective than DHA monotherapy. Given the cardiovascular benefits and limited side effects of omega-3 fatty acids when compared to antipsychotics, supplementation with EPA or EPA/DHA combination in 1 to 2 g daily is reasonable for the prevention and adjunctive treatment of psychosis. However, caution should be used in patients at risk of bleeding.
Attention-Deficit Hyperactivity Disorder
In the brain, the principle fatty acid is DHA which increases in the frontal cortex during childhood and adolescence. 105 This deposition of DHA is associated with neurocognitive maturation. 105,106 Disruption in the DHA accumulation in the maturing brain can lead to cognitive and physical problems. 105,106 It has been postulated that altered fatty acid concentrations are associated with symptoms of attention-deficit hyperactivity disorder (ADHD). 107 Most, but not all studies, report lower concentrations of omega-6 fatty acids, DHA and EPA, and higher omega-6:omega-3 fatty acid ratio in children with ADHD. 107 In addition, low concentrations of omega-3 fatty acids have been observed in the plasma phospholipids and erythrocytes of subjects with ADHD. 108 In children, studies indicate alterations of omega-3 fatty acids are related to cognitive problems of ADHD, while changes in omega-6 fatty acids are associated with physical deficits. 109,110 This is supported by one functional magnetic resonance imaging study reporting DHA supplementation increased prefrontal cortex activation during sustained attention in healthy boys. 105 Symptom severity may be related to omega-3 plasma concentrations in children. 110 Although, one study in adults failed to find an association of omega-3 fatty acid concentrations in adults with ADHD. 111
All placebo-controlled studies are in pediatric ADHD (Table 5 ). 112 –125 Few report significant improvements in primary outcome measures with active treatment. Half of the trials failed to find a significant benefit with omega-3 supplementation, while others found benefits in subpopulations, mildly ill children, or for limited symptoms only. 112,116,117,120,121,123,125 There were no differences between groups in trials that distinguished between inattentive and hyperactive types. Several of the trials were for disorders related to ADHD. Many studies were limited by small sample size, making interpretation of negative findings difficult. Of the studies with positive findings, most reported benefit for inattention only. 114,121,122
Placebo-Controlled Clinical Trials of Omega-3 Fatty Acids for Attention-Deficit Hyperactivity Disorder (ADHD) and Related Diagnoses
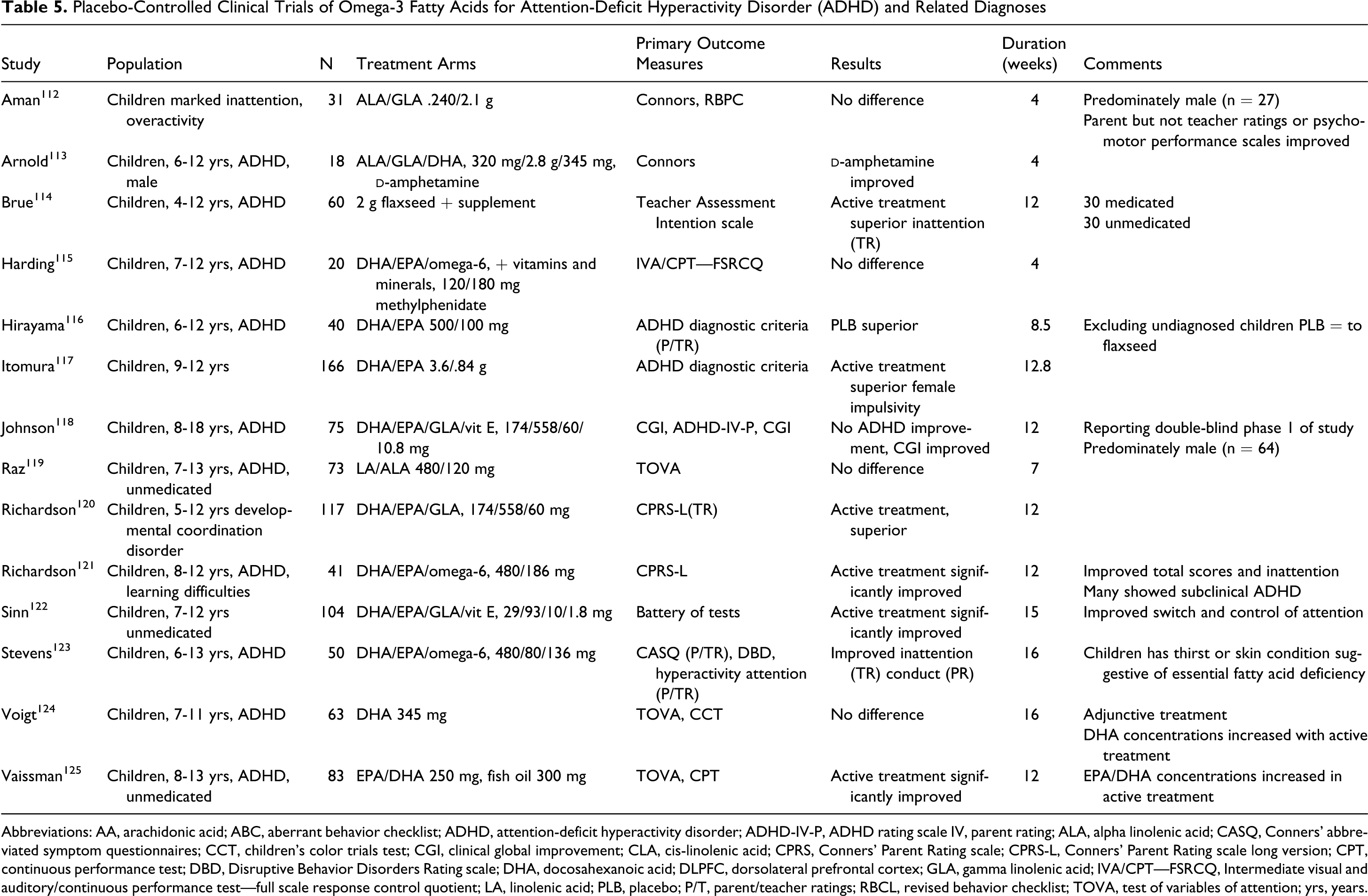
Abbreviations: AA, arachidonic acid; ABC, aberrant behavior checklist; ADHD, attention-deficit hyperactivity disorder; ADHD-IV-P, ADHD rating scale IV, parent rating; ALA, alpha linolenic acid; CASQ, Conners' abbreviated symptom questionnaires; CCT, children’s color trials test; CGI, clinical global improvement; CLA, cis-linolenic acid; CPRS, Conners' Parent Rating scale; CPRS-L, Conners' Parent Rating scale long version; CPT, continuous performance test; DBD, Disruptive Behavior Disorders Rating scale; DHA, docosahexanoic acid; DLPFC, dorsolateral prefrontal cortex; GLA, gamma linolenic acid; IVA/CPT—FSRCQ, Intermediate visual and auditory/continuous performance test—full scale response control quotient; LA, linolenic acid; PLB, placebo; P/T, parent/teacher ratings; RBCL, revised behavior checklist; TOVA, test of variables of attention; yrs, years.
Current evidence does not support a role of omega-3 fatty acids in the treatment of ADHD. However, many studies were limited by small sample size or populations without a clear diagnosis of ADHD. Though, generally well tolerated, routine recommendation of omega-3 fatty acids for the treatment of pediatric ADHD is premature. Given the lack of studies in adults, omega-3 fatty acids should not be recommended for the treatment of adult ADHD.
Autism Spectrum Disorders
The term autism spectrum disorder (ASD) encompasses a range of neurodevelopmental disorders, all of which involve impairment in social interaction, struggles with verbal and nonverbal communication, and stereotyped, repetitive behavioral patterns. 126 Classical ASD, or autistic disorder, is diagnosed when these symptoms manifest in their most severe form. Currently, Asperger’s disorder has distinct Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition [DSM-IV]) criteria, with the most notable difference being the absence of a delay in communicative abilities. 127 Individuals with ASD characteristics who do not identify with either of 2 subcategories are typically given a diagnosis of pervasive developmental disorder, not otherwise specified (PDD-NOS). 128 Although the average age of diagnosis is 3 years, marked behavioral disparities have been observed in children younger than 12 months. 129,130
The proposed etiologies of ASDs cover a broad range, including abnormalities in metabolism, inflammatory markers, genetics, neurotransmitter systems, and oxidative stress. 131–133 For instance, it has been suggested that inflammation and apoptosis play a significant role in autism, 133,134 while omega-3 fatty acids have been shown to prevent neuronal apoptosis 135,136 and influence neuroinflammation. 136 Functional polymorphisms in serotonin (5-HT) and dopamine (DA) transporters have been noted in autism, 137 while omega-3 fatty acids have been shown to affect 5-HT and DA neurotransmitter systems. 137,138 Fatty acids have wide implications in brain development and subsequent behavior, including the ability to respond to external stimuli, while abnormal responses to environmental stimulation are characteristic of autism. 139,140 In addition, low concentrations of omega-3 fatty acids have been observed in the plasma phospholipids and erythrocytes of subjects with ADHD, 108 a neurodevelopmental disorder with clinical presentation and genetic biomarkers comparable to that of autism. 141–143
Children with autism have been shown to have 20% lower omega-3 fatty acid plasma concentrations compared with mentally retarded controls. 144 The same trial reported no significant difference in the omega-6 fatty acid concentrations, which resulted in a significant increase in the omega-6:omega-3 ratio in the group with autism. Sliwinski et al analyzed plasma samples from high-functioning adolescent males and a healthy control group. 145 They discovered a statistically significant increase in plasma DHA, total omega-3 fatty acids, and the omega-6/omega-3 ratio in the autistic subjects. Wiest et al reported differences in omega-3 fatty acid concentrations were not significant when accounting for dietary intake. 144
Risperidone, a common drug therapy in ASD, may influence fatty acid profiles as well. Studies have demonstrated that chronic therapy with risperidone normalizes inflammatory biomarkers, significantly affects ALA-DHA biosynthesis, and increases omega-3 composition of peripheral and central membranes in rats with omega-3 fatty acid deficiency. 146,147 Risperidone also appears to have a wider range of symptom improvement, including aggressiveness, hyperactivity, irritability, stereotypy, social withdrawal, and lack of interests, as compared to omega-3 fatty acids which only specifically improve hyperactivity. 148
Two trials analyzed fatty acid compositions of red blood cells rather than plasma concentrations. Bell et al had positive findings, demonstrating that subjects with autism had significantly elevated concentrations of EPA and DHA and significantly reduced concentrations of AA. 149 They observed significantly higher percentages of omega-6 fatty acids and total saturates in the red blood cell membranes of subjects with regressive autism in particular, when compared to controls. Bu et al also encountered notable differences in omega-6 fatty acid profiles between children with clinical regression autism and those with early onset autism. 150 These findings indicate a potential differential etiology between classical, typical onset, autism and regressive autism, which develop after initial child development.
A collection of open-label pilot studies came to disparate conclusions. Johnson et al did not observe any clinical gains in autistic children given omega-3 supplements. 151 Politi et al did not observe any statistically significant improvements in autistic adults after omega-3 treatment, utilizing the Rossago Behavioral Checklist. 152 However, the problematic behaviors addressed by this instrument are only a portion of autism’s symptomatic picture. In contrast, Meiri et al observed a statistically significant improvement in subjects treated with omega-3 fatty acids. 153 Meguid et al also observed positive results in autistic children administered with a preparation of both omega-3 and omega-6 fatty acids. 154 Beneficial effects of omega-3 supplementation in children were also demonstrated in an open-label trial by Patrick and Salik, who specifically looked at language and learning skills. 155
RCTs investigating the effects of omega-3 fatty acid treatment in autism are limited (Table 6 ). 151–157 One RCT reported no significant difference between autistic subjects treated with omega-3 fatty acids as compared to placebo. 156 However, there were nonsignificant reductions in hyperactivity and stereotypy subscales. Another randomized control trial noted improvements, including nonsignificant decreases in hyperactivity, with omega-3 treatment. 158 This trial was unique in that it analyzed cytokines as a biomarker of anti-inflammation effects of omega-3 treatment. Surprisingly, there was a statistically significant increase in the tumor necrosis factor-α (TNF-α) plasma concentrations in the treatment group as compared to placebo. One cytokine, interleukin 2 (IL-2), demonstrated a negative correlation with hyperactivity.
Omega-3 Fatty Acids in Autism Spectrum Disorders
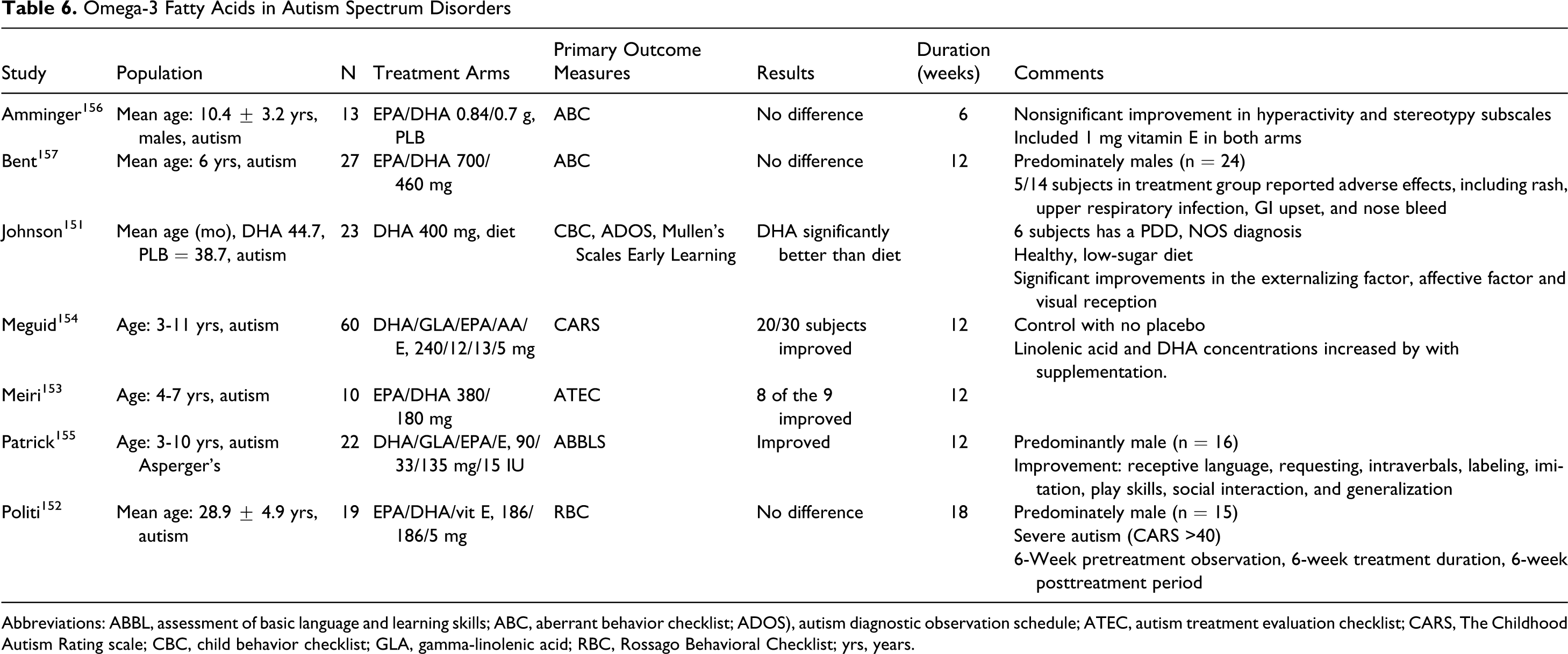
Abbreviations: ABBL, assessment of basic language and learning skills; ABC, aberrant behavior checklist; ADOS), autism diagnostic observation schedule; ATEC, autism treatment evaluation checklist; CARS, The Childhood Autism Rating scale; CBC, child behavior checklist; GLA, gamma-linolenic acid; RBC, Rossago Behavioral Checklist; yrs, years.
In summary, 4 of the 7 clinical trials demonstrated statistically significant changes. The lack of positive findings in the remaining trials is inadequate to fully discredit omega-3 fatty acids' potential benefit in improving symptoms of autism. Nonsignificant conclusions could be attributed to insufficient omega-3 dosing or improper EPA/DHA ratios. In addition, variability in results could be attributed to the presence or absence of vitamin E, which some trials included in their treatment arm to avoid lipid peroxidation. It is plausible that the treatment durations were too brief to allow substantial improvements to take place. However, Meiri et al declared that most of the improvements they observed occurred within the first 6 weeks, although raw data for this were not reported. 153
Several drug classes are typically used to manage some behavioral manifestations of autism, including antipsychotics, psychostimulants, antiepileptics, and antidepressants. Unfortunately, the side effects of these medications are often a limiting factor. 158 More trials are warranted, particularly in adult populations, before an unequivocal conclusion can be made regarding omega-3’s role in therapy. However, as omega-3 fatty acids are fairly innocuous, inexpensive, and readily available, a trial of omega-3 fatty acids in autistic children may be appropriate. Combinations of EPA and DHA showed the greatest benefit. Unfortunately, there is insufficient evidence to define a single most-effective dose or ratio. Children tolerated doses as high as 840 mg EPA and 700 mg DHA. However, trials administering doses as low as 52 mg EPA and 90 mg DHA yielded positive results. These particular trials also administered vitamin E (5 or 10 mg/d), which suggests a dose-sparing effect. 155,156 There is evidence for EPA/DHA ratios between 1.5:1 and 2:1, although this is from only 2 trials. 154,156 Those considering a trial treatment with omega-3 fatty acids should consult a health care practitioner prior to initiating therapy, as the FDA has not approved the use of fish oil supplements in children (<18 years). Omega-3 fatty acids' inhibition of platelet aggregation warrants precaution in those at an increased risk of bleeding or being treated with anticoagulants. 157
Anxiety Disorders
There are limited studies of omega-3 fatty acid supplementation in anxiety disorders. Many of the studies address only a select population. In terms of active treatment, a study of 126 university students with significant test anxiety reported 3 weeks of omega-3/omega-6 supplementation was associated with improved appetite, mood, organization, and concentration compared with placebo. 159 The authors also reported a significant decrease in salivary cortisol with active treatment. This finding should be interpreted with caution since the placebo-treated students had nonsignificant decreases in salivary cortisol as well.
Compared with placebo, anger and anxiety have also been reported to decrease with omega-3 fatty acid supplementation in men with substance abuse. 160 Researchers found 3 months of EPA/DHA supplementation decreased the anxiety scores in patients with substance abuse compared with placebo. The differences in anxiety symptoms remained significant for 3 months following the discontinuation of the supplements.
Studies of omega-3 fatty acids in obsessive compulsive disorder are limited. Fux and colleagues reported EPA supplementation was ineffective for the treatment of obsessive compulsive disorder. 161
Results regarding omega-3 fatty acid supplementation in posttraumatic stress disorder (PTSD) are conflicting. One study was terminated early when 2 g daily intake of EPA was found to worsen symptoms in 5 of 6 patients. 162 However, Matsuoka et al reported open-label treatment with omega-3 fatty acids could decrease the risk of subsequent PTSD in patients with accidental injuries. 163
Data are too limited to assess the efficacy of omega-3 fatty acids in the treatment of anxiety disorders. While they may be beneficial in those with comorbid mood and anxiety disorders, omega-3 fatty acids should not be routinely used for patients with PTSD.
Other Disorders
Omega-3 fatty acids have been explored in a limited fashion in many disorders including substance abuse and borderline personality disorder. However, there are insufficient data to draw any conclusions about the effectiveness of omega-3 fatty acids in these disorders. Omega-3 fatty acids have been studied extensively in cognition, cognitive decline, dementia, Alzheimer’s disease, and cognitive symptoms associated with other disorders. This is beyond the scope of this review.
Safety of Omega-3 Fatty Acids
Clinical trials demonstrate the risk of serious adverse events with omega-3 fatty acids are comparable with placebo. The most common side effects reported were gastrointestinal (diarrhea and belching). The FDA has recognized intakes up to 3 g/d of omega-3 fatty acids are safe. 19 The FDA has also recognized and approved qualified health claims for EPA and DHA. 19 One study did report an increase in bleeding time after EPA supplementation, but this increase did not result in clinical side effects. 90 However, other studies report no changes in bleeding time. 75 In one large study of pregnant women there was no increase in the rate of bleeding with omega-3 fatty acid supplementation. 60 In fact, the study found decreased rates of preterm labor with omega-3 fatty acid supplementation.
While fish may be contaminated with heavy metals, omega-3 fatty acid supplements usually contain very limited quantities of organochloride contaminants and no methylmercury. 168 However, significant levels of contaminants have been reported with some supplements. 163,164 While omega-3 fatty acid purification processes substantially decrease the risk of environmental contamination, krill oil can be used as an alternate source of marine-derived fish oils for those who remain concerned. 165 For those wishing to increase omega-3 fatty acid intake through fish consumption, the FDA recommends avoiding fish high in methylmercury such as shark, swordfish, king mackerel, or tilefish. 166 Instead consider recommending fish low in methylmercury content such as shrimp, canned light tuna, salmon, pollock, and catfish. 166
Conclusions
Omega-3 fatty acids have been studied in numerous disease states. They have cardioprotective effects and are relatively safe and inexpensive. In general, omega-3 fatty acids were well tolerated by many groups including pediatric and geriatric populations. While safe when taken in usual daily doses, caution should be used with large doses in patients at risk of bleeding abnormalities. Beyond that caution, side effects of fatty acids appear to be mild and primarily involve the gastrointestinal tract (ie, nausea, diarrhea, and belching).
The bulk of the data support omega-3 fatty acids' role in the treatment of mood disorders. While data are promising for psychiatric illness beyond affective disorders, it is premature to routinely recommend omega-3 fatty acids as the primary treatment for most other psychiatric disorders. However, given the favorable side effect profile and cardiovascular benefits of omega-3 fatty acids, they would appear to be safe for most populations.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.