
Abstract
Valproic acid is widely used in the treatment of behavioral disturbances in patients with dementia; however, there is uncertainty about its dosing and studies have reported mixed findings. The current article examines published trials of valproic acid in the treatment of patients with dementia to identify whether an optimal dosing strategy exists. Secondarily, valproic acid dosing from published studies is compared with a real-world 5-year sample of valproic acid prescribing. Twenty studies met selection criteria and were included in the review. Based primarily on uncontrolled trials and the current retrospective study, valproic acid serum levels between 40 and 60 mcg/mL and relatively low doses (ie, 7-12 mg/kg per d) are associated with improvements in agitation in some patients with dementia. At the same time, similar valproic acid levels produced no significant behavioral improvements in most placebo-controlled studies and led to substantial side effects in some patients. Considerable trial design differences exist between controlled and uncontrolled trials. Overall, valproic acid appears to have limited efficacy as monotherapy in many patients with dementia. Its optimal role may be in combination with other psychotropics as a treatment of agitation associated with dementia.
Background
The use of anticonvulsants in patients with dementia, of which valproic acid is the most commonly prescribed, remains controversial. Interest in valproic acid as a therapy in patients with dementia stems from plausible mechanisms of action and a lack of treatments with balanced efficacy and safety. Valproic acid has been postulated to produce symptomatic improvements in dementia via its actions on gamma-aminobutyric acid (GABA) and N-methyl-
A number of reviews regarding the use of valproic acid in patients with dementia have been published, often with conflicting conclusions. Older reviews, based primarily on open-label and retrospective studies, generally end with positive statements regarding the potential of valproic acid in patients with dementia. 22–28 On the other hand, more recent reviews that incorporated controlled trials did not usually reach such positive conclusions. 1,29–32 Some of this uncertainty may stem from the variety of valproic acid dosing strategies employed in previous studies and the clinical reality that optimal dosing of valproic acid for behavioral disturbances in dementia remains uncertain. Previous reviews have not clearly identified optimal dosing and controlled trials have left clinicians with unanswered questions regarding the prescribing of valproic acid in patients with dementia. Many of the controlled trials of valproic acid in patients with dementia employed fixed doses, target doses prior to flexible dosing, or minimum dose requirements that may have increased the likelihood of medication side effects while hindering clinicians from achieving optimal doses of valproic acid. 33–36 The appropriate dosing and therapeutic monitoring of valproic acid in patients with dementia are important when considering the variability in valproic acid pharmacokinetics in the elderly, side effect profile of valproic acid, susceptibility of older adults to medication side effects, and inconsistency between valproic acid serum concentration and dose. 37,38 The purpose of the current review is to examine published trials of valproic acid in the treatment of patients with behavioral disturbances in dementia to specifically identify whether an optimal dosing strategy exists. Secondarily, we will compare valproic acid dosing from published studies with a 5-year sample of valproic acid prescribing in a real-world setting to explore whether differences in valproic acid dosing are present between published trials and clinical practice.
Methods
Review Component
We conducted a MedLine, International Pharmaceutical Abstracts, and clinicaltrials.gov search through April 2011 for articles or trials written in English that contained combinations of the following terms: valproate, valproic, divalproex, depakote, dementia, and Alzheimer. As a result of the initial search process, the references of published articles we identified were also examined for any additional studies appropriate for inclusion in this review. Studies were included if they had at least 10 patients, an efficacy outcome, and reported (or we were able to calculate) mean valproic acid daily dose and mean valproic acid serum level. The term valproic acid will be used throughout the article to represent all formulations of the drug (ie, valproic acid, valproate, and divalproex).
Retrospective Study Component
We retrospectively examined valproic acid dosing in patients admitted to a 10-bed Senior Behavioral Medicine Unit (SBMU) between January 2006 and December 2010. The unit is a locked geriatric psychiatry ward located near a metropolitan city in North Carolina. Medically stable patients of at least 55 years who have a primary psychiatric diagnosis are eligible for admission. Patients are admitted from multiple counties in North Carolina via numerous referral sources. The SBMU is the only facility of its kind in the county or adjacent counties.
We included patients with an existing diagnosis of dementia who were taking valproic acid. Individuals in whom valproic acid was initiated while an inpatient or continued as part of outpatient therapy were eligible for study inclusion. At least 1 steady state serum level of valproic acid reflecting the optimized valproic acid dose at discharge must have been drawn during each person’s stay. Patients with psychiatric or medical diagnoses for which valproic acid might also be used as therapy were excluded from the study (eg, seizure disorder, bipolar disorder, schizoaffective disorder, migraine headaches, etc). Individuals with other medical causes for the behavioral disturbances related to their admission were also excluded (eg, delirium, medication withdrawal, intoxication, etc). Demographic, diagnostic, medication, and drug level data were collected using each patient’s medical chart and from discussions during multidisciplinary treatment team rounds. Chart data were gathered and treatment team attended as a regular part of the primary investigator’s clinical duties. This information was then examined for the current study.
The primary objective of our retrospective study was to describe valproic acid dosing among adults admitted to a geriatric ward, experiencing behavioral disturbances associated with dementia. This was accomplished by examining each patient’s optimized discharge dose of valproic acid (ie, prescribed dose at the time of discharge), steady state valproic acid serum level associated with the discharge valproic acid dose, and weight. Secondarily, we examined whether residential status (home vs facility), scheduled use of antipsychotics, scheduled use of benzodiazepines, or use of valproic acid on admission was associated with valproic acid dose (mg/kg) or serum level (mcg/mL). Analysis of variance was utilized for these secondary objectives. We also examined the relationship between valproic acid serum level and valproic acid dose, weight, and serum albumin using Pearson correlation. We conducted analyses using SPSS version 15.0. Tests were 2-tailed with statistical significance set at a P value <.05. The medical center’s institutional review board approved this retrospective study; informed consent was not required.
Results
Review Component
Twenty studies met selection criteria and were included in the review (Table 1 ). Eighteen of the studies examined the effects of valproic acid on patients with psychosis or behavioral disturbances in dementia, 33–36,39–52 one investigation involved valproic acid for the prevention of behaviors, 53 and another trial investigated the tolerability of valproic acid. 54 Seventeen of the 20 investigations administered divalproex, the remaining 3 trials employed sodium valproate. 35,48,51 Overall, the mean age of patients was 80 (standard deviation [SD] 5), most had AD, and the mean Mini-Mental State Examination (MMSE) at baseline was 10 (SD 4). Agitation and aggression were the most common indications for valproic acid use. Only 2 studies involved outpatients, 53,54 the remaining were based on inpatient units (n = 8) 34,35,39,43,44,46–49 or long-term care or nursing facilities (n = 10). 33,36,40–42,45,48,50–52 The mean daily dose of valproic acid employed was 878 mg (SD 346) at a mean serum level of 52 mcg/mL (SD 10). Mean valproic acid serum levels among the studies ranged from 36 to 69 mcg/mL. Unfortunately, only 8 of the 20 investigations reported data that allowed for the calculation of weight-based doses (mean = 12 mg/kg [SD 4]). 33,35,36,39,45,51,52,54 Seven of the 20 trials were randomized, double-blinded, and controlled, 33,35,36,45,52–54 6 of these were efficacy trials. 33,35,36,45,52,53 All other studies were open label (n = 8) or retrospective (n = 5) in design.
Valproic Acid Studies Included in Current Review
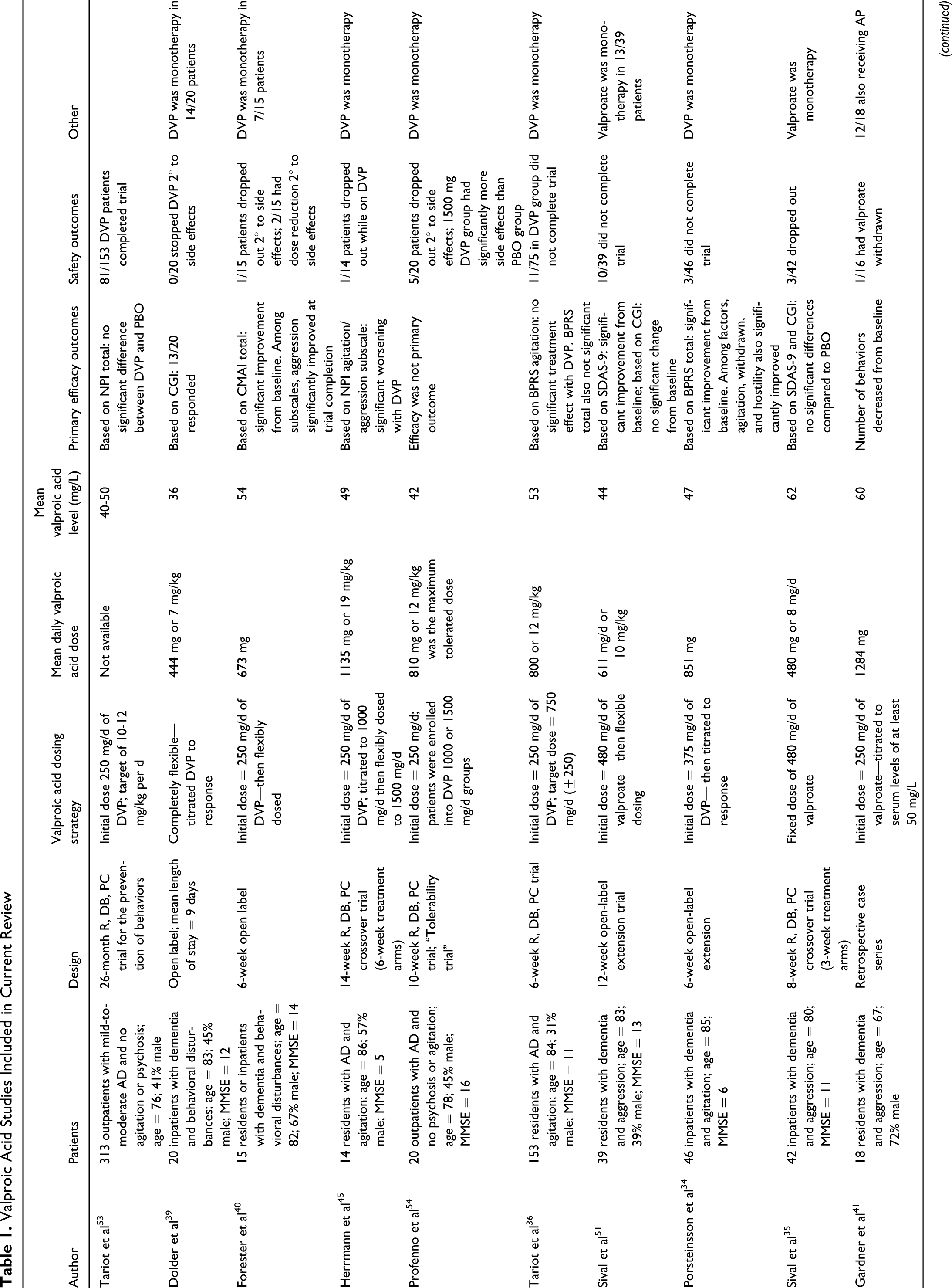
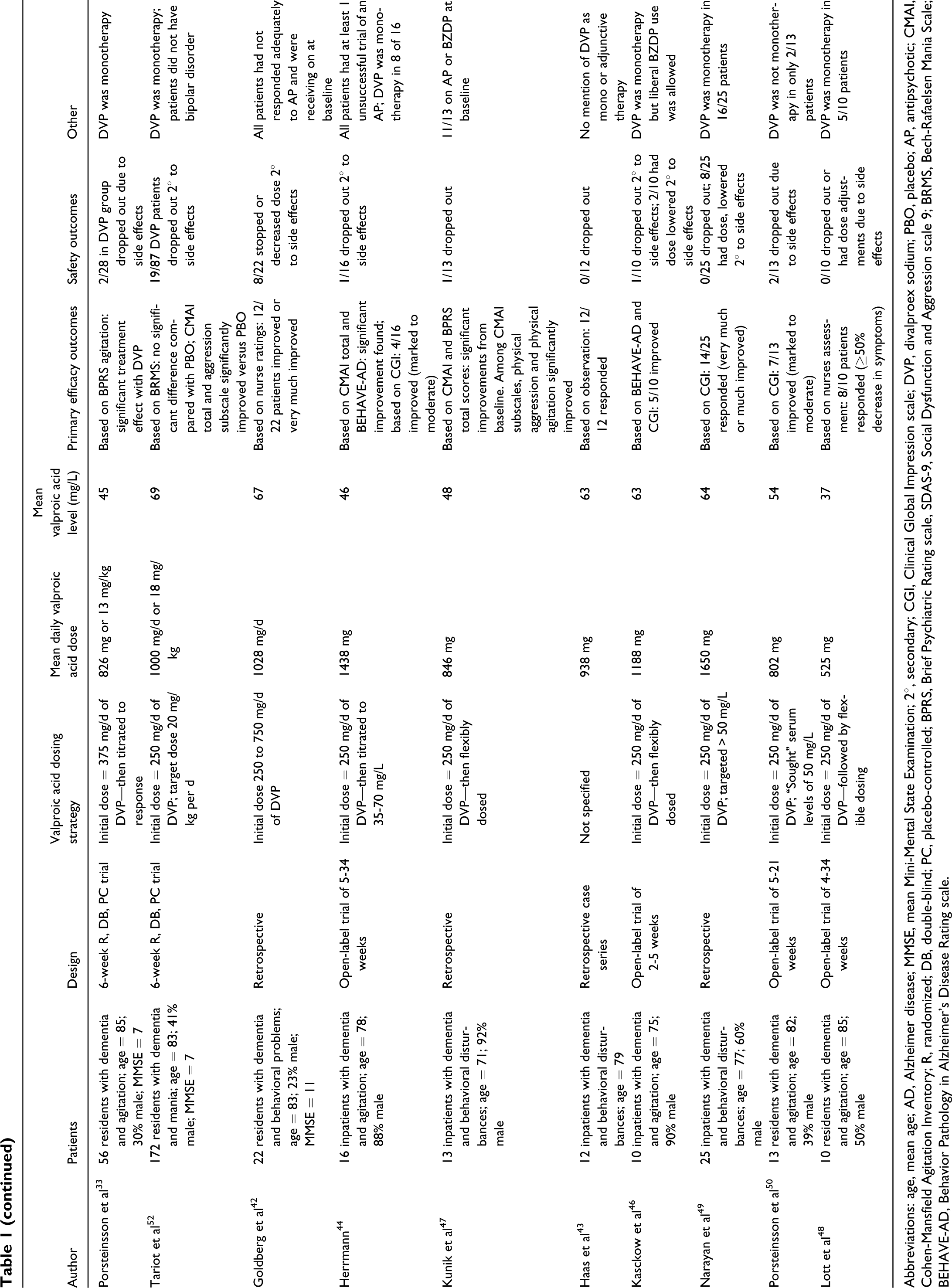
Abbreviations: age, mean age; AD, Alzheimer disease; MMSE, mean Mini-Mental State Examination; 2°, secondary; CGI, Clinical Global Impression scale; DVP, divalproex sodium; PBO, placebo; AP, antipsychotic; CMAI, Cohen-Mansfield Agitation Inventory; R, randomized; DB, double-blind; PC, placebo-controlled; BPRS, Brief Psychiatric Rating scale, SDAS-9, Social Dysfunction and Aggression scale 9; BRMS, Bech-Rafaelsen Mania Scale; BEHAVE-AD, Behavior Pathology in Alzheimer’s Disease Rating scale.
In terms of efficacy, 14 (74%) of 19 studies reported statistically or clinically significant improvements in their respective primary outcome measures. 33,34,39–44,46–51 Only 1 (17%) of 6 efficacy studies that were randomized, blinded, and controlled found significant behavioral improvements with valproic acid based on their primary outcome measure. 33 In contrast, all 13 of the uncontrolled efficacy trials reported improvements. Upon further examination, a lack of clarity in the target behaviors investigated and the nonspecific nature of some of the behavioral assessments used makes it difficult to clearly gauge the role of valproic acid among studies. This problem occurs from differences in trials that then hinder direct comparison of results. For instance, most studies examined patients with dementia and agitation or aggression, but 6 investigations were nonspecific when it came to the target symptom being studied. 39,40,42,43,47,49 All 6 of these trials reported positive results but also tended to use nonspecific outcome assessments. Thus, it is difficult to understand what valproic acid specifically improved. Seven studies used and reported behavioral scales along with the scale’s components, allowing for more insight into which target symptoms valproic acid may be most useful. 33,34,36,40,45,47,52 Five of these 7 studies found statistically significant improvements in agitation and to a lesser extent aggression. Among these 7 trials, 4 were placebo controlled, only 2 of which reported significant improvements versus placebo. 33,52 Study limitations prohibited analysis of which aspects of agitation valproic acid may or may not improve.
The median valproic acid serum level among controlled trials was 49 mcg/mL compared with 54 mcg/mL among uncontrolled trials. Such a difference in efficacy by trial design despite similarities in serum levels necessitates further analysis. The controlled trials tended to be longer in duration and enrolled more patients. At the same time, the prescribing and place in therapy for valproic acid differed by study design. All the controlled trials employed valproic acid as monotherapy. On the other hand, only 8% of the uncontrolled trials limited the use of valproic acid as a monotherapy. 34 Most of the uncontrolled trials had a mix of patients, some receiving valproic acid as monotherapy and many others receiving concomitant antipsychotics or benzodiazepines. Valproic acid serum levels were similar between studies using valproic acid as monotherapy and those employing valproic acid in combination therapy. In terms of valproic acid dosing, 71% of the controlled trials utilized fixed dose or target dose strategies compared with only 42% of all uncontrolled trials reporting their valproic acid dosing strategy.
Differences in efficacy outcomes were likely affected by the behavioral assessment chosen for each study’s primary outcome. Seven of the 14 uncontrolled trials relied on nonspecific (eg, Clinical Global Impression [CGI]) or general clinician observation scales to measure efficacy. 23,39,42,43,48–50 In contrast, all the controlled investigations utilized psychopathology rating scales, many of which were specific to geriatric psychiatry (eg, Neuropsychiatric Inventory (NPI), Cohen-Mansfield Agitation Inventory [CMAI]) and had the ability to measure changes in specific behavioral symptoms such as psychosis or agitation. 33,36,45,52,53
Retrospective Study Component
Seventy-two patients met the selection criteria and were included in the analysis. They were of a mean age of 80 (SD 7) and had a mean MMSE score of 12 (SD 7) at the time of admission. Patients tended to be Caucasian (86%), male (72%), and came from a facility (75%). AD (64%) was the most common dementia diagnosis. Agitation and aggression were by far the most common reasons for admission to the SBMU. At the time of discharge, most patients were receiving an acetylcholinesterase inhibitor (21%), memantine (25%), or a combination of both medication types (17%). Antidepressant use was also common, with 34 of 72 individuals prescribed this class of psychotropic at the time of discharge. Valproic acid as a monotherapy for behavioral symptoms represented a minority of patients; 31% were receiving scheduled doses of an antipsychotic and 33% were prescribed a benzodiazepine in addition to valproic acid on discharge from the inpatient unit.
Scheduled doses of valproic acid were initiated in 44 of 72 patients while the remaining individuals (39%) were continued on valproic acid. The mean daily dose of valproic acid at the time of discharge was 578 mg (SD 312) and the mean steady state serum level associated with this prescribing was 42 mcg/mL (SD 19). Based on weight, this represented a mean valproic acid dose of 8 mg/kg (SD 5) at the time of discharge. Patients who were admitted on valproic acid had higher serum levels (50 vs 36 mcg/mL; F 1,64 = 7.15, P = .01) and valproic acid doses (11 vs 7 mg/kg; F 1,50 = 9.61, P = .003) at discharge than those who were initiated on valproic acid on or after admission. Residential status, the use of scheduled antipsychotics, or the use of scheduled benzodiazepines were not significantly associated with valproic acid serum level or dose (P value range = .071-.56). Albumin and patient weight were not significantly correlated with valproic acid serum level (P value range = .58-.98); valproic dose at discharge was significantly correlated with serum level at discharge (Pearson coefficient = .64, P = .01).
Valproic Acid Dosing: Review Versus Retrospective Study
Valproic acid dosing utilized in the 20 trials reviewed was similar but somewhat higher than our current retrospective examination. Serum valproic acid levels between 40 and 60 mcg/mL were the most common therapeutic range achieved in both previously published studies and our current investigation. An important difference is the use of valproic acid as monotherapy. Controlled trials of valproic acid predominantly restricted its use to monotherapy, whereas our study and many of the previously published uncontrolled trials allowed for valproic acid to be used with other psychotropics, especially antipsychotics. Interestingly, similar valproic acid serum levels were achieved regardless of whether valproic acid was monotherapy or combination therapy. These findings call into question the effectiveness of valproic acid as a monotherapy in many patients with behavioral disturbances in dementia. At the same time, the appropriateness, effectiveness, and safety of valproic acid as an adjunctive treatment in patients with dementia needs to be further studied. Our retrospective study of valproic acid was limited by a lack of clinical rating scales, short duration, involvement of a single geriatric psychiatric unit, and small number of patients. On the other hand, it was designed to provide real-world insight into the use of valproic acid in patients with dementia and patients were carefully selected to exclude confounding factors (eg, delirium, non-steady state valproic acid levels, unclear indication for use). The demographics of the previously published trials and the current retrospective study were similar, allowing for easier comparisons in valproic acid dosing and serum levels. Regardless of limitations, our study highlights the commonplace use of relatively low doses of valproic acid in patients with dementia.
Safety Considerations
The use of available treatment options for behavioral disturbances in patients with dementia, including antipsychotics, benzodiazepines, and anticonvulsants, are often limited due to adverse effects. Antipsychotics have been linked to increased cardiovascular events and mortality in patients with dementia. 30 Additionally these agents should be monitored for metabolic effects, anticholinergic side effects, extrapyramidal symptoms, and QT prolongation. Benzodiazepines have been associated with falls and cognitive impairment in elderly patients and those with dementia. Carbamazepine is associated with potentially severe adverse effects and clinically relevant drug–drug interactions. 23,24 Valproic acid is also associated with problematic side effects. There are several hypothesized variables, which may affect the safety and tolerability of valproic acid. Medication-specific factors include drug formulation, frequency of daily use, dose, titration rapidity, and plasma concentration. In addition, some patient-specific features include age, severity of dementia, ambulatory status, and concomitant medications.
Six randomized, placebo-controlled trials have evaluated safety and tolerability with valproic acid use in patients with dementia and associated behavioral disturbances. These studies varied in dose (480-1135 mg/d), titration schedules, and generally had short treatment durations (3-10 weeks). 33,35,36,45,52,54 Overall incidence or mean number of adverse events were significantly higher in treatment groups when compared with placebo in 4 of these studies. 33,45,52,54 Somnolence and thrombocytopenia occurred more frequently with the use of valproic acid. The clinical implications of these adverse effects are of great consequence as they may predispose patients to falls or worsen the outcomes of a fall, respectively. One study by Tariot et al was suspended early due to a disproportionate dropout rate in the treatment group due to adverse effects (22% vs 4%, P ≤ .001), driven primarily by somnolence. 52 The authors attributed this to an excessive dose and titration schedule for the patient population (125 mg twice daily increased by 125 mg daily to a target dose of 20 mg/kg per d). Subsequent trials titrated doses only every 3 to 7 days. These studies did not specifically evaluate the differences in sedation; however, they included a combined adverse effect end point that included sedation. Three of the 5 trials showed a statistically significant increase in this end point with valproic acid compared with placebo. 33,35,36,45,54 Although dose and titration schedule were frequently implicated as a cause for increases in adverse effects, a dose–side effect relationship was not assessed in all the controlled investigations. Two studies stated that neither serum level nor dose was associated with the incidence of overall adverse effects. 33,35 Authors of 1 study were concerned about accuracy of levels and were unable to evaluate an effect and the other 2 trials did not address a potential dose–side effect relationship. 36,45,54 Platelet levels were evaluated in 5 trials, 4 of which showed a significant decrease compared with placebo. 30,33,36,45,52,54
Other important adverse effects which should be considered with valproic acid therapy are diarrhea, weight loss, and decreased MMSE score. 36,52,54 In patients with dementia, electrolyte disturbances and dehydration due to diarrhea may present a considerable risk, potentially contributing to falls and cardiovascular events. Weight loss, which is a common concern in those with dementia, may also pose a significant problem for this patient population. Additionally, the food and drug administration (FDA) has issued a boxed warning regarding valproic acid’s potential to cause hepatotoxicity and pancreatitis. 30 The risk of hepatotoxicity is highest among children under the age of 2 and typically occurs within the first 6 months of therapy. 23,29,38 None of the 6 placebo-controlled trials reported incidence of either of these adverse effects.
Clinical and Research Implications
The current review highlights that valproic acid for the treatment of behavioral disturbances in dementia involves serum levels less than those routinely used for bipolar disorder (40-60 mcg/mL vs 50-125 mcg/mL, respectively). Of the behavioral symptoms seen in patients with dementia, agitation appears to be the most amenable to valproic acid treatment. Controlled clinical trials clearly demonstrate that achieving such a serum level does not necessarily lead to significant behavioral improvement. In fact, similar serum levels of valproic acid tended to not produce significant behavioral benefits in controlled trials while leading to improvements in uncontrolled trials. Our examination of dosing strategies used in previously published studies found that few investigations took patient weight into account and some that did reported conflicting results. 55 Not accounting for weight when dosing valproic acid may create uncertainty among clinicians and variability in the use of valproic acid in patients with dementia, especially with respect to initial dose and titration. In the current review, studies that showed benefits with valproic acid used relatively low amounts that were titrated to doses between 7 and 12 mg/kg per d. Expert consensus guidelines on the treatment of dementia also advocate for lower daily doses of valproic acid (initial dose of 250-375 mg and target dose of 625-825 mg) but do not clearly account for patient weight or serum levels. 1,56 Initiating and titrating valproic acid without factoring in patient weight may lead to more side effects and poorer tolerability. Regardless, valproic acid should be individually dosed in an effort to maximize benefit while minimizing side effects. Future trials that more flexibly use valproic acid or at least initiate valproic acid taking weight into account are warranted. Although the 20 reviewed studies show some potential benefit of valproic acid as a behavioral treatment in dementia overall, controlled trials bring into question the effectiveness of valproic acid as monotherapy for many patients with behavioral disturbances in dementia. Previously published uncontrolled trials and our current retrospective study hint that the role of valproic acid in many patients with dementia may be limited to use with another psychotropic. It has been suggested that the combination of valproic acid and an antipsychotic produces central nervous system effects different than either agent alone. 40,57 As opposed to concomitant use of benzodiazepines or other anticonvulsants, the GABAergic effects of valproic acid and the dopaminergic actions of antipsychotics, when used together, may allow for lower doses of each drug. 40 At the same time, our finding that similar valproic acid serum levels were achieved regardless of whether valproic acid was monotherapy or combination therapy leads to several important questions including (1) what is the active entity or entities when valproic acid is used in conjunction with other psychotropics, (2) what psychotropics, if any, should be used with valproic acid, and (3) should clinicians target different valproic acid serum levels based solely on the monotherapy status of valproic acid? Controlled trials of valproic acid as adjunctive or combination therapy in patients with dementia are needed. Fortunately, 3 trials with ongoing recruitment (NCT00315900, NCT00208819, and NCT00197834) are examining the use of valproic acid in patients with dementia, including valproic acid versus an atypical antipsychotic and valproic acid in addition to an atypical antipsychotic. 53 Hopefully, these and other future investigations will shed more light on the appropriate use or nonuse of valproic acid in dementia. Studies that specifically enroll patients with dementia and agitation and then assess the effect of treatment on agitation and its subtypes (eg, aggression, physical disruption, verbal disruption, social inappropriateness) are also needed. Based on limited data, valproic acid does not appear to be helpful for the prevention of behavioral disturbances in dementia.
Conclusion
Valproic acid may be beneficial in some patients with agitation associated with dementia. Based primarily on uncontrolled trials, valproic acid serum levels between 40 and 60 mcg/mL and relatively low doses of valproic acid (ie, 7-12 mg/kg) are associated with symptomatic improvement. At the same time, the same range of valproic acid serum levels has not been shown to produce significant behavioral improvement in most controlled studies. On the other hand, differences in the role of valproic acid (monotherapy vs combination therapy and flexible dosing vs less flexible dosing) leave important questions unanswered. The optimal role of valproic acid in the treatment of behavioral symptoms in dementia may be in combination with other psychotropics, although additional data are needed. Valproic acid does not appear to be beneficial as a modality to prevent behavioral symptoms. Clinicians should titrate valproic acid, taking patient weight into account, in an effort to reduce side effects. In addition, the ability of valproic acid to produce problematic and even serious side effects in some older adults cannot be overlooked and clinicians must use valproic acid with caution in patients with dementia.
Footnotes
The authors completed all works related to the manuscript as part of their regular job duty, and no additional funding was used in the preparation of the manuscript.
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: the first and second authors have no actual or potential conflicts of interest to disclose. Dr McKinsey serves as a speaker for Lilly Pharmaceuticals.
The author(s) received no financial support for the research, authorship, and/or publication of this article.