
Abstract
The purpose of this review is to discuss the clinical application of pharmacogenomics for select drug therapies (eg, proton pump inhibitors [PPIs], codeine, and carbamazepine) and to highlight limitations and challenges that preclude implementation of pharmacogenomics into clinical practice. Genetic polymorphisms of cytochrome P450 (CYP) enzymes and the presence of the human leukocyte antigen (HLA)-B*1502 allele influence drug disposition and/or response. A portion of PPI pharmacokinetic and pharmacodynamic variability can be explained by CYP2C19 genotype. However, conflicting evidence exists related to Helicobacter pylori cure rates based on CYP2C19 genotype. For codeine, adverse drug reactions in neonates through breast-feeding from CYP2D6 ultra-rapid metabolizers have been reported. However, there is lack of conclusive evidence regarding the overall influence of CYP2D6 polymorphisms on codeine efficacy and toxicity. Although CYP2C19 and CYP2D6 genotyping tests are available, clinical utility remains low. The presence of the HLA-B*1502 allele is associated with carbamazepine-induced Stevens-Johnson syndrome (SJS) and/or toxic epidermal necrolysis (TEN). Pharmacogenomic testing is required prior to initiating carbamazepine in high-risk patients. Lack of sufficient resources, provider knowledge, and ethical, legal, and social issues are several limitations and challenges to implementing pharmacogenomic testing in clinical practice.
Learning Objectives
At the conclusion of this article, the participant will be able to:
Identify the functional effects of select genetic polymorphisms and the impact on drug dosing, efficacy, and/or toxicity.
Describe pharmacogenomic tests for select medications based on current evidence for testing recommendations and clinical use.
Discuss currently available evidence-based recommendations for pharmacogenomic testing for select medications.
State at least one study design limitation that is observed in pharmacogenomic studies.
State at least one challenge that affects implementation of pharmacogenomic testing into clinical practice.
Introduction
Pharmacogenomics is a rapidly developing field that has important potential clinical application on individualizing therapy to maximize efficacy and/or minimize toxicity. Numerous, but similar definitions of pharmacogenetics/pharmacogenomics have been proposed by professional organizations, regulatory agencies, and researchers. Pharmacogenetics is defined as “the study of genetic causes of individual variations in drug response.” 1 Pharmacogenomics is defined as “the genome-wide analysis of genetic determinants of drug efficacy and toxicity.” 2 While pharmacogenetics focuses on a single or a few genes, pharmacogenomics examines genes in all chromosomes. Although pharmacogenetics and pharmacogenomics are used interchangeably, for purposes of this review, the preferred term will be pharmacogenomics.
This review discusses the pharmacogenomics of specific drug therapies (eg, proton pump inhibitors [PPIs], codeine, and carbamazepine) and highlights the limitations and challenges with clinical applications of pharmacogenomics testing. Each example will discuss (1) background, (2) gene/allele of interest and functional effect, (3) population prevalence, (4) clinical relevance of the polymorphism related to dosing, efficacy, and/or toxicity, and (5) pharmacogenomic testing and recommendations. The therapeutic areas were selected based upon the level of evidence for testing recommendations that either support or refute the role of pharmacogenomic testing and clinical utility. Clinical utility was based upon the frequency of pharmacogenomic testing in the clinical setting. For example, with carbamazepine, the level of evidence of pharmacogenomic testing is high as well as its clinical utility. Regarding codeine, the level of evidence for pharmacogenomic testing is moderate, while the clinical utility is low at this time. Reviews of pharmacogenomic principles, concepts, and nomenclature are published elsewhere 3,4 and will not be discussed.
Understanding the Clinical Significance of Polymorphisms
A polymorphism for a specific protein may vary in terms of the functional effect, population prevalence, and clinical relevance. Consequently, a systematic approach to understanding polymorphisms is suggested (Table 1). Since proteins are generally affected by the polymorphism, it is important to first identify the polymorphism. Enzymes, drug transporters, and/or receptors are examples of proteins that are genetically polymorphic, of which the functional effect can result in increased, decreased, or no change in protein activity. The next step is to consider whether population variation exists for a polymorphism. Examples exist where a polymorphism is present in a higher frequency in a specific ethnic group. 5 In determining clinical relevance, relationships between the polymorphism and drug and disease for an individual should be examined. Drug dosing, efficacy, toxicity, pharmacokinetics, and/or pharmacodynamics may be affected by the polymorphism. A polymorphism may also influence disease prognosis, susceptibility, or be used as a screening test for certain diseases. 6
Systematic Approach to Understanding Polymorphisms a

a Reprinted from Joseph Ma, “Module I: Principles and Concepts, PharmGenEd™ Program.” July 16, 2009, by permission of PharmGenEd™. Copyright © 2009 Regents of the University of California. All rights reserved.
Examples of Clinical Application of Pharmacogenomics
Proton Pump Inhibitors
Background
PPIs (omeprazole, esomeprazole, lansoprazole, dexlansoprazole, pantoprazole, and rabeprazole) are indicated for treatment of various gastric acid-related disorders (eg, duodenal ulcer, gastric ulcer, gastroesophageal reflux disease, and Zollinger-Ellison syndrome). They are used in combination with 1 or 2 antibiotics for Helicobactor pylori (H pylori) eradication. 7,8 PPIs are irreversible inhibitors of the H+/K+ ATPase pump, thus impacting acid secretion in the gastric tract. Detailed reviews of PPI pharmacokinetics are published elsewhere. 8,9 Omeprazole, esomeprazole, lansoprazole, and pantoprazole are primarily metabolized by CYP2C19 and to some extent by CYP3A. However, the extent of CYP2C19 and CYP3A metabolism between PPIs is variable. 10 Rabeprazole is predominantly metabolized via nonenzymatic reduction to a thioether. 8,11
Gene/Allele of Interest and Functional Effect
The CYP2C19 gene is located on chromosome 10 (10q24.1-q24.3) and contains 9 exons. 12,13 CYP2C19*1 codes for normal (wild-type) enzyme activity. At least 27 variant alleles for CYP2C19 have been identified, 14 with the most extensively described variant alleles being CYP2C19*2 and CYP2C19*3. Regarding CYP2C19*2, a splicing defect in exon 5 occurs, resulting in early termination of protein synthesis. 15 CYP2C19*3 is a premature stop codon single-nucleotide polymorphism, which results in a truncated protein. The functional effect of these polymorphisms is a complete loss of (or null) enzyme activity. Other CYP2C19 alleles result in a loss of (CYP2C19*4-*8) or reduced (CYP2C19*9, *10, and *12) enzyme activity. 14,16 In contrast, increased enzyme activity is associated with CYP2C19*17. 17
Population Prevalence
In caucasians, Asians, and African Americans, CYP2C19*2 frequencies are approximately 15%, 30%, and 17%, respectively, while the CYP2C19*3 frequencies are approximately 0.04%, 5%, and 0.4%, respectively. 9,18 –20 Allele frequencies for CYP2C19*17 are approximately 18% in caucasian and Ethiopian populations and 4% in Asian populations. 21
A gene–dose effect is commonly observed for medications metabolized by CYP2C19, thereby allowing stratification of subjects by CYP2C19 genotype. CYP2C19 homozygous extensive metabolizers (EMs) are individuals who possess 2 wild-type alleles, CYP2C19 heterozygous EMs are individuals who possess 1 wild-type and 1 decreased/null variant allele, and CYP2C19 poor metabolizers (PMs) are individuals who possess 2 decreased/null activity alleles. 22 The population prevalence of CYP2C19 PMs ranges from 1% to 4%, 15% to 23%, and 2% to 7% in caucasians, Asians, and African Americans, respectively. 18
Clinical Relevance
Although H pylori dual/triple therapies for eradication vary in terms of PPI use and in PPI dosing, there are currently no published studies that have examined PPI dosing strategies based on CYP2C19 genotype. This may be due to the large therapeutic window of PPIs, low incidence of clinically significant adverse effects, and multitude of dual/triple therapy regimens that are available. There is suggestion that higher PPI doses be considered in homozygous EMs, yet it remains to be implemented in clinical practice. 23
The majority of clinically relevant data have focused on the effect of CYP2C19 genotypes on H pylori eradication, with little attention to adverse effect risk. PPIs are unique in that pharmacokinetic (PK) variability affects pharmacodynamic (PD) variability. Omeprazole area under the concentration–time curve (AUC) is 7- to 14-fold higher in PMs compared to homozygous EMs. 24 –26 Omeprazole AUC correlates with intragastric pH (r = .87, P < .0001), of which CYP2C19 PMs have higher intragastric pH concentrations compared to CYP2C19 EMs. 26,27 A higher intragastric pH has been shown to increase antibiotic concentrations and improve antibiotic bioavailability and stability. 28 –31
The PK and PD variabilities for PPIs, explained to some extent by CYP2C19 genetic polymorphisms, have resulted in different H pylori cure rates. In one study, Japanese patients (n = 62) with confirmed H pylori infection were administered dual therapy with omeprazole and amoxicillin for several weeks. H pylori cure rates were 28.6%, 60%, and 100% in homozygous EMs, heterozygous EMs, and PMs, respectively (Table 2). 23 These results are consistent with a majority of studies with omeprazole. 32 –36 In addition, several meta-analyses have concluded that omeprazole efficacy is dependent on CYP2C19 genotype. 37,38
Select Examples of H pylori Cure Rates Based on CYP2C19 Genotype
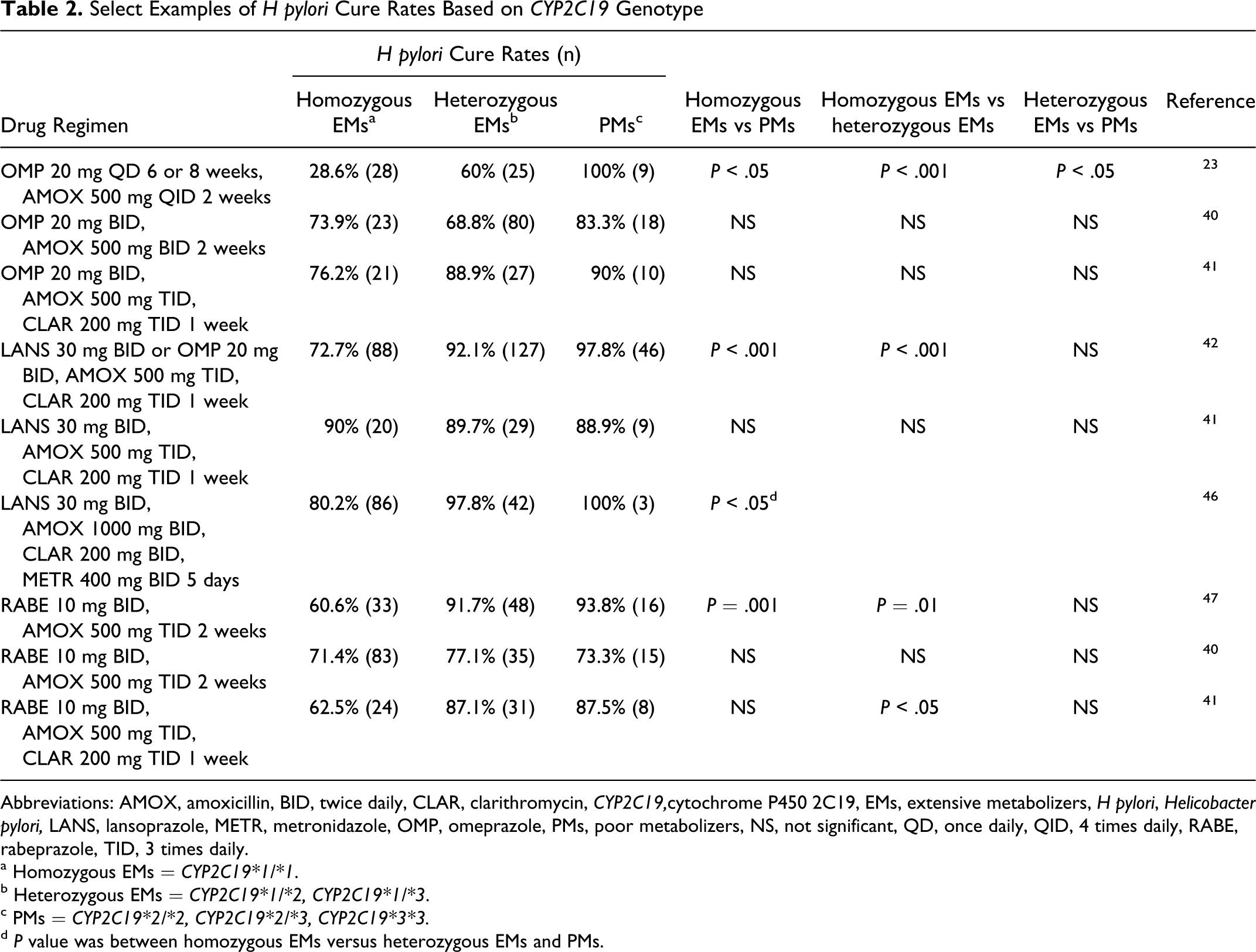
Abbreviations: AMOX, amoxicillin, BID, twice daily, CLAR, clarithromycin, CYP2C19,cytochrome P450 2C19, EMs, extensive metabolizers, H pylori, Helicobacter pylori, LANS, lansoprazole, METR, metronidazole, OMP, omeprazole, PMs, poor metabolizers, NS, not significant, QD, once daily, QID, 4 times daily, RABE, rabeprazole, TID, 3 times daily.
a Homozygous EMs = CYP2C19*1/*1.
b Heterozygous EMs = CYP2C19*1/*2, CYP2C19*1/*3.
c PMs = CYP2C19*2/*2, CYP2C19*2/*3, CYP2C19*3*3.
d P value was between homozygous EMs versus heterozygous EMs and PMs.
There are conflicting data regarding no difference in H pylori cure rates based on CYP2C19 genotype for omeprazole (Table 2). 39 –41 In one study, triple therapy with omeprazole, amoxicillin, and clarithromycin for 1 week was administered to patients with H pylori confirmed peptic ulcer disease (n = 183). H pylori cure rates were 76.2%, 88.9%, and 90% in homozygous EMs, heterozygous EMs, and PMs, respectively, with no difference based on CYP2C19 genotype (Table 2). 41 Conflicting data also exist for lansoprazole, 35,41 –46 rabeprazole, 39 –41,47 –50 and pantoprazole (Table 2). 51,52 Comparisons between studies are complicated due to the differences in the dual or triple drug regimens used and variability in PPI and/or antibiotic dosing.
Testing Availability and Recommendations
A Food and Drug Administration (FDA)-approved test is commercially available (AmpliChip® CYP450, Roche Diagnostics, Indianapolis, IN) for CYP2C19 genotyping. A whole blood sample is collected, DNA is extracted and then tested by a polymerase chain reaction–based microarray that analyzes the presence or absence of CYP2C19*2 and *3 alleles. Currently, there are no CYP2C19 testing recommendations for PPIs. The clinical pharmacology and drug–drug interaction sections in the prescribing information for esomeprazole, pantoprazole, and rabeprazole have been revised but with no recommendations for testing. 53 Recent publications of PPI use in patients who are on antiplatelet therapy 54 have influenced professional organizations to publish expert consensus statements. For managing therapy with thienopyridines and PPIs, the American College of Cardiology Foundation/the American College of Gastroenterology/the American Heart Association state that CYP2C19 testing has “not yet been established.” 55
Codiene
Background
Codeine is a weak opiate agonist in the central nervous system and is indicated for the relief of mild to moderately severe pain. 56 Codeine is a prodrug that converts to an active metabolite, morphine, via CYP2D6 by O-demethylation to exert its analgesic activity. 57 –59
Gene/Allele of Interest and Functional Effect
The CYP2D6 enzyme catalyzes hydroxylation or demethylation of multiple drugs such as neuroleptics, antidepressants, some beta-blockers, and codeine. 60 The CYP2D6 gene is located on chromosome 22, with at least 80 known variants of CYP2D6. 14 The interindividual variability of CYP2D6 enzyme activity can be explained by factors such as the genetic variation of CYP2D6. 61 –63 Genetic polymorphisms of CYP2D6 include phenotyping subgroups of PM, intermediate metabolizer (IM), EM, and ultra-rapid metabolizer (UM). 58,59 The EMs are considered to have normal enzyme activity. 64 –67 The median AUCs of the morphine metabolite increases from PM to EM to UM. 59 The CYP2D6*3, *4, *5, *6, and*7 alleles have been reported to account for the majority of decreased CYP2D6 enzyme activity. 61,63 In addition, the decreased activity of CYP2D6 in IMs has been shown to result from *9 and *10 alleles. 61 Gene duplication of CYP2D6 found in UMs is associated with higher plasma concentration and AUCs of morphine than in EMs. 59
Population Prevalence
Data pertaining to the population prevalence of codeine polymorphisms and metabolizer types are estimates only based on the studied populations. In the case of CYP2D6, the allele frequencies have been studied among European caucasians, Asians, and African Americans with variations found in CYP2D6*4, *5, and *10. 68 The most prevalent variant allele in caucasians is CYP2D6*4, ranging from 12% to 21%. 68 Other alleles found in caucasians include CYP2D6*3 (1%-2%), *5 (2%-7%), and *6 (1%). 68 Asians have the highest frequency (38%-70%) of CYP2D6*10; other alleles found in Asians include CYP2D6*4 (<1%) and *5 (4%-6%). 68 African Americans have the lowest prevalence rates for CYP2D6*4 (2%), CYP2D6*5 (4%), and CYP2D6*10 (6%). 68
The prevalence rates of CYP2D6 PMs are observed in caucasians (5%-10%), followed by African Americans (3%) and Asians (1%). 62,69 The prevalence rates of CYP2D6 UMs are observed in Europeans (3% in northern Europe, 1%-10% in western Europe, and 10% in southern Europe) and Saudi Arabians (10%-30% in northeast African countries). 70 –72 The prevalence rates of CYP2D6 UMs have also been reported in Ethiopians (29%). 60
Clinical Relevance
There is no definitive study reporting the efficacy of codeine associated with CYP2D6 polymorphisms. However, a study evaluating oxycodone (which has a similar chemical structure with codeine and is metabolized by CYP2D6) showed that PMs have a 2- to 20-fold decrease in analgesic effects compared to EMs, whereas the UMs had a 1.5- to 6-fold increase in analgesic effects. 73 However, there was no noticeable reduction in analgesic effects comparing PMs and EMs when oxycodone was given intravenously in a postoperative study. 73 Other studies have shown that an increased pain threshold is found in EMs but not in PMs. 62,74 The PMs have impaired O-demethylation; therefore, the analgesic effect of codeine may not be exerted in PMs. 58 Even though PMs may not experience analgesic effects expected from codeine, they can still develop side effects (eg, sedation, headaches, dizziness, and dry mouth), which may be related to codeine itself rather than its metabolites. 75 UMs experience greater analgesic effects but increased risks for opiate toxicity. 59,76,77
Evidence regarding the effect of CYP2D6 polymorphisms on codeine toxicity is primarily derived from case reports in neonates from breast-feeding UMs. 78 A case report described an adverse drug event related to codeine in a breast-feeding mother taking codeine 30 mg and paracetamol 600 mg for postpartum episiotomy pain management. 78,79 Her codeine dosage on day 1 was 60 mg (2 tablets) every 12 hours. However, due to side effects of somnolence and constipation, she took half of the dose from day 2 to day 14. Unfortunately, her 13-day-old baby died from a morphine overdose with a serum concentration of 70 ng/mL (neonates breast-fed by mothers receiving codeine typically have morphine serum concentrations of 0-2.2 ng/mL). 80 The morphine concentration found in her breast milk stored on day 10 was 87 ng/mL (normal range is 1.9-2.5 ng/mL for doses of 60 mg every 6 hours). The mother was genotyped and determined to be an UM of codeine (heterozygous for a CYP2D6*2A allele with CYP2D6*2 × 2 gene duplication). 78 The correlation between increased codeine concentrations and adverse effects in breast-feeding neonates has been observed in multiple studies. 81 –83 Subsequently, the FDA issued a warning, which was included in codeine’s prescribing information, stating that “maternal use of codeine can potentially lead to serious adverse reactions, including death, in nursing infants” and that “If a codeine containing product is selected, the lowest dose should be prescribed for the shortest period of time to achieve the desired clinical effect. Mothers using codeine should be informed about when to seek immediate medical care and how to identify the signs and symptoms of neonatal toxicity, such as drowsiness or sedation, difficulty breast-feeding, breathing difficulties, and decreased tone, in their baby.” 56,84
UMs have a higher rate of sedation compared to EMs (91% vs 50%, P = .069). 59 Other potential side effects for UMs include euphoria, dizziness, and visual disturbances 76,77,85 or more severe symptoms such as extreme sleepiness, confusion, shallow breathing, or respiratory depression. 56 Inhibitors of CYP2D6 will produce a phenotype similar to that of PMs (ie, lack of analgesic effect). Therefore, potential adverse drug interactions between codeine and CYP2D6 inhibitors should be monitored. 56
Testing Availability and Recommendations
Currently, the AmpliChip® DNA microarray, which can detect 33 CYP2D6 alleles, is the only approved test for CYP2D6 polymorphisms in the United States. 86,87 Laboratory monitoring is not necessary and no formal recommendation is required prior to initiation of codeine therapy. 79,84
Carbamazepine
Background
Carbamazepine is an anticonvulsant that is indicated for partial and generalized seizures, trigeminal neuralgia, and bipolar disorder. 88,89 The exact mechanism of action is unknown, but it has been shown to block the voltage-gated sodium channels. Carbamazepine is primarily metabolized by CYP3A4 to an active metabolite, carbamazepine-10,11-epoxide. 88 Carbamazepine has been linked to life-threatening idiosyncratic, type B adverse drug reactions, compared with type A reactions which are dose dependent. 90 These reactions can be severe cutaneous reactions ranging from Stevens-Johnson syndrome (SJS) to toxic epidermal necrolysis (TEN). The incidence of SJS/TEN is less than 2 patients per million per year 91 and the rate of death with these conditions (in absence of carbamazepine) range from 5% and 35% for SJS and TEN, respectively. 92 Recently, investigators have discovered an association with human leukocyte antigen (HLA)-B*1502 allele and the risk of SJS and TEN, specifically in Asians, who are prescribed carbamazepine. Most recently, HLA*3101 and HLA*1511 alleles have been recognized as potentially contributing to hypersensitivity reactions. 93 –95
Gene/Allele of Interest and Functional Effect
Due to early observations of hypersensitivity reactions in families and identical twins, the HLA has been a primary target for analysis of SJS/TEN reactions, which also tend to be familial in pattern. 96 The HLA-B*1502 allele and its association with SJS/TEN appears to be phenotype specific in that the allele is not associated with other hypersensitivity reactions due to carbamazepine, such as mild maculopapular eruptions (MPEs) or drug reactions with eosinophilia systemic symptoms. 97,98 The relationship between HLA-B*1502 and SJS/TEN appears to be drug specific in that the allele does not predict SJS/TEN by drugs other than carbamazepine. 99 However, other aromatic anticonvulsants such as phenytoin, oxcarbazepine, and lamotrigine may also cause similar hypersensitivity reactions in persons with the HLA-B*1502 allele. 100 The SJS/TEN hypersensitivity reactions have been theorized to be due to a noncovalent interaction between carbamazepine and HLA-B*1502 complex, leading to a CD8+-mediated cell death. 97,101
Population Prevalence
The high incidence of carbamazepine-induced SJS/TEN in Asians is correlated with the high frequency of HLA-B*1502 in the same population. The population prevalence of the allele is estimated to range from 10% to 15% in people from China (Han Chinese), Indonesia, Malaysia, Taiwan, Thailand, the Phillipines, and Vietnam, 2% to 8% in people from South Asia and less than 1% in Japanese, Koreans, African Americans, Europeans, and Hispanics. 102 –104
Clinical Relevance
While a preliminary study has been published regarding the role of microsomal epoxide hydrolase and its prediction of maintenance doses of carbamazepine, 105 there is no definitive study that has shown any specific gene/allele to accurately predict doses or clinical efficacy of carbamazepine. The most confirmed data are related to the toxicity associated with HLA-B*1502 and carbamazepine treatment. It was previously shown that caucasians who tested positive for the HLA-B*1502 allele were not at risk for carbamazepine-induced hypersensitivity. 106 In the landmark study of 44 Han Chinese patients, there was 100% association with the HLA-B*1502 allele and carbamazepine-induced SJS/TEN. 107 A follow-up study showed 59 of 60 patients with carbamazepine-induced SJS/TEN tested positive for the HLA-B*1502 allele. 98 The one patient who did not test positive for the HLA-B*1502 allele tested positive for the HLA-B*1558 allele. In comparison, 6 out of 144 controls (tolerant to carbamazepine) were found to be carriers for the HLA-B*1502 allele (OR = 1357, 95% confidence interval [CI]: 193.4-8838.3, P = 1.6 × 10−41). 98 In a separate study, a significant difference in the SJS/TEN incidence was found among patients who received carbamazepine depending on whether they were HLA-B*1502 carriers (100%) or noncarriers (14.5%). 103
In a study of 4877 Taiwanese patients who were candidates for carbamazepine therapy, 7.7% of the patients testing positive for the HLA-B*1502 allele were given an alternative medication or advised to continue their prestudy medication. The remaining 92.3% of the patients who tested negative for the HLA-B*1502 allele were advised to take carbamazepine. 108 Mild transient rash occurred in 4.3% of subjects. SJS/TEN did not develop in any HLA-B*1502-negative patient and when compared to historical controls was statistically significant (0% vs 0.23%, P < .001). 108
In addition to Chinese and Taiwanese patients, the HLA-B*1502 allele was studied in Thai patients in 2 studies. A case–control study was conducted in a Thai population in which the odds ratio for developing carbamazepine-induced SJS/TEN was 54.76 (95%CI: 14.62-205.13, P = 2.89 × 10−12) among those testing positive for HLA-B*1502. 109 The positive predictive value and negative predictive value of the HLA-B*1502 allele were 1.92% and 99.96%, respectively. Another study showed a strong association between HLA-B*1502 and carbamazepine- and phenytoin-induced SJS but not MPE. 110 Of the 81 patients with epilepsy, 31 subjects had antiepileptic drug-induced SJS/MPE. HLA-B*1502 was associated with carbamazepine-induced SJS and phenytoin-induced SJS (P = .005 and P = .0005, respectively).
As discussed before, the HLA-B*1502 allele may increase the risk of toxicity from other anticonvulsant drugs (lamotrigine, oxcarbazepine, and phenytoin) by contributing to SJS/TEN. 98,111,112 In a case–control study, HLA-B*1502 was present in 8 (30.8%) of 26 patients who received phenytoin and developed SJS/TEN (OR = 5.1, 95% CI: 1.8-15.1, P = .0041) and 3 (100%) of 3 patients who were tolerant to carbamazepine (OR = 80.7, 95% CI: 3.8-1714.4, P = 8.4 × 10−4). This was theorized to be partially due to similarities in aromatic structure between carbamazepine, oxcarbazepine, phenytoin, and lamotrigine. 98 Clinically, there is an estimated 20% to 30% cross-reactivity probability between these drugs. 113,114
In addition to HLA-B*1502, multiple HLA alleles have been recently identified as potential markers for carbamazepine-induced hypersensitivity reactions. The HLA-A*3101 has been associated with carbamazepine-induced hypersensitivity reactions in Japanese and Europeans. 94,95 Among Japanese, the HLA-B*1511 has been shown to be a risk factor for carbamazepine-induced SJS/TEN. 93 The HLA-B*1508, *1511, and *1521 as well as *1502 are all members of the HLA-B75 type and have been detected in studies in India and Thailand. One study reported an association with HLA-B*1518, HLA-B*5901, and HLA-C*0704 alleles and severe cutaneous adverse drug reactions. 115
Test Availability and Recommendations
HLA typing will indicate whether patients are positive if either 1 or 2 alleles of HLA-B*1502 are present. In 2007, the FDA recommended that all patients of Asian descent be screened for the HLA-B*1502 allele before initiating carbamazepine therapy. This recommendation is also reflected in the black box warning in the prescribing information of carbamazepine. 88 Therefore, prior to initiation of this drug in high-risk patients, genotyping is recommended.
It is important to note that patients who have been treated with carbamazepine for an extended period do not need testing for the HLA-B*1502 allele. The SJS/TEN reactions generally occur within the first 2 months of treatment and even with a positive HLA-B*1502 status, patients are considered to be at low risk. 102 However, patients who test negative for the HLA-B*1502 allele and receive carbamazepine should still be monitored clinically for development of hypersensitivity reactions since other genetic and nongenetic factors may contribute to these adverse drug reactions.
Limitations and Challenges of Pharmacogenomic Clinical Application
Pharmacogenomics has the potential to impact clinically relevant outcomes in drug dosing, efficacy, and toxicity, thus resulting in recommendations for testing. However, for PPIs and codeine, pharmacogenomics has not provided conclusive evidence to require such testing. A potential reason is that determining clinical relevance for some drugs will involve both genetic and nongenetic factors. Equally important is determining the extent of contribution of such factors. For example, adherence to therapy, antimicrobial resistance, and concomitant medication use are nongenetic factors that impact H pylori cure rates, 116 and all may play a significant role in treating disease.
Due to the low prevalence of a specific variant allele in a studied population, numerous pharmacogenomic studies were conducted with small sample sizes. In PPI studies, there was an unequal distribution of homozygous EMs, heterozygous EMs, and PMs, with a smaller number of PMs (Table 2). A small sample size is a study design limitation that increases the probability of an error due to a lack of sufficient statistical power. Results from such studies may not be accurate. Ideally, a pharmacogenomic study should have sufficient statistical power, with an equal stratification of subjects across groups. However, this may not be achievable as many variant alleles carry a frequency of 1% to 2% in the population. 5,117 In summary, caution is warranted in interpreting the clinical relevance of pharmacogenomic studies with small sample sizes.
Implementation of pharmacogenomic testing into clinical practice remains a major challenge due to issues related to lack of readily available resources, feasibility, level of evidence, and ethical, legal, and social issues. 4 There is also suggestion that health care providers’ knowledge on evidence-based information regarding pharmacogenomics testing is lacking. 118 In one study, 80% of pharmacist respondents disagreed that pharmacogenomics was an integral part of his or her pharmacy school curriculum. 118 This may be due to the sample population as the majority of respondents had more than 10 years of practice experience.
As pharmacists are anticipated to play an important role to prepare health systems and pharmacies in this emerging field, pharmacists need to obtain current pharmacogenomic information in order to translate the evidence into clinical practice. Several evidence-based genomics and/or pharmacogenomics online resources are available (Table 3). The PharmGenEd™ program is designed to provide pharmacists, physicians, students, and other health professionals access to evidence-based pharmacogenomic information. The objective of PharmGenEd™ is to help health care professionals increase awareness about current knowledge of the validity of pharmacogenomic tests and their potential clinical implications. Educational materials are designed to be relevant for clinical practice and include case vignettes for interactive learning. Continuing education lectures are available at national/regional/local professional meetings and via the program’s Web site. Using a train-the-trainer approach, the PharmGenEd™ program disseminates pharmacogenomics educational materials to qualified speakers and trainers.
Available Evidence-Based Genomics and/or Pharmacogenomics Online Resources

Abbreviations: CDC, Center for Disease Control and Prevention; FDA, US Food and Drug Administration.
Conclusions
There is increasing awareness of the contribution of genetic polymorphisms on impacting clinical outcomes. Although numerous studies have reported differences in PPI PK and PD variability based on CYP2C19 genotype, conflicting evidence exists regarding H pylori eradication rates for the majority of PPIs. Consequently, no formal recommendations exist to support CYP2C19 testing to predict PPI efficacy. The tragic case report of a baby death possibly related to CYP2D6 and codeine illustrates the importance of identifying patients with altered metabolism. However, CYP2D6 testing is not required prior to starting patients on codeine. In contrast, HLA-B*1502 testing is required prior to initiating carbamazepine in high-risk patients due to strong supportive evidence linking HLA-B*1502 and carbamazepine-induced SJS/TEN. Limitations and challenges of pharmacogenomic clinical application exist and need to be addressed prior to implementation of testing into clinical practice.
Continuing Education Credit
The NYSCHP is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. This program provides 1.6 contact hours (0.16CEUs) of continuing education. Universal Activity Number is 0134-0000-12-072-H01-P. Submission of exam for CE credit expires 8/31/2015.
A grade of 70% or above is required to earn the CE credit. Repeat examinations will be permitted once for a grade below 70%.
 There is no charge to NYSCHP members. Non Members are required to submit a processing fee of $15 and most go to www.nyschp. org to pay the fee to gain access to the online quiz. In lieu of this fee, a completed membership application with your dues may be submitted.
There is no charge to NYSCHP members. Non Members are required to submit a processing fee of $15 and most go to www.nyschp. org to pay the fee to gain access to the online quiz. In lieu of this fee, a completed membership application with your dues may be submitted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Materials presented in this article were made possible from the program funded by the Center for Disease Control and Prevention (CDC No. 1U38GD000070), “Pharmacogenomics Education Program: Bridging the Gap between Science and Practice” (PharmGenEd