
Abstract
Acute bronchitis is a disease characterized by inflammation of the large airways within the lung accompanied by a cough lasting from 1 to 3 weeks. The inflammation occurs as a result of an airway infection or environmental trigger, with viral infections accounting for an estimated 89% to 95% of cases. Symptomatic treatment of cough is primarily required for patients, though in most cases the condition is self-limiting. Therapy consists of both nonpharmacological and pharmacological options to include antibiotics and antivirals, antitussive agents, protussive agents, and beta-2-agonists. This article reviews the treatment options for acute bronchitis and recommends criteria for use.
Keywords
AB is a 75-year-old male presenting to the emergency department with a chief complaint of cough for 10 days with purulent sputum and shortness of breath. The patient has a past medical history of stabilized congestive heart failure without a history of pulmonary disease. Vital signs include a temperature of 99.1°F, respiratory rate of 20 breaths/min, and a heart rate of 91 beats/min. On auscultation of the lungs wheezing is present without rales. AB reports an allergy to azithromycin.
Introduction
Acute bronchitis is the fifth most common diagnosis for patients presenting with a primary symptom of cough lasting from 1 to 3 weeks.1,2 The disease is characterized by inflammation of the large airways within the lung accompanied by a cough without the presence of pneumonia as confirmed by the absence of an infiltrate on chest radiograph. 3 The cough may last for up to 3 weeks in about 50% of patients due to either an infectious or a noninfectious etiology. 4 No matter the etiology, the triggering factor leads to an inflammatory response within the epithelium of the bronchi causing mucus production and airway hyperresponsiveness.
There are an estimated 10 million office visits per year by patients seeking medical attention for acute bronchitis, leading to 10 ambulatory visits per 1000 people/year. 1 A large part of treatment costs are a consequence of patients receiving on average two prescriptions per visit and the disease resulting in 2 to 3 days of missed work. 5 Office visits for acute bronchitis result in a prescription for antimicrobial therapy in 70% to 90% of the cases, though most cases are due to a virus. 2
Pathogenesis
Acute bronchitis is an inflammation of the epithelium of the bronchi secondary to an airway infection or environmental trigger that clinically presents as a cough. 2 Viral infections account for an estimated 85% to 95% of acute bronchitis cases with bacterial causes being more common in patients with chronic health problems. 3 The most frequently isolated viruses include influenza A and B, parainfluenza, and respiratory syncytial virus, while coronavirus, adenovirus, and rhinovirus are encountered less commonly. Bacterial pathogens involved are those that cause community-acquired pneumonia such as Mycoplasma pneumonia, Streptococcus pneumonia, Haemophilus influenza, Moraxella catarrhalis, and Bordetella pertussis.
Diagnosis
The diagnosis of acute bronchitis is primarily clinical since there are no specific diagnostic criteria. It should be differentiated from asthma or bronchiolitis which presents as a progressively worsening cough along with wheezing, shortness of breath, and hypoxemia. 4 Many patients misdiagnosed with acute bronchitis are actually presenting with acute cough due to asthma exacerbation, the common cold, or acute exacerbation of chronic obstructive pulmonary disease (COPD). 1 A thorough assessment of the patient should be performed to rule out other causes of the cough including a physical examination, medication and social history, and tobacco use evaluation. Distinguishing acute bronchitis from a simple upper respiratory infection within the first few days of illness is difficult. However, cough greater than 7 days is suggestive of acute bronchitis. The cough in acute bronchitis usually lasts for 2 to 3 weeks, and airway hyperresponsiveness may last for 5 to 6 weeks. A different diagnosis should be considered for cough lasting greater than 3 weeks. Cough in the absence of fever, a respiratory rate less than 24 breaths/min, and a heart rate of less than 100 beats/min are suggestive of the diagnosis. 3
Healthy adults diagnosed with acute bronchitis are typically uncomplicated cases; though, patients with underlying lung disease (ie, COPD or bronchiectasis), congestive heart failure, or immune compromise are at high risk for complications. 1 The color of the sputum is not an accurate predictor in the differentiation between viral or bacterial etiologies, and in greater than 30% of patients the causative pathogen remains unidentified. Viral and bacterial cultures and serologic assays are not routinely performed for identification purposes. Patients with severe spastic cough should be evaluated for pertussis.
It is important to rule out other causes of cough with or without phlegm production, such as the common cold, reflux esophagitis, acute asthma, or COPD.1,4 Differentiating acute bronchitis from the common cold and acute exacerbation of chronic respiratory condition (ie, COPD, asthma) is challenging based upon the symptoms. The symptoms of the common cold (ie, nasal stuffiness and discharge, sneezing, sore throat, and cough) are shared by those of acute and chronic bronchitis. 3 Acute bronchitis patients typically present with symptoms of bronchial obstruction, wheezing, and dyspnea on exertion, as seen in asthma exacerbation. However, with acute bronchitis cough persists beyond the acute period of 5 to 7 days. Differential diagnoses for acute cough with or without phlegm are listed in Table 1.
Differential Diagnosis for Acute Cougha
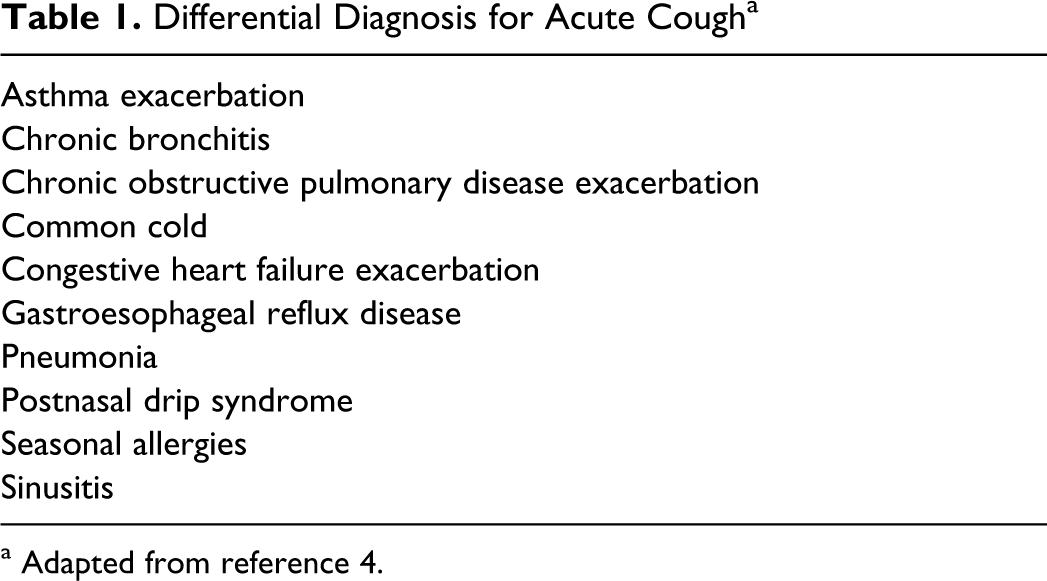
a Adapted from reference 4.
Treatment Options
Symptomatic treatment for cough is primarily required for patients presenting with acute bronchitis since the infection is likely viral in nature. Evidence does not consistently support treatment since acute bronchitis is a self-limiting condition. 6 Many patients will present with symptoms of the common cold and may benefit from treatment with acetaminophen, a nonsteroidal anti-inflammatory medication, or nasal decongestant.
The primary goal of treatment is reduction of symptoms, but improving patient function and quality of life are also important. Studies have shown that despite aggressive treatment of acute bronchitis many patients seen in the emergency department will have recurrent symptoms requiring hospitalization.1,2 Acute bronchitis therapy consists of both nonpharmacological and pharmacological therapies including antibiotics, antivirals, antitussives, protussives, and beta-2-agonists.
Nonpharmacological
Reasonable nonpharmacological treatment options include reduction of environmental cough triggers and vaporized treatments, especially in environments with low humidity. 2 Patients should be counseled to rest and increase their fluid intake, especially if a fever is present.
Antibiotics
On average, 70% to 90% of office visits for acute bronchitis result in the patient receiving a prescription for either an antiviral or an antimicrobial medication. 2 A study by Mainous et al of Medicaid claims data found that 75% of patients presenting with acute bronchitis were prescribed an antibiotic. 7 Antimicrobial therapy should be reserved for those cases where a pathogen is isolated or in high-risk patients presenting with symptoms of influenza infection during influenza season. 4
A majority of systematic reviews have found no benefit from using antibiotics with the exception of a modest reduction in duration of symptoms. 3 Routine antibiotic treatment has not been shown to have a consistent impact on the duration or severity of the illness or on the development of complications such as pneumonia. 8 A 2004 Cochrane review of 9 randomized trials found a statistically significant reduction in cough duration with antibiotic treatment but concluded that the risk of potential adverse effects offset the small benefit seen with antibiotic therapy. 9 A 2009 Cochrane review of 14 randomized trials concluded that patients receiving antibiotics (erythromycin, azithromycin, amoxicillin/clavulanate, doxycycline, trimethoprim-sulfamethoxazole, and cefuroxime) did have better outcomes than those receiving placebo. 10 Those receiving antibiotics had a reduction in days feeling ill and a reduction in days with limited activity, though there was no significant difference in presence of productive cough at follow-up or mean duration of cough. Arguments against using antibiotics in acute bronchitis include the cost, adverse effects, and changes in bacterial susceptibilities with only modest improvement in symptoms. Identifying the subgroup that will likely benefit from antibiotic use is difficult, with it being most important to rule out the presence of pneumonia when considering treatment. 7 Patients with symptoms of upper respiratory illness and those that have been sick for less than a week may be the least likely to benefit from therapy with an antibiotic. 10 Clinical trials have examined the use of elevated biomarkers, procalcitonin, and C-reactive protein in guiding antimicrobial therapy in patients with respiratory infections with limited implications for clinical application.11–13
Selection of antibiotics is based on activity against the common pathogens (Streptococcus pneumonia, Haemophilus influenza, and Moraxella catarrhalis) involved in acute bronchitis and the ability of the agent to penetrate into the sputum and bronchial mucosa. 14 Rarely is the causative pathogen isolated, occurring in only about 30% of cases. 4 The choice of antibiotic prescribed for the treatment of acute bronchitis has changed over time. Amoxicillin, doxycycline, erythromycin, and trimethoprim-sulfamethoxazole are commonly used for the treatment of acute bronchitis; however, due to increasing resistance, practitioners may prefer to use second-generation and third-generation cephalosporins or macrolides. If the infection is thought to be due to pertussis, the patient should be treated with a macrolide started as soon as possible to reduce transmission. Symptoms that are strongly suggestive of pertussis infection include recent exposure to a case of pertussis, whooping sound, or posttussive vomiting. 1 Treatment regimens for pertussis include erythromycin 500 mg 4 times daily for 14 days, clarithromycin 500 mg twice daily for 14 days, or azithromycin 500 mg on day 1 followed by 250 mg daily for 4 days. Antibiotics show the greatest clinical benefit when started early within the first week. Dosages for antibiotics commonly used in the treatment of acute bronchitis are listed in Table 2.
Antibioticsa
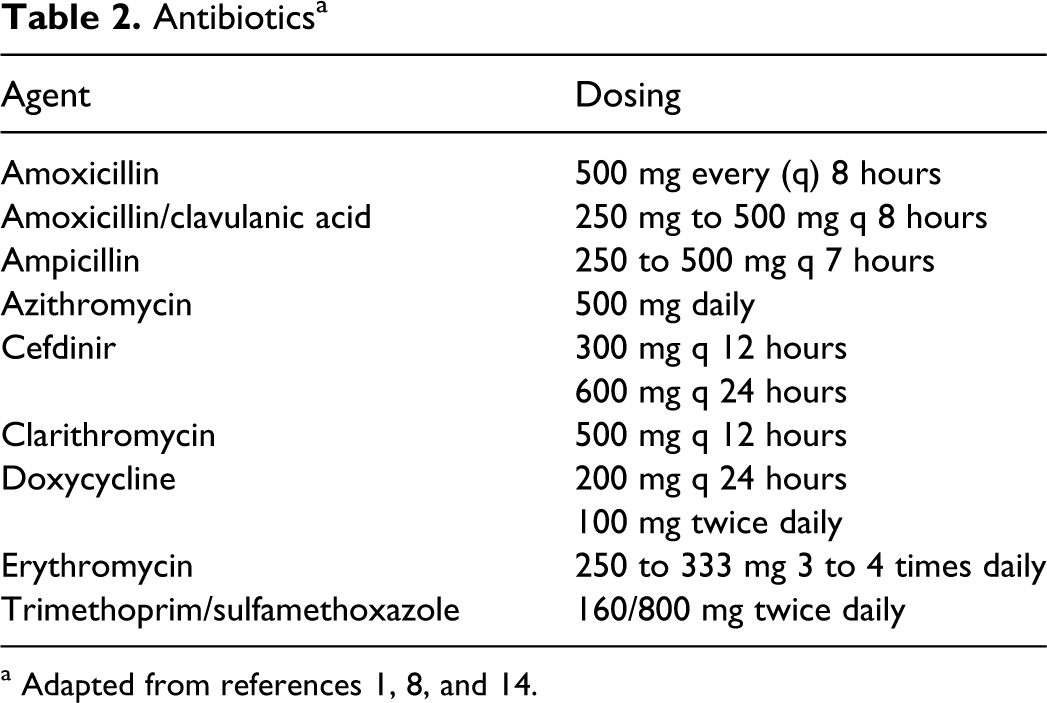
a Adapted from references 1, 8, and 14.
The optimal duration of antimicrobial therapy has not been determined in patients with acute bronchitis. European guidelines for patients with lower respiratory tract infection recommend maintaining treatment to an average of 7 to 10 days. 14 However, shortening the length of therapy has also been advocated as a way to prevent resistance. A meta-analysis performed by Falagas et al found that short-duration (5 days) antimicrobial treatment was associated with fewer adverse events and was as effective as longer duration of treatment. 15
Beta-2-Agonists
There have been 4 randomized, controlled trials examining the efficacy of beta-2-agonists in acute bronchitis.16–19 The effect of albuterol, specifically either oral or inhaled, on cough has been studied in 3 randomized trials.16–18 Hueston investigated the efficacy of albuterol as compared to erythromycin, both given as liquid preparations, in adults presenting with cough. 16 There were fewer patients in the albuterol group with productive cough at 7 days as compared to the erythromycin group (P < .001), but there was no difference in missed days of work or daily activities. The study was repeated using an albuterol inhaler with similar findings of reduced cough at 7 days (P = .02). 17 Littenberg et al conducted a study in 104 adults with cough of less than 4 weeks’ duration comparing albuterol 4 mg by mouth 3 times daily for 7 days to placebo. 18 The study found that there was no significant difference between patients receiving the albuterol as compared to placebo in measures of efficacy, and there were significantly more adverse effects in the treatment group. A study by Melbye et al compared inhaled fenoterol, a short-acting beta-2-agonist available outside of the United States, to placebo in 80 patients with acute bronchitis. 19 There was an observed improvement in symptom scores for those patients receiving fenoterol that presented with bronchial hyperresponsiveness, wheezes on auscultation, or a forced expiratory volume in 1 second less than 80% as compared to the same patient group with placebo. Patients with normal lung findings at the start of the study did not improve with treatment.
Patients presenting with acute bronchitis may have bronchospasm present and treatment with a bronchodilator would be effective. Studies have shown a decrease in cough and have observed patients returning to work earlier when treated with bronchodilators as compared to those treated with antibiotic therapy.16,17 There is consistent data to support the use of beta-2-agonist therapy in decreasing the duration of cough in those patients with troublesome cough and airway hyperresponsiveness.16–19 Additionally, patients with airflow obstruction at baseline and wheezing may benefit from beta-2-agonist therapy.16–20 A Cochrane review of beta-2-agonists in acute bronchitis concluded that there may be a reduction in symptoms, such as cough, in those with evidence of airflow obstruction. 20 Common adverse effects associated with the use of beta-2-agonists include tremor, nervousness, and shakiness.
Antitussive and Protussive Therapy
Therapy for the cough associated with acute bronchitis may target controlling the cough (antitussive) or increasing secretions (protussive). 1 The American College of Chest Physicians recommend a short course of antitussive therapy to reduce severe coughing during acute illness (such as hydrocodone, codeine, or dextromethorphan) though there is a lack of consistent evidence showing the benefit. There have been no double-blind placebo-controlled studies examining the use of codeine on cough with acute bronchitis, and results of clinical trials with dextromethorphan are conflicting. Antitussive therapy is recommended in those patients with a cough causing discomfort where inhibition of airway secretion clearance will not delay healing. 21 Patients presenting with a persistent mild cough may benefit from dextromethorphan while severe cough may require therapy with codeine or codeine derivative. The efficacy of antitussive therapy depends on the cause of the cough. Cough due to viral respiratory tract infections has not been shown to respond to antitussive therapy, but chronic cough has been shown to improve with antitussive therapy. 2 The tendency of these agents to dry bronchial secretions may aggravate the cough and prolong recovery. Antitussive agents and their dosages are listed in Table 3.
Antitussive Agentsa

a Adopted from reference 22.
Protussive therapy would be indicated in patients requiring clearance of airway secretions. The clinical effectiveness of this type of therapy is questionable, and therapeutic trials have failed to show favorable effects on the cough associated with acute bronchitis. 1 Physicians commonly prescribe guaifenesin in dosages of 600 to 1200 mg as protussive therapy for cough, and it is a component in many over-the-counter antitussive therapies.
Pharmacist’s Role
The pharmacist, as a part of the health care team, can assist in improving outcomes by optimizing the treatment in patients diagnosed with acute bronchitis. Appropriate selection and dosing of antibiotic therapy may be guided by the pharmacist as well as selection of supportive therapies for cough as outlined in Table 4. Pharmacists may also play a role in reducing the unnecessary use of antibiotic agents in treating acute bronchitis and identifying those populations that may benefit from therapy. Patients either seen in the emergency room or admitted to the hospital require counseling for appropriate use of nebulizer or metered dose inhaler prior to discharge to ensure optimal therapy. Pharmacists can counsel on appropriate use, adverse effects, and anticipated outcomes with pharmacotherapy. Finally, for those patients that are admitted to the hospital, the pharmacist is able to recommend transition from intravenous to oral therapies.
Criteria for Use of Selected Pharmacologic Agents in Acute Bronchitis
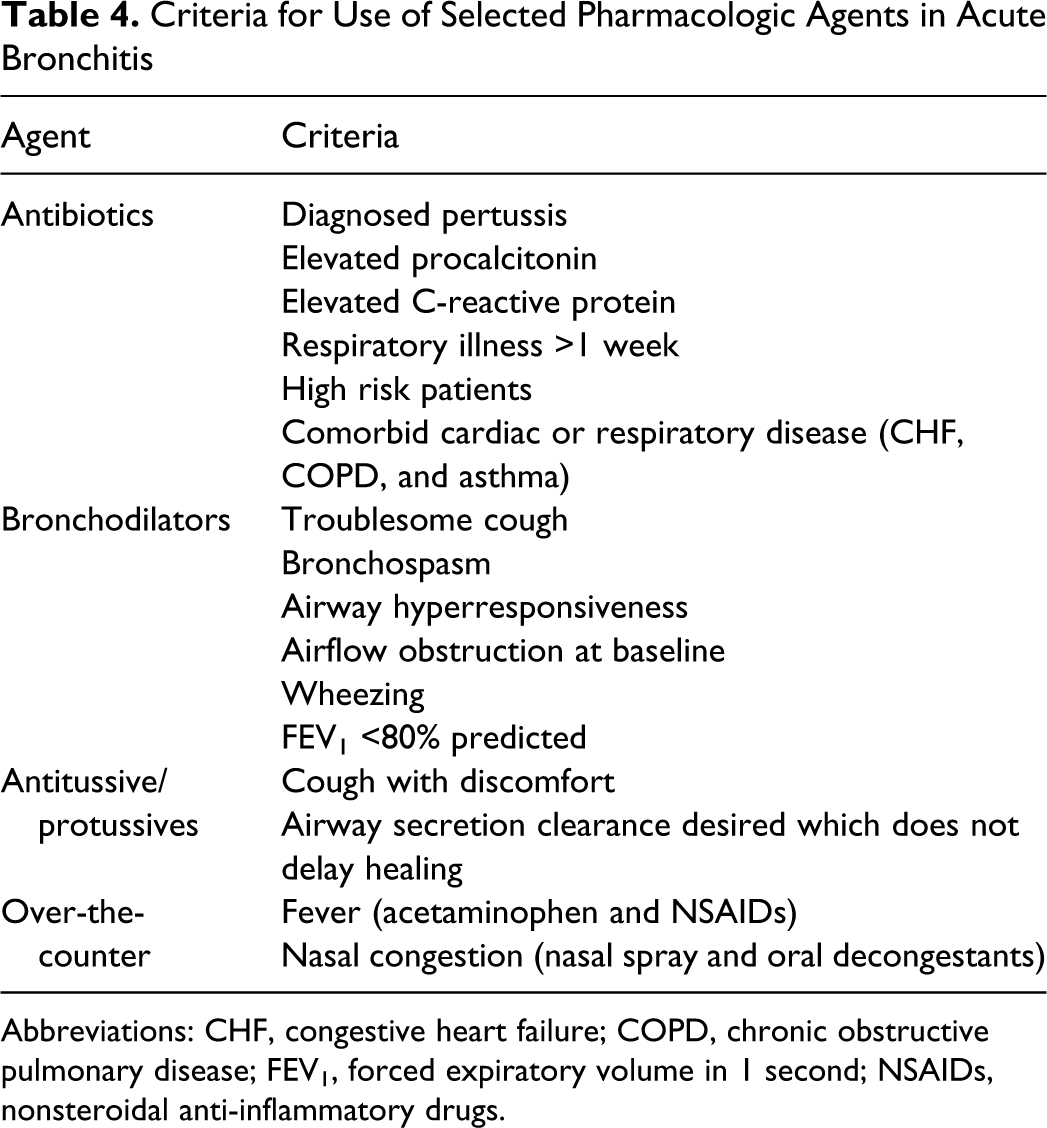
Abbreviations: CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; NSAIDs, nonsteroidal anti-inflammatory drugs.
Patient Case
Given AB’s age, presentation, history of cardiac disease, and duration of cough, he would be eligible for treatment with antibiotics and other supportive therapies. Since a previous allergy to azithromycin is noted, a preferred agent would be a third-generation cephalosporin, doxycycline, or amoxicillin/clavulanic acid. AB will also likely benefit from a protussive agent due to his phlegm production and bronchodilator since wheezing is present.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.