
Abstract
Objectives:
The aim was to compare nursing staff compliance over the years, per health care unit, and per drug use process step.
Methods:
Compliance assessment was performed by nursing consultants with direct observation of the registered nurses and nursing assistants during the performance of 7 steps of the drug use process. A total of 36 compliance criteria were developed. The compliance to drug use process criteria was measured in 2007 (Prephase), 2008 (post 1), and 2011 (post 2). Totally, 10 health care units were evaluated, with a minimum of 10 doses evaluated per health care unit, including a minimum of 5 parental doses and a total of 100 nurses observed.
Results:
A total of 142 nurses were observed in the prephase, 140 nurses in the post 1 phase, and 98 in the post 2 phase (90% regular staff and 10% float staff). The overall compliance rates went from 77% in 2007 up to 87% in 2008 and down to 78% in 2011.
Conclusions:
This cross-sectional observational study revealed a significant difference in the drug use process compliance in terms of drug preparation and drug administration for inpatients at the bedside, between 2007 and 2011.
Introduction
In Canada, 54 steps make up the hospital drug use process, as defined by the Ministère de la santé et des services sociaux du Québec (eg, purchase, storage, labeling, management of expired drugs, etc). 1 This complex process is organized according to the federal 2 and provincial laws, 3 accreditation standards, 4 required organizational practices, 5 regulatory authority statements and guidelines, 6 and other positions from the professional associations and independent organizations. 7 This normative framework has been adopted in order to offer a safe health care environment to patients and health care workers. However, such a complex framework of standards presents a challenge for health care workers in terms of day-to-day compliance. Indeed, it is difficult to ensure that standards are regularly performed by health care workers when technologies, drugs, and policies and procedures are continuously updated. This complex framework of standards is a big challenge for health care workers, and barriers to compliance include lack of communication, skepticism, and disagreement toward the standards, lack of supplies and equipments, and lack of motivation. 8 Some guidelines were written in order to help health care workers to adhere to new standards. 9 In the course of our preparation for an accreditation visit to our center, a 500-bed mother–child teaching hospital, a pre-post observational study was conducted from 2007 to 2008 to evaluate the compliance with the drug use process at the bedside. 10 Three years later, the same study was repeated to see whether any progress was made.
Methods
This cross-sectional prospective observational study was conducted at the Sainte-Justine University Hospital Center.” The aim was to compare the nursing staff compliance over the years, per health care unit, and per drug use process step. Outpatient activities were excluded. A total of 36 compliance criteria were developed using the self-evaluation compliance tool that the Ministère de la santé et des services sociaux published in 2005 for the Quebec drug use process. 11 The health care units evaluated are described in Table 1 and the criteria are described in detail in Table 2. Seven steps of the drug use process were evaluated: planning, preparation, labeling, administration, verification, registration, and waste management. The compliance of these 36 criteria was measured, respectively, in 2007 (prephase) and 2008 (post 1). Following the 2007 compliance measurements, a hospital-wide intervention was implemented to increase compliance. The interventions were chosen based on the key issues that were identified following the 2007 compliance measurements. 10 Interventions included Web pharmacy notes, nursing assistant/chief-unit reminders to nursing staff, face-to-face coaching with nursing staff by nurse educators for nonconformities identified, and so on. These interventions were implemented in 2007 and reinforced until 2011. Another measurement was conducted in 2011 (post 2) and compared to these two previous measurements (pre and post 1).
Overall Compliance Rates With the Drug Use Process per Health Care Unit per Year
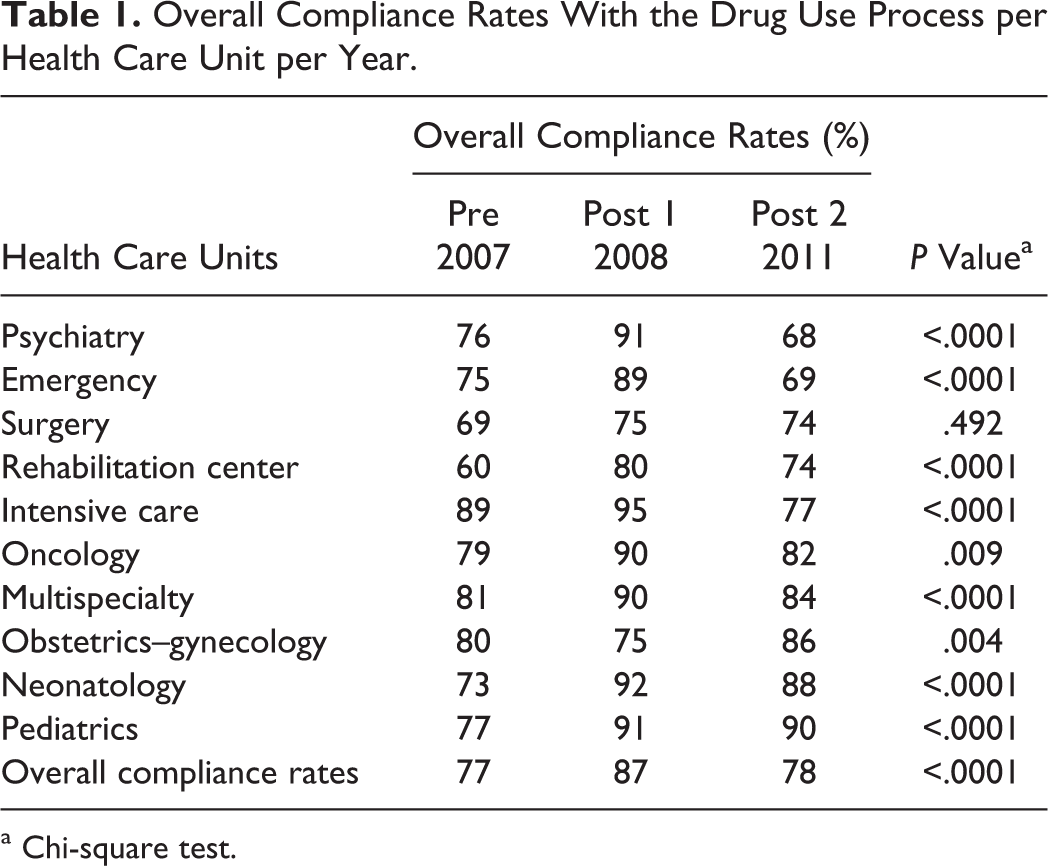
a Chi-square test.
Compliance Rate With the Drug Use Process per Criterion per Year

Abbreviations: N/A, nonapplicable (no observations were made); MAR, medication administration record.
a (N) values refer to applicable direct observations realized.
b Chi-square test.
Compliance assessment was performed by the nurse educators with direct observation of the registered nurses and nursing assistants. Nurses were chosen for observation if they were present at the time a specific health care unit was being evaluated. All nurses volunteered to participate in this evaluation. Different nurses were evaluated over time. Observations were carried out between March 11, 2011, and April 11, 2011, by 6 nurse educators. The 36 criteria and the form were explained to each of the observers by our research assistant using the same method in pre- /post 1 phase to ensure uniformity and common understanding of the rules. Nurses were aware that they were being observed. Observers had to specify whether the criterion was compliant (C), noncompliant (NC), or not applicable (NA) for each drug observation.
A convenience sample was used. No sample size calculations were performed for statistical purposes. We assessed the compliance in 10 health care units (pediatrics, neonatology, psychiatry, emergency, multispecialty clienteles, intermediate care and pediatric intensive care, obstetrics–gynecology, surgery, hemato-oncology, and rehabilitation) for a minimum of 10 doses per health care unit, including a minimum of 5 parental doses and a total of 100 nurses were observed. The units to be observed were chosen to represent the main units from the hospital.
The data were entered using a spreadsheet (Microsoft Excel® and Microsoft Access®, Portland, Oregon) and statistical analysis was performed with SPSS, 15.0, Chicago, Illinios. The compliance rates were calculated for each criterion per year and globally. Differences in the compliance rate were calculated using a chi-square test. A P value below .05 was considered significant.
Results
The study of post 2 phase was conducted in 2011 (n = 98 nurses observed, 90% regular staff and 10% float staff). The prephase was conducted in 2007 (n = 142 nurses observed) and the post 1 phase was conducted in 2008 (n = 140 nurses observed). Table 1 provides the overall compliance rates per health care unit, per year. Overall compliance rates were 77% in 2007, 87% in 2008, and 78% in 2011. In 2011, lower compliance rates were observed in 3 health care units that had no decentralized pharmacists on a regular basis (psychiatry, surgery, and emergency).
Table 2 provides the compliance rates with the drug use process per criterion per year. The compliance rates were below 80% for 17 (39%) of the 36 criteria in 2011, for 12 (33%) of the 36 criteria in 2008, and for 18 (47%) of the 36 criteria in 2007. In 2011, criteria with poor compliance (<50%) included the presence of the room number (37%), route of administration on handwritten labels (33%), date/hour of installation of continuous infusion on handwritten labels (20%), pills not in bags or crushed/cut in the ward pharmacy are properly identified on the label (patient name, room number, name of medication; 33%), bringing the Medication administration record (MAR) to the bedside (40%), allergy check with patients’ bracelet at bedside (46%), and the presence of date/hour of installation on tubing (25%). The compliance rate of 6 criteria differed significantly between 2007 and 2011, with a decrease in compliance rates for 2 criteria and an increase in compliance rates for 2 criteria. From 2008 to 2011, a significant decrease was observed for the 13 criteria.
Discussion
The cross-sectional observational study shows that compliance with the drug use process for inpatients at the bedside was reduced between 2008 and 2011 for the majority of the criteria. Although the overall compliance significantly increased after the first structured intervention in 2008 (post 1 phase), the overall compliance was reduced to prephase status and compliance was reduced for 12 of the 36 criteria in 2011. Ultimately, since the overall compliance rate is of 78% in 2011, there is still a 22% overall compliance gap for all patient health care units audited in our hospital.
Patient safety is certainly a high priority goal in the health care sector and all stakeholders support legislative and normative actions aimed at reducing medication errors. At the same time, the scientific literature is very mixed regarding the impact of accreditation standards and norms and their impact on patient safety. For instance, Miller et al conducted a systematic review of epidemiology and evidence supporting reduction strategy recommendations for medication errors in pediatric care. 12 Among the 26 approaches recommended to reduce medication errors in pediatrics, only 6 approaches relied on study results, while all the other approaches were solely based on expert opinions. Our compliance criteria have been designed using normative standards in order to improve the compliance with our drug use process. Are we working toward the right targets? Are persistent noncompliant results a good surrogate marker of recurrent risks within our institution? These results and questions led to reflection on the pharmacy-nursing committee, following discussion of the results.
Lower compliance rates were observed in particular for nonoptimal identification, labeling, and documentation of patients, drugs, and reports. In a local retrospective study, we described all medication errors declared in our hospital from 2004 to 2010. Out of a total of 11 731 medication errors reported, 66% were related to drug administration, 9% to documentation and transcription, and 25% to other factors. 13 Although this study confirms that drug use process at the bedside is the right target for audits of compliance with the drug use process, it is difficult to establish a link between current noncompliance and declared medication errors. For instance, not bringing the MAR to the patient’s bedside may explain omitted drug doses (29% of the medication errors), inappropriate/incorrect drug dose schedules (14%), wrong infusion rates (12%), wrong doses (11%), or wrong drug concentrations (6%). Unit dose packs torn in the ward pharmacy rather than at the bedside may explain wrongly administered doses (12%) or expired doses given to a patient (4%). Further studies are required to identify optimal approaches to teach best practices in the clinical settings.
Through a nonstructured discussion, we were able to list at least 5 key factors that may explain the residual noncompliance of the 7 steps of our local drug use process. (1) Since an emerging number of norms apply to the drug use process, decision makers, team leaders, and health care workers are overwhelmed by the amount of information. Faced with the huge number of criteria that must be met, the average health care worker is unable, on a day-to-day basis, to consider hundreds of compliance criteria. For instance, in Quebec, we were able to point out 5 different key standards published from 2008 until now that account for at least 400 criteria (eg, Drug Sterile Compounding—Chapter 797 of the United States Pharmacopeia, 2008, 14 Prevention Guide for the Manipulation of Hazardous Drugs of the Association paritaire pour la santé et la sécurité du travail du secteur affaires sociales (ASSTSAS), 2008, 15 Medication Management Standards of Accreditation Canada, 2008, 4 Standards de pratique en pharmacie of the Ordre des pharmaciens du Québec, 2010, 6 and Medication Management Standards of the Agence de santé de Montréal, 20101). This number of standards is difficult to manage and audit prospectively in a large institution. It is also a challenge for the management staff to integrate all theses norms into a coherent strategic planning process. (2) With some standards there is a lack of clarity and assessability. Unclear statements can be difficult to implement and evaluate. For instance, Jordane et al evaluated at 90% the clarity and at 76% the assessability of the 2008 version of Accreditation Canada’s Medication Management Norms. The clarity and assessability were pivotal in the drafting of our 36 specific criteria for the drug use process. 16 (3) Detailed and explicit standards can artificially delineate tasks. Although this delineation may contribute to a better description and ability to evaluate certain aspects of a task, it may complicate the knowledge transfer process. For instance, Accreditation Canada’s Medication Management Norms have distinct criteria for double patient identifiers, systematic allergy checks, in-time documentation on MARs for administered doses, and so on. These criteria are not included in a single “optimal drug administration” section of the drug use process. Knowledge transfer can be optimized by limiting the overlap of normative sources and pairing similar criteria and chronological processes. (4) Some norms may not be perceived as very meaningful to clinicians and treated as irrelevant or not a priority, which can change the current practices. For instance, an increased knowledge and perception of the causes of medication errors can have an impact on the nursing practices. 17,18 (5) Health care workers are no different from other people and are often resistant to change. Although it is acknowledged that it is sometimes better to use “disruptive change approaches” to effectively change a process, such approaches are often not realistic in the complex health care processes. 19 Grigg et al recognize that medication administration is an increasingly complex process that requires adaptability in the part of nurses. 20 This study has reinforced the importance of redefining drug use process priorities in our hospital given sustained noncompliance. Following a 2011 accreditation visit to our institution, we developed a consolidated Web platform to integrate all applicable standards into the drug use process, pairing similar criteria and displaying a concatenated version of all of them. This tool, combined with our pharmacy-nursing and drug use process committee consultations, will help to identify key priority actions to improve our local drug use process.
This study has a number of limitations. Its cross-sectional design represented a limited number of observations (between 98 and 142 nurses) at 3 points in time. However, directobservation is time consuming and cannot be repeated easily. A smaller number of nurses were observed in the post 2 phase due to time constraints. Although direct observation was limited to 1 (post 2 phase) or 2 observers (prephase and post 1 phases), there was no second validation of the observations documented by the observer/observers. Nurses were aware that they were being observed.
Conclusion
This cross-sectional observational study revealed a significant difference on the drug use process compliance in terms of drug preparation and drug administration for inpatients at the bedside between 2007 and 2011. The overall compliance rate improved from 77% in 2007 to 87% in 2008, but the compliance decreased to 78% in 2011. Although the overall compliance significantly increased after the first structured intervention in 2008 (ie, from 77% to 87%), the overall compliance decreased to 78% in 2011. Ultimately, there is still a 22% overall compliance gap for all patient health care units audited in our hospital in 2011.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.