
Abstract
Acute coronary syndrome (ACS) is a devastating adverse cardiovascular event with a massive burden on patient morbility and mortality, as well as the economy. Approximately 1.2 million people are hospitalized annually for ACS in the United States, with direct medical costs estimated at $150 billion in 2009. Rehospitalization is common, often as the result of recurrence of the initial event or complications of ACS or its therapy. Thrombosis is central to the pathogenesis of ACS. The current standard of care includes dual antiplatelet therapy, which reduces platelet activation and aggregation, integral steps for forming a thrombus. However, antiplatelet therapy does not prevent continued thrombin generation or the deposition of fibrin in the clot and residual risk of a recurrent event remains high. New oral anticoagulants offer a mechanism of action that is different from and complementary to that of antiplatelet agents. The ATLAS ACS-TIMI 51 (Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome–Thrombolysis in Myocardial Infarction 51) trial, using rivaroxaban, is the first trial of the new oral anticoagulants to show a benefit when added to antiplatelet therapy in reducing ACS events and mortality. While there was more major bleeding with the addition of rivaroxaban, fatal bleeding was not increased. These agents, if added to the current standard of care, might substantially reduce the high clinical and economic consequences of ACS.
Continuing Education Learning Objectives
By the end of the article, the reader should be able to:
Describe the burden of acute coronary syndrome (ACS). Explain the processes of hemostasis and thrombosis in the context of ACS. Identify the limitations of current antiplatelet and anticoagulant therapy in ACS. Compare and contrast the pharmacokinetics and pharmacodynamics of novel anticoagulants. Discuss the limitations of warfarin for ACS. Compare and contrast the variable clinical results of anticoagulants in ACS. Identify potential barriers for implementation of triple antithrombotic therapy.
Introduction
In the United States, acute coronary syndrome (ACS) is highly prevalent and has important clinical and economic consequences. In 2009, the number of discharges with a diagnosis of ACS from US hospitals was approximately 1.2 million. 1 Of these, it is estimated that 785 000 were new adverse cardiovascular events and 470 000 were recurrent events. 1 The negative impact of ACS on patient morbidity and mortality is extremely high. Specifically, among patients ≥65 years of age, 25% of men and 30% of women will die within 1 year of experiencing a first myocardial infarction (MI). 1 Also, those who survive a first acute event at any age have a chance of a recurrent event or death 1.5 to 15 times higher than that of the general population. 1
Acute coronary syndrome costs the American health care system more than $150 billion annually, with approximately 60% of these costs related to rehospitalization. 2 Furthermore, approximately 20% of the ACS patients are rehospitalized within 1 year of the initial event. From 21% to 33% of ACS patients have at least 1 rehospitalization for ACS, with mean charges in one study of $52 000. 3,4 In another study, in which 13 731 patients with ACS were followed for a mean of 9.75 months, total health care costs were $309 million or $22 529 per patient, with 71% of those costs attributable to hospitalizations. 5 Clearly, any treatment strategy with the potential to reduce the economic burden of hospitalizations related to ACS would be highly valued.
Pathogenesis of Artherothrombosis
The 3 clinical manifestations of ACS, based on the presence or absence of ST-elevation on the electrocardiogram and elevation of myocardial biomarkers, are ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI), and unstable angina (UA). While manifesting differently, the 3 forms of ACS share a common pathophysiology, with atherosclerotic plaque rupture and thrombosis central to the pathogenesis of all. Although the formation of atherosclerotic plaques within the arteries begins early in life, in later years, cardiovascular (CV) risk factors such as older age, hypertension, dyslipidemia, smoking, diabetes, and certain genetic profiles accelerate plaque formation. Some plaques may remain stable, but “vulnerable” plaques are weak and subject to rupture as the result of vascular injury. 6 After atherosclerotic plaque rupture, platelets adhere to the site of vascular injury through binding to collagen and von Willebrand factor. Platelet agonists such as thrombin, collagen, adenosine diphosphate (ADP), and thromboxane A2 contribute to platelet activation, which produces platelet shape change, release of agonist containing granules, and ultimately activation of glycoprotein IIb/IIIa receptors. As fibrinogen selectively binds to the activated glycoprotein IIb/IIIa receptors, platelets are linked together, aggregate, and form a platelet plug in the area of injury. This occlusion in the artery is then stabilized by the conversion of fibrinogen to fibrin and grows within the incorporation of the platelet-fibrin meshwork, which prevents further blood flow to ischemic myocardium. 7 -11 Patients with UA and NSTEMI typically have an acute coronary occlusion that partially blocks the coronary vessel and results in a critical decrease in myocardial oxygen supply. Patients presenting with STEMI, on the other hand, typically have complete occlusion of coronary vessels and require immediate reperfusion therapy to restore myocardial blood flow to the ischemia area. 10,11
The coagulation cascade, a series of linked enzyme reactions wherein proteins are activated, also plays an important role in the development of coronary thrombosis. 7 -11 Initiation of the coagulation cascade can be triggered by tissue factor in the extrinsic pathway or by surface activation space via the intrinsic pathway. Both pathways lead to the common pathway beginning with the activation of factor X, which ultimately directs the generation of thrombin, the major component of the clotting cascade. Once small amounts of thrombin are initially produced, thrombin then activates a number of positive feedback loops to significantly increase its own production. 8,9 Thrombin increases the activation of factor VII, which combines with factor IXa and calcium on the surface of platelets forming the tenase complex. This complex is responsible for the activation of large amounts of factor X. Thrombin also increases the activation of factor V, which combines with factor Xa and calcium on the surface of platelets forming the prothrombinase complex. This complex is responsible for the activation of large amounts of thrombin, which is commonly referred to as the thrombin burst. Thrombin is then responsible for converting fibrinogen into stable fibrin in the thrombotic occlusion. 10,11 The fibrin clot is further strengthened by factor XIIIa, which is also activated by thrombin. Additionally, thrombin is also considered to be the most potent activator of platelets, which leads to platelet shape change, release of activator rich granules, expression and activation of glycoprotein IIb/IIIa receptors, and ultimately platelet aggregation. 8-11
Antithrombotic Acute and Long-Term Treatment
Once hospitalized, patients with ACS are managed with a combination of anti-ischemic therapies, antiplatelet agents, anticoagulants, fibrinolysis, or revascularization with percutaneous coronary intervention (with or without stent placement) or coronary artery bypass grafting (CABG) surgery. Antiplatelet agents may include aspirin, glycoprotein IIb/IIIa inhibitors including abciximab, eptifibatide, or tirofiban, and P2Y12 receptor inhibitors such as clopidogrel, prasugrel, or ticagrelor. Despite this treatment, however, procoagulant factors continue to exert effects for long periods of time after ACS patients have been clinically stabilized, so long-term or life-long antithrombotic therapy may be required to prevent recurrent events. 12,13 Postdischarge therapy for patients with an ACS event usually includes the combination of anti-ischemic and multiple antiplatelet medications but does not include any long-term anticoagulant medications.
Due to the critical role of platelets in the creation of arterial thrombosis, acute and chronic antiplatelet therapy is considered standard of care for patients with ACS events. Aspirin inhibits platelet activation by inhibiting the cyclooxygenase enzymes and thromboxane A2 synthesis, whereas the P2Y12 receptor antagonists prevent ADP from stimulating the P2Y12 platelet receptor and subsequent signaling. 9 By reducing platelet activation and aggregation, these agents have been so successful in reducing the incidence of recurrent ACS events 14 –17 that they are recommended in published guidelines for all patients with ACS, regardless of clinical manifestation and whether they were initially treated medically or invasively. 18 –20 Currently, the most commonly used P2Y12 receptor inhibitor is clopidogrel, but prasugrel and ticagrelor are also approved by the US Food and Drug Administration (FDA) and contribute to market share. 16,17 Per published recommendations, treatment with dual antiplatelet therapy (aspirin and a P2Y12 inhibitor) following an ACS event usually continues for up to 1 year following hospital discharge, and aspirin is often administered for life. 18 –20
Although P2Y12 receptor inhibitors are effective following ACS, limitations exist for clopidogrel and the other approved medications. Clopidogrel, a thienopyridine, is plagued by a high level of interindividual variability in antiplatelet response due to variable absorption and conversion from prodrug to its active metabolite. In particular, genetic variation in the cytochrome P450 (CYP) 2C19 enzyme explains a portion of the pharmacokinetic and pharmacodynamic variability of clopidogrel as this enzyme is able to metabolize clopidogrel to its active metabolite. 21,22 The third generation thienopyridine prasugrel produces more consistent platelet inhibition compared to clopidogrel, but as a consequence, is associated with an increased risk of bleeding, including fatal bleeding.16 The higher risk of bleeding has been predominantly associated with specific patient groups. To help mitigate the increased risk, prasugrel is contraindicated in patients with a history of transient ischemic attack or stroke and has a precaution for use in patients aged ≥75 years or who weigh less than 60 kg (FDA label). Similarly with ticagrelor, general caution is warranted if treating patients at high risk for bleeding. In addition to the higher bleeding rate demonstrated in clinical trials,17 ticagrelor also requires twice a day dosing, which negatively impacts pill burden for the patient and also potentially adherence. In addition to these issues, the efficacy of ticagrelor in the patients treated in the United States in its major Phase III clinical trial has been questioned due to the results of a regional subgroup analysis. 23 Due to these complicating and distinctive features, selecting the optimal P2Y12 receptor antagonist is difficult, and the best agent for preventing adverse cardiovascular events and balancing bleeding risk is oftentimes not clear for individual patients before and during treatment.
The most important limitation of dual antiplatelet therapy is that patients treated with recommended medications remain at high risk for recurrent events, regardless of the selection of agent. Specifically, in the most recent Phase III clinical trials, subjects treated with clopidogrel, prasugrel, or ticagrelor had a recurrent event rate of 10 to 12% in the 6 to 15 months following initiation of dual antiplatelet therapy with aspirin and any of the P2Y12 receptor antagonists. 16,17
Therefore, one explanation for the incomplete effectiveness of antiplatelet medications for preventing recurrent events is that thrombin remains uninhibited and may continue to activate platelets and precipitate ACS events despite multiple mechanisms of platelet inhibition. 24,25 Although dual antiplatelet therapy has greatly reduced ischemic outcomes compared to placebo and aspirin, there remains an unacceptably high residual recurrence rate of approximately 10% per year, even in patients receiving the newer and more potent antiplatelet agents. 14 –17 Moreover, increasing doses of antiplatelet agents does not appear to increase efficacy. In the CURRENT-OASIS 7 trial (Clopidogrel and Aspirin Optimal Dose Usage to Reduce Recurrent Events—Seventh Organization to Assess Strategies in Ischemic Syndromes), increasing the dose of aspirin to 300 to 325 mg/d did not improve the efficacy compared with doses of 75 to 100 mg/d, whereas doubling the dose of clopidogrel for the first 7 days of treatment failed to improve efficacy but did increase major bleeding events (P = .01). 26 Consequently, the need remains for a more efficacious long-term antithrombotic therapy for ACS that does not at the same time pose unacceptable bleeding risks to patients.
Anticoagulation in ACS Treatment
Based on the current pathophysiologic understanding of platelets in ACS, effective anticoagulant therapy should inhibit thrombin generation or the action of thrombin on platelets. Although patients are treated with both anticoagulant and antiplatelet therapy during the acute phase of an ACS event, anticoagulant therapy is discontinued once they have been stabilized, whereas dual antiplatelet therapy is continued for up to 12 months and aspirin often for life. 18 –20 While aspirin and P2Y12 receptor inhibitors act on the thromboxane A2 and ADP pathways, respectively, they do not prevent continued thrombin generation after the initial ACS event. 27 Thus, there may still be room for improvement in reducing ischemic outcomes by a separate mechanism. There has been increasing interest in adding an anticoagulant to antiplatelet therapy with a P2Y12 receptor inhibitor plus aspirin. Potentially, when added to the current standard of care, an anticoagulant agent that acts on the thrombin pathway could offer a more comprehensive approach to intervention in the thrombosis process than is provided by the use of antiplatelets alone.
Most anticoagulant agents used in the treatment of ACS are available only as injectable formulations and, therefore, are not optimal for long-term use. On the other hand, warfarin is an orally administered anticoagulant that targets formation of several proteins in the coagulation cascade and has been studied for ACS. In one trial, the use of warfarin in combination with aspirin therapy in patients with ACS did achieve a significant reduction in ischemic events compared with aspirin alone (10.5% vs 27%; P = .004). 28 In other trials, however, this combination of aspirin and full-dose warfarin did not improve outcomes but did increase bleeding events, tempering initial enthusiasm for this approach. 29,30
The potential role of warfarin in ACS has been further studied and evaluated by meta-analyses. For instance, a meta-analysis of 10 randomized trials (n = 5938) evaluating the addition of warfarin to aspirin after an ACS event with a target international normalized ratio (INR) greater than 2.0 has been conducted. 31 The addition of warfarin to aspirin significantly reduced the rate of MI [0.56 (95% confidence interval (CI) 0.48 – 0.69)] and ischemic stroke [0.46 (95% CI 0.27 – 0.77)] compared to aspirin alone. However, the addition of warfarin to aspirin provided no reduction in the risk of death [0.96 (95% CI 0.77 – 1.20)]. Furthermore, the nonmortality benefits were offset by an almost 2.5 fold increase in the risk of major bleeding (95% CI 1.7 – 3.7) and a 2.6 fold increase in minor bleeding (95% CI 2.0 – 3.3). One limitation of this particular meta-analysis is that 2 of the 10 studies made up about 75% of the total patients. 31
A separate and larger meta-analysis identified 14 trials (n = 25,307) comparing warfarin and aspirin to aspirin alone after an ACS event. 32 This meta-analysis included trials regardless of the target INR. The primary outcome of all-cause death, MI, or thrombotic stroke was not significantly reduced with the addition of warfarin to aspirin [odds ratio (OR) 0.96, 95% CI 0.90 – 1.03), but major bleeding was increased (OR 1.77, 95% CI 1.47 – 2.13). The authors then conducted a “restricted” analysis that included only trials with a target INR of 2.0 to 3.0, which was only about 30% of their initial number of patients (n = 7836). In this separate analysis, the primary outcome was significantly reduced by the use of warfarin and aspirin (OR 0.73, 95% CI 0.63 – 0.84) compared to aspirin alone, but the effect on the increase in major bleeding was more prominent (OR 2.32, 95% CI 1.63 – 3.29). 32 It is important to note, that all of the studies in both of these meta-analysis were conducted before the use of P2Y12 receptor inhibitors. Therefore, these studies have evaluated the combination of warfarin to aspirin, but not warfarin added to dual antiplatelet therapy.
Because of this heightened bleeding risk, warfarin is reserved in guidelines for NSTE ACS either as monotherapy for patients who are intolerant of aspirin or clopidogrel or for patients who have an alternative indication, such as atrial fibrillation, left ventricular thrombus, or cerebral, venous, or pulmonary emboli. 18 Patients who receive warfarin with dual antiplatelet therapy require frequent international normalized ratio monitoring to ensure that they are maintained at the lower end of the therapeutic range because bleeding risk is even higher with three antithrombotic agents. 18
New Oral Anticoagulants
Thrombin is the one of the most potent stimuli for platelet activation, but the thrombin-mediated platelet activation pathway is not directly or potently affected by current antiplatelet therapy. 8 –10 New oral anticoagulants have been developed to complement the antithrombotic effects of the antiplatelet agents. By intervening in the coagulation cascade to directly inhibit thrombin, these new oral anticoagulants may provide an additional mechanism of efficacy (Figure 1). 8,9
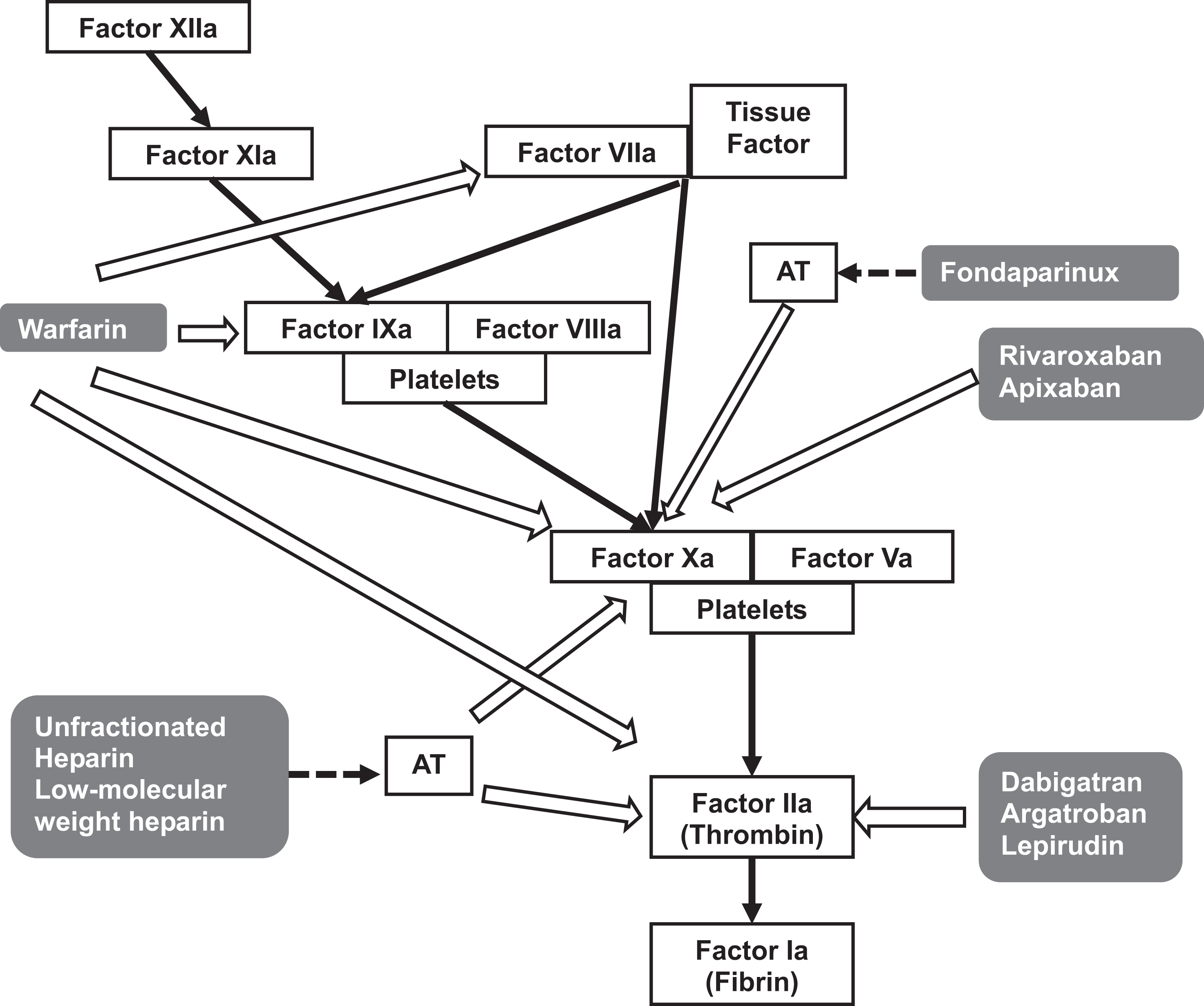
Targets of anticoagulant drugs. AT indicates antithrombin.
The new oral anticoagulants offer a number of advantages over warfarin. While warfarin typically requires 4 to 7 days to achieve adequate anticoagulation, the new agents share a rapid onset of action of about 2 to 4 hours. 33,34 The new oral anticoagulants also lack the many drug–food interactions that characterize warfarin and have less drug–drug interactions. Finally, they have a predictable anticoagulation response, so the routine and expensive coagulation monitoring required with warfarin is unnecessary. 33 –35 This predictable anticoagulant response also allows for fixed doses, which make them simple and attractive for outpatient use. Alternatively, one limitation of all of the new oral anticoagulants compared to warfarin is the lack of a reversal agent. Table 1 compares the pharmacokinetic and pharmacodynamic properties of these newer agents. Table 2 shows the key clinical trials for the new oral anticoagulants discussed below. 36 –41
Pharmacokinetics and pharmacodynamics of the newer oral anticoagulants.
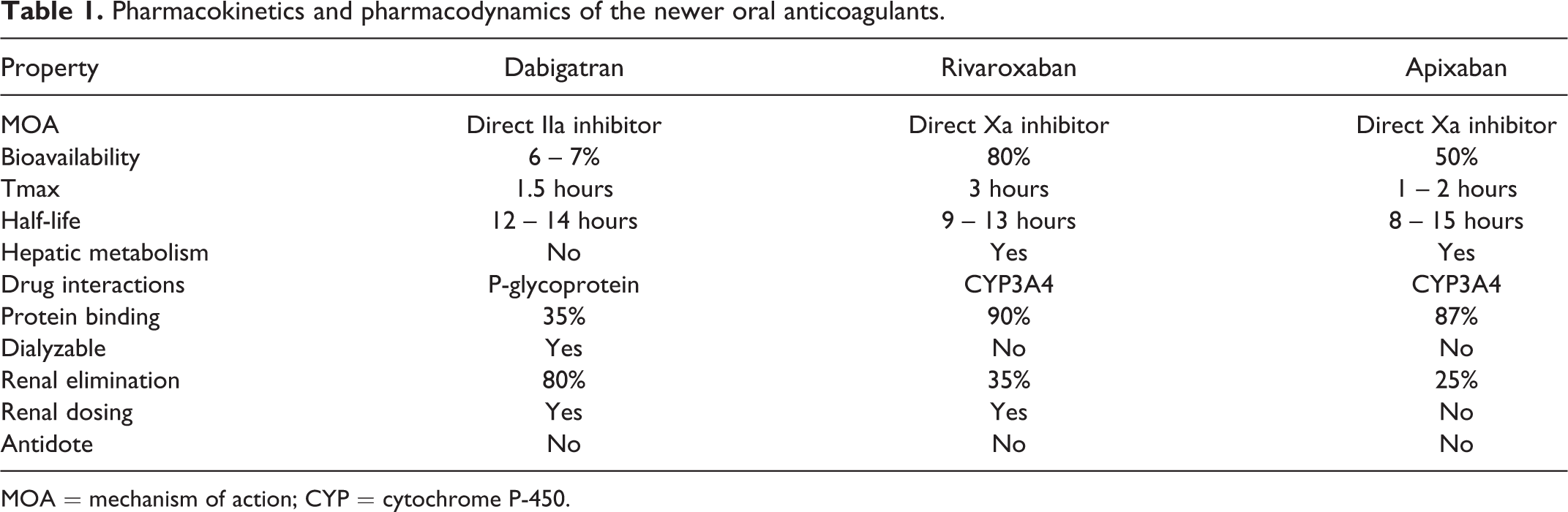
MOA = mechanism of action; CYP = cytochrome P-450.
Major ACS Clinical Trials of Newer Oral Anticoagulants.
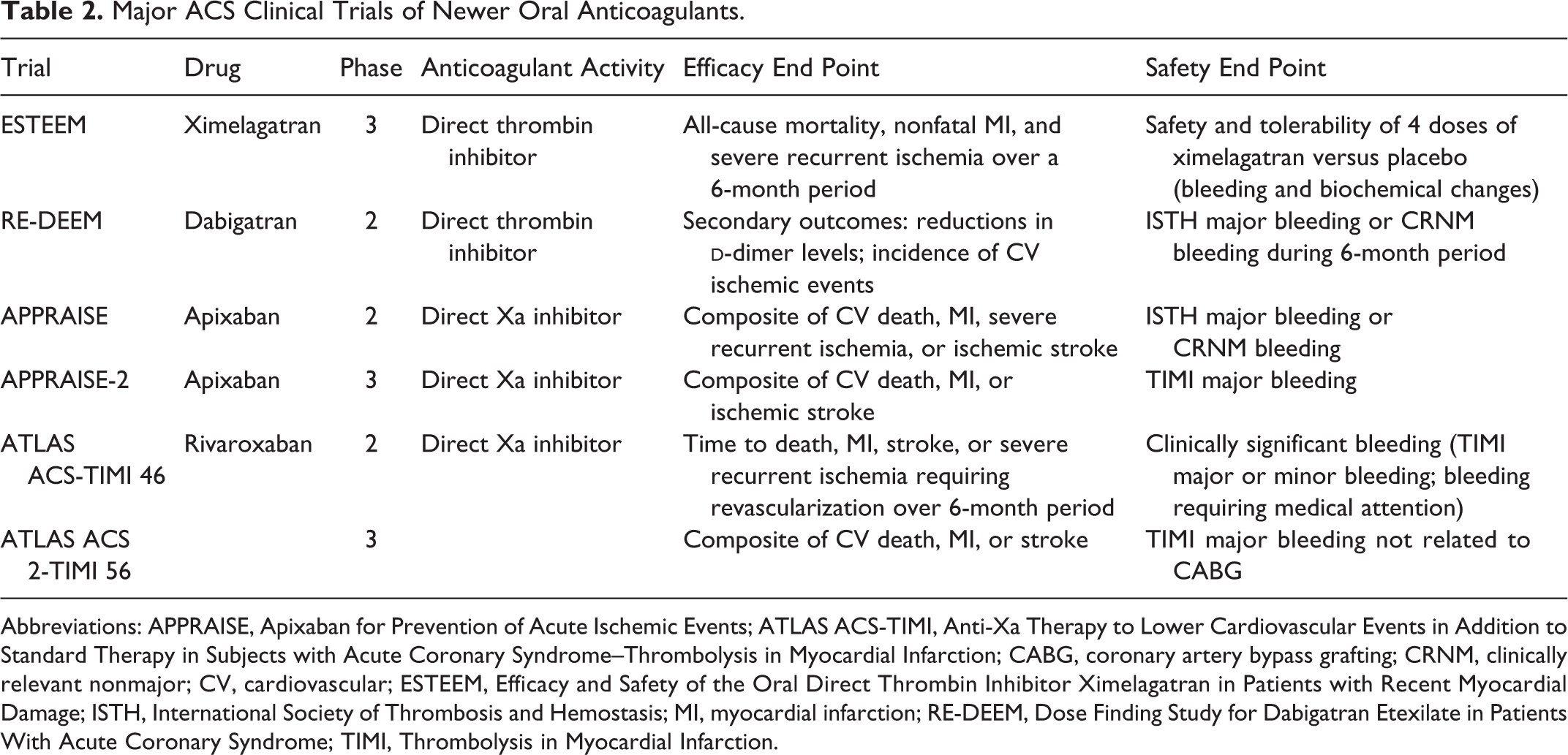
Abbreviations: APPRAISE, Apixaban for Prevention of Acute Ischemic Events; ATLAS ACS-TIMI, Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome–Thrombolysis in Myocardial Infarction; CABG, coronary artery bypass grafting; CRNM, clinically relevant nonmajor; CV, cardiovascular; ESTEEM, Efficacy and Safety of the Oral Direct Thrombin Inhibitor Ximelagatran in Patients with Recent Myocardial Damage; ISTH, International Society of Thrombosis and Hemostasis; MI, myocardial infarction; RE-DEEM, Dose Finding Study for Dabigatran Etexilate in Patients With Acute Coronary Syndrome; TIMI, Thrombolysis in Myocardial Infarction.
Direct Thrombin Inhibitors
Direct thrombin inhibitors (DTIs) inactivate free circulating and fibrin-bound forms of thrombin and limit thrombus growth and thrombogenesis. 42 The ESTEEM trial (Efficacy and Safety of the Oral Direct Thrombin Inhibitor Ximelagatran in Patients with Recent Myocardial Damage) demonstrated that ximelagatran, an early oral DTI, when used in combination with aspirin, was more effective than aspirin alone in preventing the composite end point of death, nonfatal MI, and severe recurrent ischemia. 36 Development of ximelagatran was discontinued in 2006 because of liver toxicity but not before providing preliminary evidence for the concept of DTIs as effective drugs for the secondary prevention of ACS.
Dabigatran
Dabigatran etexilate is a newer oral DTI that was approved in the United States in 2011 for the prevention of stroke in patients with atrial fibrillation. In the phase 2 dose-finding RE-DEEM trial (Dose Finding Study for Dabigatran Etexilate in Patients With Acute Coronary Syndrome), dabigatran was studied in 1861 patients with ACS, 99% of whom were receiving concomitant dual antiplatelet therapy. 37 In RE-DEEM, patients were enrolled following either STEMI (60%) or NSTEMI (40%) and randomized to twice daily treatment with dabigatran 50 mg, 75 mg, 110 mg, 150 mg, or placebo. The primary outcome was the composite of International Society on Thrombosis and Haemostasis (ISTH) major or clinically relevant nonmajor bleeding events over a 6-month treatment period. While not powered for efficacy, data on CV death, MI, and stroke were also collected.
Patients receiving dabigatran had a dose-dependent increase in bleeding events, with rates of 3.5%, 4.3%, 7.9%, and 7.8% for the 50, 75, 110, and 150 mg twice daily dabigatran doses, respectively, compared to 2.2% with placebo (P < .001 for linear trend). 37 There was no clear difference in the efficacy outcome between the dabigatran and placebo groups. The composite efficacy outcome occurred in 3.8% of patients in the placebo group, compared with 4.6% in the 50 mg, 4.9% in the 75 mg, 3.0% in the 110 mg, and 3.5% in the 150 mg dabigatran groups. While the 2 highest doses of dabigatran yielded the fewest ischemic events, they also had an almost 4-fold increase in bleeding events compared to placebo. To our knowledge, no phase 3 trials of dabigatran are planned in patients with ACS.
Recently, some safety concerns have arisen with regard to dabigatran. A meta-analysis found an increased risk of MI in patients receiving dabigatran compared with various controls. 43 This meta-analysis takes into account all studies of dabigatran with multiple comparators and varying durations of therapy. An additional analysis of the RE-LY (Randomised Evaluation of Long term anticoagulant therapY) trial found that risk of MI was also increased with dabigatran compared with warfarin in an analysis of ACS events. 44 Meanwhile, the FDA has undertaken an investigation of postmarketing reports of serious bleeding in patients receiving dabigatran. 45 Hemorrhaging appears to be associated with very elderly patients who may have declining or impaired kidney function, and lower doses of dabigatran may be more appropriate for this age group, but an advisory to this effect has not been issued to date. 46
Direct Factor Xa Inhibitors
Factor Xa is at the central point of the clotting cascade and responsible for converting prothrombin to thrombin. While several direct factor Xa inhibitors are in various stages of development, apixaban and rivaroxaban have been investigated in phase 3 trials in patients with ACS.
Apixaban
The phase 2 dose-finding trial of apixaban in patients with an ACS event was the APPRAISE trial (Apixaban for Prevention of Acute Ischemic Events). The APPRASE trial (n = 1715) evaluated apixaban 2.5 mg twice daily, 10 mg once daily, 10 mg twice daily, and 20 mg once daily compared to placebo. 38 Nearly all patients were receiving aspirin and 76% were also receiving clopidogrel. The primary outcome of ISTH major and clinically relevant nonmajor bleeding was higher in all apixaban groups compared to placebo. The 2 highest doses of apixaban were stopped early due to excess bleeding. Bleeding occurred in 3.0% of placebo patients compared to 5.7% with apixaban 2.5 mg twice daily (P = .09), and 7.9% with apixaban 10 mg once daily (P = .005). These 2 doses of apixaban also tended to have lower rates of ischemic end points (7.6% and 6.0%, respectively) than that of to placebo (8.7%). 38
The phase 3 trial of apixaban for the prevention of recurrent ACS events was the APPRAISE-2 trial. Patients in the APPRAISE-2 trial were randomized to receive apixaban 5 mg twice daily or placebo in addition to standard of care with clopidogrel plus aspirin. 39 While the trial was designed to enroll approximately 10 800 patients, it was terminated early (n = 7392 and 9 months of mean follow-up) because of an excess of clinically important bleeding events in the apixaban arm without a corresponding reduction in ischemic events. The rates of ISTH major or clinically relevant nonmajor bleeding events occurred in 3.2% of patients receiving apixaban, compared with 1.2% of those receiving placebo (P < .001). There were also significant increases in major bleeding and intracranial bleeding with the use of apixaban. The incidence of CV death, MI, or stroke was 7.5% in patients receiving apixaban and 7.9% of those receiving placebo (P = .51). Similarly to dabigatran, no additional studies of apixaban are being conducted in the setting of ACS due to unacceptable bleeding rates.
Rivaroxaban
Rivaroxaban is a direct factor Xa inhibitor that was approved in 2011 for prophylaxis against venous thromboembolism in patients undergoing hip or knee replacement surgery. Since that time, it has also been approved for the prevention of stroke and systemic embolism in patients with atrial fibrillation and for the treatment of deep vein thrombosis and pulmonary embolism and long-term secondary VTE prevention.
In the phase 2 ATLAS ACS-TIMI 46 trial (Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome–Thrombolysis in Myocardial Infarction 46), 3491 patients with recent ACS were assigned at the physician’s discretion to either aspirin alone (stratum 1) or aspirin plus a P2Y12 inhibitor (stratum 2). Patients were then randomized to receive rivaroxaban 5, 10, or 20 mg once daily or the same total dose given twice daily, or placebo for 6 months. 40 The primary safety outcome was clinically significant bleeding (TIMI major or minor bleeding or bleeding requiring medical attention). While not powered for efficacy, data on the incidence of death, MI, stroke, or severe recurrent ischemia requiring revascularization were also collected.
Clinically significant bleeding in stratum 2 patients occurred in 3.8% of placebo patients, and increased in a dose-dependent fashion for patients receiving rivaroxaban, with the lowest rate occurring in patients receiving 2.5 mg twice daily, up to 17.8% for patients receiving 20 mg once daily (P < .001 for trend). 40 The composite ischemic end point occurred in 5.1% of stratum 2 placebo patients compared with 4.0% with rivaroxaban 2.5 mg twice daily and 3.4% with rivaroxaban 5 mg twice daily. All other doses of rivaroxaban had higher ischemic event rates compared to placebo. 40 On the basis of this trial, rivaroxaban doses of 2.5 and 5 mg twice daily were selected for the phase 3 trial because they appeared to offer the best balance between safety and efficacy.
The Phase III ATLAS ACS 2-TIMI 51 trial was a randomized, double-blind, placebo-controlled trial conducted to determine whether rivaroxaban added to standard therapy would reduce CV death, MI, or stroke. Patients hospitalized with an ACS event (n = 15,526) were randomized 1:1:1 to rivaroxaban 2.5 mg twice daily, rivaroxaban 5 mg twice daily, or placebo. Approximately 99% patients received aspirin and 93% received a P2Y12 receptor inhibitor. The primary efficacy end point was a composite of CV death, MI, or stroke and the main safety end point was the incidence of non-CABG TIMI major bleeding.
After a mean follow-up of 13 months, the combined rivaroxaban groups demonstrated a significant 17% relative reduction in the primary end point compared to placebo (8.9% vs 10.7%; P = .002). For patients undergoing PCI with stent placement, rivaroxaban therapy demonstrated a significant 31% relative reduction in stent thrombosis compared to placebo (2.3% vs 2.9%; P = .008). Benefits of rivaroxaban therapy were consistent across all regions and subgroups except for patients with a history of stroke or transient ischemic attack. All-cause mortality was significantly reduced by 35% in patients receiving rivaroxaban 2.5 mg twice daily compared to placebo (2.9% vs 4.5%; P = .004), while the rivaroxaban 5 mg twice daily group did not demonstrate this same benefit (4.4%; P = .89 compared to placebo).
Randomization was stratified on the basis of planned use of thienopyridine (clopidogrel or ticlopidine). In the 93% of patients in the stratum with dual antiplatelet therapy, the addition of rivaroxaban provided a significant reduction in the primary endpoint [hazard ratio (HR) 0.86, 95% CI 0.75 – 0.98). Patients in the stratum who received only aspirin, the addition of rivaroxaban seemed to provide an even larger reduction in the primary endpoint (HR 0.69, 95% CI 0.45 – 1.05). While the aspirin result is not statistically significant, it should be noted that the CI is quite wide due to the fact this analysis included only 7% of the patients in the trial.
From the safety standpoint, there was a significant increase in non-CABG TIMI major bleeding with rivaroxaban treatment compared to placebo (2.1% vs 0.6%; P < .001) as well as an increase in the incidence of intracranial hemorrhage (0.6% vs 0.2%; P = .009). These increases in bleeding events were significant for both doses of rivaroxaban, with numerically higher rates with the higher dose of rivaroxaban. Rates of both fatal bleeding and fatal intracranial hemorrhage were not significantly increased by the use of rivaroxaban compared to placebo.
With the 2.5 mg twice daily dose of rivaroxaban, there would be 1 less ischemic event and 1 less death for every 63 patients treated, at the cost of 1 extra major bleed for every 83 patients treated and 1 extra intracranial hemorrhage for every 500 patients treated. Therefore, the results of ATLAS 2-TIMI 51 suggested that low doses of rivaroxaban added to the current standard of care may represent a new treatment strategy in patients after recent ACS.
Potential Benefits and Challenges
Improvements in medical care, more extensive education, and greater use of evidence-based guideline-recommended therapies have resulted in substantially reduced cardiac hospitalizations and mortality over the last few decades. 1 However, ACS continues to have a recurrence rate of approximately 10% per year with the current standard of care. 14 –17 These recurring events place a significant burden on the health care system. The new oral anticoagulants have mechanisms of action that are complementary to antiplatelet agents and have the potential to improve outcomes and reduce rehospitalizations in ACS. This reduction in event rates could ultimately result in significant cost savings as well as reductions in patient morbidity and mortality.
The potential benefits of anticoagulant use in ACS are countered by the inherent challenges associated with triple antithrombotic therapy. Importantly, the addition of a direct thrombin or Xa inhibitor will undoubtedly increase the risk for bleeding. It is important to note that there is currently no antidote for reversal of the anticoagulant activity for any of these newer oral anticoagulants. Identifying the optimal dose to provide beneficial thrombotic protection with the lowest bleeding risk is laborious and complicated. Furthermore, the added antithrombotic agent will increase the medication costs to payors and patients. The additional pill burden—up to twice a day dosing for some agents—and out-of-pocket expenses could negatively impact adherence for the anticoagulant and other medications critical for preventing adverse cardiovascular events following ACS. Identifying and optimizing appropriate candidates for triple antithrombotic therapy will be critical for balancing the risks and benefits of additional therapy in this complex patient population.
The optimal management of patients with ACS continues to evolve as new therapies and strategies of care are developed and proven effective. Physician adherence to evidence-based cardiac care and consensus guidelines, however, remains a challenge. 47 In patients with ACS who may benefit from the addition of an oral anticoagulant for long-term care after hospital discharge, the new agents, which lack the management problems associated with warfarin, may simplify long-term therapy and make it more attractive to both caregivers and patients.
Conclusions
Arterial thrombosis is a complex process that warrants a multitargeted approach. Dual antiplatelet therapy has improved long-term outcomes but does not affect thrombin-mediated platelet activation. Even with adherence to guideline recommendations, there remains a substantial residual risk of ACS events and death after the acute episode. By limiting thrombotic events, the new oral anticoagulants complement the current standard of care and have the potential to improve outcomes in ACS and to reduce the burden of this very costly condition.
Continuing Education Credit
The New York State Council of Health-system Pharmacists (NYSCHP) is pleased to provide you with the opportunity to obtain continuing education credit for this article online at HealthSystemCE.org (http://www.healthsystemce.org); login using your email address and HSCE password; then click the ‘‘Journal CE’’ tab. There is no charge to NYSCHP members. If you are not a member of NYSCHP, call 1-518-456-8819 to pay the $15 fee to access the quiz and obtain the password necessary to access the Journal's CE article. In lieu of this fee, a completed membership application with your dues may be submitted.
A grade of 70% or above is required to earn the CE credit. Repeat examinations will be permitted once for a grade below 70%.
 The NYSCHP is approved by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education. This activity provides 1.4 contact hours (0.14 CEUs) of continuing education. The Universal Activity Number is 0134-0000-13-080-H01-P. Submission of exam for CE credit expires August 31, 2016.
The NYSCHP is approved by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education. This activity provides 1.4 contact hours (0.14 CEUs) of continuing education. The Universal Activity Number is 0134-0000-13-080-H01-P. Submission of exam for CE credit expires August 31, 2016.
Footnotes
Acknowledgment
The authors would like to acknowledge Ruth Sussman, PhD, who provided editorial support in preparation of this manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Since submission of this manuscript, Paul Dobesh, PharmD, FCCP, BCPS, has served as a consultant to both BMS and Janssen Pharmaceuticals.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.