
Abstract
This review presents clinical pearls for initiating liraglutide (Victoza®, Novo Nordisk Inc) therapy for the management of type 2 diabetes and selecting patients who will benefit from liraglutide therapy. Liraglutide, a once-daily glucagon-like peptide 1 receptor agonist, is Food and Drug Administration approved as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes. Liraglutide is effective for reducing hemoglobin A1c levels by 0.8% to 1.5% in patients with type 2 diabetes as monotherapy or in combination with other diabetic medications (such as metformin, sulfonylureas, rosiglitazone, or basal insulin) when compared with placebo and these other diabetic medications, including exenatide. Overweight or obese patients with type 2 diabetes or those with insulin resistance are good candidates for liraglutide therapy because liraglutide use is associated with weight loss (about 2%-4% of initial body weight) and improved β-cell function. The incidence of hypoglycemia with liraglutide is low; therefore, liraglutide would be a safe therapy choice for patients at risk or with a history of symptomatic or severe hypoglycemia. Nausea seems to be the most problematic adverse effect associated with liraglutide therapy, but it is usually transient and is minimized with dose titration.
Introduction
Victoza (liraglutide), a glucagon-like peptide 1 (GLP-1) receptor agonist, is Food and Drug Administration (FDA) approved as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes (Table 1). 1 Its efficacy and safety have been studied as monotherapy and combination therapy (with metformin, sulfonylureas, or rosiglitazone) in comparative clinical trials. Current diabetes treatment algorithms and guidelines were published before liraglutide’s approval in the United States, but it is expected that liraglutide would be considered as an adjunct or alternative to, in case of intolerance, metformin therapy. Clinical pearls for initiating liraglutide therapy for the management of type 2 diabetes and selecting patients who will benefit from liraglutide therapy are addressed in this review.
Liraglutide Product Formulation, Storage, and Dosing. 1

Pharmacokinetics and Pharmacodynamics of Liraglutide. 1
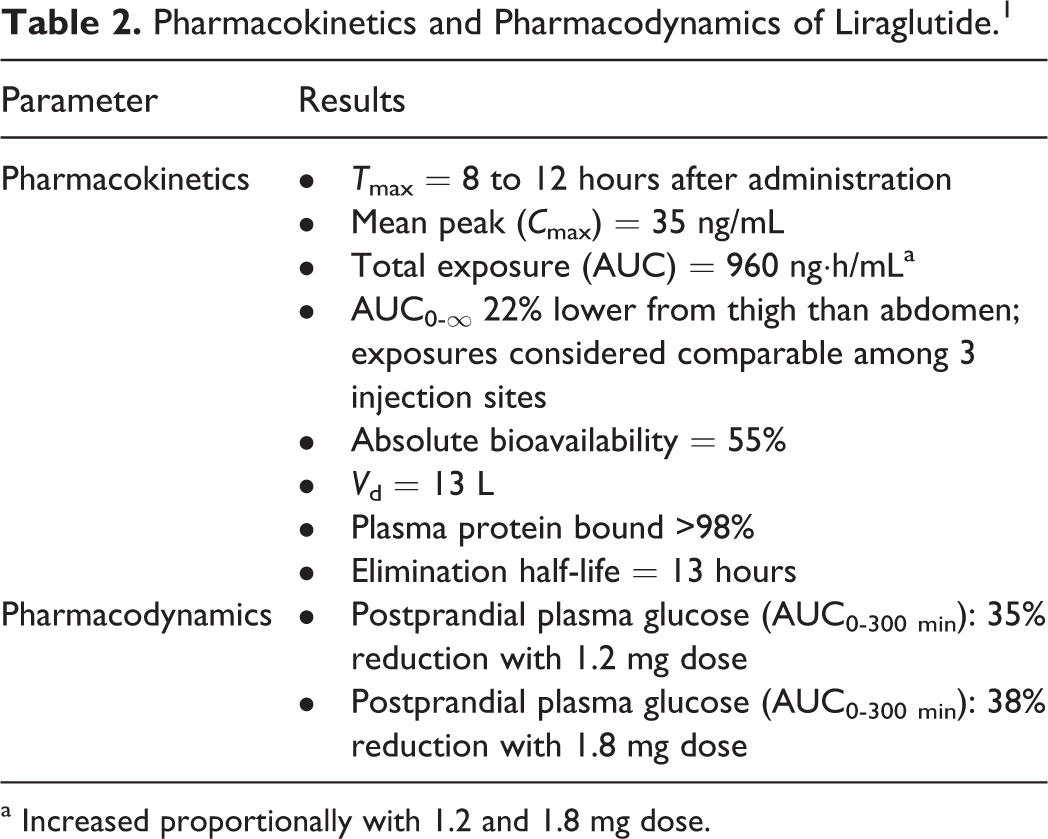
a Increased proportionally with 1.2 and 1.8 mg dose.
Algorithm and Guideline Application to Clinical Practice and Liraglutide Use
Per the 2009 American Diabetes Association and the European Association for the Study of Diabetes (ADA/EASD) consensus statement, the tier 1 (well-validated core) step 1 therapy for type 2 diabetes is lifestyle modification to decrease weight and increase activity and metformin 500 mg once or twice daily titrated to 1000 mg twice daily. 2 However, lifestyle modification and metformin therapy are sometimes insufficient to control hyperglycemia because of insulin resistance primarily caused by or secondary to weight gain. ADA/EASD recommends a hemoglobin A1c (HbA1c) goal of less than 7% 2 ; however, less than 40% of patients with diabetes will meet this target HbA1c. 3 Many US clinicians use 7% as the HbA1c target level for the majority of patients with type 2 diabetes because this target value is associated with a reduced incidence of diabetes-related microvascular complications 4 and seems to be associated with fewer hypoglycemic events. In comparison, the American Association of Clinical Endocrinologists/American College of Endocrinology (AACE/ACE) Diabetes Glycemic Control Algorithm Consensus Panel recommends a target HbA1c goal of 6.5%. 5 AACE/ACE prioritizes choices of medications according to safety, risk of hypoglycemia, efficacy, simplicity of use, anticipated degree of patient adherence, and cost. 5 The more aggressive HbA1c target of 6.5% (vs 7%) is generally reserved for recently diagnosed young patients at low risk of developing hypoglycemia, who have not developed diabetes-related macrovascular complications. The HbA1c should be maintained at >6% for patients with preexisting cardiovascular (CV) disease and a long duration of diabetes based on recent study results that suggest increased mortality with lower HbA1c targets (<6%) for high-risk patients with advanced type 2 diabetes. 4
According to the Global Partnership for Effective Diabetes Management, early and effective interventions to achieve target HbA1c levels are needed to maximize treatment benefits, as even short periods of hyperglycemia increase the risk of microvascular and macrovascular complications. 6 While most clinicians would agree with this philosophy, it is easier said than done. Many clinicians feel that lifestyle modification should be tried first, depending on the HbA1c, although they also believe it is usually insufficient to control hyperglycemia. As pharmacists, medications are an important part of practice, and in most cases, lifestyle modification alone is not enough. However, it is also known that a healthy diet and regular exercise are crucial to increase the effectiveness of diabetic medications like metformin and liraglutide.
ADA/EASD and AACE/ACE recommend metformin monotherapy as first-line therapy for type 2 diabetes. 2,5 AACE/ACE also recommends thiazolidinediones (TZDs), dipeptidyl peptidase-4 (DPP-4) inhibitors, and alpha-glucosidase inhibitors. 5 Metformin is considered the cornerstone of monotherapy and is usually the most appropriate initial choice for monotherapy unless there is a contraindication, such as renal disease, hepatic disease, gastrointestinal (GI) intolerance, or risk of lactic acidosis. Unless contraindicated, most patients with type 2 diabetes are taking metformin or have been given a trial of metformin. In addition to lifestyle modifications and metformin, ADA/EASD also recommends insulin and sulfonylurea therapy as tier 1, step 2 drug therapy (adding on to step 1). 2 Sulfonylurea therapy reduces HbA1c by 1% to 2% and is rapidly effective; however, it is associated with weight gain and hypoglycemia. In combination with metformin, weight gain is minimized, although patients may still develop hypoglycemia. Another potential issue is that some patients do not initially respond to metformin or sulfonylurea therapy. As with any secretagogue, sulfonylureas may hasten the rate of β-cell function decline, so these agents are beneficial early in the disease course but most lose effectiveness as the disease progresses. For alternatives to sulfonylurea therapy that also meet the goal of preserving β-cell function, metformin, GLP-1 receptor agonists, and even insulin may be suitable therapeutic options. However, because of its generic status, sulfonylurea therapy is still commonly prescribed after metformin therapy has failed, for patients who are unable to afford more costly medications. Sulfonylurea and insulin therapy have a relatively higher rate of hypoglycemic events and incidence of weight gain than other diabetic medications; whereas metformin and GLP-1 receptor agonists are generally not associated with either of these negative effects. 2
Liraglutide, GLP-1 Receptor Agonist Overview
GLP-1 receptor agonists stimulate insulin release from pancreatic β-cells in the presence of elevated glucose concentrations and decrease glucagon secretion, which lowers blood glucose concentrations until euglycemia is achieved. 1 Also, these effects decrease gastric emptying, which can increase or cause satiety (probably through a central effect). GLP-1 receptor agonists decrease HbA1c by 1.0% to 1.5%, reduce weight (about 2%-4% of initial body weight), and have a low incidence of hypoglycemia. 1,2 Pharmacokinetics and pharmacodymamics of liraglutide appear in Table 2. ADA/EASD recommends GLP-1 receptor agonists as tier 2, specifically when hypoglycemia is particularly undesirable. 2 Liraglutide was FDA approved in January 2010, after the ADA/EASD consensus statement (2009) was published, and it is not included by name in the current consensus statement. Liraglutide is effective as monotherapy and in combination with metformin and other diabetic medications after failure of metformin therapy. 1 Therefore, it is expected that liraglutide would also be considered tier 2.
AACE/ACE recommends that the second component of dual therapy be an incretin mimetic (ie, exenatide), a DPP-4 inhibitor, a glinide, or a sulfonylurea (recommended in stated order) and that the first component be metformin or a TZD, which will serve as an insulin sensitizer. 5 The GLP-1 receptor agonist, exenatide, is included as a second preferred component because of its safety profile (it has a low incidence of hypoglycemia because stimulation of insulin release is glucose dependent) and its potential for promoting weight loss. 5 AACE/ACE published this algorithm before liraglutide’s FDA approval, 1 but it is expected that liraglutide would also be considered the second preferred component based on the same rationale (safety and weight loss potential), with the added benefit of improved medication adherence with once-daily dosing. In a meta-analysis of 38 recent randomized, placebo-controlled trials to assess the efficacy of incretin-based medications in adult patients with type 2 diabetes, liraglutide ranked highest for clinical efficacy (1% reduction in HbA1c) followed by sitagliptin (0.8% reduction) and exenatide (0.8% reduction) when compared with placebo. 7
Monotherapy
Liraglutide monotherapy could be a good option for patients with type 2 diabetes who have a contraindication to or cannot tolerate metformin. In 2 clinical studies, liraglutide monotherapy significantly decreased HbA1c from baseline compared with placebo and a sulfonylurea. 1,8 In a double-blind, randomized clinical study, 746 patients with early type 2 diabetes were administered liraglutide 1.2 mg (n = 251) or 1.8 mg (n = 247) or glimepiride 8 mg (n = 248) once daily for 52 weeks. 8 HbA1c levels decreased from baseline by 0.5% ± 1.2% with glimepiride, 0.8% ± 1.2% with liraglutide 1.2 mg, and 1.1% ± 1.2% with liraglutide 1.8 mg (P < .0001; liraglutide 1.8 mg vs glimepiride). Patients receiving liraglutide lost an average of 2 to 2.5 kg, which was sustained throughout the 52-week study, whereas those taking glimepiride gained about 1 kg (P = .0001 for liraglutide 1.8 mg vs glimepiride 8 mg) of weight. In an open-label extension trial, 1 after 2 years of treatment, the HbA1c change was −0.6% with glimepiride compared with −0.9% with liraglutide 1.2 mg. Patients receiving liraglutide therapy for 2 years maintained HbA1c levels similar to the values observed after 1 year of therapy. Mean body weight reductions were maintained over 2 years in both liraglutide groups, while the glimepiride group gained weight. A significant reduction in waist circumference was observed with liraglutide 1.2 mg (4.0 cm) and liraglutide 1.8 mg (4.9 cm) compared with glimepiride (1.0 cm; P = .0413 for liraglutide 1.2 mg and P = .0095 for liraglutide 1.8 mg vs glimepiride). The rates of minor hypoglycemic events were 0.21 events per patient-year with liraglutide 1.2 mg and 0.22 with liraglutide 1.8 mg, which are significantly lower than the rate observed with glimepiride (1.75; P < .0001 for both comparisons vs glimepiride). Liraglutide may serve as an alternative to a sulfonylurea because of the beneficial effects on weight and potential for β-cell preservation.
Neither the ADA/EASD nor the AACE/ACE recommends GLP-1 receptor agonists as monotherapy for the management of type 2 diabetes; however, DPP-4 inhibitors are suggested as monotherapy by AACE/ACE. 2,5 The data reviewed here show that liraglutide is effective as monotherapy; therefore, it could be considered for patients who are unable to tolerate metformin or in whom metformin is contraindicated. This is relevant especially for those patients who are overweight and have been unable to control or lose weight with lifestyle modifications.
Combination Therapy
Liraglutide provides additional HbA1c reductions when added to failed metformin therapy. In a randomized, double-blind, placebo-controlled clinical trial, 9 1091 patients with type 2 diabetes received metformin 1 g twice daily and either liraglutide 0.6, 1.2, or 1.8 mg once daily or glimepiride 4 mg once daily. Compared with placebo, all liraglutide groups had a significant reduction in HbA1c of 1.0% for liraglutide 1.2 and 1.8 mg and glimepiride (P < .0001; treatment vs placebo) and 0.7% for liraglutide 0.6 mg, and an increase of 0.1% for placebo. Body weight decreased in all liraglutide groups (by 1.8-2.8 kg from baseline) compared with an increase in body weight in the glimepiride group (by 1.0 kg; P < .0001).
Liraglutide is effective with TZDs and metformin, but weight loss, instead of weight-neutral effects, is observed with the latter combination. These effects were noted in a double-blind, placebo-controlled, clinical study of 533 type 2 diabetic patients given liraglutide 1.2 or 1.8 mg once daily or placebo in combination with metformin 1 g twice daily and rosiglitazone 4 mg twice daily. 10 Mean HbA1c values decreased significantly in patients who received liraglutide compared with placebo (1.5% for both 1.2 and 1.8 mg liraglutide and 0.5% for placebo; P < .001) and dose-dependent weight loss occurred with liraglutide 1.2 and 1.8 mg (1.0 and 2.0 kg, respectively) compared with weight gain with placebo (0.6 kg; P < .0001). GI adverse events were observed more commonly with liraglutide, but most occurred early in the course of treatment and resolved within the first 4 weeks of use. Adding liraglutide to a sulfonylurea produced greater improvements in glycemic control and weight loss than did adding rosiglitazone. 11 All of these liraglutide combinations have been very successful in reducing HbA1c and with the added benefit of limiting weight gain. Decreased insulin resistance and weight loss observed with liraglutide in combination with oral agents may allow the discontinuation of sulfonylurea therapy, leading to better outcomes for the patient. Of note when initiating liraglutide therapy, it may be necessary to reduce the dose of the secretagogue agent by one-third to one-half (depending on the patient) once the maximum dose of liraglutide is achieved.
GLP-1 Receptor Agonist Comparison
Liraglutide and exenatide have a low incidence of hypoglycemia and decrease weight. In a comparative trial, liraglutide was significantly more effective at reducing HbA1c than exenatide, although the differences may not be clinically significant. In a multinational, open-label trial, adults with type 2 diabetes not adequately controlled with metformin, a sulfonylurea, or both, were randomized to receive additional liraglutide 1.8 mg once a day (n = 233) or exenatide 10 mcg twice daily (n = 231). 12 Liraglutide reduced the mean HbA1c by 1.1% compared with exenatide (0.8%) with an estimated treatment difference of −0.3% (P < .0001). More patients achieved a HbA1c value of <7% with liraglutide therapy than with exenatide (54% vs 43%, respectively; P < .001) although mean weight loss was similar between groups (3.24 kg for liraglutide and 2.87 kg for exenatide). In an extension study, patients who switched from exenatide 10 mcg twice daily to liraglutide 1.8 mg once daily or continued liraglutide had significant improvement in HbA1c and other glycemic and nonglycemic parameters. 13 Switching from exenatide to liraglutide further reduced HbA1c from 7.2% at week 26 to 6.9% at week 40 (0.32%; P < .0001), fasting blood glucose ([FBG] 0.9 mmol/L, 17.8 mg/dL; P < .0001), body weight (0.9 kg; P < .0001), and systolic blood pressure ([SBP] 3.8 mm Hg; P < .0001) with minimal minor hypoglycemia (1.30 episodes/patient-year) or nausea (3.2%) compared with baseline. Consistent with reductions in FBG, the mean homeostasis model of β-cell function (HOMA-B) assessment significantly increased by 14.5% (P < 0.001). Among patients continuing liraglutide, further decreases in body weight (0.4 kg) and SBP (2.2 mm Hg) were observed with a low incidence of hypoglycemia and nausea (0.74 episodes/patient-year of minor hypoglycemia and 1.5% of patients experienced nausea). 13
Although 2-year data are available, it may be too early to determine whether there are important differences in long-term weight loss between these agents, since liraglutide has only been on the market a relatively short time. However, weight loss seems to be maintained for at least 2 years for most patients. Some of our patients have achieved a dramatic weight loss of 20 to 30 lbs and corresponding HbA1c reductions of 2% to 2.5% with liraglutide therapy. Subsequently, the weight loss contributed to dramatic improvement in lipid and BP values. Choosing between these agents often depends on formulary coverage, but patient-specific reasons can guide therapy decisions. Both agents are very effective in clinical practice. Medication adherence may not be an issue with exenatide even though it is given twice daily and may be less of a concern with the availability of once-weekly exenatide. However, anecdotally, many patients prefer the once-a-day injection and the flexibility to take liraglutide without regard to meals.
Compared with insulin, patients receiving liraglutide in combination with oral diabetic medications have experienced similar reductions in HbA1c levels and reductions in body weight (at this time, liraglutide is not FDA approved for use with prandial insulin). Liraglutide has been compared with insulin glargine (both in combination with metformin and sulfonylurea) in a controlled clinical trial. Patients with type 2 diabetes were randomized to receive liraglutide 1.8 mg once daily (n = 232), placebo (n = 115), and open-label insulin glargine (n = 234) in combination with metformin 1 g twice daily and glimepiride 4 mg once daily. 14 Liraglutide therapy improved glycemic control and reduced body weight compared with placebo and insulin glargine. HbA1c reduction from baseline was 1.3% with liraglutide, 1.1% with glargine, and 0.2% with placebo. The difference in HbA1c reduction with liraglutide compared with insulin glargine was within the predefined noninferiority margin (of 0.4 percentage points). Mean weight loss from baseline was 1.8 kg for the liraglutide group and 0.42 kg for placebo (P < .001). Body weight increased by 1.6 kg with insulin glargine therapy and a mean difference of −3.43 kg (95% confidence interval, −4.00 to −2.86 kg; P < .0001 vs liraglutide) was reported. Although liraglutide was noninferior to insulin in this clinical trial, there is no maximum dose of insulin and therefore no ceiling on the potential HbA1c reduction with insulin, whereas the maximum dose of liraglutide is 1.8 mg daily. Liraglutide, however, is a good therapeutic option prior to initiation of insulin in patients with existing β-cell function. Liraglutide in combination with basal insulin therapy has been shown in clinical trials to further reduce HbA1c and minimize weight gain. In insulin-naive patients with type 2 diabetes, coadministration of liraglutide 1.8 mg and insulin detemir produced an additive glucose-lowering effect and did not significantly alter the pharmacokinetic profile of either drug. 15 Although weight loss is not generally desired for patients with type 1 diabetes, weight loss was observed in a group of these patients given insulin and liraglutide. In a small clinical trial of 29 type 1 diabetes patients (with and without residual β-cell function), 18 of the 19 patients receiving liraglutide and insulin lost an average of 2.3 kg (±0.3 kg; P < .001 vs insulin monotherapy). 16
Nonglycemic Effects
In preclinical trials, incretin-based agents decreased BP and reduced inflammation; however, the long-term safety and potential positive effects on CV outcomes in patients with diabetes and established CV disease are still unknown. 17 Effects such as weight loss, low-density lipoprotein (LDL), and triglyceride (TG) concentration reductions, and SBP reduction (with and without hypertension medication use) are observed with liraglutide. A meta-analysis of 3 large pooled-data studies with liraglutide showed a significant 2.7 to 4.5 mm Hg reduction (vs comparators; P < .5) in SBP, but no significant decrease in diastolic BP ([DBP] 0.2-0.4 reduction vs comparator; P value not reported). 18 Long-term, open-label, follow-up studies of exenatide showed mean decreases from baseline of 3.5 mm Hg (P < .0063) and 3.3 mm Hg (P < .0001) in SBP and DBP, respectively, over the 3-year study period. 19 Liraglutide use was associated with improvement in LDL cholesterol (up to −0.28 ± 0.07 vs −0.10 ± 0.07 mol/L; −5 ± 1.25 vs −1.78 ± 1.25 mg/dL; P < 0.05 vs placebo) and TG concentrations (up to −0.38 ± 0.10 vs −0.13 ± 0.11 mmol/L; 6.78 ± 1.78 vs 2.32 ± 1.96 mg/dL; P < 0.05 vs placebo).8,10 Weight loss associated with liraglutide was described previously in this review. Although not well studied, these effects could benefit type 2 diabetes patients with obesity, dyslipidemia, or hypertension. Theoretically, GLP-1 agonist effects on CV risk factors and blood vessels should reduce CV risk. 17 We should have a better understanding of the CV effects of GLP-1 agonists when results of the multiple, ongoing CV outcome studies become available.
Contraindications to GLP-1 Receptor Agonists
C-cell thyroid cancer
Thyroid cancer with high doses of liraglutide has been reported in a murine model. 1,20 In clinical trials, there have been 4 reported cases of thyroid C-cell hyperplasia among patients treated with liraglutide 1 ; 1 additional case of thyroid C-cell hyperplasia has subsequently been reported. Of the 5 patients treated with liraglutide, 4 had elevated calcitonin concentrations at baseline and throughout the trial. Until additional data in humans become available, liraglutide should be avoided in those patients with a personal or family history of thyroid C-cell tumors, including medullary thyroid carcinoma and multiple endocrine neoplasia syndrome type 2. 1 While this type of thyroid carcinoma is rare, patients are extremely concerned about it. A good counseling session prior to use usually addresses any patient concerns and increases the patient’s confidence in the treatment choice.
Pancreatitis
Hemorrhagic or necrotizing pancreatitis with use of GLP-1 receptor agonists has been reported in the literature; however, more data are needed before a causal relationship with GLP-1 receptor agonists can be confirmed. The mechanism by which GLP-1 receptor agonists could cause pancreatitis is not known. Acute pancreatitis and its association with GLP-1 receptor agonist use is complex because having type 2 diabetes, obesity, and high TG levels are risk factors for developing acute pancreatitis. 21 Typical signs and symptoms of pancreatitis include persistent severe abdominal pain or cramping that radiates to the back and may or may not be accompanied by nausea and vomiting. If signs and symptoms of pancreatitis occur, the GLP-1 receptor agonist should be discontinued and appropriate medical attention and diagnostic evaluations should be initiated. Although uncommon in clinical practice, the onset of pancreatitis can be sudden or develop over an extended period of time depending on individual risk factors. One of the difficulties of evaluating the incidence of pancreatitis in this population is that the symptoms of pancreatitis mimic adverse effects associated with the medication. If symptoms of abdominal pain and nausea do not resolve within the first week of therapy, discontinuation of therapy should be considered and appropriate laboratory tests should be performed to rule out pancreatitis. If related to GLP-1 agonist use, symptoms typically resolve soon after therapy discontinuation. In some cases, insulin is required for a short period of time until pancreatitis and hyperglycemia improve. Alternative agents to GLP-1 receptor agonists should be considered in patients with a history of pancreatitis. Until results from postmarketing studies become available, patients taking a GLP-1 receptor agonist should be monitored carefully for signs and symptoms of acute pancreatitis.
Adverse Events
Nausea
Prolonged or severe nausea can limit the use of GLP-1 receptor agonists. Titration with liraglutide reduces the incidence of nausea and improves the transition to effective treatment. 1 Less-persistent nausea was observed with liraglutide compared with exenatide therapy. The most frequent and severe adverse events reported in 1 clinical trial were dyspepsia for liraglutide patients (3 of 235) and nausea for exenatide patients (4 of 232). 12 The incidence of nausea was similar initially; however, nausea was less persistent with liraglutide (estimated treatment rate ratio, 0.448 vs exenatide). By the end of the 26-week study period, 3% of patients treated with liraglutide reported nausea (n = 5/202) compared with 9% of exenatide patients (n = 16/186). The mechanism by which GLP-1 receptor agonists (including liraglutide) cause nausea is unknown. One possible mechanistic cause of nausea includes delayed gastric emptying. To minimize GI adverse effects, liraglutide should be initiated at 0.6 mg daily for 1 week and increased by 0.6 mg weekly until the desired HbA1c goal is obtained or until a maximum dose of 1.8 mg daily is achieved. 1 The likelihood of prolonged nausea is less with liraglutide compared with exenatide. In addition, the severity of nausea appears to be less with liraglutide. Nausea may be confused with a sensation of fullness in some patients and, therefore, could be alleviated by reducing food portion size. 22,23 Patients can cope better with this adverse effect if they are warned about the possibility of nausea with the initiation and/or titration of therapy and informed that it typically subsides over the first few weeks of use. Increasing fluid intake, symptomatic use of antacids, and drinking a sugar-free carbonated beverage after injection may help alleviate nausea. Based on the elimination half-life, patients should reinitiate liraglutide at the dose of 0.6 mg if more than 3 days have passed since the last dose of liraglutide (refer to Table 2). 1 This approach should minimize GI symptoms associated with the reinstatement of liraglutide. The patient should be titrated to a therapeutic dose as quickly as possible while avoiding GI symptoms.
Renal failure
Unlike exenatide and some DPP-4 inhibitors, liraglutide is endogenously degraded without a specific organ as a major route of elimination. 24 Renal dysfunction did not increase exposure of liraglutide in patients with type 2 diabetes; therefore, patients with renal impairment do not require dosage adjustment of liraglutide therapy. In addition, liraglutide has not been shown to be directly nephrotoxic. 1 However, postmarketing reports indicate that acute renal dysfunction and worsening of chronic renal dysfunction has occurred with liraglutide therapy, usually in association with nausea, vomiting, diarrhea, or dehydration, which required hemodialysis in some patients. 1 Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status. Altered renal function was reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents. Therefore, the prescribing information inserts for both exenatide and liraglutide recommend to use caution when initiating or escalating doses of liraglutide in patients with renal impairment. 1,25 We have not seen much nausea associated with liraglutide therapy, and so it may be that the issues with renal impairment with liraglutide have been noticeably less. Because liraglutide is newer to the market, the verdict is still not in on the relationship between renal dysfunction and liraglutide therapy. In most cases, new-onset renal impairment is more the result of dehydration than drug-induced nephrotoxicity. With the current information available, for patients with renal dysfunction, insulin may be the safest choice.
Hypesensitivity reactions
Postmarketing reports of serious hypersensitivity reactions (such as anaphylactic reactions and angioedema) have been reported with the use of liraglutide. 1 If a hypersensitivity reaction occurs, the patient should discontinue liraglutide and other suspected medications and seek medical attention.
Summary
GLP-1 receptor agonists can address many of the unmet needs of diabetes treatment such as a low risk of hypoglycemia, weight loss, and long-term safety and tolerability. 26 Compared with other diabetic medications, which are available as generics or oral formulations, GLP-1 receptor agonists are more expensive when only the product cost is considered. Liraglutide was cost effective compared with rosiglitazone when used in combination with glimipiride. 27 Cost-effectiveness analyses for other classes of diabetic medications are not available. However, studies are needed that consider the costs associated with reduced rates of hypoglycemia events, weight loss, and other nonglycemic effects. Since diabetes and CV disease are often associated with obesity, GLP-1 receptor agonists have the potential to reduce this major risk factor. The benefits of glucose control and weight loss may ultimately reduce the need for hospital and emergency room visits and thereby decrease the overall health care costs, despite the small increase in medication cost.
Footnotes
Acknowledgments
The author wishes to thank Beatriz Manzor Mitrzyk, PharmD, of MedVal Scientific Information Services, LLC, for providing medical writing and editorial assistance.
Authors’ Note
This article was prepared according to the International Society for Medical Publication Professionals’ Good Publication Practice for Communicating Company-Sponsored Medical Research: the GPP2 Guidelines.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: funding to support the preparation of this manuscript was provided by Novo Nordisk Inc.