
Abstract
Due to the increased incidence and recurrence of Clostridium difficile infection, health care providers are seeking new and alternative treatments to the standard antibiotic therapy. The objective of this article is to present a review on the background, microbiologic efficacy, clinical efficacy, and safety of fecal microbiota transplantation and to provide an overview of emerging treatment options currently under investigation. Emerging treatment options discussed include the use of monoclonal antibodies directed against toxins A and B, C difficile vaccination, and transplantation of nontoxigenic C difficile strains.
Introduction
Clostridium difficile infection (CDI) is a gastrointestinal (GI) disease caused by C difficile, a spore-forming, gram-positive bacillus that produces 2 exotoxins (toxins A and B). The pathogenesis of CDI is complex and multifactorial but is believed to be due to an alteration in the intestinal microbiota, production of toxins, and impaired host immunity. 1 CDI is the most common cause of infectious diarrhea in the health care setting. 2 Based on a report by Lessa et al, the discharge rate for patients with any diagnosis of CDI from short-stay hospitals in the United States increased from 3.82 per 1000 discharges in 2000 to 8.75 per 1000 discharges in 2008. This increase was especially dominant in those ≥65 years of age. 3 With the increased rate, 1 study found the estimated excess cost of CDI in US acute care facilities in 2008 may have been up to $4.8 billion. 4
Initial episodes of CDI are treated with either oral metronidazole or oral vancomycin depending on the severity of the disease. In patients with complicated CDI (eg, hypotension, shock, ileus, and megacolon), treatment with high-dose oral vancomycin plus intravenous metronidazole is recommended. In those patients with complete ileus, vancomycin instilled rectally may be considered. 2 Approximately 20% to 35% of the patients will experience a recurrence of symptoms after treatment of an initial CDI episode. Once recurrence occurs, up to 65% of the patients will have repeated episodes that can continue for months to years. 5 The first recurrence is typically treated with the same treatment as the initial episode, while second recurrences and beyond are treated with a tapered and/or pulsed oral vancomycin regimen. 2
Due to poor treatment outcomes of recurrent CDI and its financial burden on the health care system, health care providers are seeking new and alternative treatment options to the standard antibiotic therapy of metronidazole and vancomycin. One suggested alternative treatment that has become increasingly more accepted is fecal microbiota transplantation (FMT). This is evident in a recent survey to assess whether gastroenterologists and/or infectious disease specialists in Houston, Texas, would support and refer patients to a newly developed, local FMT treatment center. The survey found that 89% (49 of 55) of the gastroenterologists and 81% (26 of 32) of the infectious disease specialists would refer a patient with recurrent or refractory CDI to the treatment center. 6 Other emerging treatments currently under investigation include the use of monoclonal antibodies directed against toxins A and B, C difficile vaccination, and transplantation of nontoxigenic C difficile strains.
The objective of this article is to present a review on the background, microbiologic efficacy, clinical efficacy, and safety of FMT and to provide an overview on the use of monoclonal antibodies, vaccination, and transplantation of nontoxigenic C difficile strains for the treatment of CDI.
Fecal Microbiota Transplantation
Background
FMT is a suggested alternative treatment for recurrent CDI. This treatment approach involves transplanting fecal suspension from a healthy donor to patients with GI disorders, such as CDI, via colonoscopy, fecal enema, or nasogastric tube. Although transplanted fecal microbiota is believed to restore the natural balance of the patient’s disrupted GI flora due to antibiotic usage or other factors, the precise mechanisms are not fully understood. Proposed mechanisms include regeneration of colonization resistance, restoring normal GI flora, and the direct antagonistic activity of the normal flora to C difficile. 7 Despite the unpleasant nature of the treatment, its use dates back to the fourth century Chinese medicine for the treatment of food poisoning and severe diarrhea. Furthermore, fecal bacteriotherapy is a well-known practice in veterinary medicine in a process referred to as transfaunation and rumen transfaunation. 8 In modern history, the first case report describing the use of FMT in human subjects was published in 1958. Four patients with pseudomembranous enterocolitis were treated with FMT and showed dramatic response in the first 48 hours. 9 Since then, a plethora of case reports have emerged describing individual success and various protocols to perform FMT.
Human colonic microbiota composition is known to be relatively stable after the first years of life 10 owing to the colonization resistance of GI flora. This refers to the ability of natural GI flora to exhibit innate resistance to colonization of potentially invasive species. 11,12 The theoretical mechanisms involved in the colonic flora homeostasis include secretion of bactericidal substances, competition for intestinal adherence, and even regulation of immune responses. 13 Although the composition of the colonic flora is relatively stable in healthy patients, it has become clear that antibiotic therapy can disrupt the balance and richness of microbial communities in such a way that it may favor colonization, overgrowth, and/or toxin production by C difficile. 14–16 Moreover, this effect can be lasting in adults and infants. 17,18 Chang et al analyzed the fecal microbiome of 4 adult patients with an initial episode of CDI, 3 with recurrent CDI, and 3 control subjects using culture-independent analysis of 16S ribosomal RNA (rRNA)-encoding gene sequences. Compared with those from control subjects and patients with an initial CDI episode, the fecal communities in patients with recurrent CDI were highly variable in bacterial composition and were characterized by markedly decreased diversity. 17 In another study, fecal samples from 9 infants who received parenteral ampicillin and gentamicin were analyzed 4 and 8 weeks after the end of treatment. Significant changes in colonic microbiota were noted compared to control subjects, suggesting considerable alterations in the evolution of the gut microbiota. 18 Finally, along with antibiotic-related effects on gut microbiota, hospital exposure was shown to have an association with notable changes in gut microbiota—namely dominance of Firmicutes sp and loss of Bacteroides sp strains—and risk of CDI. 19
Microbiologic Efficacy
Three studies evaluated the microbiologic changes in colonic composition following FMT in patients with GI disorders such as CDI, irritable bowel syndrome (IBS), Crohn’s disease, and constipation. In 1989, investigators studied 6 patients with chronic relapsing CDI who were treated with FMT. Posttreatment fecal samples showed loss of C difficile and its toxin and colonization by Bacteroides sp, which was absent in pretreatment samples. The finding suggests that disruption in normal fecal microbiota composition plays an important role in acquiring C difficile, and if not restored can contribute to recurrent CDI following initial treatment. 20
The second study by Khoruts et al used terminal restriction fragment length polymorphism and 16S rRNA gene-sequencing approaches to characterize the colonic composition of a 61-year-old female patient with recurrent CDI and pseudomembranous colitis before and after receiving FMT via colonoscopy from a healthy related donor. Patient was treated with nitazoxanide, due to repeated failure of conventional treatment, until the day before the procedure. Fecal samples from the patient were collected 7 days prior to procedure (−7), on day of procedure (0), then 14 and 33 days following FMT. Fecal samples on days −7 and 0 showed lack of Bacteroides sp strains while showing a predominance of Clostridium sp strains and variation between fecal and intestinal microbiome. Postprocedure samples on day 14 showed dramatic changes in colonic composition that was highly similar to the donor and dominated by Bacteroides sp strains. By day 33, slight changes were noted compared to day 14 yet dominated by Bacteroides sp, Ruminococcaceae sp, and Anaerosipes sp strains. Overall, fecal microbiota composition of the study patient showed marked similarity to that of the donor, while exhibiting rapid and complete recovery of symptoms during the study period. 21
The final study by Grehan et al examined 10 patients aged 22 to 57 years with IBS, Crohn’s disease, or constipation and 4 male donors aged 40 to 49 years with no antibiotic exposure in the 2 months preceding recruitment. Patients received various combinations of vancomycin, metronidazole, doxycycline, and rifampin for 5 to 10 days before FMT. Multiple infusions were administered daily for 5 to 15 days (mean = 9.1 ± 3.25 days). Fecal samples were collected at enrollment, evening before the procedure, and then 4, 8, and 24 weeks after completing infusions. A molecular approach, via polymerase chain reaction-denaturing gradient gel electrophoresis, was used to map the bacterial populations from patients’ and donors’ fecal samples. Similar to the previous study, posttransplant fecal samples showed marked similarity to healthy donors’ microbiota than patients’ own pretransplant samples. The restored microflora was largely stable for 24 weeks posttransplant with slight variations over time. 22 Despite lacking patients with CDI, the study offers an important observation of the efficacy and durability of FMT in reestablishing and maintaining the natural richness of colonic bacterial communities. Results of all 3 studies offer key clues to explain the theorized mechanism of action of FMT and its robust effect on the microbiota composition.
Clinical Efficacy
The published literature has shown FMT to be an effective and promising option for the treatment of recurrent CDI. In a recent study, 26 patients with recurrent CDI received FMT via colonoscopy. FMT was found to be simple, safe, and 92% effective in preventing CDI relapse. All patients included in this study had a least 3 recurrences of CDI, and all had been previously treated with metronidazole, Saccharomyces boulardii, and repeated tapering courses of vancomycin. 23
In January 2013, van Nood et al published the first randomized controlled trial (RCT) investigating the efficacy of FMT for recurrent CDI. Patients were randomly assigned to 1 of the 3 therapies, an initial high-dose vancomycin regimen (500 mg 4 times daily for 4 days), followed by bowel lavage and a subsequent infusion of donor stool via nasalduodenal tube; a standard high-dose vancomycin regimen (500 mg 4 times daily for 14 days); or a high-dose vancomycin regimen with bowel lavage. The primary end point was cure without relapse for 10 weeks. Due to the promising results, the study was closed to new enrollments only after 43 of the planned 120 patients were enrolled. Patients who received FMT had an 81% cure rate after the first infusion versus 31% in the vancomycin alone group (P < .001) and 23% in the vancomycin with bowel lavage group (P < .001). It is important to note that exclusion criteria in this study included patients who were receiving concomitant antibiotics for non-CDIs; had prolonged immunodeficiency due to recent chemotherapy, human immunodeficiency virus (HIV) with a CD4 count of less than 240, or use of prednisone at a dose of at least 60 mg/d; pregnant; admission to an intensive care unit; or need for vasopressor medication. Although these patients at high risk of recurrent CDI were excluded, the results of this study support the use of FMT as a standard alternative treatment modality. 24
Further review of the available case reports highlights the questions that need to be answered by future studies. A potential treatment consideration is whether the patient is infected with the C difficile ribotype 027 strain that has been linked to severe diarrhea and a higher relapse rate. 25 A recent retrospective study of 70 patients suggests FMT is effective in these patients as well. During the first 3 months after FMT, symptoms resolved in all the patients without the 027 C difficile strain. Of the 36 patients with the 027 ribotype, 89% had a favorable response. 26
Limited data on long-term response to FMT have also been published. A 91% primary cure rate and a 98% secondary cure rate have been shown in 77 patients with recurrent CDI who failed multiple treatment courses of metronidazole and/or vancomycin. This study demonstrated that 1 FMT may not restore the intestinal microbiome completely, and a second transplantation may be needed to fully restore the richness and diversity of the intestinal microbiome. 27 However, other literature suggests that the number of infusions given may not influence the outcome rates. 28
The literature also suggests administration technique of FMT can influence the response rate. Patients who have received FMT via a gastroscope or nasojejunal tube had the lowest resolution rate by route compared to enema or colonoscopy. 28 To note, the most recent studies on FMT have chosen colonoscopy as the route of choice. 23,26 However, studies that have administered FMT via nasogastric tubes have also shown success rates as high as 94%, 29 and a pooled analysis of case reports showed equivalent efficacy between FMT via colonoscopy and those via nasogastric tube. 30 Another consideration must be the fact that colonoscopy may not be possible in the severely ill. 31 A higher resolution rate (93%) has been seen when the donor was related (family members and spouses or partners) compared to when the donor was unrelated (84%). The volume of stool administered has also corresponded with a higher resolution rate, where greater than 500 mL has shown a 97% resolution rate compared with an 80% resolution rate when less than 200 mL was administered. 28
Interestingly, a recent proof-of-principle study has shown promising results with a synthetic stool mixture. Investigators developed “RePOOPulate” from purified intestinal bacterial cultures derived from a single healthy donor. This product was administered via colonoscopy to 2 patients with recurrent CDI who had failed at least 3 courses of metronidazole or vancomycin. Both patients were infected with the ribotype 078, an emerging hypervirulent strain that has been associated with community-acquired CDI. The results of the study were positive, as both patients returned to normal bowel patterns within 3 days and remained symptom free for 6 months. The proposed benefits of a synthetic stool mixture are the ability to control the composition of bacteria and the need to screen for viruses or other pathogens. 32 Ultimately, it is foreseeable that this method may replace the need for fecal donors. 33
Although the current literature has shown promising results, there have been no studies of FMT for prophylaxis and only 1 RCT to compare FMT with conventional treatments for CDI. However, the present evidence suggests that FMT may be a viable option for patients with multiple recurrences of CDI in order to prevent further recurrence. 34
Safety
In the studies reviewed that included protocols for FMT, donors were screened for both blood and stool pathogens prior to FMT. There was no standardized screening procedure identified. Common blood pathogens tested for included hepatitis A, B, and C viruses; HIV; and Treponema pallidum (syphilis). Stool pathogens screened for included C difficile, Shigella, Salmonella, Camplyobacter, Yersinia, ova, and parasites.
Of the studies reviewed, 7 reported no adverse events associated with FMT (Table 1). 23,35–40 In an RCT comparing FMT to vancomycin alone and vancomycin with bowel lavage, investigators reported no significant differences in adverse effects between the study groups. The majority of adverse effects reported in the FMT group occurred on the day of infusion and included diarrhea, belching, and abdominal cramping. In all patients, symptoms resolved within 3 hours. 24 In a study by Aas et al, investigators reported 2 deaths in 18 patients. One of the patients was undergoing peritoneal dialysis for end-stage renal disease and developed peritonitis 3 days post-FMT. The investigators could not exclude that the use of the nasogastric tube did not contribute to the patient’s death. The other death was due to pneumonia 14 days post-FMT. 29 In a study of 15 patients, administration of FMT via a nasogastric tube was well tolerated with 1 patient experiencing an upper GI hemorrhage thought to be due to the use of aspirin and nonsteroidal anti-inflammatory drugs rather than the FMT procedure. 41 Mattila et al reported no adverse effects in 70 patients. Four patients infected with the ribotype 027 strain did not respond to FMT and died within 3 months. There was no evidence that the death of these patients was associated with the FMT. An additional 10 patients died during the 1-year follow-up period due to unrelated illnesses. The investigators also reported no transmission of infection between donors and recipients. 26 In a study of 77 patients, Brandt et al reported no immediate adverse events. Two patients in the study associated FMT with an improvement in preexisting allergic sinusitis and arthritis. Four patients reported new medical conditions after FMT, which included peripheral neuropathy, Sjogren’s disease, idiopathic thrombocytopenic purpura, and rheumatoid arthritis. There were 7 patient deaths that were considered to be unrelated to FMT. 27 Based on the currently available literature, FMT does appear to be a safe alternative treatment option for recurrent CDI.
Summary of Safety Data of FMT.
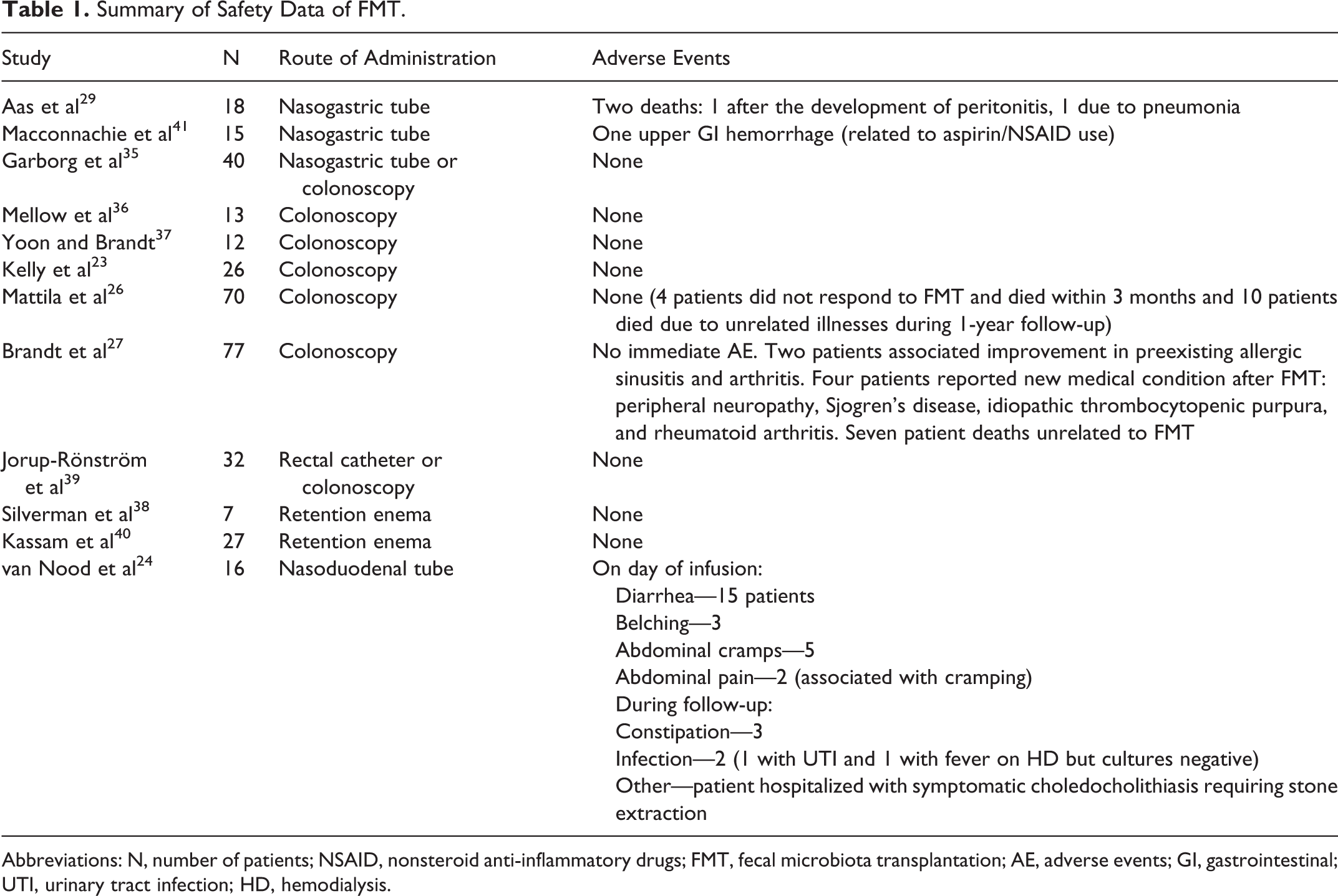
Abbreviations: N, number of patients; NSAID, nonsteroid anti-inflammatory drugs; FMT, fecal microbiota transplantation; AE, adverse events; GI, gastrointestinal; UTI, urinary tract infection; HD, hemodialysis.
Emerging Treatment Options
Monoclonal Antibodies
One question that is actively being studied is the role of antibodies against C difficile toxins A and B and the consequences when an individual is unable to produce an adequate amount of antibodies. Approximately 50% of the relapse incidents are due to reinfection with a different C difficile strain rather than the previously acquired strain, and relapsing disease has been shown to be unrelated to the acquisition of antibiotic resistance. Therefore, there is a strong belief that insufficient immune response gives rise to symptomatic illness. Furthermore, the possibility of manipulating host immune response with passive immunization is starting to peak investigators’ interest. 42
The role of toxins in disease has increasingly intrigued investigators of C difficile. Purified toxin A has potent enterotoxic and proinflammatory activity in addition to being cytotoxic. Toxin B does not have enterotoxic activity in animals, but it is a more potent cytotoxin. Studies are primarily in animals, but they have shown that toxin A is lethal to mice and hamsters while toxin B is not. However, they appear to act synergistically together, and it appears that strains that exhibit only toxin B are still able to cause intestinal symptoms in humans. 42 These toxins appear to be heavily produced in hypervirulent strains and absent from nontoxigenic strains. 43 Thus, the most promising studies have administered antibodies directed against both toxins A and B.
Randomized control trials have found monoclonal antibodies to be comparable to metronidazole in preventing recurrence. A notable phase II randomized, double-blind, placebo-controlled trial showed promising results. 44 One fully human monoclonal antibody targeted against C difficile toxin A (CDA1) and a second against toxin B (CDB1) were developed. The primary end point was first episode recurrence, and secondary end points included the number of days to resolution of the initial episode, severity of the initial episode, and failure of antibiotic treatment. From 30 participating centers, 200 patients were included, and all patients received standard-of-care antibiotics to treat C difficile. Only 7% in the antibody group had a recurrence of CDI compared to 25% in the placebo group (P < .001). Another significant result that favored the antibody group included time to recurrence. However, there were no significant differences in the severity of diarrhea during the initial episode, the median or mean number of days to resolution of the initial episode, or the portion of patients in whom treatment failed when comparing the placebo group and the antibody group. All adverse effects were mild to moderate in nature, with headache being the most frequently reported. 44
Interestingly, high levels of serum antibodies do not seem to guarantee protection from recurrence. Although significantly fewer patients in Lowy et al’s study who received the antibody had recurrence of CDI, there were some patients with high serum levels of neutralizing antibodies who had a recurrence. Therefore, serum levels may not always reflect adequate levels in the intestinal mucosa. 44 It has been shown that systemic antibodies do reach the gut, but the effect of antibodies on the development of cellular and humoral immunity is not yet fully understood. 45 In addition, low serum antibodies to toxin B has been significantly associated with recurrent CDI and higher serum antibodies to toxin B have offered protection from recurrent CDI. 46 Animal studies have shown an even stronger correlation between the level of antitoxin B antibodies than with the level of antitoxin A antibodies and the rate of recurrence. 47 However, in other animal studies, serum antitoxin B antibodies were unable to offer protection from the administration of lethal doses of toxin B, while a combination of antitoxin B and antitoxin A antibodies showed decreased mortality rate from 100% in the control group to 55% in the antibody group. 48
Another question yet to be fully answered regarding monoclonal antibody treatment for C difficile is its effect on the hypervirulent ribotype 027 strain. In animal models, novel monoclonal antibodies were also effective against the ribotype 027 strain. 43 More human studies are needed to further validate their efficacy.
Overall, the mechanism by which the development of systemic antibodies affects toxin-related disease in the colon is still unclear, but the association with a lower recurrence rate of CDI should not be ignored. This passive immunization may be ideal for groups of patients who are likely to have a recurrence. This is especially true for those patients who are unlikely to have an adequate response to active immunization. 49 Although intravenous immunoglobulin is another form of passive immunization, it is not known whether the commercial preparations actually contain C difficile toxin antibodies or if another type of antibody is responsible for apparent benefit. 1 Given the promising results already published in the literature, there is hope that current clinical trials will further elucidate the benefits that monoclonal antibodies will have against CDI. Currently, there are 2 phase III studies that are recruiting participants.
Clostridium difficile Vaccines
There are several issues that need to be addressed for the development of an effective vaccine for the prevention of both primary and recurrent CDI. These include appropriate antigen selection (eg, toxin vs nontoxin, toxoid or genetically engineered peptides, single-toxin antigen vs both toxin A and B antigens), systemic versus mucosal delivery, patient selection to demonstrate immune response and protection (eg, age, risk factors for CDI), and determination of duration of protection. 50 Vaccines for CDI have been in development for over 2 decades; however, their use and research in humans have been limited until recently. In November 2010, the United States Food and Drug Administration (FDA) granted fast track designation to an investigational C difficile vaccine. The FDA’s fast track program is designed to facilitate and expedite the development of new drugs and vaccines that are intended to treat or prevent serious diseases and fulfill an unmet medical need. This candidate vaccine is a formalin-inactivated, highly purified preparation of both toxoids A and B. It is a lyophilized formulation, reconstituted with diluent containing aluminum hydroxide as adjuvant and delivered intramuscularly. The proposed indication is for the prevention of CDI in patients with a planned hospitalization, long-term care or nursing home residents, and adults with comorbidities that require frequent or prolonged antibiotic use. 51 In March 2012, Greenberg et al published the results of 2 phase I, dose-finding studies of the investigational vaccine. A total of 50 healthy adult (18-55 years) and 48 elderly (≥65 years) volunteers were randomized to receive C difficile toxoid vaccine (2, 10, or 50 µg) or placebo on days 0, 28, and 56. Seroconversion for toxin A by day 56 was 100% for volunteers aged 18 to 55 years who received any dose and 50% (2 µg), 89% (10 µg), and 100% (50 µg) for elderly volunteers. Seroconversion for toxin B was lower in both the age groups. In volunteers aged 18 to 55 years, the seroconversion rate for toxin B appeared to increase with dose, and no volunteer who received placebo seroconverted. The investigators reported no deaths or vaccine-related serious adverse events. All volunteers aged 18 to 55 years reported at least 1 adverse event, the most common of which were injection site reactions and were more common in those who received the candidate vaccine. In volunteers aged ≥65 years who received the candidate vaccine, 97% reported at least 1 adverse event versus 83% in those receiving placebo. Injection site pain and erythema were more commonly reported in those volunteers who received the candidate vaccine compared to placebo. 52 Based on the data from phase I studies, 2 phase II studies using a dose of 50 µg or higher were initiated. One of the phase II studies has been completed, but results are pending. This study was designed to investigate the vaccine-based approach for prevention of recurrent CDI in recently infected patients. 51 There currently are at least 2 additional investigational vaccines recruiting for phase I studies.
Transplantation of Nontoxigenic C Difficile Strains
Colonization by nontoxin-producing strains of C difficile has been postulated as an alternative approach to protect against acute and recurrent CDI by toxigenic strains for over 25 years. Furthermore, primary asymptomatic colonization with C difficile—regardless of toxigenicity—was shown to have an association with decreased risk of developing CDI in 810 hospitalized patients followed up by prospective rectal swab culture. 53 In 4 animal studies, antibiotic-treated hamsters were harmlessly colonized with nontoxigenic strains of C difficile. Study animals subsequently exhibited significant protection and survival when challenged with toxigenic strains of C difficile. 54–57 In 1987, 2 patients aged 88 and 76 years with recurrent CDI were treated with 3 daily oral doses of a nontoxigenic strain of C difficile. Both the patients did not relapse following bacteriotherapy, and no adverse effects were noted. 58 In a recent phase I safety study in healthy human subjects, administration of single or multiple doses of an oral suspension of spores of a nontoxigenic strain of C difficile was compared to placebo for up to 28 days. Successful colonization was detected using stool cultures, and molecular typing was used to confirm the identity of the transplanted strain. No colonization was detected in the single-dose group, while successful colonization was detected at least once during study period in all the subjects who received multiple doses. Toxin-producing strains of C difficile were not detected during the 28-study period in the treatment group, while 5 (56%) of 9 subjects who received placebo tested positive for either toxin-negative or toxin-positive C difficile strains. No serious or severe adverse events were noted, and no subjects prematurely withdrew from the study. Reported adverse effects during study period included diarrhea, dyspepsia, abdominal pain and discomfort, constipation, flatulence, and gingival pain. 59 Currently, a phase II dosing and safety trial for prevention of recurrent infection in patients with CDI is underway.
Conclusion
Treatment of CDI continues to be a clinical challenge, especially in those patients with multiple recurrent episodes. Health care providers are seeking new and alternative treatments due to poor treatment outcomes with the current standard antibiotic therapy and the increased burden CDI has on the health care system. Based on the available evidence, FMT has been found to be safe and effective. Other emerging treatment options for CDI offer promising results. Preliminary clinical trials of monoclonal antibodies have shown clinically and statistically significant decreases in recurrence rate and time to recurrence. However, monoclonal antibodies may not have a significant effect on disease progression or resolution during the initial episode, leaving subsequent clinical trials to answer questions regarding their place in therapy. There are currently at least 3 vaccines for CDI under investigation. One of the vaccines has completed 1 phase II study, and results are pending. Transplantation of nontoxigenic strains is an intriguing approach that will require further validation in clinical trials.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.