
Abstract
Antimicrobial stewardship programs are essential to health care institutions to promote the appropriate use of antibiotics not only to decrease antimicrobial resistance but to prevent the spread and infection of Clostridium difficile. Clostridium difficile–associated diarrhea is increasing rapidly in the United States and is now considered a major public health problem that poses an immediate threat to the health of patients prescribed antibiotics, more so than antimicrobial resistance. Clostridium difficile–associated disease is the result of collateral damage to the normal bacterial flora of the human body, which is an inevitable consequence of any antibiotic use. Antimicrobial stewardship programs such as audit with feedback and antibiotic restriction are designed to help limit Clostridium difficile infections and other hospital-associated organisms by optimizing antimicrobial selection, dosing, de-escalation, and duration of therapy. These programs also incorporate implementation of hospital-wide guidelines, staff education, enforcement of infection-control policies, and the use of electronic medical records when possible to help control antibiotic use. This article reviews the literature on how antimicrobial stewardship programs impact Clostridium difficile rates and discusses experiences in designing, implementing, monitoring, and follow-through of such programs.
Clostridium difficile–associated disease (CDAD) is one of the leading hospital-acquired infections in the United States and has increased to historic highs. CDAD infections have been linked to approximately 14 000 deaths per year with an estimated increase of hospital costs of between US$897 million and US$1.3 billion. 1 Although many conditions have been associated with the increased risk of CDAD, the most common is the overuse of antimicrobial agents.
Antibiotic usage accounts for up to 30% to 50% of a hospital pharmacy’s nonlabor budget; therefore, controlling inappropriate antibiotic usage has become a major focus for many institutions. 2 At least 30% of the hospitalized patients are given an antibiotic, and these agents are inappropriate between 22% and 65% of the time. 3–5 Hecker et al 6 performed a retrospective evaluation of antimicrobial use in an inpatient setting in 2001. In a 2-week period, they found 30% (576 of 1941) of antimicrobial days of therapy (DOT) were inappropriate. More specifically, 33.3% (192 of 576) of inappropriate DOT were due to therapy that was continued longer than necessary, and 32.5% (187 of 576) of inappropriate use were for noninfectious or nonbacterial syndromes.
Clostridium difficile and Antimicrobial Use
Clostridium difficile is the causative organism of antibiotic-associated diarrhea and colitis. Colonization of the intestinal tract occurs via the fecal–oral route and is facilitated by disruption of normal intestinal flora due to antimicrobial therapy. The organism is capable of elaborating exotoxins that bind to receptors on intestinal epithelial cells, leading to inflammation and diarrhea. C difficile colonization primarily occurs in hospitals and long-term care facilities. Patients who become hospitalized and are prescribed broad-spectrum antibiotics are at an increased risk of this infection. Patients usually become colonized from unsanitary rooms, medical devices, or hospital personnel. However, if a patient becomes colonized, he may still not develop disease. In order for C difficile to flourish and cause disease, several factors need to be in place. Patients who are elderly, immunocompromised, and who are prescribed a broad-spectrum antibiotic have an increase risk of developing C difficile. However, any patient at any age or immune status is at risk when prescribed a broad-spectrum antibiotic, especially when the antibiotic is not necessary.
The reasons why broad-spectrum antibiotics contribute to C difficile infections are not fully understood. Most organisms within a host will not overgrow when other organisms are present (patient not on antibiotics) because of competition for host resources. For the most part, anaerobes prevent other anaerobes from overgrowth. It appears that the disruption of indigenous flora by antimicrobials, in particular drugs that cause major disruption of the anaerobic microflora (clindamycin, cefoxitin, and ceftriaxone [high excretion into intestinal tract]). However, many agents that cause minor disruptions of the anaerobic flora (trimethoprim-sulfamethoxazole and fluoroquinolones) have been associated with C difficile. 7 As a class, fluoroquinolones have poor in vitro activity against C difficile and anaerobes but seem to be associated with C difficile strains that are highly resistant to them. Beta-lactam/beta-lactam inhibitors combinations appear to be less strongly associated with CDAD, because they are highly active against many C difficile strains. 7
Antimicrobial Stewardship
The primary goal of an antimicrobial stewardship program (ASP) is to optimize clinical outcomes while minimizing unintended consequences of antimicrobial use, including the toxicity, the selection of pathogenic organisms, and the emergence of resistance. 8 A prominent pharmacy activity within the structure of a stewardship program is to closely monitor prescribed agents in order to avoid inappropriate antibiotics, duplicate therapy, and unnecessary lengths of therapy.
The concept of an ASP is designed to limit inappropriate antibiotic use while optimizing antimicrobial selection, dosing, route of administration, and duration of therapy. Tight control of antibiotics will optimize clinical cure or prevention of infection while limiting unintended consequences such as the emergence of resistant organisms and the development of C difficile–associated diarrhea. Strategies to limit the misuse of antibiotics are broadly divided into 2 models, prior authorization (formulary restriction or usage criteria) and antibiotic audit with feedback. 8 Antibiotic audit usually involves a pharmacist with infectious diseases (IDs) certification and/or training who reviews prescribed antibiotics and performs interventions as needed. 9 This model provides physicians with prescribing autonomy. It also eliminates the potential for a delay in therapy if an ID physician or if an ID pharmacist is not available to approve the antibiotics. In published surveys, physicians agreed that knowledge of antibiotics is important and that they would like more education and feedback on their antibiotic selections. Physicians also agreed that local guidelines are more helpful than national guidelines. 10–12 The prior authorization model involves a required approval of given antibiotics from either an ID physician or an ID pharmacist. In some situations, this model can lead to a delay in therapy, especially if the prescribing physician is unable to reach the ID personnel for approval in a timely fashion and the dispensing pharmacists cannot release the medication until approval is confirmed.
The Infectious Disease Society of America (IDSA) defines an ASP as a “rational, systematic approach to the use of antimicrobial agents in order to achieve optimal outcomes.” 8 The exact role of ASPs will vary from institution to institution, but the overall goals remain similar. There is no perfect ASP nor does the “one-size fits all” approach apply for any of these activities. As stated by Aldeyab et al, 13 one important aspect of developing an effective antibiotic-monitoring policy is the identification of the specific antimicrobial agents associated with the local issue (ie, CDAD) and then modify practice toward changing that outcome. The policy included both stewardship approaches, restricted the use of high-risk antibiotics (cephalosporins and fluoroquinolones clindamycin), and performed audit with feedback on lower risk antibiotics not included in the policy. As a result of this policy, C difficile rates were decreased from 1.5 cases/1000 bed days to 0.5 cases/1000 bed days during a 2-year time period.
Successful programs can be as varied as the institutions in which they are implemented and are limited only by the creativity of the people involved. Multiple elements will be required to create a successful program, and continual revision to those processes may be necessary to mature the program. Some elements that appear to be similar between productive stewardship programs include a prospective audit with feedback, formulary restrictions, antibiotic usage guidelines, staff education, de-escalation, and the use of electronic medical records (EMRs). 8 Depending upon individual capabilities and background, some of these activities can be combined to optimize outcomes.
ASP: Audit With Feedback
Audit with feedback is an essential part of any stewardship program. Auditing usually begins with an evaluation of the prescribing practices and the antibiotic delivery process by either the stewardship physician or the pharmacist, with the results of the audit reported to the institution and physicians. Depending upon the facility, evaluations can be either prospective or retrospective. Retrospective data can provide useful information regarding activities in the institution; however, these evaluations are more passive toward the physician and may result in delayed feedback and defensiveness, making modifications of practices more difficult. Prospective activities can have a more immediate effect due to the direct interaction between the physician and the stewardship program. The physician or pharmacist can provide interactive feedback and education to the prescriber on a case-by-case basis. This may alter future prescribing patterns but can be time intensive. This was the approach taken by Elligsen and colleagues 14 at their institution to control broad-spectrum antimicrobial use. All patients in the intensive care units who were receiving 3 days of broad-spectrum antibiotic therapy were evaluated by the stewardship pharmacist. Opportunities for optimization of care were identified and entered into a tracking database to determine the compliance of the responsible physician. As a direct result of these activities, monthly broad-spectrum use decreased from 644 DOT per 1000 patient-days to 503 DOT per 1000 patient-days (P < .001).
Another study that reported prescription audit with feedback was by Yam et al 15 in 2012. A clinical pharmacist, not ID trained, would review selected broad-spectrum antibiotics for appropriateness and make recommendations when necessary to the prescriber. In addition, the pharmacist would present the cases to the ID physician for review either as electronically or as weekly case presentations. Over 13 months from May 2010 to June 2011, 311 patient cases were reviewed. Antimicrobial costs from 2009 to the first 2 quarters of 2011 decreased from US$13 521 to US$6 583.52 per 1000 antimicrobial costs from 2009 to the first 2 quarters of 2011 decreased from US$13 521 to US$6583.52 per 1000 patient days, respectively. Additionally, hospital-acquired C difficile infection rates decreased from an average of 5.5 cases per 10 000 patient-days to an average of 1.6 cases per 10 000 patient-days.
De-Escalation
De-escalation of antibiotics is an important component of an ASP. De-escalation is defined as switching broad-spectrum antibiotics to narrower spectrum antibiotics as appropriate. De-escalation may be necessary once the patient’s diagnosis is confirmed, when empiric therapy is no longer necessary, or when final culture and sensitivity results are known. Once de-escalation criteria are developed, a member of the stewardship team should evaluate each patient individually. As necessary, a communication message can be left in the chart, or preferably, a direct interaction with the prescriber either via telephone (voice or text) or on medical rounds can be initiated by a pharmacist in order to discuss the de-escalation criteria. A problem with leaving notes in the chart is the inherent delay associated with this process as well as the need for follow-up by another member of the pharmacy staff. Physicians may hesitate to change therapy if the recommendation is different from their usual practice, or because the patient is improving. With continued effort and reporting, antibiotic prescribing will be improved; however, some inappropriate use is to be expected. The pharmacist who is either accepting antibiotic orders or monitoring antibiotic usage whose recommendation to de-escalate was not accepted by the prescribing physician should address de-escalation opportunities directly to the stewardship team leader who may then decide on further steps with the patient’s medical team. This approach may help in increasing de-escalation criteria compliance.
Antibiotic Restriction
Another antibiotic control strategy many organizations utilize is formulary restriction with preauthorization. Kallen et al 16 used this approach specifically to combat an outbreak of CDAD during 2006. Beginning in 2005, an increase in the rate of the North American pulsed-field gel electrophoresis type 1 strain causing CDAD was observed at their community hospital. After extensive evaluation, it was decided to completely restrict fluoroquinolones, since studies suggested this class of antimicrobials may be highly associated with an increased risk of CDAD. As a result of the restriction, they were able to demonstrate a significant change in the slope of hospital-onset CDAD trend (P < .001) during the time of the restricted medication, along with a significant decrease in the use of antimicrobial agents. Fluoroquinolone usage was decreased from 17.6 DDDs per 100 patient days to 6.0 DDDs per 100 patient days (P < .001).
The antibiotic restriction strategy was also implemented in a study by Muto et al. 17 As part of a comprehensive C difficile infection control bundle, they restricted the use of high-risk C difficile causative agents (clindamycin, Ceftriaxone, and levofloxacin) by requiring prior approval from an IDs physician or pharmacist. Before the initiation of the infection control bundle in 2000, the C difficile rate peaked at 7.2 infections per 1000 hospital discharges. Since then the rate has decreased to 3.0 infections in 2006 along with a 54% decrease in the CDAD-associated antimicrobials.
Antibiotic restriction as part of stewardship may be a useful tool. The institution selects specific agents that may be contributing to an outbreak or a change in resistance patterns and requires approval by specified individuals before the pharmacy can dispense the medication. This gives each hospital control over specific antibiotics; however, this can be a difficult process for hospitals to implement. To minimize delay in patient care, there must be someone available at all times for medication use review and approval. This may be difficult for smaller institutions and may even increase labor costs. Additionally, physicians may learn what is required for approval and manipulate the system to utilize the medication (eg, “yes, I’m concerned about Pseudomonas), bypassing the program and its potential benefits.
Hospital Wide Guidelines
Organizations may develop institutional-specific mediation guidelines for multiple disease states. Guidelines can be targeted for each individual hospital formulary, site of infection, patient population, and resistance patterns. With time and use, guidelines may help modify physicians prescribing patterns. Implementation of guidelines is similar in many ways to restricting antibiotics; the major difference is that approval is not required prior to having the medication dispensed. This approach was taken by Talpaert et al 18 in 2006. The goal of their plan was to implement narrower spectrum antibiotic guidelines throughout their institution in an effort to decrease rates of CDAD. Usage of agents regarded as “high risk” for causing CDAD was dispensed; however, a member of the ASP team was notified to ensure that the patient was evaluated. When prescribed medications fell outside of the criteria of the guidelines, the pharmacist would intervene and try to optimize patient care. As a result of these actions, the institution documented a statistically significant decrease in CDAD associated with the interventions as well as usage of targeted antimicrobials.
Hospital-wide guidelines were also implemented in a study by Valiquette et al 19 in 2006. In order to help control an epidemic of nososcomial C difficile infections in a tertiary care hospital in Quebec, they implemented a nonrestrictive ASP and local treatment guidelines, which focused on decreasing the use of antibiotics most commonly associated with CDAD (cephalosporins, ciprofloxacin, clindamycin, and macrolides). Their results not only showed a marked decrease in total antibiotic use by 23% but also showed a decrease in targeted antibiotics by 54%, their incidence of nosocomial CDAD decreased by 60% over a 3-year period. Although the implementation of guidelines requires less resources than restrictions (as described previously), guidelines require continual reevaluation and maintenance by the stewardship team to ensure they stay current with the resistance patterns of the hospital and reflect the consensus of experts in the specific disease area.
Staff Education
One element of stewardship programs, which is underappreciated in many institutions, is education. The IDSA guidelines 8 consider education essential for influencing prescribing behavior in conjunction with other elements as described. Stewardship team members need to understand the use of antimicrobials and be well versed in the current medical literature. In turn, these ASP team members must educate the prescribers of their health system. Practitioners who understand the underlying issues and concerns appear to be more willing to modify behavior than those just being forced to change by policies and regulations. Education to health care workers can be as varied as the stewardship programs themselves. Some institutions find teaching sessions useful, whereas others utilize posters and pocket-card reminders. 17,18,20 Face-to-face discussions may prove to be the best to collaborate with certain practitioners, or communication through chart documentation is appropriate for others, whereas those with computer physician order entry systems (CPOEs) or EMR may utilize electronic resources to update the prescribers. 14,18,21 Regardless of the type, the educational component of an ASP seems to be beneficial for the long-term modifications of prescribing patterns. It should be emphasized, however, that education alone is an inadequate modality for sustained improvement in antibiotic usage. Rather, it must be combined with other ASP steps enumerated in this article.
Electronic Medical Record
The use and monitoring of compliance within a health care system is becoming more feasible, as institutions implement EMR and CPOE. The use of electronic resources as part of the ASP contributes significantly to decreases in overuse of antibiotics as reported by Cook et al. 21 This study reported that when the EMR was implemented, the stewardship pharmacist was able to increase the number of charts reviewed, increase clinical recommendations, and increase the number of recommendations accepted by 36.6%, 98.1%, and 124%, respectively (P < .0001). The study also demonstrated that decreased antimicrobial use resulted in decreased rates of CDAD to 18.7% and hospital-acquired methicillin-resistant Staphylococcus aureus (MRSA) fell to 45.2% since the implementation of the EMR. The electronic systems may allow for more patients to be evaluated, and interventions made in a shorter length of time, resulting in better overall care for the patient.
An example of a fully integrated EMR is at Lincoln Medical Center, a 400 bed inner-city hospital that has over 125 000 emergency department (ED) visits per year, 25,000 admissions per year, and over 350 000 outpatient clinic visits per year. CPOE has been available since 2000, and fully EMR was initiated in 2005. Also, automated dispensing machines were placed throughout the facility in 2003. This type of technology allows for changes in prescribing practice such as automatic stop orders for all medications between 3 and 7 days, implement treatment protocols within the order entry screen, and insert appropriate typical doses and dose adjustments based on the renal function. All notes, consults, clinic notes, ED notes, medications, laboratory values, imaging, and microbiology are online, which allow for faster review of patient charts. In addition, pharmacists can write an electronic pharmacotherapy note (intervention documentation) for inpatients that populate within the daily medical notes section of the EMR.
ASP Implementation
In order to implement an ASP, the stewardship team must address the specific needs of the individual institution, be built on available resources, adhere to the limitations and advantages of each institution, and have both the available staff and the technological infrastructure. 22 Following support from senior leadership and administration, an ASP model can be accomplished by identifying patients receiving inappropriate therapy and effectively communicating with prescribers. The ASP model should also be able to recognize hospital-wide prescribing issues in order to modify current and future prescribing with education and guideline implementation. An advisable step before formal development of any program is to retrospectively evaluate the institution and determine where problems exist, for example, by performing a drug-utilization evaluation on the most commonly prescribed broad-spectrum antibiotics to determine appropriateness of use. This aspect can be especially important when determining the cause of a CDAD outbreak.
Once institution-specific problems have been identified, it is necessary to evaluate potential causes of those problems. An unbiased process evaluation may demonstrate current practices and policies that may enable physicians to unwittingly contribute to inappropriate antibiotic use. For example, at University Medical Center of Southern Nevada (UMCSN) in Las Vegas, institutional process evaluation found that many antibiotic treatment courses extended beyond the recommended standard length. 23 Upon further investigation, it was determined that automatically generated medication renewal forms being provided to the physicians were greatly contributing to the excessive antibiotic duration. The UMCSN policy at the time was to have the pharmacy computer system automatically generate the forms, and that they be placed in the chart 48 hours prior to the expiration of any medication order. As a convenience, the physician could choose to “renew” or “DC” that medication rather than having to write a new order. When audited, it was found that in many instances, all medications were being renewed regardless of continued need. Once discovered, the policy was modified to exclude antimicrobial agents from these renewals. Currently, the pharmacy computer system generates a notification for the physician that the antibiotic order is approaching 10 DOT and will automatically discontinue unless a new order is written. This policy change has decreased the average antibiotic length of time from between 16 and 20 days to an average of 13.3 days. 23 Although not specific to CDAD, decreased inappropriate use of antibiotics by shortening duration may minimize development of all hospital-associated pathogens.
Inner City ASP Program
Since 2002, Lincoln Medical Center has recognized the importance of the rational use of antibiotics. Lincoln employs full-time in-house physicians for all areas of medicine and surgery. This helps to promote the rational use of antibiotics whereby hospital-wide prescribing issues can be addressed and discussed directly with the in-house staff. The ASP began in the first half of fiscal year 2004. The implemented ASP at Lincoln incorporates many of the features of the antimicrobial management team concept as described and reported by Carling et al in 2003. 24 A clinical pharmacist who specializes in ID was hired to implement this program who is responsible for evaluating patients prescribed broad-spectrum antibiotics and making recommendations with the patients physician or with an ID physician. This study reported a decrease in the incidence of C difficile from 2.2 cases per 1000 patient-days to 1.4 cases over 2 years. The study also reported an 18% decrease in overall antibiotic expenditures over 4 years, where most of the savings were related to the use of less costly drugs with little reduction in overall antibiotic usage.
The implemented ASP at Lincoln Medical Center follows the model of prescription audit with feedback. All broad-spectrum antibiotics are identified via a daily antibiotic report and are concurrently monitored for appropriateness. Monitoring only a selected group of antibiotics may result in an increase in the use of unmonitored antibiotics. 4 The antibiotic report is reviewed daily for appropriate antibiotic selection based on the dose, indication, antibiotic length of therapy, empiric therapy, streamlining therapy, unnecessary antibiotics, and culture and sensitivity. Once antibiotic issues are recognized, an intervention is performed either immediately via telephone or discussed on IDs rounds or on internal medicine rounds; the intervention is then documented in the medical record.
Pharmacist rounding daily with the ID team or internal medicine teams not only helps to build strong relationships with the medical team but also allows for real-time discussion on interventions as well as education. The ID pharmacist should understand specific IDs states and be able to help choose the best regimen for the patient. Pharmacy presence on the medical floors greatly improves efficiency and timeliness of antibiotics administered to the patient by addressing potential issues immediately.
Outcomes
Since the implementation of the program in FY04, there has been many antibiotic interventions and prescribing trends addressed over the years. The various recommendations made by the stewardship team more than likely lead to decreases in rates of hospital onset organisms such as C difficile, MRSA, and Klebsiella. Although there is no specific intervention data to show, most of the stewardship interventions were to discontinue antibiotic therapy that decreases cost, antibiotic usage, C difficile rates, and length of therapy. Increasing lengths of therapy of mostly any antibiotic probably plays a strong role in increasing C difficile rates, which was reported in a study by Pepin et al. 25 This study showed that increased duration of therapy of most classes of antibiotics correlated with an increased adjusted hazard ratio of developing C difficile. Fluoroquinolones at 4 to 6 DOT and at 7 days or greater of therapy had the highest adjusted hazard ratios for developing C difficile compared to all other antibiotics studied.
Lincoln Medical Center showed a 60% decrease in overall antibiotic spending, see Figure 1. The majority of the decreased spending is related to recommendations based on the discontinuing therapy and the use of narrower, less costly antibiotics. Lincoln’s patient admit day per year decreased from 94,427 in FY03 to 81,441 in FY11, a 13.7% decrease, while admissions to medicine increased from 10,195 in FY03 to 13,165 in FY11 and antibiotic cost/pt day decreased 35% (Figure 2). In addition, patient’s average length of stay decreased from 4.77 days in FY03 to 3.55 days in FY11, a 26% decrease.
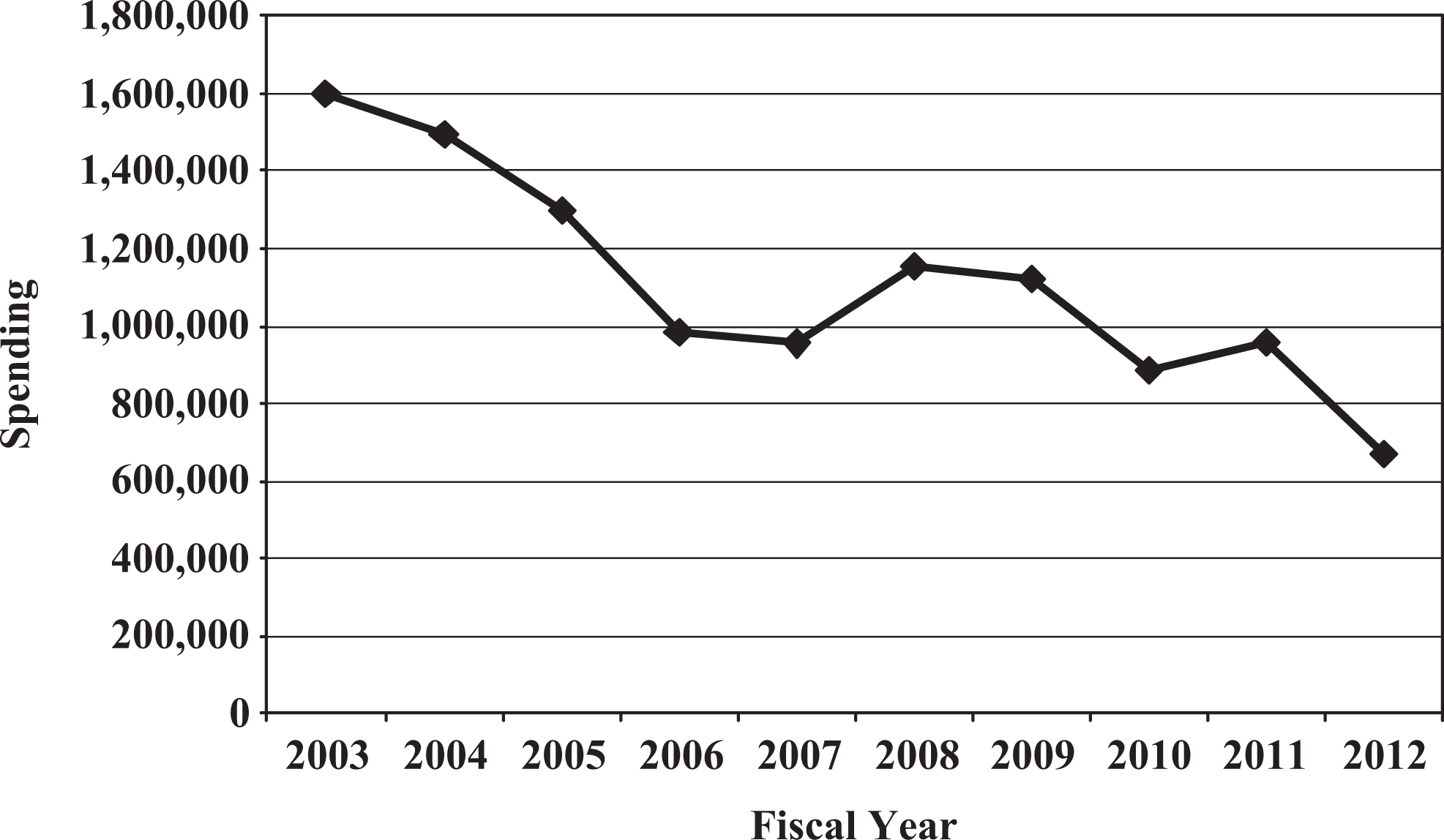
Anti-infective fiscal year spending.
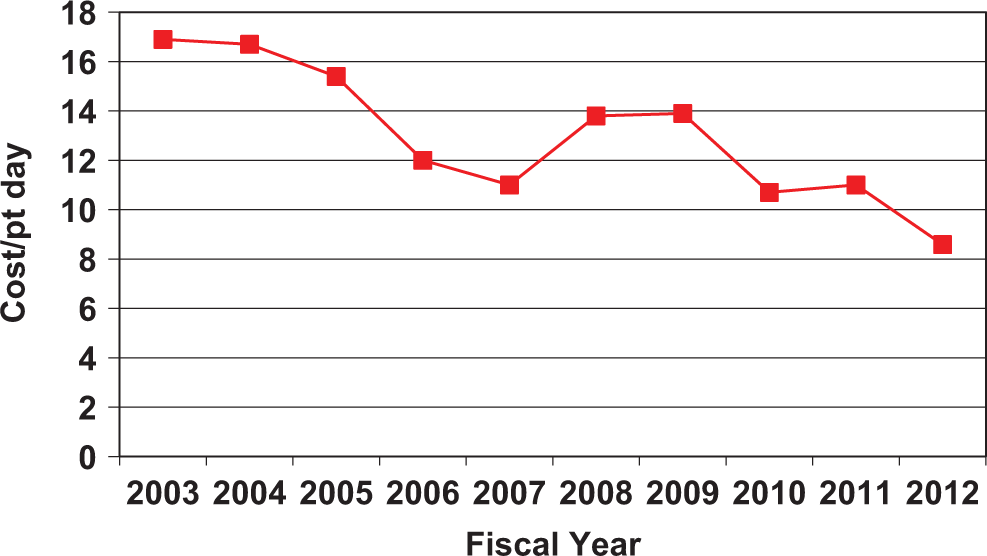
Total antibiotic cost per patient day. Patient day data include all patients admitted to medicine, intensive care unit, surgery, pediatrics, and gynecology.
Antibiotic cost/Usage data
Figures 3 and 4 show the most common antibiotics prescribed with the number of completed doses given to patients. The first drug-specific challenge noted was the unrestricted use of imipenem in FY04. This antibiotic was heavily monitored at the onset of the program, and the number of doses used from FY03-04 decreased by 2000 doses. In FY09-10, the use of imipenem increased due to the increase in suspected extended-spectrum beta-lactamase (ESBL) Klebsiella infections, although the actual rates of ESBL Klebsiella infections decreased from 9.8% in 2006 to 6.1% in 2012. Vancomycin usage remained constant from FY03-06, but in the following years, its use increased due to the increasing rates of CA-MRSA skin and soft tissue abscess while MRSA bacteremias decreased from 13.3% (67 of 501) in 2004 to 3.2% (38 of 1188) in 2010, and hospital-acquired MRSA rates decreased from 28% (55 of 196) in 2004 to 4.7% (27 of 577) in 2010. No other agents for MRSA are used in significant amounts, because Lincoln has established strict MRSA guidelines.
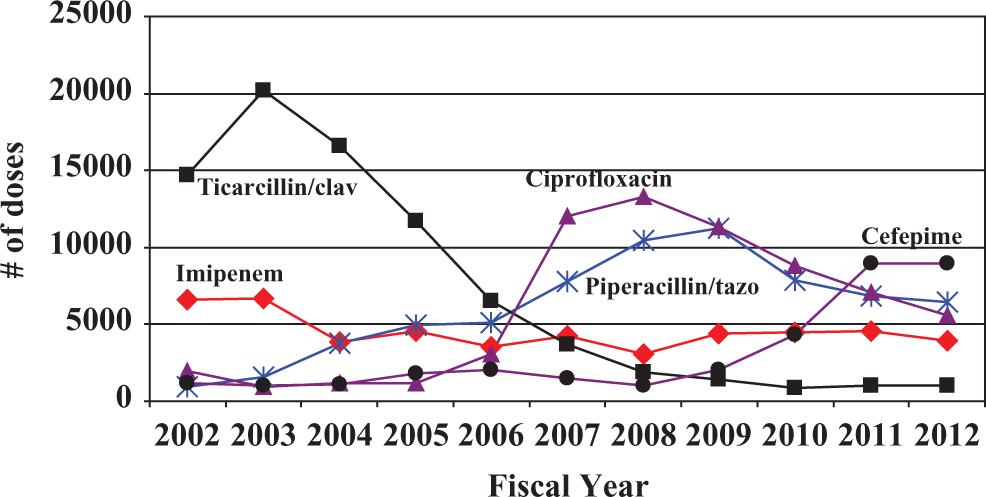
Antibiotic usage per fiscal year.
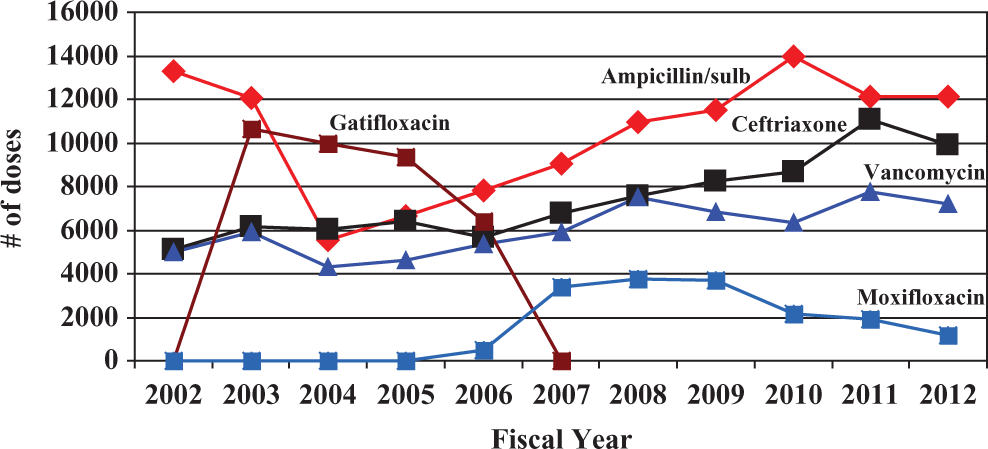
Antibiotic usage per fiscal year. In FY 2006, Lincoln switched from gatifloxacin to moxifloxacin as the flouroquinlone of choice.
Another antibiotic-specific challenge encountered was the use of ticarcillin/clavulanate. Since its use peaked in FY04, tighter control was implemented, and its use decreased significantly between FY05 and FY06. In FY06, a new health care-associated pneumonia (HCAP) guideline was published. From 2006 to 2009, the use of piperacillin/tazobactam increased substantially due to the new terminology for patients with pneumonia. In FY09, the stewardship team recommended cefepime for its HCAP patients rather than piperacillin/tazobactam. This switch was incorporated into the hospital’s pneumonia guideline, which represented a significant cost savings (US$15 per day for cefepime compared to US$60 per day for piperacillin/tazobactam). In addition to cost savings, this switch resulted in a decrease in empiric anaerobic coverage of patients who for the most part do not need broad anaerobic coverage. This switch may have played a role in decreasing C difficile rates. The new HCAP guideline also resulted in an increased use of ciprofloxacin for double coverage in combination with piperacillin/tazobactam. The stewardship team saw a rapid increase in the number of doses of ciprofloxacin from 2000 doses in 2006 to 11 000 doses in 2008. The ASP team then recommended against the use of double coverage in 2009, and the 2010 ciprofloxacin doses decreased to 3000.
Other cost saving/appropriate usage changes included the appropriate dosing of ceftriaxone and ampicillin/sulbactam. In FY04, most prescribers were prescribing a 2-g dose of ceftriaxone instead of the 1 g dose (Figure 5). In FY05, a recommendation was implemented to use ceftriaxone 1 g for most indications including pneumonia. Similarly, in FY05, a recommendation was implemented to use ampicillin/sulbactam 1.5 g for most indications rather than the 3.1 g. Since these recommendations were implemented, there was an increase in the usage of the lower dose antibiotic and a decrease in the usage of the higher doses. In both of these cases, the lower dose is about half the cost of the higher doses. Most infections can be treated with the lower doses without compromising patient care except for in patients diagnosed with meningitis or osteomyelitis, which require the higher doses for penetration purposes. With the increase in ceftriaxone use since 2005 as the primary agent for community-acquired pneumonia, there was a substantial decrease in the respiratory fluoroquinolone use from 9980 doses in 2005 to 1152 doses in 2012 which may also contribute to lower C difficile rates.
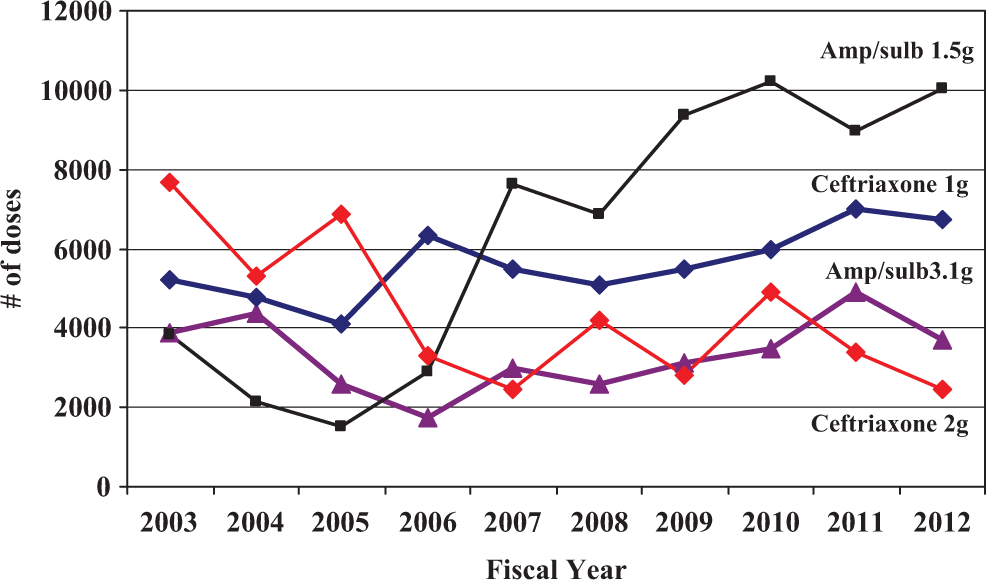
Ceftriaxone and ampicillin/sulbactam usage.
Microbiological Data
Although CDAD is one of the most common hospital-onset infections nationally, Lincoln Medical Center seems to be consistently below the national average rates. The average rate at Lincoln over the last 7 years is 2.6 cases/10,000 patient days (Figure 6) compared to the national rate of 7.4 cases per 10,000 patient days. 1 In fiscal years 2007 and 2008, Lincoln saw a dramatic increase in the use of ciprofloxacin (Figure 3). There may have been an association between this increase in ciprofloxacin usage with the increase in CDAD rates, 3.6 cases/10,000 patient days in 2007 and 3.9 in 2008. Once this issue was addressed and guidelines were implemented, in FY2009, ciprofloxacin usage began to decline from its peak, and the rates of CDAD decreased to 2.2. Usage of ceftriaxone has increased at least 50% from 2005 to 2012, but CDAD rates did not change in parallel.
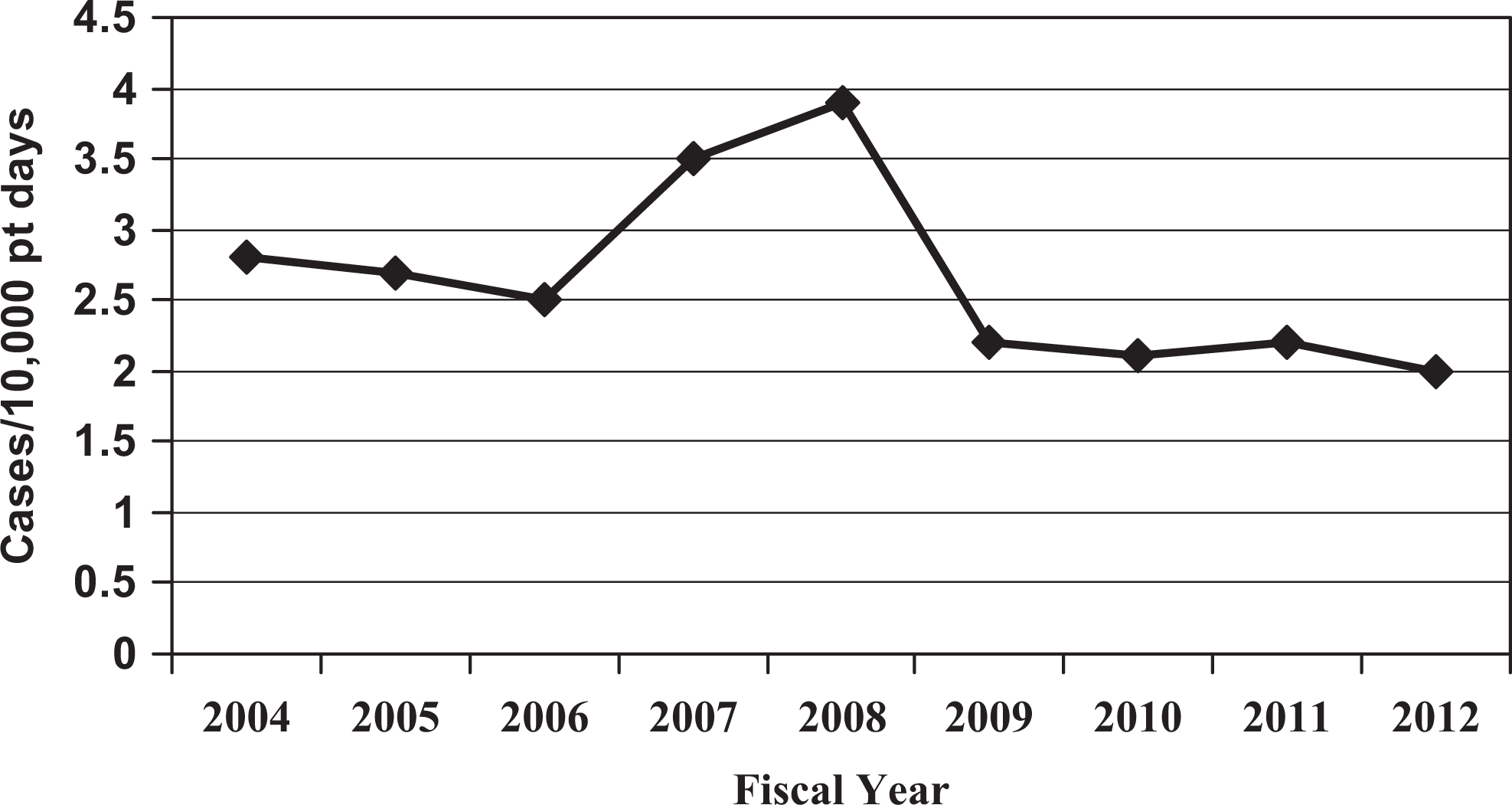
Hospital-associated Clostridium difficile rates.
Infection Control Departments
Although the described elements of stewardship programs appear straightforward, there must be a collaborative effort of multiple disciplines. The department of Infection Control and Prevention must be an intricate part of the stewardship program primarily in the role of prevention. An institution can put together pages of regulations and restrictions to control prescribing patterns and overuse of medications, but without a strong infection control program, the organisms can and will continue to spread and colonize the establishment. With an organism such as C difficile, prevention of spread throughout the institution must always be a priority for day-to-day operations and to control outbreak situations. Several institutions have published experiences in regard to control of CDAD outbreaks utilizing strict infection control practices. 17,26 Each of these reports have multiple processes in common including isolation of patients, appropriate hand hygiene with soap and water, and enhanced environmental cleaning with appropriate compounds (ie, bleach). Both the studies demonstrated a decrease in the rates of CDAD, but neither could specifically state the improvements were due to infection control activities alone. Combined with the enhanced infection control prevention measures, ASPs may have also contributed to the overall success of decreasing CDAD rates.
Conclusions
Antimicrobial stewardship can be a useful tool for an institution in its fight against CDAD. Although many individuals think “stewardship” is a fancy way of saying “controlling” antibiotics, in reality it is a broad phrase for all activities institutions perform, develop, and implement with the aim of decreasing inappropriate antibiotic utilization and preventing or controlling hospital-associated diseases such as CDAD. There are as many types of stewardship programs as there are hospitals and health care organizations. Studies have demonstrated that ASPs work in a variety of settings. Studies have also demonstrated that no single activity will optimize poor prescribing habits, improve susceptibilities, or control for the development of CDAD in a health care system. Improved prescribing, monitoring, and analysis of data require a concerted effort by a multidisciplinary team to investigate, evaluate, and develop a continually evolving action plan that will make antimicrobial stewardship a successful instrument toward the elimination of CDAD.
Stewardship programs do not always demonstrate positive results as they must show and identify unwanted results in order to make changes in prescribing practices. Antibiotics will always be required in sick patients within any institution, so cost savings and decrease in usage will have its limits. With the continued efforts of an antimicrobial stewardship team, any changes in prescribing patterns should be monitored and discussed with pharmacy, leadership, and physicians. Change takes time but in the long run, documentation, monitoring, education, guidelines, and close follow-up of the most appropriate use of antibiotics will demonstrate the most efficient way to prescribe antibiotics.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.