
Abstract
Background:
Medication use in the intensive care unit (ICU) depends on creatinine-based glomerular filtration rate (GFR) estimates. Urine output deterioration may precede the creatinine rise resulting in delayed recognition of GFR reductions. Our objective was to quantify the disparity between estimated GFR (eGFR) and true GFR in ICU patients with hospital-acquired oligoanuric acute kidney injury (hAKI).
Methods:
This single-center cohort study examined adults who met the Acute Kidney Injury Network stage III urine output criterion ≥48 hours after ICU admission. True GFR was ≤15 mL/min/1.73 m2, and eGFR was described by 6 different creatinine-based equations. True GFR and eGFR were compared on the day of hAKI diagnosis and followed for 4 days using multivariable linear regression with generalized estimating equations, adjusting for day and method.
Results:
Of the 691 patients screened, we enrolled 61 patients. After adjustment for multiple comparisons and day, there were significant differences in eGFR between the estimation methods and true GFR (P < .001). After day adjustment, eGFR overestimated true GFR by 17 to 50 mL/min/1.73 m2 and overestimation persisted through the fourth day of hAKI (P ≤ .001).
Conclusion:
Creatinine-based equations overestimated GFR in ICU patients with hAKI. This study highlights a population at risk of medication misadventures in whom systems optimization should be considered.
Background
Hospitalized patients with renal dysfunction are at high risk of adverse drug events. In a study of patients with estimated creatinine clearances <80 mL/min, only one-third of medications ordered electronically were at the appropriate dose and frequency for the degree of renal dysfunction. Although incorporation of guided dose algorithms into computerized physician order entry (CPOE) significantly improved error rates, nearly half of the medication orders remained inappropriate at the conclusion of this study. 1 In the intensive care unit (ICU) in particular, treatment decisions depend on early identification of acute kidney injury (AKI) and accurate assessment of glomerular filtration rate (GFR). Inaccurate interpretations of renal function in this setting contribute to adverse drug events, which negatively impact patient care and health care costs. 2 The risk/benefit analysis of exposure to agents such as intravenous contrast or nephrotoxic antimicrobials hinges on timely and accurate assessment of an ICU patient’s renal function. 3 Also, renal dysfunction may precipitate dangerous toxicities associated with many common ICU medications, including, but not limited to anticoagulants, anti-infectives, analgesics, sedatives, and paralytics. 3 –7
Although the existing definition of AKI depends on both the serum creatinine concentration and urine output, the calculated GFR estimate typically utilizes only creatinine. 8 Oliguria often precedes the serum creatinine rise and consequently may herald an opportunity for earlier diagnostic and therapeutic optimization not readily identified by an isolated evaluation of creatinine. 9,10 The present logic imbedded in clinical decision support tools such as CPOE, hospital rule-based systems, and automated calculations hinges medication dose recommendations on creatinine. 11,12 Unfortunately, the degree and duration of GFR overestimation by creatinine-based estimates in ICU patients whose true GFR is low, as indicated by urine output, remain unknown. Therefore, the purpose of this study was to evaluate the GFR predictions of 6 creatinine-based equations in critically ill patients with new onset sustained oligoanuric AKI ≥48 hours after ICU admission (hospital-acquired AKI [hAKI]) who have a lag in creatinine rise. 13
Methods
Subject Identification and Data Collection
This retrospective cohort study examined adult ICU patients at a single academic medical center who developed hAKI between January 2006 and June 2011. The institutional review board approved the protocol and waived the need for informed consent for the retrospective evaluation of existing medical records. Included patients experienced urine output ≤0.3 mL/kg/h for ≥24 consecutive hours or anuria in 12 consecutive hours, consistent with the Acute Kidney Injury Network (AKIN) stage III urine output criterion ≥48 hours after ICU admission. 8,14 Evaluation for hAKI began at the time of ICU admission due to inconsistent documentation of urine output in noncritically ill ward patients at the institution. Excluded individuals experienced any stage of AKI or required renal replacement therapy (RRT) within the first 48 hours of ICU admission, did not have an indwelling urinary catheter, or had a history of end-stage renal disease or renal transplantation. Individuals retain the opportunity to opt out of minimal risk retrospective research, and those who did were also excluded from the study. CPOE, automated renal function calculations, dose recommendation pop-ups, and rule-based prompts for renal dose adjustments were consistently available and unchanged throughout the study timeframe. Outcome analysis included only the first ICU admission for each patient during the study timeframe.
Derivation of True GFR
Given the inability to retrospectively apply a gold-standard measure of GFR, 2 methods were used to determine the true GFR of patients, in general, who meet the AKIN stage III urine output criterion. First, after obtaining informed consent, we prospectively conducted 8-hour urine creatinine clearances in 4 similar nonincluded ICU patients with stage III AKI. The calculation for urine creatinine clearance (mL/min) used was (Creatinineurine [mg/dL] × volume of urine [mL])/(Creatinineserum [mg/dL] × Collection time [hours] × 60). The serum creatinine ranged from 1.5 to 3.7 mg/dL, urine output was between 0.12 and 0.18 mL/kg/h, and the median calculated clearance was 11 mL/min (range 7-17 mL/min). Second, we queried 14 international experts with demonstrated scholarly contribution to AKI and GFR literature. All respondents were affiliated with academic medical centers and the majority had 10 or more years of practice experience with greater than 50% of their activities devoted to direct patient care. The survey used the Delphi technique to reach the consensus that the true GFR of patients who meet the AKIN stage III urine output criterion (urine output less than 0.3 mL/kg/h for 24 hours or anuria for at least 12 hours) is ≤15 mL/min/1.73 m 2 . It is based on these 2 similar results that the true GFR for comparison in the present study was set at 15 mL/min/1.73 m 2 for included patients.
Data Collection
Collected data pertained to patient demographics (age, sex, race, actual body weight [ABW], ideal body weight [IBW], body mass index [BMI], body surface area, comorbid conditions) and severity of illness (Acute Physiology and Chronic Health Evaluation III [APACHE III], Sequential Organ Failure Assessment [SOFA]). Other gathered information included admission diagnosis, presence or absence of shock and its type, need for vasoactive support, and mechanical ventilation. Concurrent medications that could interfere with the renal tubular secretion of creatinine were collected (ie, trimethoprim, cimetidine, and probenecid). Although these agents are rarely used in modern ICUs, they could artificially increase serum creatinine concentrations and lead to underestimation of true GFR by creatinine clearance.
Baseline serum creatinine was the most recent available value within 6 months preceding hospital admission or as documented in the electronic medical record by a board certified nephrologist. 15 Renal parameters were collected daily from onset of hAKI (day 0) until ICU discharge, recovery of urine output, initiation of RRT, or death (when available) up to a maximum of 7 days (days 0-6).
Physician order priority (stat or routine) dictated the specimen type collected (plasma or serum) for creatinine measurement, which was performed using the Roche enzymatic creatinine assay on either Roche Modular Analytics (D module) or Cobas 6000 c501 chemistry analyzers for serum samples and the Roche Cobas Integra 400 Plus chemistry analyzer for plasma samples (Roche Diagnostics, Indianapolis, Indiana). The analytical measurable range for the enzymatic creatinine assay was 0.4 to 27.0 mg/dL for the Integra 400 analyzer and 0.1 to 23.0 for the other Roche chemistry analyzers (×4 dilutions allowed). In patients with an active order for intravenous catecholamines, a rule-based process prompted a change to the Roche Jaffe creatinine assay (Roche Cobas Integra 400 Plus chemistry analyzer) that has an analytical measurable range of 0.4 to 15 mg/dL.
End Points
True GFR based on urine output was compared to 6 existing creatinine-based estimated GFR (eGFR) equations: Cockcroft-Gault with actual body weight (CG-ABW), Cockcroft-Gault with ideal body weight (CG-IBW), Jelliffe, Modified-Jelliffe, Modification of Diet in Renal Disease (MDRD), and Chronic Kidney Disease Epidemiology Collaborative (CKD-EPI; Table S1
Data Analysis
A sample size of 48 patients was necessary to detect a 5 ± 12 mL/min/1.73 m 2 difference among 2 estimates with 80% power using a paired t test with a 2-sided significance level of .05 (nQuery Advisor Version 6.0; Statistical Solutions, Cork, Ireland). 15,21 Descriptive data were summarized by medians with interquartile ranges (IQRs; 25th and 75th percentiles) and counts (percentages). Due to patient attrition over time associated with discharge, RRT, recovery or death, analyses were performed from day 0 through day 3, instead of through study day 6. Comparisons of GFR were made using multivariable linear regression with generalized estimating equations, adjusting for day and estimation method. Tukey-Kramer adjustment was used for multiple comparisons between equations. All analyses were performed using SAS v9.2 (SAS Institute Inc, Cary, North Carolina). All tests were 2 sided, and P values less than .05 were considered statistically significant.
Results
Patients
Of the 691 patients screened, 61 patients with hAKI met inclusion criteria. Primarily, excluded patients developed AKI <48 hours from ICU admission based on serum creatinine (N = 194; 31%), required continuous RRT within 48 hours of ICU admission or prior to the development of oligoanuria (N = 177; 28%), or did not develop AKI during the ICU stay (N = 137; 22%). The included patients were mostly caucasian (77%) with a median age of 63 years (IQR 48-73) and evenly distributed between males and females. Nonoperative indications comprised the majority of admission diagnoses (62%), and there was a high severity of critical illness reflected in the proportion of patients with shock (51%) and APACHE III and SOFA scores of 64 (54-89) and 7 (5-10), respectively (Table 1). Obesity occurred commonly with 43% of patients possessing a BMI ≥30 kg/m 2 and a median difference between ABW and IBW of 28 (14-50) kg. 16 Past medical history of cancer and end-stage liver disease arose infrequently (21% and 15%, respectively).
Baseline Patient Characteristics and Demographic Data.
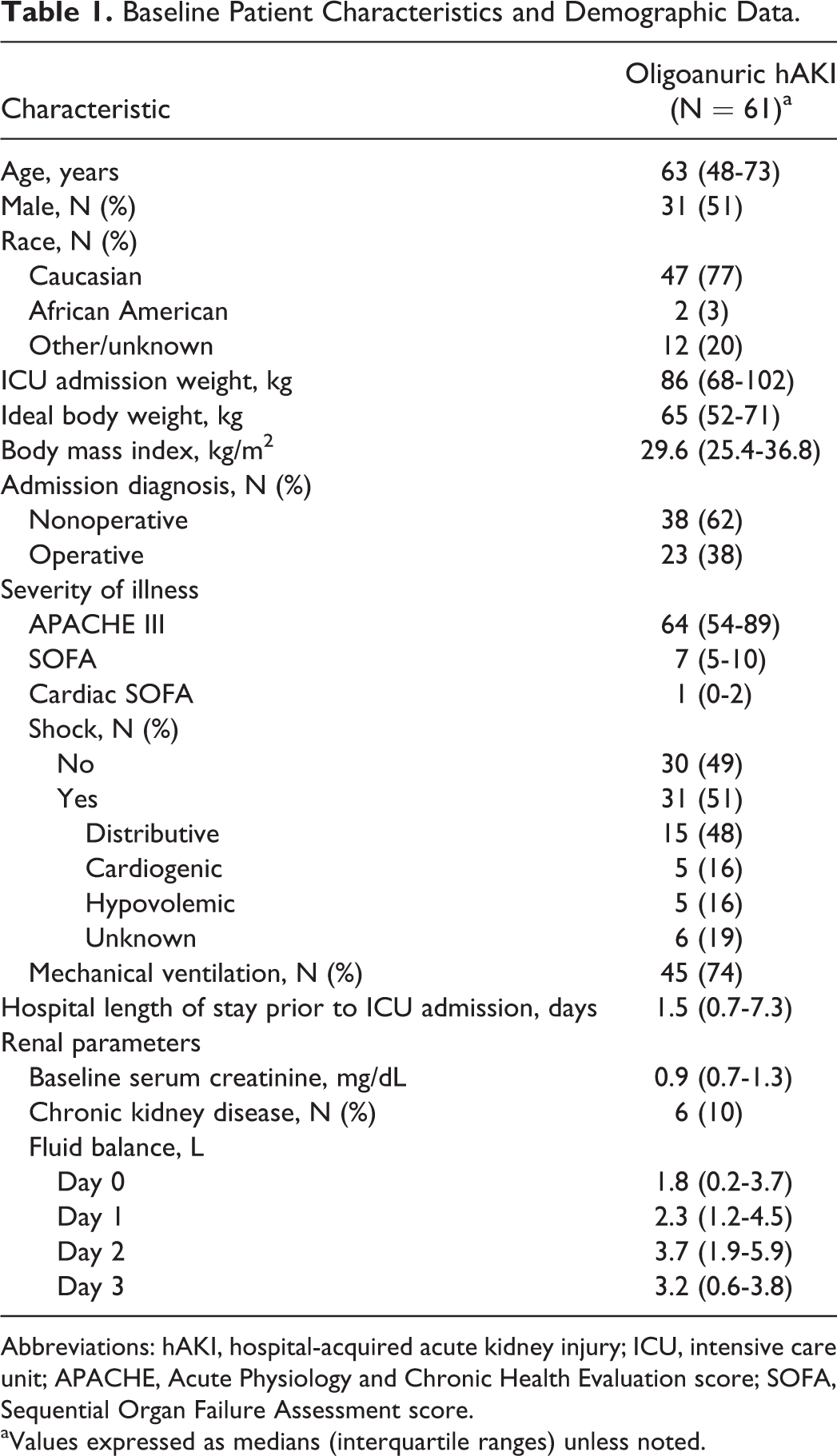
Abbreviations: hAKI, hospital-acquired acute kidney injury; ICU, intensive care unit; APACHE, Acute Physiology and Chronic Health Evaluation score; SOFA, Sequential Organ Failure Assessment score.
aValues expressed as medians (interquartile ranges) unless noted.
Few patients carried a documented history of chronic kidney disease in the electronic medical record (N = 6; 10%; 1 with stage III, 2 with stage IV, and 3 without documentation of staging). However, retrospective evaluation of estimated baseline GFR revealed 21 (34%) individuals with a baseline eGFR <60 mL/min/1.73 m 2 (N = 11, eGFR 45-59 mL/min/1.73 m 2 ; N = 7, eGFR 30-44 mL/min/1.73 m 2 ; and N = 3, eGFR 15-29 mL/min/1.73 m 2 ). Rarely patients used a priori identified medications known to significantly influence serum creatinine (trimethoprim 10%, no cases of cimetidine or probenacid use). Median (IQR) hospital and ICU lengths of stay were 29 (17-50) days and 17 (7-33) days, respectively.
End Points
Oligoanuric hAKI began a median of 9 (IQR 5-17) days into hospital admission and 5 (3-10) days into ICU stay. Patients reached urine output recovery/ICU discharge (43%), need for RRT (41%), or death (16%) after a median of 1.6 (1.1-2.2) days of hAKI.
Each of the 6 creatinine-based equations markedly overestimated true GFR in patients with oligoanuric hAKI (Figure 1). After adjusting for the effect of day and multiple observations per person, eGFR utilizing CG-IBW most closely approximated true GFR (17 mL/min/1.73 m 2 deviation from true GFR of 15 mL/min/1.73 m 2 ; P < .001). The Jelliffe equation least effectively approximated the true GFR with an adjusted deviation from true GFR of 50 mL/min/1.73 m 2 (P < .001). There was marked variability among all equations studied (Table 2). Additionally, after controlling for differences between creatinine-based eGFR equations and multiple comparisons per person, daily GFR estimations significantly overestimated true GFR on each of the first 4 days of hAKI. Inaccuracy of estimated GFR varied nearly inversely with time from hAKI onset (Figure 2). Prespecified subgroup analyses in obese patients, individuals with cancer, and those with distributive shock similarly demonstrated statistically significant overestimation of true GFR for each equation on hAKI day 0 (P ≤ .008, P < .001, and P ≤ .008, respectively). Analyses on subsequent study days were not performed due to small sample sizes in these subgroups.
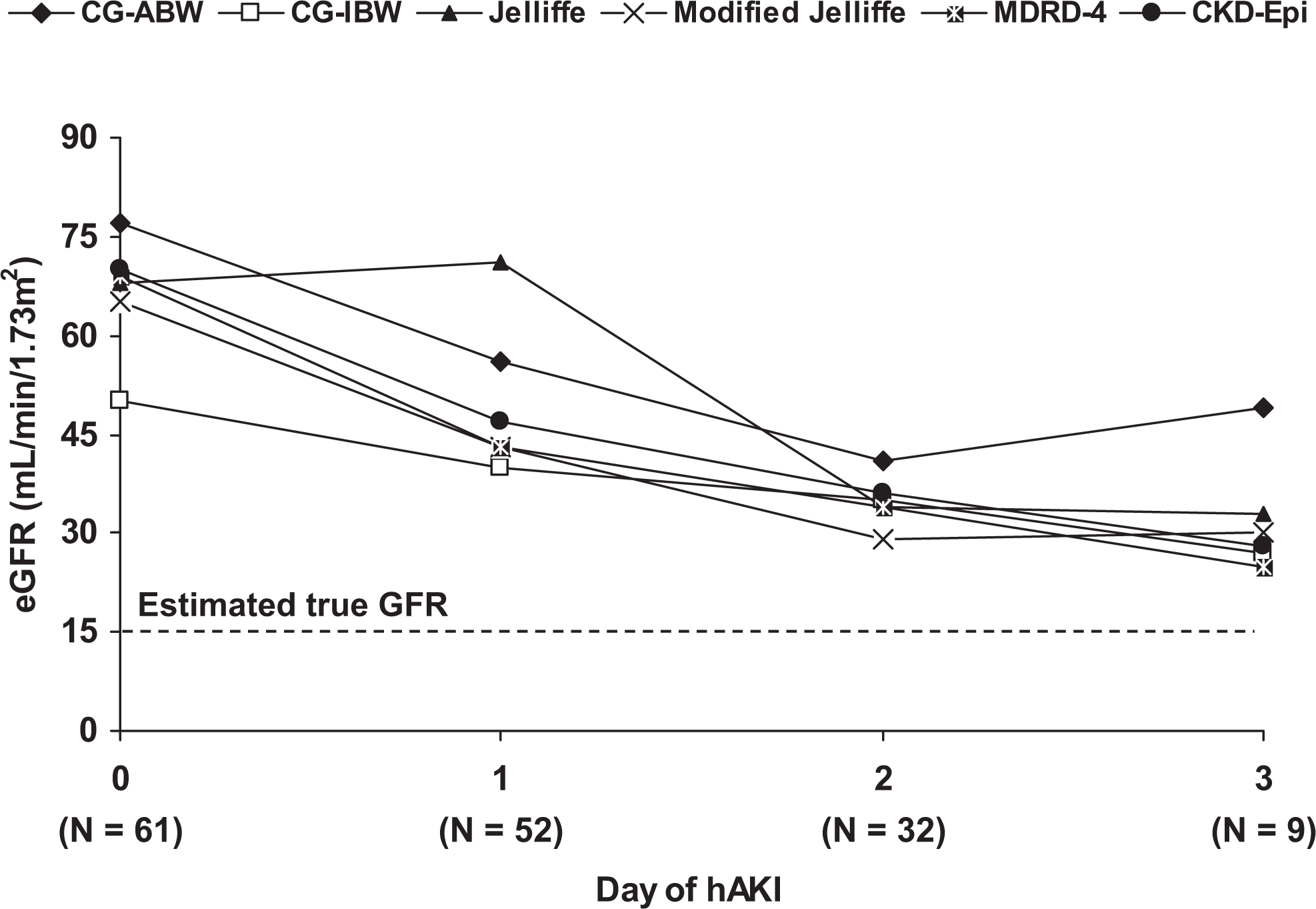
Median estimated GFR (eGFR) using 6 creatinine-based equations in oligoanuric hospital-acquired acute kidney injury (hAKI) according to time from hAKI onset. GFR indicates glomerular filtration rate.
Median Estimated GFR (eGFR) After Day Adjustment and in Comparison to True GFR.
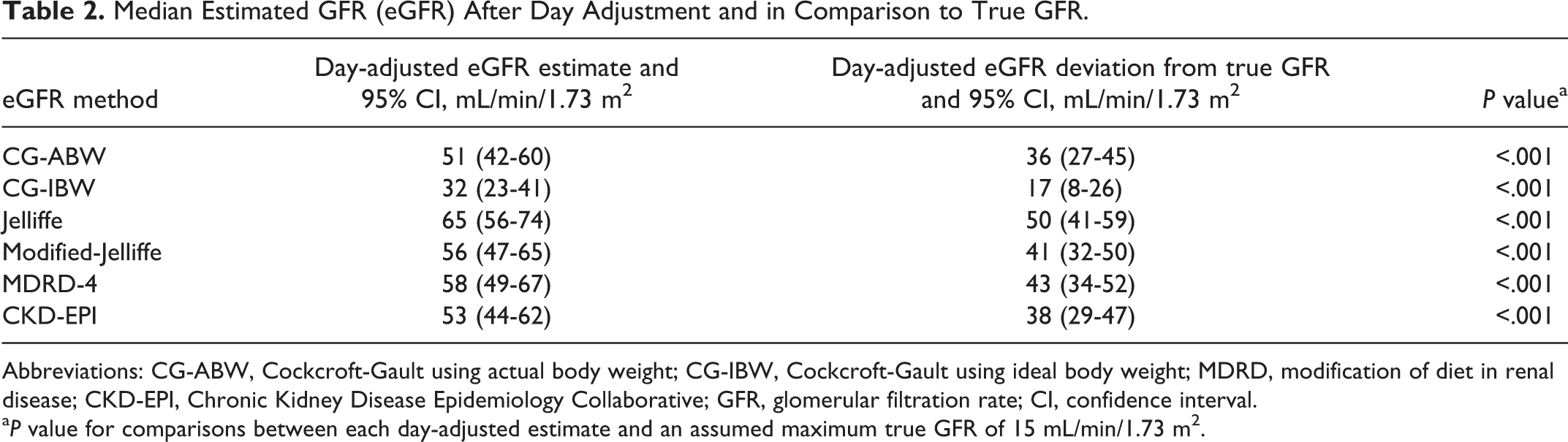
Abbreviations: CG-ABW, Cockcroft-Gault using actual body weight; CG-IBW, Cockcroft-Gault using ideal body weight; MDRD, modification of diet in renal disease; CKD-EPI, Chronic Kidney Disease Epidemiology Collaborative; GFR, glomerular filtration rate; CI, confidence interval.
a P value for comparisons between each day-adjusted estimate and an assumed maximum true GFR of 15 mL/min/1.73 m 2 .
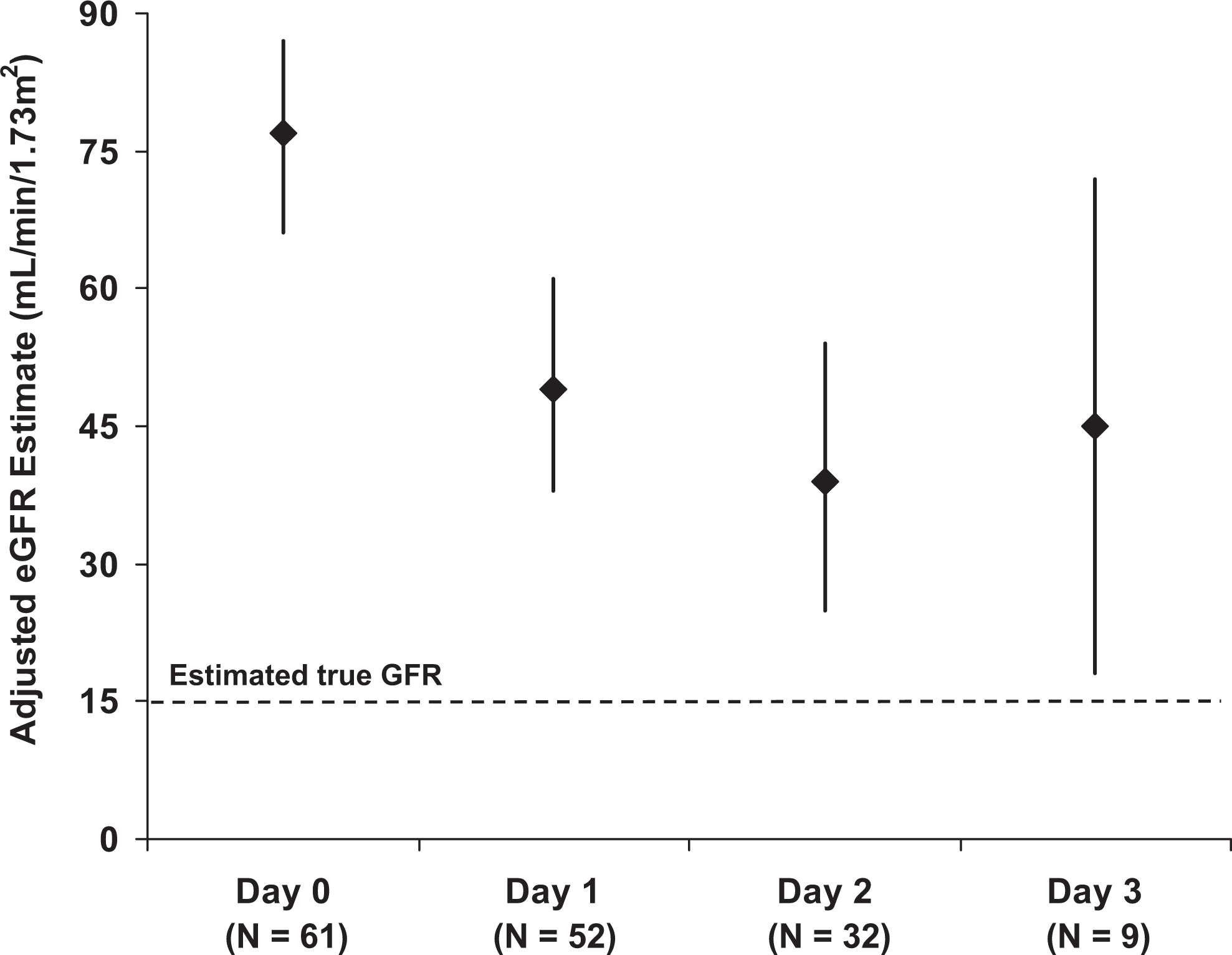
Method-adjusted GFR estimates with 95% confidence intervals on the first 4 days of oligoanuric hAKI compared to an assumed true GFR of 15 mL/min/1.73 m 2 (day 0: P < .001, day 1: P < .001, day 2: P = .001, and day 3: P = .03). eGFR indicates estimated glomerular filtration rate; hAKI, hospital-acquired acute kidney injury.
Discussion
The present study highlights the frequency of significant and protracted GFR overestimation by creatinine-based estimates in ICU patients with oligoanuric hAKI. The CG-IBW most closely estimated true GFR but still demonstrated a 17 mL/min/1.73 m 2 multiple-comparison and day-adjusted disparity versus a true GFR of 15 mL/min/1.73 m 2 . We expanded upon previous studies to demonstrate that the Jelliffe, Modified-Jelliffe, and CKD-EPI equations performed similarly to the CG-ABW, CG-IBW, and MDRD equations. Despite correction for multiple eGFR equations utilized, significant discrepancies persisted between eGFR and true GFR out to the fourth day of hAKI. These data identify a patient group in the ICU at high risk of significant GFR misinterpretation by automated systems and clinicians, which may result in unforeseen medication accumulation and renal and nonrenal toxicities.
Creatinine-based GFR estimation equations have undergone great scrutiny in the medical literature. The majority of validation studies evolved from medically stable hospitalized patients or population-based CKD studies, not the critically ill patients. 22 –24 Several subsequent studies sought to quantify the predictive value of these equations among ICU patients, yet few included individuals with a reduced GFR, hemodynamic instability, or unstable renal function. 11,21,25 –27 Robert and colleagues found more than 10-fold variability in GFR estimates (CG-ABW 11-226 mL/min/1.73 m 2 and CG-IBW 10-169 mL/min/1.73 m 2 ) in a group of patients with measured GFRs < 30 mL/min/1.73 m 2 . 11 Similarly, among 63 patients with 24-hour urine creatinine clearances ≤30 mL/min, the CG-ABW, CG-IBW, and the Jelliffe equations significantly overestimated the GFR but to a substantially smaller degree (5.1-13.3 mL/min; P < .05 for each comparison). 21 Consistent with existing literature we found the overestimation of true GFR when applying creatinine-based estimation equations to patients with baseline reductions in renal function in the ICU. Our data showed poor performance of the Jelliffe and Modified-Jelliffe equations in patients with reduced and unstable renal function, which differs from the findings of Jelliffe and Bouchard et al. 15,28 Sample differences may represent the reason for divergent findings among these studies. Specifically, the cohort of 12 patients from the Program to Improve Care in Acute Renal Disease (PICARD) study population included nonoliguric individuals with serum creatinine rise ≥0.5 to 1 mg/dL and compared eGFR equations to urine creatinine clearance. Despite oligoanuria among patients in the present study, a higher daily cumulative fluid balance existed in the Bouchard et al cohort (2.0-6.7 L), which may have influenced the performance of the Modified-Jelliffe equation. 15
Deterioration of urine output is often one of the first signs of impending AKI and poor predictive ability of eGFR, due to the lag time associated with creatinine rises. 8,14 Prowle et al demonstrated that urine output <0.5 mL/kg/h predicts the subsequent doubling of serum creatinine with fair certainty. 9 Also, use of either the serum creatinine or urine output criterion identified 21% more patients with AKI than use of creatinine changes alone. Not only did new diagnoses of AKI occur more often but also earlier when considering both criteria as opposed to creatinine in isolation. 29 We demonstrated consistent overestimation of GFR by creatinine-based equations out to the fourth day of AKI, yet the degree of deviation from true GFR appears to diminish over time. These data offer new information about creatinine kinetics and eGFR predictions during severe AKI in critically ill adults.
Our data reinforce known concerns about the use of creatinine-based equations in the hospital, particularly in critically ill patients with AKI. Unfortunately, this approach remains central to medication dosing in this setting, likely due to the reliance on CPOE, rule-based technology, automated calculations, and the lack of aviable alternative method. 12,30,31 In a group of 1337 hospitalized individuals with known renal dysfunction based on creatinine, providers selected an inappropriate antimicrobial dose in 1 of the every 3 patients. 32 A separate initiative notified providers via a CPOE alert if a 0.5-mg/dL rise in creatinine occurred during therapy with any 1 of the 122 prespecified nephrotoxic or renally eliminated agents. These authors demonstrated that significantly more nephrotoxic medications were avoided and medication doses adjusted after implementation of the CPOE intervention. 31 Yet in each of these cases, the time course of intervention relative to actual underlying GFR changes was not reported. Also, serum creatinine was the only renal marker, which drove the alert; urine output was not considered in the models. We suspect that the infrequency with which strict urine output is available in the majority of hospitalized patients may explain this gap both in practice and the literature. Fortunately, the recent development of novel ICU-specific electronic interfaces could make possible a tailored approach to physician alerts, which incorporates multiple markers of GFR (eg, creatinine and urine output) when screening for medication toxicity and dose optimization. 33
Several important limitations exist for this type of study. No clinically applicable gold standard of true GFR exists to measure renal function during the dynamic course of oligoanuric AKI. Measured GFR, with iothalamate or iohexol for example, is resource intensive, captures a single moment in time, and is not readily available at all centers. Other previously studied approaches to estimate GFR in the ICU such as urine creatinine clearance or cystatin C are infrequently utilized outside of the scope of research and are not extensively validated in this patient population. 15,34 In the present study, we determined true GFR through a consensus from experts in the field and the results of prospectively collected urine creatinine clearances on a small number of nonincluded patients. These findings were extrapolated to establish the reference GFR for comparison in this study, but the authors emphasize that the true GFR of patients with AKI is dynamic and would be extremely difficult to ascertain with a retrospective evaluation. We also acknowledge that although the CKD-EPI equation used in this analysis was current during the study timeframe, it has since been updated. 35 Although the new CKD-EPIcreatinine equation may demonstrate improved validity for measured GFR, we feel that this difference is unlikely to have meaningfully altered our findings. Although the heterogeneity of the included sample allows for application of these results to multiple ICU settings, it prohibited us from evaluating the implications on dosing of specific medication classes. We hypothesize given the degree of GFR overestimation, alternate medication use strategies should have been considered in many patients, and future study could explore this question.
Conclusions
In ICU patients with oligoanuric hAKI, GFR decline, as evidenced by decreases in urine output, may be missed by creatinine-based estimates out to the fourth day of AKI. These patients are at high risk of inadvertent exposure to nephrotoxins and medication toxicity, particularly at the outset of oligoanuric renal dysfunction. Systems-based initiatives including electronic notifications and rule-based alerts, which include both urine output and creatinine, should be used in this setting. Among individuals with stage III hAKI, clinicians should consider pursuing renal dose adjustments based on GFR <15 mL/min/1.73 m 2 rather than the overestimate derived from calculated GFR with serum creatinine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by a research grant from Mayo Clinic Pharmacy Services Discretionary Fund.