
Abstract
Deinstitutionalization in the 1960s shifted the care of the mentally ill from state-funded institutions to community settings. Unfortunately, funding to support the treatment needs of this population has continued to be minimized, and countless individuals have not received much needed care. This has resulted in a large increase in mentally ill patients surfacing in jails, homeless shelters, and emergency departments. Subsequently, the federal government has begun to prioritize funding to address the mental health needs of our communities. Pharmacists are in a unique position to influence treatment outcomes for patients with mental illnesses, and the current state of health reform provides avenues for the pharmacist to become an essential part of the health care delivery team in numerous ambulatory care clinical settings. The challenges with adherence, medical and psychiatric comorbidities, polypharmacy with psychotropics, potential for life-threatening adverse effects, and the ever-present need for patient education are but a few reasons why pharmacists can be utilized to provide Medication Therapy Management services for these patients.
The importance of caring for those with mental illnesses continues to rise. In 2012, there were an estimated 9.6 million adults, aged 18 or older, in the United States with severe mental illness. 1 The increase in worldwide incidents, ranging from terrorist attacks/wars in Iraq and Afghanistan to recurrent natural disasters, have contributed to increasing diagnosis of mental illness (depression, posttraumatic stress disorders, and other affective disorders), congruent with the strain on funding of mental health initiatives because of said increase. In a survey conducted by Substance Abuse and Mental Health Administration, the top 4 reasons that people had not received mental health treatment included the inability to pay for treatment, feeling they could handle the mental health issue without treatment, mismanagement of time, and lack of knowledge regarding resources for services. 2
For the past 40 years, several federal initiatives have attempted to bring order to this situation. In 1955, congress passed the Mental Health Study Act, which formed the basis of the Community Health Care Act of 1963. This Act was a federal legislation that mandated increased treatment of mental illnesses in community settings as opposed to state-run psychiatric facilities. 3,4 Many states could not accommodate the expertise and facility needs of this population through community settings, resulting in a disproportionate number of individuals being incarcerated, developing substance abuse disorders, living with their families, unemployed, and/or homeless. The Reagan administration shifted funding efforts to the provision of Mental-Health Block Grants for individual states. President Barack Obama’s Administration has taken several key steps, through the Omnibus Appropriations Bill and Affordable Care Act (ACA), to increase access to mental health services. The Omnibus Appropriations Bill secured US$115 million for new mental health initiatives through Mental Health First grants, comprehensive program development, behavioral health workforce training, programs targeting young adults at high risk of mental illness, and Mental Health Block grants. 5 Funding was also appropriated for the National Child Traumatic Stress Network and suicide prevention programs. 6 The ACA has provided funding to help Community Health Centers across the country establish or expand mental and behavioral health services for people living with mental illnesses or addiction. Consequent to these efforts in health reform, enrollees can receive free preventive care, prescription discounts for seniors, protection against health care fraud, small business tax credits, consumer assistance, and increased access to health care through the health insurance marketplace. Also, insurance companies can no longer deny coverage due to preexisting conditions. Additional outcomes to the program include the expanded young adult coverage available to children up to 26 years old through their parents’ insurance, insurance companies now needing justification for charges in holding them responsible, direct coverage to women for preventative services, and so on. 7
These federal mandates and the ever-increasing number of patients with psychiatric disorders are providing an opportunity for pharmacists practicing in this arena to play a more vital role in the health care delivery to this population. This article will describe models of practice that can be duplicated or implemented for patients with mental illness and will identify resources to assist the clinician in delivery of these services.
The emergence of Accountable Care Organizations and the integrated patient-centered medical home (PCMH) model speak to the need for Medication Therapy Management (MTM) to be incorporated into health care delivery. Within the PCMH model, integration of mental health is of focus in identifying mental health problems, monitoring the outcomes, and coordinating treatment more closely with mental health specialist in support of patient management. 8 Given reports that there is a national shortage of psychiatrists in the United States, often more in rural areas, new collaborations allow hospitals and community health centers to patch together consistent treatment programs for people with mental illness. 9,10 Whether this is truly sufficient remains to be determined. Given the, ever present, budget cuts across various branches of government and impact these budget cuts press upon the mental health system, pharmacists, working within the community, have a unique opportunity to enhance the delivery of pharmaceutical care to patients with mental illnesses. Although some PCMH models may depict pharmacists as players in the care of the patients, oftentimes this element remains unnoticed in some US health care settings. Although most knowledgeable parties view Primary Care Providers (PCPs) and Care Managers and Mental Health (MH) Specialists as primary team members within the care of the patients and nurses, physical/occupational therapists, pharmacists, and so on, as secondary team members, primary team members often rely on this “secondary” cohort in the care of patients having mental illness. 11 It can be argued that the role of the pharmacists in this new-aged model may need to be placed in the core group with other health care professionals (Figure 1).

Patient-centered medical home model.
The level of accessibility for patients to receive psychotropics through various outlets, such as retail pharmacies, community health centers, mental health clinics, substance abuse clinics, Veterans Affairs (VA) Centers, mail order pharmacies, support groups, Mental Health Organizations, and inpatient hospitalizations, makes pharmacists even more critical to the success of the patient recovery. Pharmacists instrumentally reinforce adherence, assisting with the acquisition of medications, preventing hospitalizations, providing patient education, improving cost utilization, conducting screenings, and providing insight into medication dosing, side effects, drug interactions, and selection of medications to prescribers. 12 -15 Since mental illnesses often coexist with all chronic health problems, this can often complicate the response to standard treatment modalities.
Pharmacists play an instrumental role in managing medication use in patients receiving treatment for mental illnesses. 16 The MTM model within psychiatry has been an ongoing venture that offers a wide opportunity for improved outcomes for the patient. Currently, the National Conference of State Legislatures (NCSL) reported, in 2011, that 18 states with state/public employees, institutional patients, and Medicaid plans reimburse MTM services provided by qualified pharmacists. The NCSL acknowledges the efforts of 10 organizations representing the pharmacy profession in outlining the core elements of MTM. The Medicare Part D and MTM Requirements, under federal statutes 423.153(d), include Mental Health as one of the chronic conditions that can be a target for beneficiaries. Many services can be paid through the Medicaid A payer, the academic or clinic center in which the services are offered or exist as part of the psychiatric services the pharmacy or clinic provides and, therefore, these services are not billed separately for services. 17
Clinic Models
Although every state may not have worked out the logistics of the MTM reimbursement of pharmacists, many psychiatric pharmacists have not allowed this to deter them from providing cognitive and other nontraditional services. The literature suggests that community pharmacists have been providing services for patients in mental health settings in various ways for, at least, 30 years. Most of the services have taken place in inpatient settings and Veterans Affairs Medical Centers (VAMC), but several initiatives have been developed through collaborations with universities and community-based organizations. Identifying unique practice settings and using these models to break through in your own setting should be considered when meeting the 5 core standards of the MTM model. The next section provides examples that demonstrate the provision of various services to assist patients with mental illness.
VAMC have been forerunners in the delivery of pharmaceutical care initiatives that may or may not include dispensing of medications, with the most elaborate mental health care systems. Some of the initial collaborative drug therapy management protocols were initiated in VAMC ambulatory care clinics, including, but not limited to, anticoagulation, pharmacotherapy, and diabetes clinics. The VAMC hospitals provide mental health services ranging from inpatient, residential, to outpatient services at its medical centers and clinics. The VAMC utilizes pharmacists for traditional dispensing and quality assurance roles ranging from provision of recommendations to prescribers, collaboration with heath care teams, prescription under protocol, provision of preventive medicine, managing the VAMC drug formulary, participation in the home-based primary care/geriatric care programs, and playing a critical role in health information technology. These roles have allowed pharmacists to make impactful differences with inpatient and outpatient health care for dosing modifications, recommend therapies, and point-of-care testing, in addition to patient counseling and education.
Several ambulatory clinics with a focus on mental illness have been established in the VAMCs such as Mood Disorders Consult Clinics, Clozapine Clinic, Medication Monitoring Clinics, Refill/Renewal Clinics, Depression Clinics, and Smoking Cessation Clinics. Pharmacists providing services in each of these clinics may provide patient education, monitor laboratory test results, check adherence, help determine appropriateness and effectiveness of psychotropics, identify and prevent medication-related problems, minimize polypharmacy, dispense needed medications, and/or notify prescribers if problems ensue with medication.
Pharmacists involved with Clozapine Clinics are recognized as Shared Care Responsibility Providers within the Clozapine Treatment Team (CTT). The pharmacist describes side effects, signs of neutropenia, emphasizes the need for compliance, orders laboratory testing, and notifies the patient, prescriber and pharmacy service if problems ensue. The pharmacist sees patients on a weekly, biweekly, or 4-week interval based on current duration of therapy, symptom control, and tolerability assessments. The pharmacist reviews white blood cell and absolute neutrophil counts for clozapine per protocol and communicates with the National Clozapine Coordinating Center along with making dosing recommendations to the CTT physician. The pharmacist is also responsible for completing a Drug Utilization Evaluation as part of the facility's Quality Assurance plan when requested. Finally, the pharmacist provides information regarding the number of patients receiving clozapine, abnormal WBC/ANC results, clinical interventions, and termination reports and subsequent justification to the Pharmacy & Therapeutics Committee as needed.
Patients in the Medication Monitoring Clinic typically take valproic acid, lithium, carbamazepine, or an atypical antipsychotic requiring consistent serum drug concentration and metabolic parameter monitoring. Patients enrolled for the metabolic monitoring must have hyperlipidemia, hypertension, diabetes or risk factors for diabetes, and have, at least, 3 characteristics of metabolic syndrome. Pharmacists involved in this clinic will evaluate the effectiveness of therapy and monitor laboratory values relating to metabolic syndrome, side effects of the medications, and blood serum concentrations of medications when appropriate. Dosage changes are made by the pharmacist, when appropriate, to manage symptoms of the disorder or side effects of a medication after discussion with the treating psychiatrist. Patients receive education on potential side effects of their medications along with weight management counseling.
Pharmacists work with the Social Work Service in the VAMCs for the Refill/Renewal Clinic. The pharmacist evaluates patient’s current therapy in monitoring for tolerability, efficacy, and adherence. The pharmacist also requests necessary laboratories, ensures follow-up appointments, and provides a short supply of medications (up to 1 month) to treat patients until his or her next scheduled appointment. A treating psychiatrist must have seen patients within 6 months of his or her walk-in visit, even if he or she arrives from another VA facility with the aid of access to electronic medical records.
Pharmacists involved in Smoking Cessation Clinics provide management of patients desiring assistance with smoking cessation through counseling and educating patients on proper use, storage, administration, side effects, and disposal of the smoking cessation products. Pharmacists also assist patients with problems or concerns that they may encounter during cessation of smoking, with new prescription orders, refills, or the titration of doses for smoking cessation medications. The pharmacist also has the authority to make dose adjustments or changes in smoking cessation products, as deemed necessary. Pharmacists may initiate new prescriptions, add refills, renew medication, prescribe combination therapy, or discontinue therapy as deemed necessary. They also screen for anxiety and depression and suggest treatment, where necessary.
Pharmacists also participate in Pain Clinics in VAMCs. In this capacity, they monitor the use and tolerability of narcotics, adjust doses of pain medications, order and evaluate appropriate laboratory tests, schedule follow-up visits, initiate pain contracts, assess adherence, assess the potential for addiction, and serve as an education resource for other disciplines. They also screen for anxiety and depression and suggest treatment, where necessary.
Other ambulatory care environments, managed care organizations, community mental health clinics, specialty clinics, universities, grocery and other retail pharmacy establishments, also offer services for patients with mental illness.
Some managed care entities have ambulatory Depression Clinics similar to VAMCs. Typically, the clinical pharmacy specialist evaluates patients immediately after the initiation of antidepressant medications. Primary care practitioners refer patients to the clinic, and the pharmacist has limited prescribing privileges. The pharmacist coordinates follow-up with patients through scheduled office visits and telephone calls. The primary goal of the collaboration is to improve consistent adherence in patients taking antidepressants. Discussions have begun regarding reimbursement in this facility since the passing of the SB493 in California.
Another future clinical service model to be provided, within a managed care organization, will provide comprehensive psychiatric care to families planning to have children, from conception through the postpartum period. Patients will be utilizing home visits and telepsychiatry, in addition to traditional clinic visits. The efforts will be a multidisciplinary venture, consistent with the PCMH model, wherein the financial model had not yet been elucidated at the time of this publication.
Finally, opportunities for MTM also exist with childhood disorders. Although applicable to adults, the attention-deficit disorders lend themselves to predictable monitoring of adherence, weight, side effects, and response to treatment, with the use of stimulants and nonstimulant treatment options. Pharmacists can also provide education with regard to managing particular side effects associated with related stimulants, namely, insomnia, tics, and appetite changes. Pharmacists can also assist in providing instructions on the proper use of a stimulant patch, pharmacodynamic, and pharmacokinetic characteristics of these medications, monitoring for the impact of stimulants and atomoxetine on the blood pressure as well as investigating the need for treatment of co-occurring psychiatric disorders, such as depression and substance abuse disorders. The use of nonstimulants also creates opportunities for pharmacists to educate patients, parents, and educators alike. Childhood depression is also seen in pediatric patients, and, due to the limited number of Food and Drug Administration (FDA)-approved antidepressants for children, pharmacists can assist in selection and monitoring services. Additionally, pharmacists can be instrumental in suggesting and monitoring treatment options for Tourette’s disorder.
Community Health Centers provide a variety of services, utilizing numerous disciplines. The pharmacist provides a comprehensive medication review and provides documentation of the encounter in the patient’s chart, to the patient, and to the providers. The pharmacist operates under collaborative practice agreements with the clinic. The pharmacist also coordinates refills. The referrals come from psychiatrists, therapists, physicians, nurses, and case managers or through a community organization providing support for patient employment and housing. The centers may assist with setting appointments for the MTM services.
Clinics serving indigent patients also utilize the assistance of pharmacists to provide mental health services. Pharmacists evaluate patients referred by primary care practitioners for psychiatric or cognitive complications and the need for comprehensive drug therapy management. Patients with depression, dementia or cognitive impairment, anxiety, sleep complications, Bipolar disorder, smoking cessation, psychosis, or a need for medical education are referred to the pharmacist. Pharmacists provide patient counseling and education to all patients in English or Spanish. Pharmacists may refer patients to social services workers or other health professionals, as needed. Pharmacists determine the need and frequency for follow-up.
Pharmacists take opportunities to provide assistance to patients with mental health disorders through ambulatory clinics where mental disorders, frequently, prevail. For example, there exists a high prevalence of depression in individuals being screened or treated for dementias. Often, caregivers are equally susceptible to these disorders and can be included in treatment efforts. Another example exists in patients being treated for other neurological disorders such as Parkinson’s disease, multiple sclerosis, or cerebrovascular disease, in which pharmacists can assist in recommending and monitoring effectiveness of treatment choices. 18
Collaborations between clinical educators and community agencies and community centers also create opportunities to involve student pharmacists in the delivery of MTM services. The Tobacco Cessation Quit Intervention and Follow-Up Program, for example, utilizes the services of pharmacists who are tobacco treatment specialists as well as local administrative support for the continued management of the Pharmacist-Assisted Tobacco Cessation Quit Intervention Program currently offered at Florida Agricultural and Mechanical University’s College of Pharmacy. The goal of this project is to improve abstinence rates in patients using smoking cessation products, within a community setting, by utilizing a pharmacist-based smoking cessation program.
Clinical pharmacists provide individualized counseling to participants who demonstrate a desire to quit smoking. Patients will be recruited through the “Quit Smoking Now” classes that are offered through Florida State University’s Big Bend Area Health Education Centers. Once identified, participants receive 1 individualized counseling session followed up by telephone counseling on a regular basis for a 6-month period. Eight weeks of nicotine replacement therapy is supplied by Big Bend Area Health Education Centers to the patients.
Opportunities for Patient Education in Mental Health
There are various psychotropics available in a myriad of formulations, offering innumerable opportunities for counseling and education. Off-label use of these medications, multiple psychiatric indications, and the use of polypharmacy by providers have all increased the application of these medications, securing their inclusion in the most frequently prescribed medication lists. Because of these practices, the risk of drug interactions and potential synergistic and adverse reactions has also increased and created opportunities for pharmacists in this arena to be more involved in patient education. Certain combinations of psychotropics can also increase the likelihood of certain psychiatric side effects and syndromes like extrapyramidal side effects, neuroleptic syndrome, serotonin syndrome, metabolic syndrome, and postdelirium sedation syndrome. 19 -24 Since prescribers typically do not manage medications used outside their specialty area, there is an opportunity for the pharmacist to provide education to the patient about these syndromes and communicate to prescribers when there are concerns requiring interventions. Pharmacists should educate the patient about the signs and symptoms of the side effects and syndromes as well as work with prescribers to avoid combinations of medications that can cause these syndromes.
Additionally, pharmacists inform patients about when psychotropics will begin to start providing their clinical effects, instruct patients on how to use topical psychotropic preparations, instruct patients on tapering and titrating strategies when starting or discontinuing psychotropics, and educate patients on important side effects or adverse events that require medical attention. In the event that orally dissolvable preparations and certain injectables are prescribed, the pharmacist can inquire about drug allergies and/or injection site reactions that could complicate therapy. One important skill that pharmacists have is the ability to educate patients about the use of comorbid medications, herbal medications, vitamins, and other nonprescription medications that can compromise efficacy from psychotropics. 25 Pharmacists can provide valuable information about when the psychotropics and other medications should be administered to minimize drug interactions, utilize chronotherapeutic principles, and avoid interfering with vegetative symptoms like sleep. 26 Various agents in the anticonvulsant and antidepressant classes can cause drug interactions by inducing or inhibiting the cytochrome P450 system, but several psychotropics can be affected by other medications that can cause drug interactions. 27 -29 Pharmacists can also reinforce the education efforts of other health care providers by explaining the symptoms that the medications are being used to addressed and can serve as resources for identifying local and national consumer groups and organizations providing services to mentally ill patients. Finally, mental health providers often have limited insight on patient experiences from the psychotropics between clinic visits, and pharmacists can provide side effect queries and feedback to prescribers. Collectively, all of these patient education efforts will improve adherence and efficacy.
Psychotropics in Special Populations
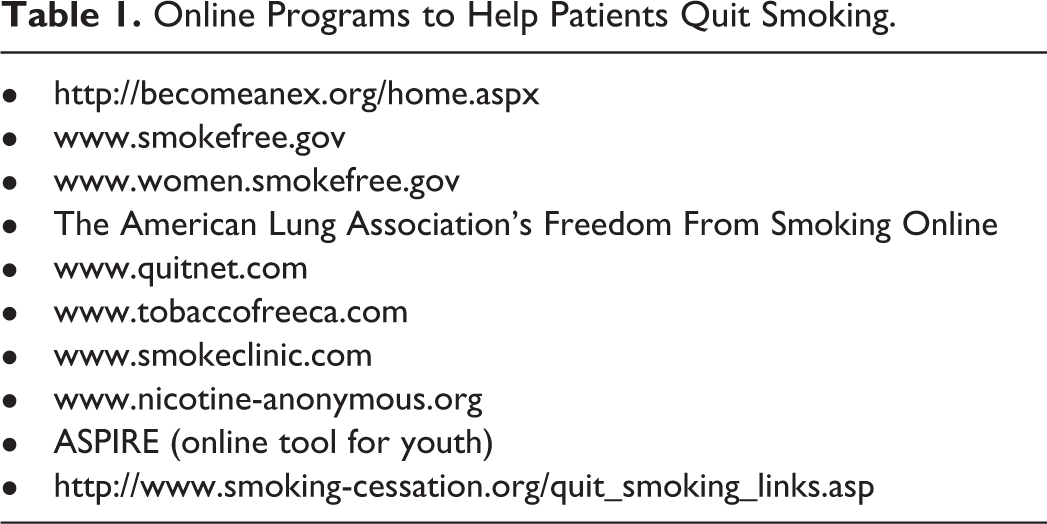
Psychiatric pharmacists have many other ways in which to impact clinical practice, especially in special populations. This population is often characterized as those patients who may be pregnant or lactating, due to the associated teratogenic effects and the need to evaluate the risks and benefits for use of psychotropics in patients who are or are planning to get pregnant. 30 Pharmacists in the ambulatory setting have a unique opportunity to educate patients about the proper use and risks associated with herbal products. Given that pharmacodynamic and pharmacokinetic changes may be present in the aged population, an increased risk for more adverse effects and a need for more pharmacist intervention on several layers, including assistance with the selection of certain psychotropics, monitoring for cognitive effects, preventing those that can increase risk of falls, monitoring of herbal products (given the high use in this population and overall polypharmacy that may be a result of chronic cooccurring disorders) becomes necessary. Psychotropics in children under the age of twelve can also cause for additional opportunities to evaluate the FDA approval status and should be used as a last option due to the possibility of obesity and juvenile diabetes, in addition to the possibility of substance abuse issues. 31 Additionally, substance abuse can be challenging to treat in mentally ill patients, and, therefore, presents an opportunity for pharmacist to assist in the aversion and cessation efforts in areas such as smoking (Table 1), along with the monitoring of withdrawal symptoms in special clinic settings where physicians administer treatment.
Online Programs to Help Patients Quit Smoking.
Finally, Assertive Community Treatment (ACT) teams are also an opportunity for pharmacists to provide education and support. The teams assist severe and persistent mentally ill individuals who typically do not respond to traditional services. Pharmacists can assist with medication acquisition, delivery, adherence, education, administration, and serve on the advisory boards alongside members of the ACT team and consumer advocates.
New Opportunities in Screening and Prevention Services
There has been quite a challenge for many geographical locations to either establish or maintain an MTM model for the purpose of reimbursement. Given the present day law, the ACA, there are new opportunities and mandates in place that may cause many physicians to seek out pharmacists’ specialized services in psychiatric pharmacy. Utilizing a pharmacist can be helpful in providing and interpreting screenings for mental illnesses, especially in areas where access to psychiatrists and other mental health specialists is limited for early detection of mental illnesses and allow an opportunity for pharmacists and other clinicians to monitor the effectiveness of psychotropics used for mental illnesses.
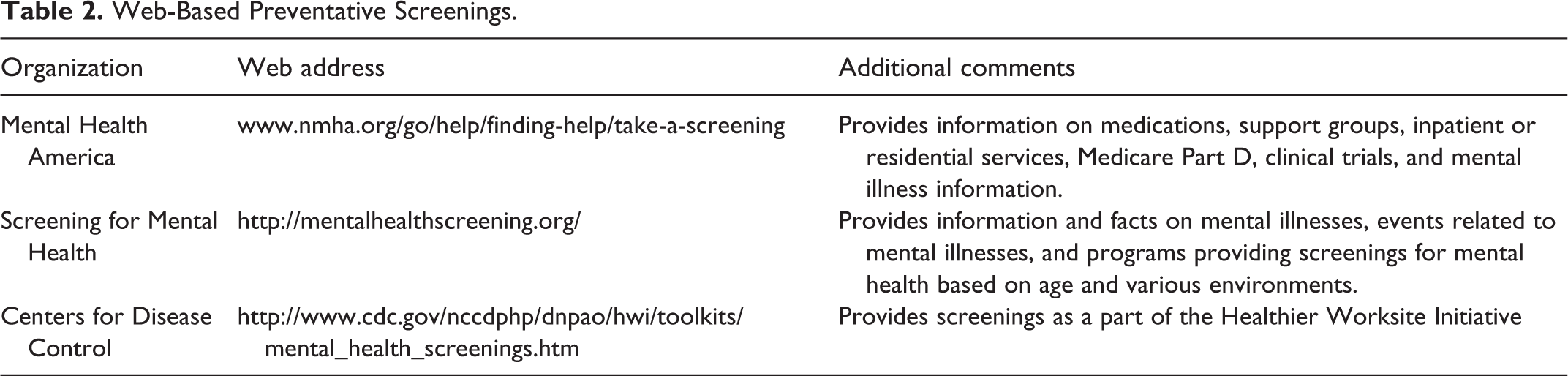
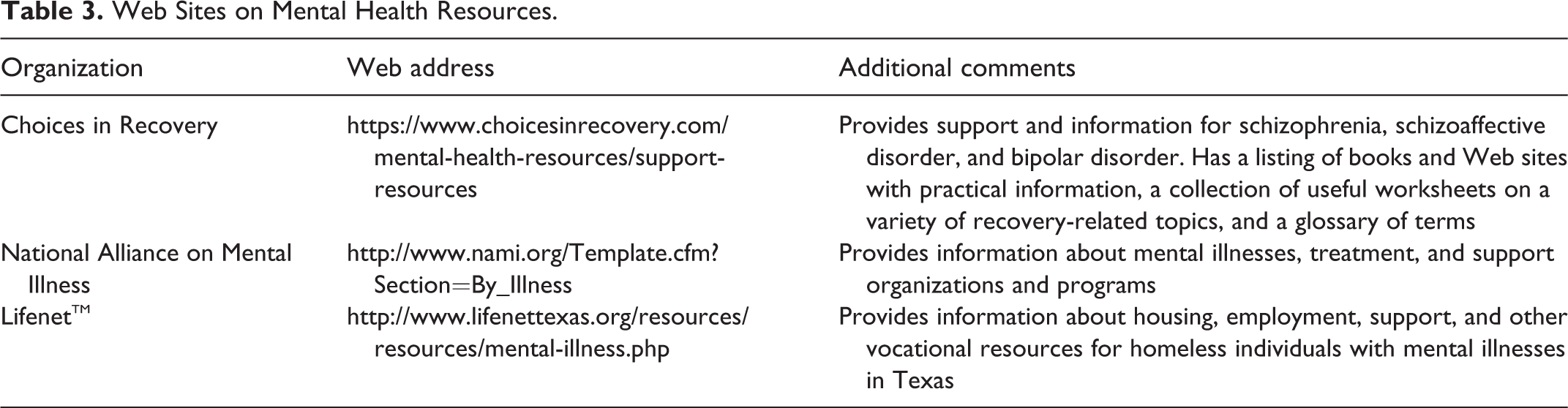
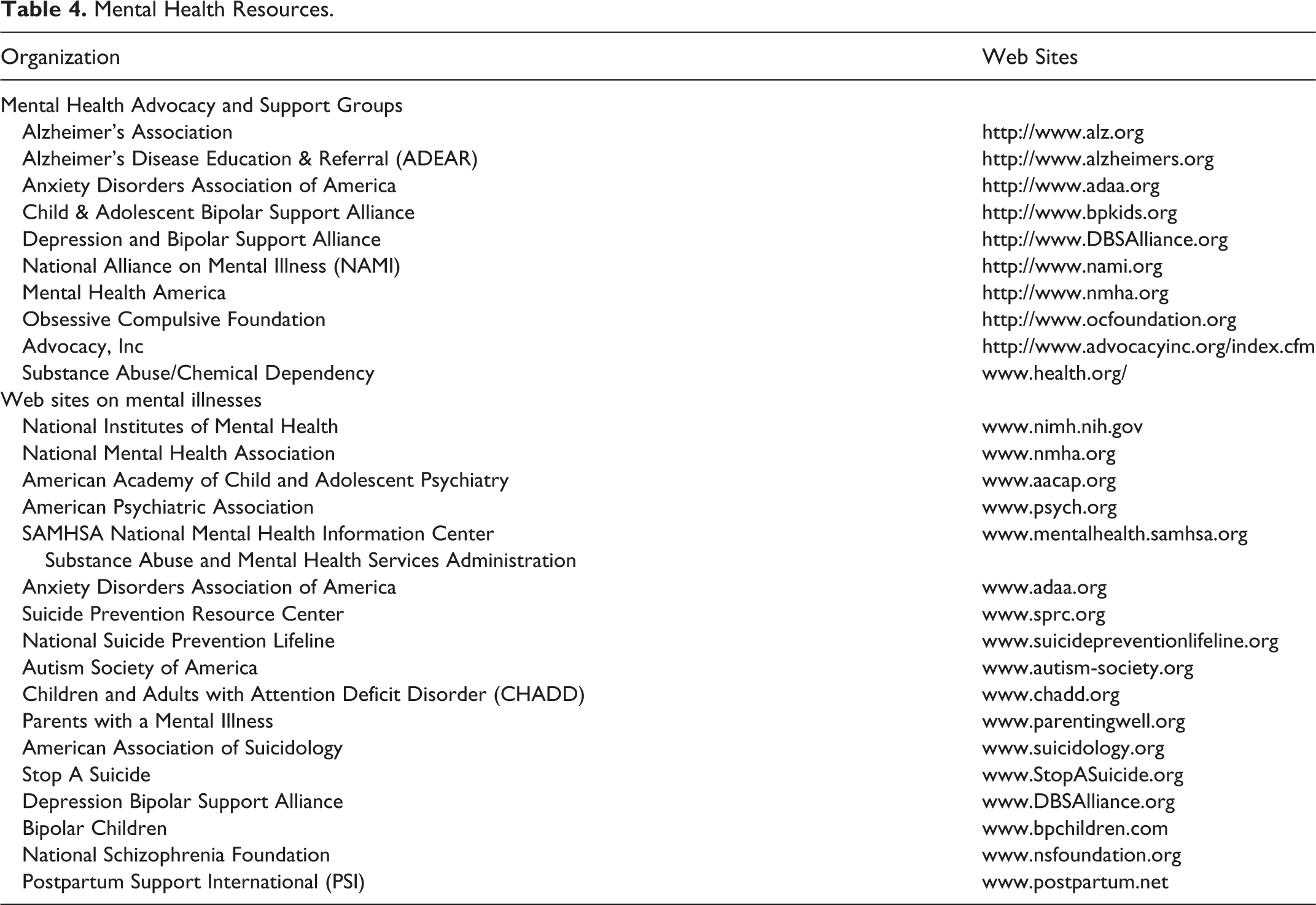
Additional opportunities for prevention strategies under the ACA in which psychiatric pharmacists could involve themselves include alcohol screening, domestic and interpersonal violence screening, tobacco use for all adults and cessation interventions for tobacco users, alcohol and drug use in adolescents, autism screening, and behavioral screening. (2) There are several free and anonymous online screening tools available for consumers and health care professionals. Pharmacists can identify reputable sites and interpret the findings of screenings, refer patients to appropriate mental health practitioners, as necessary. Table 2 summarizes a list of helpful Web sites and organizations that have free online screenings. Collaboration with other disciplines such as psychiatrists, psychologists, and social workers may also allow pharmacists to provide feedback on medication response. Tables 3 and 4 provide Web sites with information on mental health resources that will be beneficial for both consumers and health care professionals.
Web-Based Preventative Screenings.
Web Sites on Mental Health Resources.
Mental Health Resources.
Billing remains an issue and may only be applicable in certain settings. Academia may not be an option for MTM billing, given the duties are generally a part of the job description. This is similar to the government ambulatory care clinics with the VA hospitals/clinics. Ambulatory pharmacy practices may be the most commonly used group to optimize this option if this option is available in their state. A study in 2011 by Beatty et al evaluated, using an online survey, the billing trends of pharmacists where the majority of the pharmacists were practicing in a physician office setting (23.6%) versus health-system outpatient facility setting (21.7%), and community pharmacy setting (20.2%), also the highest overall. Of the 276 pharmacists, 54% of pharmacists reported billing for MTM services. Pharmacists who saw their patients for an in-office visit were also more likely to bill for their services. Overall, the study found that there were inconsistencies in the billing techniques and reimbursements. 32
In closing, psychiatry is a plausible platform for MTM practice due to monitoring requirements, potential for drug interactions, the use of poly pharmacy, cost considerations, and the risks associated with adverse events with psychotropics. Pharmacists must be appropriately credentialed and skilled to ensure the delivery of quality services. Pharmacists are already involved in MTM-like practices, but additional opportunities to expand the clinical practice of pharmacy are becoming more recognized as caregivers by managed care organizations and reimbursement practices for their services exist within health care reform efforts. As previously mentioned, the limited number of FDA-approved treatment options for children and off-label use practices seen with psychotropics creates an opportunity for pharmacists to be instrumental in providing insight into the appropriate selection of the psychotropic medications. Additionally, given the ACA and the push for physicians to work in the PCMH model, pharmacist inclusion will be required for care, eradicating the need for pharmacist-saught opportunities for consideration and willing participants for collaboration. For the purposes of dependent state reimbursement, it may be necessary to have the facility in which one practices to reimburse a salary and, then, bill for an “Incident to Physician” visit. This requires the physician to have physical contact with the patient and can be achieved through pharmacist interview of the patient and development of a physician-shared treatment plan. Whatever method is used to accomplish pharmacist provider recognition for service reimbursement, whether the services are built into the scope of practice or the pharmacist provider bills through the MTM model, the end result will be optimal care of patients with a specialist trained in drug therapy as related to mental illness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Karimah S. Bell Lynum is employed by Janssen Scientific Affairs, LLC, a company of Johnson & Johnson.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.