
Abstract
Cholesterol management is an important factor in the modification of primary and secondary cardiovascular events. Guidelines emphasize incorporation of appropriate medication therapy and lifestyle adjustments to reduce low-density lipoprotein cholesterol (LDL-C) for cardiovascular disease (CVD) risk reduction. Of note, studies and nation-wide statistics indicate many patients do not achieve their LDL-C goals. Eliminating barriers and challenges associated with cholesterol management will allow patients to reach prespecified goals for CVD risk reduction. As the nation transitions to covering more individuals, the need for additional health care providers is evident. Pharmacists are accessible and knowledgeable health care contributors who can assist in optimizing patient outcomes. This article discusses the pharmacist’s role in addressing challenges and barriers in cholesterol management.
The management of dyslipidemia continues to be a national focus due to its essential role in coronary heart disease (CHD). 1 In 2010, CHD caused 1 in 6 deaths within the United States averaging in death every 1 minute 23 seconds. 2 Ischemic heart disease and stroke were listed as the 2 top leading causes of death in the world, respectively, in 2011 by the World Health Organization. 2 Although medical advancements have likely played a role in decreasing the amount of individuals dying due to ischemic heart disease and stroke, these disease states have remained the top leading causes of death over the last decade. 3 Perhaps equally as devastating is the reduced quality of life and life expectancy experienced by patients surviving cardiovascular events as life expectancy has been reported to be reduced up to 15 years and quality of life decreased by 50%. 4 -8 The economic repercussions of cardiovascular disease (CVD) prove costly as well with an average of 315.4 billion dollars spent on direct and indirect cost in 2010 for CVD and stroke. 2
A major goal of CVD prevention is to prevent or delay disease that may result in potentially devastating events. Landmark trials have illustrated the benefit of improving lipid profiles on CVD outcomes in primary and secondary prevention trials. 9 -12 Lipid-lowering drugs are employed to modify the risk of patients at risk of CVD by decreasing low-density lipoprotein cholesterol (LDL-C), the portion of the lipid panel revealed in epidemiologic and clinical studies to be the main cause of CHD. 1 The 3-hydroxy-methylglutaryl coenzyme A reductase inhibitors, also known as statins, are the most widely utilized class of lipid-lowering medications due to unequivocal evidence of its benefit in patients with CVD. Statins are the most potent drugs available for reducing LDL-C levels, lowering plasma cholesterol by 20% to 60%. Additionally, statins’ pleiotropic effects provide benefits to patients independent of the lipid lowering seen in other cholesterol medications. 13
Due to the established benefit of lipid-lowering therapy, medication management remains an integral focus in modification of CVD risk. Many factors may contribute to patients not receiving optimal drug therapy for primary and secondary CVD prevention including side effects, drug interactions, nonadherence, failure to titrate to appropriate dose, and inadequate follow-up. Furthermore, the incorporation of lifestyle management is extremely important to modify the risk of primary and secondary CVD events. Additional resources are needed to ensure patients are receiving appropriate care and education as the recommendations for lipid management advances. Pharmacists are well equipped to provide counseling to patients regarding the significance of lifestyle modification, safety and effectiveness of drug therapy, and alternative recommendations as needed. The National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) recommends utilizing pharmacists to improve adherence to lipid-lowering medication and outcomes in patients with CVD. 1 An updated cholesterol management guideline released by the American College of Cardiology (ACC)/American Heart Association (AHA) has broadened the use of statins and the recommendations for those needing statin therapy; therefore, pharmacists will be essential to providing care to these individuals as pharmacists have proven beneficial in an array of settings. 14
National Cholesterol Guidelines
The 2002 NCEP ATP III guidelines recommend individual risk assessment and treatment with lifestyle and lipid lowering for individuals with risk factors for CHD. These guidelines recommend a “treat to target” approach to LDL-C levels, which has been used extensively over the past 15 years (Table 1). 15 The primary recommended lipid-lowering medication are statins; however, additional pharmacotherapy (eg, bile acid sequestrants [BASs] or niacin) is suggested as monotherapy or in combination with statin therapy to assist patients in achieving their specified LDL-C target. 1 The 2013 ACC/AHA guideline on the treatment of blood cholesterol signifies a major divergence from the NCEP ATP III guidelines. The new guideline endorses initiation of moderate to high-intensity statin monotherapy to provide a desired percentage lowering of LDL-C in patients with atherosclerotic cardiovascular disease (ASCVD) based on 4 statin benefit groups (Table 2). Nonstatin therapy (ie, BAS, fibric acid derivatives, niacin, and cholesterol-absorption inhibitors) is only recommended in statin-intolerant patients after trial of alternative statin or dosing regimens. 15
Lipid-Lowering Goals and Recommended Low-Density Lipoprotein Cholesterol Levels for Drug Initiation From the National Cholesterol Education Program Interim Report.
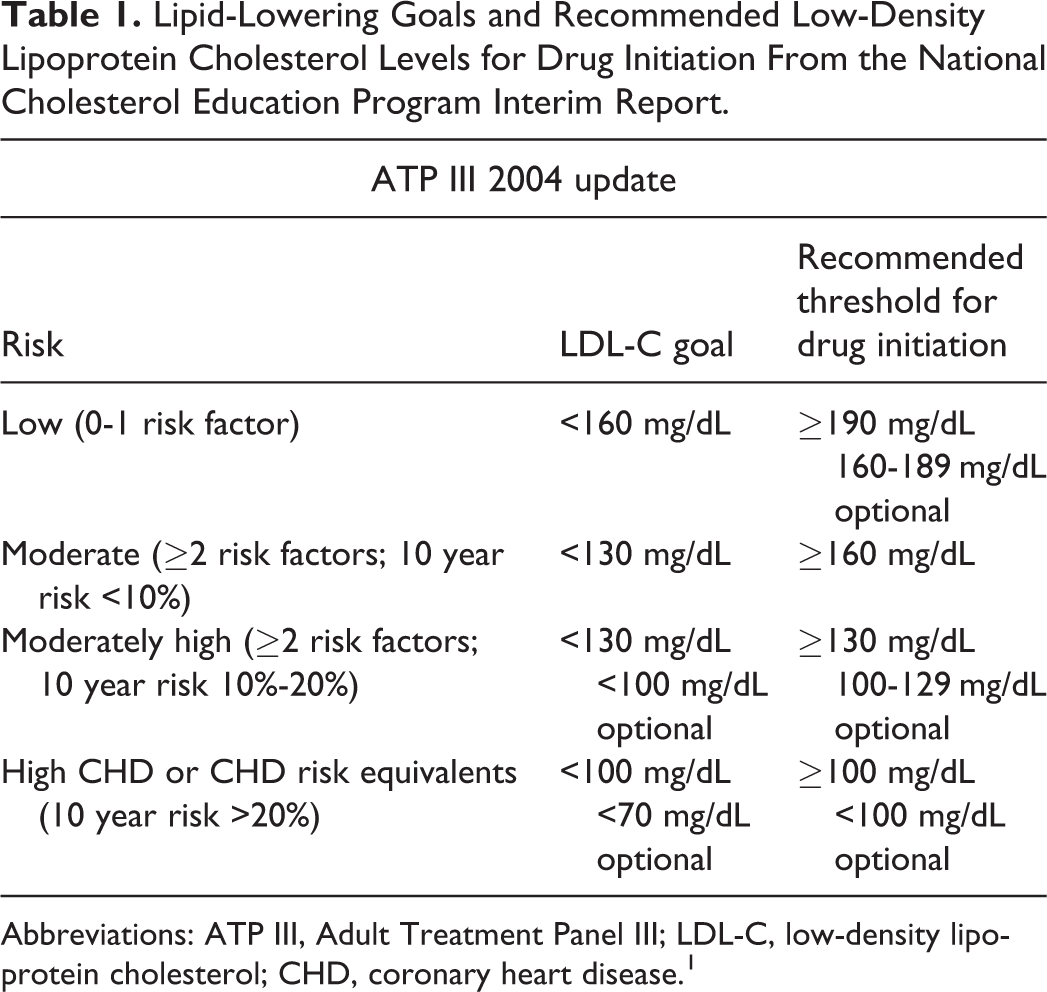
Abbreviations: ATP III, Adult Treatment Panel III; LDL-C, low-density lipoprotein cholesterol; CHD, coronary heart disease 1 .
Lipid-Lowering Recommendations From the 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults.
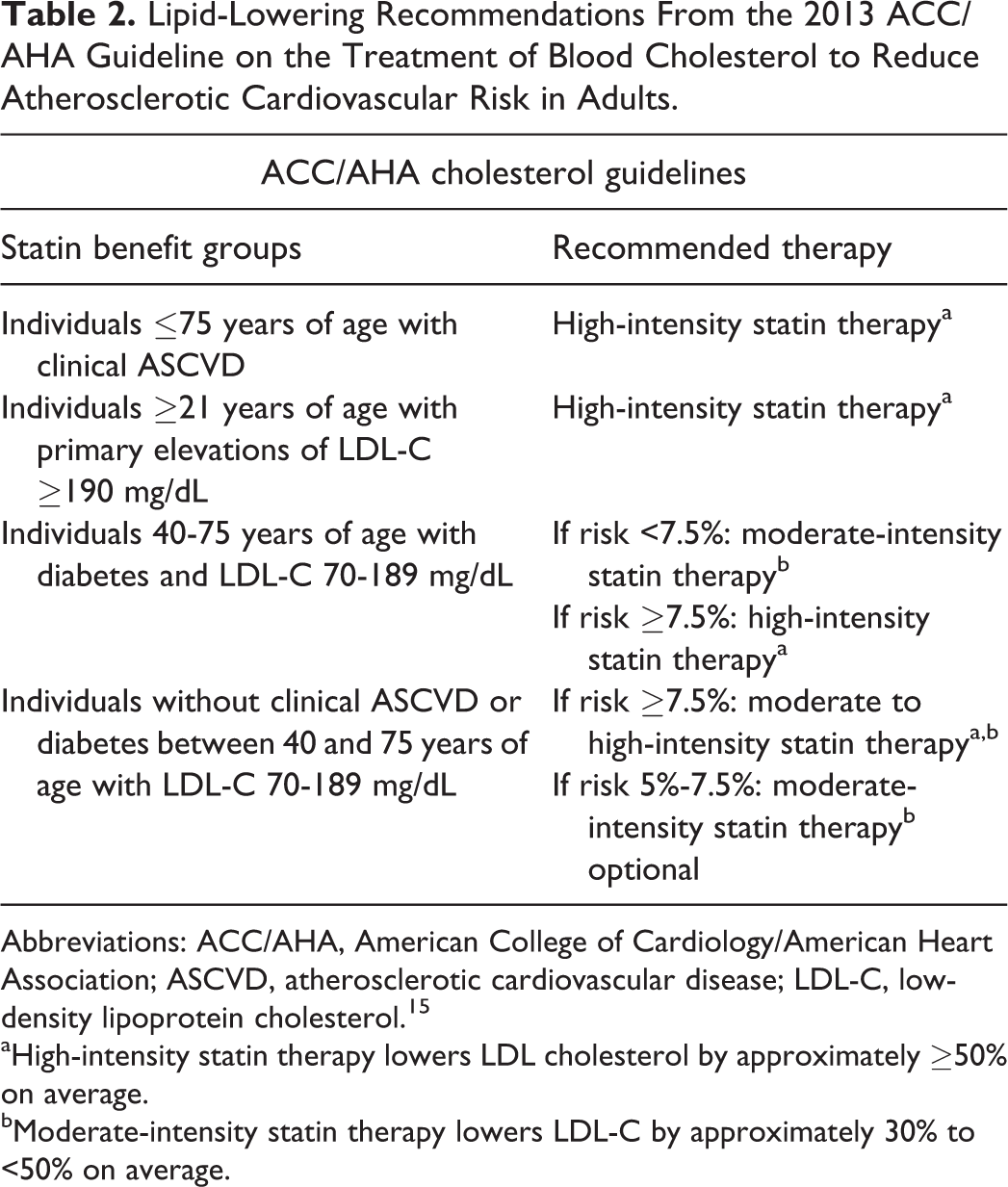
Abbreviations: ACC/AHA, American College of Cardiology/American Heart Association; ASCVD, atherosclerotic cardiovascular disease; LDL-C, low-density lipoprotein cholesterol 15 .
aHigh-intensity statin therapy lowers LDL cholesterol by approximately ≥50% on average.
bModerate-intensity statin therapy lowers LDL-C by approximately 30% to <50% on average.
The ACC/AHA guideline raises questions regarding the status quo of lipid management. Although the focus of drug therapy is evolving, pharmacotherapy remains the cornerstone of lipid management to optimize outcomes and decrease the devastation associated with CVD; therefore, pharmacists can play an integral role in lipid management. Pharmacists have assisted patients in achieving lipid targets per ATP III recommendations. Clinical pharmacists working in a group model health maintenance organization were able to assist 72.9% of patients with coronary artery disease achieve their LDL-C goal of less than 100 mg/dL compared to 25.5% at baseline. 16 Pharmacists worked in a collaborative practice model to help patients achieve a 4-fold increase in the number of patients obtaining LDL-C goals compared to the control cohort. 17,18 As the new guidelines are implemented patients and health care providers may become confused about monitoring and proper initiation of statin therapy. Pharmacists can prepare to provide education to patients and the health care team on guideline updates and implement lipid management services for patients. Pharmacists have the ability to provide screening to determine which patients should receive statin therapy, decrease nonstatin therapy use in appropriate patients, and monitor lipid profiles for improvement. In addition, pharmacists can prove themselves as a vital component of the health care team by providing recommendations on complex patients who may need additional therapy not specified in the guidelines to determine the most ideal treatment strategy for patients. As the projected amount of patients who may benefit from statin therapy grows, pharmacists’ assistance will be essential as additional resources are needed to properly care for patients.
Nonpharmacologic Therapy
Appropriate lifestyle modifications play an integral role in decreasing risks of patients with CHD. 1,19 Dietary modification and physical activity are 2 major facets of lifestyle management; however, weight control, smoking cessation, and limiting alcohol consumption also contribute greatly to overall cardiovascular health. 19 The therapeutic lifestyle changes (TLCs) approach was recommended by ATP III. 1 The AHA/ACC lifestyle management guideline does not include the TLC approach but recommends several other dietary patterns and approaches (ie, Dietary Approaches to Stop Hypertension diet, United States Department of Agriculture food pattern, and AHA diet) for patients to decrease CVD risks. 19 Recommendations for physical activity vary depending on patient specific factors; however, both guidelines recommend consistent moderate or vigorous intensity weekly activity to obtain the greatest health benefit. Interestingly, the amount of exercise plays a greater role in lipid profile modification than the intensity of exercise. 19 -21
Supplements are used by many patients for general health. The AHA recommends consistent consumption of ω-3 fatty acids obtained through diet or supplementation (eg, eicosapentaenoic acid and docosahexaenoic acid), despite controversy regarding its cardiovascular benefit. 19,22 Plant sterols and stanols appear to have beneficial effects on LDL levels as a study showed LDL-C levels lowered by 10% to 14% when participants consumed between 2 and 2.5 grams/day. 19,23 Of note, foods fortified with plant sterols/sterols usually have 0.5 to 1 g of sterol or stanols per serving. 24,25 Depending on the source, it may be difficult to consume the recommended amount of plant stanols/sterols through fortified foods to be of benefit. CholestOff®, tablet form of nonesterified plant sterols and stanols, has shown a 4.9% reduction in LDL and 2.8% reduction in total cholesterol over placebo in combination with TLC for 6 weeks in patients with hypercholesterolemia. 26 New guidelines do not advocate use of supplements to modify patients with CVD risks, which may decrease its application in the future.
A 3-month trial of lifestyle modifications before pharmacological intervention is suggested for many patients by cardiovascular guidelines. 1,19 Additionally, many patients desire to implement a nonpharmacological approach prior to medication initiation. One study found only 50% of patients were given the opportunity to change diet prior to starting statin therapy, despite the desire of 79% to initiate dietary changes prior to pharmacotherapy. 27,28 Providing patients the opportunity to be a decision maker in their health care may empower patients and allow them to “buy-in” to their treatment plan. Individualization of recommendations is key to providing lifelong changes for patients. In addition, the effects of the recommended dietary pattern continue as long as the diet is continued which highlights the importance of taking patient preferences into consideration. 15 The accessibility of pharmacists compared to nutritionist or dieticians provides a platform for the profession to become champions for lifestyle modifications. Patients should be instructed to balance calorie intake and physical activity to achieve or maintain a healthy body weight. Pharmacists can provide smoking cessation counseling, recommending nicotine or prescription therapy when needed, and stress the importance of moderation of alcohol consumption due to the potential for damage to vital organs (eg, heart and liver). 19,24,29 Implementation of appropriate lifestyle changes will allow patients to obtain the greatest benefit from lipid-lowering therapy.
Prevention and Management of Side Effects
Muscle symptoms are the most common adverse effects reported from statins and unfortunately, fear of rare but serious muscle toxicity remains a major impediment to the appropriate use of these drugs. 30,31 The cause of statin-induced myotoxicity has not been fully determined. Symptoms of myopathy usually begin within the first month of therapy; however, onset may appear later as well. The most common description of symptoms from patients includes muscular pain, tenderness, or weakness. Reported symptoms are characteristically bilateral and usually involve proximal muscles. 32 Most statin-induced myotoxicity is self-limiting and in most cases resolve within 2 months of discontinuing a statin but may persist long after exposure for 12 months or more. 27,33
Management of statin myopathy includes preventing symptoms, monitoring patients with symptoms, or creatine kinase elevations, using strategies to maintain patients on statin therapy if possible, selecting alternative therapy to lower lipids in statin intolerant patients, and constantly evaluating the risk versus benefits of statins in individual patients. 34 The first step of management of statin-induced myopathy begins with identifying a patient’s risk for the development of myopathy. ACC/AHA identifies high-risk patients to include those of advanced age (especially over 80 years and women at a higher risk than men), small body and frailty, multisystem disease (eg, chronic renal insufficiency especially due to diabetes), multiple medications, and perioperative periods. 15 Patients at higher risks of myopathy should be initiated on statins with caution and possibly started on lower doses if a strong likelihood of intolerance is expected. The statin could be later titrated up to its optimal dose if well tolerated. Correction of hypothyroidism and vitamin D deficiency should be a priority in management of statin-treated patients because both can be associated with statin-induced myotoxicity.
Patients who present with symptoms of myopathy while taking a statin should not be automatically discouraged from statin use altogether. Not all statins were created equal and intolerance to one statin does not necessarily reflect intolerance to the entire class. ACC/AHA guidelines support the initial use of high-dose statins in patients with ASCVD, so the optimal choice would be to change a patient to a different statin, that is, within the appropriate high or moderate intensity category for their risk stratification. As an alternative, titration to a lower tolerated dose is acceptable. Of note, hydrophilic statins (rosuvastatin and pravastatin) have been reported to have a lower risk of myopathy. Hydrophilic statins are less likely to enter nonhepatic cells such as myocytes and therefore may theoretically be less myotoxic. 35 In the Prediction of Muscular Risk in Observational Conditions (PRIMO) study, pravastatin and fluvastatin were the least likely to cause myalgia. 35,36 Fluvastatin XL has been proven in several studies to be well tolerated in patients who have failed other statins and is a suggested alternative to those who fail other statins. 37,38
Intermittent dosing of statins to address adverse effects without a complete compromise of the cholesterol lowering and CVD risk reduction benefits of statins has been supported in the literature and is recommended in the ACC/AHA guidelines prior to initiation of nonstatin therapy. The most extensively studied statins for intermittent dosing are rosuvastatin and atorvastatin given their longer half-lives (˜19 hours for rosuvastatin and 11-37 hours for atorvastatin). A retrospective analysis examined patients who were intolerant to daily statin therapy (76.5% due to myalgia and 19.5% due to elevated transaminases) and were switched to every other day rosuvastatin range 2.5 to 10 mg. The majority of patients tolerated the every other day rosuvastatin therapy (72.5%). The average LDL decreased 34.5% (P < .001). 27 If patients still present with muscle pain with every other day dosing, a possible alternative is to decrease the dose further to 3 times a week, which has been reported as well tolerated in some patients and provides greater benefit than complete discontinuation of a statin.
Coenzyme Q10 (CoQ10), or ubiquinone, is an end product of the mevalonate pathway, which is blocked by statins. Most studies show that statins lower serum CoQ10 levels. Small randomized, controlled trials have yielded conflicting result regarding CoQ10 supplementation and its clinical value in decreasing statin intolerance. 27 Inadequate evidence exists to definitively recommend CoQ10 supplementation.
In 2012, the FDA made several important revisions to statin labeling. One of those changes included decreasing the frequency of liver enzyme monitoring to baseline before initiating statin therapy and then as only clinically indicated thereafter. 39 The FDA concluded that serious liver injury with statins is rare and unpredictable in individuals, and routine monitoring does not appear to be effective in detecting or preventing liver injury. If liver enzymes are elevated >3 times the upper limit of normal, other causes should be further explored. Patients with liver cirrhosis, fatty liver, and chronic hepatitis B and C can be safely treated with a statin. 40 Information about the potential for generally nonserious and reversible cognitive side effects (memory loss, confusion, etc) and reports of increased blood sugar and glycosylated hemoglobin A1c levels have also been added to the statin labels. Data from observational studies and clinical trials do not suggest that these adverse effects are common. Therefore, given the overwhelming benefit of stains for risk reduction in CVD, the small increased relative risk does not outweigh benefit in patients whom statin therapy is recommended.
As many primary care physicians are faced with challenges in identifying regimens that patients can tolerate, pharmacists have proven to serve a vital role in the health care team as their ability to recommend well-tolerated regimens for patients on statins can increase the number of high-risk patients treated with statin therapy and potentially equate to CVD risk reduction. Since statins are the only agents with a robust body of evidence providing reduction in clinical end points, every effort should be made to keep high-risk patients on a statin-based regimen. 36 In many studies, pharmacist-managed clinics have been shown to improve dyslipidemia management and goal attainment compared with groups managed by primary care physicians. 27 Geber et al evaluated the level of care provided by clinical pharmacists as opposed to that furnished via standard care by physicians in patients with high baseline LDL and reported a significantly higher number of patients who attained their LDL goal among those receiving pharmacotherapy care compared to those receiving standard care. 41 Given pharmacists expertise in their ability to identify drug-related problems, obtain medication history, check for medication errors, identify drug interactions, monitor adverse drug reactions, and suggest individualization of treatment, they are well equipped to efficiently work collaboratively with providers and achieve comparable and in many cases superior outcomes.
Management of Drug Interactions
Drug interactions are a very important contributor to the risk of statin-associated adverse effects. Any drug that influences the pharmacokinetic properties of statins can affect their potential toxicity. These pharmacokinetic properties include hepatic metabolism via oxidation by cytochrome (CYP) isoenzymes or glucuronidation by the uridine diphosphate glucuronosyltransferase enzyme. 35 The CYP450 system is responsible for the microsomal metabolism of lovastatin, simvastatin, and atorvastatin, which creates the potential for drug interactions with a significant number of widely used medications. Lovastatin and simvastatin are highly reliant on CYP3A4 for elimination, whereas only about 20% of atorvastatin is metabolized by this isoenzyme. 42 Fluvastatin and to a lesser extent rosuvastatin are metabolized by CYP2C9. Pitavastatin is metabolized in the liver by glucuronidation and minimally by CYP2C9. 43 Pravastatin is the only statin not metabolized by the CYP450 system and is transformed enzymatically inside hepatocytes. 40
When statins must be used in combination with other CYP3A4 inhibitors, rosuvastatin, pravastatin, or fluvastatin are preferred to avoid interactions. In the presence of simvastatin, lovastatin, or atorvastatin, use of other drugs that inhibit the CYP3A4 system can lead to higher serum levels of statins and subsequently greater risk of myopathy. 44 Given the expansive number of medications that can interact with statin therapy providers must be vigilant of concomitant drug therapy, see Table 3.
Important Dose Limiting Drug Interactions With Statins.a
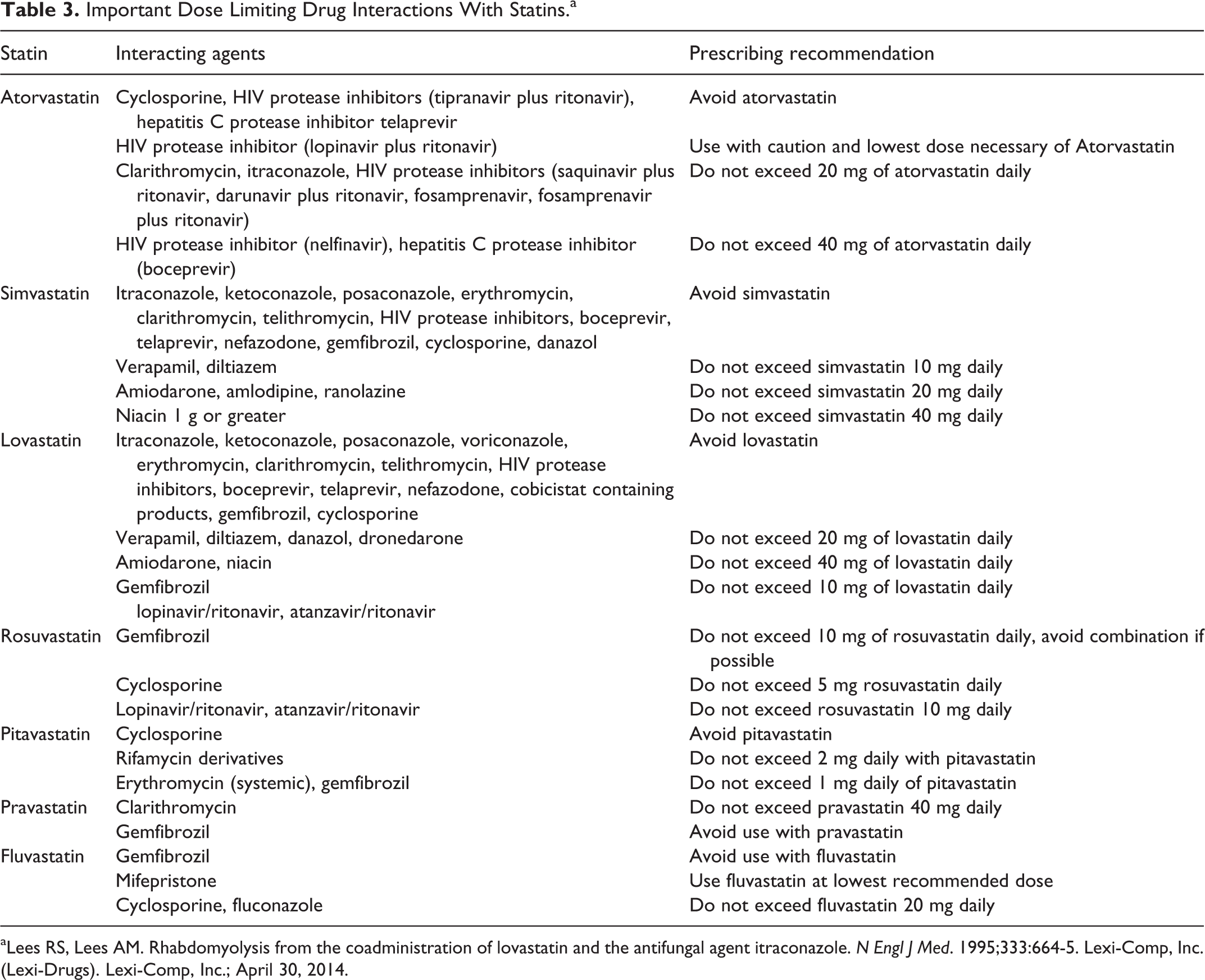
aLees RS, Lees AM. Rhabdomyolysis from the coadministration of lovastatin and the antifungal agent itraconazole. N Engl J Med. 1995;333:664-5. Lexi-Comp, Inc. (Lexi-Drugs). Lexi-Comp, Inc.; April 30, 2014.
Although many organizations have systems in place to prevent drug–drug interactions both at medication order entry and dispensing, there are often many interactions that may slip through the cracks or go unrecognized due to the fact that patients may use multiple pharmacies and not report complete use of over-the-counter medications as well as herbals. Pharmacists still play a key role in identifying potential medication issues as they counsel the patients upon dispensing medications. A randomized trial by Lipton et al evaluated a clinical pharmacist intervention involving 736 elderly patients discharged from a community hospital and taking ≥3 medications for chronic conditions. The pharmacist reviewed the drug regimens of these patients to identify drug-related problems and made recommendations to the patient’s physician. In comparison to the placebo group, the drug therapy regimens were significantly more appropriate in the intervention group, the intervention group was on less complex regimens, were more knowledgeable about the purpose of their medications, and were more compliant to their regimen. 45 This highlights that despite the use of electronic systems, there is still a significant role for pharmacist to further improve patients’ drug therapy regimens from both a safety and efficacy standpoint.
Patient Adherence
Adherence is a significant factor after lipid-lowering therapy initiation because patients receive the most benefit from lipid-lowering therapy with long-term use. It has been reported that only 50% of patients prescribed lipid-lowering medications continue taking their medication after 6 months. 46 This figure continues to drop as time goes on with an estimate of 30% to 40% adherence a year after the lipid-lowering medication is prescribed. These statistics are troublesome considering the need for chronic management of lipids to achieve the cardiovascular benefits associated with LDL lowering. Furthermore, patient nonadherence is related to increased hospitalization, decreased productivity, and premature death. 27,47
Factors leading to nonadherence to lipid-lowering therapy include medication side effects, patient’s perception of inconvenience due to treatment, regimen complexity, treatment cost, and time between diagnosis and treatment. 27 Additionally, younger age, cost, no monitoring, and perception of risk have also been linked to nonadherence. 27,28,48 Pharmacists can play a significant role in modifying many of these barriers to adherence. Patient education on the importance of pharmacotherapy to reduce CVD risks may raise awareness and modify patients’ adherence and behavior. The recommendation for statin monotherapy versus combination lipid-lowering therapy to meet LDL targets in high-risk patients may prove beneficial to patient adherence as several nonstatin lipid-lowering therapy have more complex dosing regimens. Medication affordability continues to be a major concern for patients, especially individuals on fixed incomes. As more statins become generic, the cost of statin therapy decreases allowing more patients to obtain their prescriptions. Pharmacists can play an integral role in making providers and patients aware of the ACC/AHA recommendations and potentially eliminating or minimizing combination therapy with nonstatin therapy as appropriate. Pharmacists in clinics and hospitals have the opportunity to minimize the gap between patients’ diagnosis and treatment. Project ImPACT resulted in high rates of patient compliance with prescribed treatment regimens in patients collaborating with both physicians and pharmacists. 49 Statins are often prescribed at nighttime potentially leading to patients forgetting to take their medication. Several statins have long half-lives eliminating the need for bedtime dosing; therefore, patients forgetting to take a statin recommended for night use can be switched to an alternative statin therapy without timing recommendations. Additionally, associating medications with a daily routine can decrease inconvenience and prove helpful to patient adherence rates. 50
Pharmacists are among the most trusted professions in the nation. A positive relationship with a pharmacist is likely to improve adherence as increased patient satisfaction with patient’s physician has been associated with increased adherence. 50 Adherence signifies a choice that patients make to be a partner in their health care. It is important that pharmacists continue to emphasize the benefits of therapy to help patients achieve their goals.
Failure to Titrate to Appropriate Dose
Lipid-lowering therapy is most valuable when titrated to the appropriate dose. A significant subset of patients continue on their initial doses of lipid-lowering medications without achieving recommended goals. 51 A community-based study showed that lipid management in a typical outpatient setting frequently failed to reach the target levels recommended by national guidelines for secondary prevention leading to increased cardiac events. 52 Furthermore in the Lipid Treatment Assessment Project, only 18% of patients with CHD achieved goal NCEP LDL. 53 Proper titration can be a challenge due to limited time and resources. In addition, individuals taking complex medication regimens may get confused with titration and continue initial therapy. Patients may feel a sense of guilt or failure when medication is titrated and as a result be more reluctant to take higher doses of medication.
Statin therapy can be initiated at high doses to allow patients to achieve treatment goals. 1,54 The likelihood of side effects does not substantially increase with higher doses compared to lower doses; therefore, aggressive therapy initiation may prevent failure to appropriately titrate in the future. 54 Moreover, the concern of inappropriate titration may be alleviated by the ACC/AHA recommendations that recommend statin monotherapy—allowing patients to start and continue specified therapy—versus targeting a LDL goal. Pharmacists can be of benefit through lipid clinics, involvement of pharmacists in reinforcing compliance with refills, review, and counseling of discharge medications during the transition from hospital to the community, close follow-up, and educating prescribers to initiate recommended doses of statin therapy. A randomized, controlled trial evaluating community pharmacist’s interventions in lipid management was terminated early due to the benefit found in the cohort receiving pharmacists care versus usual care. The primary end point was the composite of fasting lipid panel, initiation of a new lipid-lowering drug, or titration of a lipid-lowering medication. 53 This highlights the skills of pharmacists to provide benefit in collaboration with physicians to assist patient in achieving goals.
Inadequate Follow-Up
Approximately 33.5% of US adults ≥20 years of age had high LDL but only 33.2% had “controlled” LDL according to data from 2005 to 2008. 1 Patients may not achieve lipid-lowering goals due to inadequate follow-up as lipid control remains low in patients with limited access to health care. 16,55 As previously emphasized, proper titration of drug therapy is necessary for optimal management of hyperlipidemia. The focus of routine office visits is often centered on patients’ acute concerns versus optimization of medication therapy. 51 As a result, chronic disease states may not be actively followed. Of note, only 7.8% of office visits measure or order cholesterol levels and only 15.7% of office visits report hyperlipidemia on the medical record. 56 These shocking statistics highlight the gap between the actual screening and treatment of dyslipidemia to decrease CVD risks.
Pharmacist played a vital role in helping patients achieve their lipid goals through a pharmacist-managed, physician monitored service in patients with coronary artery disease. 16 These pharmacists incorporated close follow-up through a tracking system to prevent losing patients to follow. As a result, 73% of the CAD population achieved their lipid goals, which far exceeds the present national average. 16,56 Of note, cholesterol screening increased by over 30% in patients followed by clinical pharmacists (66.9%-97.3%) compared to usual practice. 16 Pharmacist followed up with patients in the office, via phone, and through mail providing both lifestyle and pharmacotherapy recommendations. Pharmacists can provide long-term follow-up to aid in patient achieving disease state goals. 17 Pharmacists can send patient reminder letters, schedule patients for follow-up via phone or office visits. 16
Conclusion
CVD management can pose many challenges to health care professionals. The adoption of the new ACC/AHA guidelines, which call for more aggressive therapy than that of previous guidelines means that a much larger proportion of individuals will require optimization of cholesterol therapy further complicating the management of CVD. Patients must often overcome many obstacles before benefit of statins are maximized. Cumulative evidence exists in the literature, which supports the benefit of the presence of clinical pharmacists in CVD management. As a part of a multidisciplinary team, pharmacists play a key role in lipid management therapy. Because of their accessibility to both patients and physicians, as well as their extensive knowledge base regarding drug therapy, pharmacists are in a unique position to provide appropriate collaboration to ensure successful treatment that can lead to a substantial reduction in disease burden and overall health care cost.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.