
Abstract
Hypertension affects 80 million people in the United States. It remains poorly controlled, with only 54% of diagnosed patients treated to blood pressure targets. Hypertension management is complex in part due to the volume of antihypertensive agents, variable patient needs and responses, and inconsistent design and outcomes from clinical trials. Therefore, trustworthy clinical practice guidelines have a key role in hypertension management. The United States experienced a 10-year gap in publication of hypertension guidelines, followed by multiple guideline publications in 2013. These guidelines led to more controversy than clarity, as there was discordance among them. This review summarizes the guidelines and clinical statements influencing the current debate in order to facilitate appropriate application.
Introduction
Cardiovascular diseases, such as hypertension, heart failure, and coronary artery disease, have been the number one cause of death in the United States nearly every year since 1900. 1 Hypertension is one of the most prevalent of these cardiovascular diseases, affecting almost 80 million US adults, with projections indicating that the prevalence will continue to grow over the next 15 years. 1,2 The consequences of uncontrolled hypertension are serious. Hypertension is a major risk factor leading to other cardiovascular diseases, including stroke, coronary artery disease, and heart failure, but hypertension is also directly associated with morbidity and mortality. More than 43 million office visits and 280 000 hospitalizations were associated with hypertension in 2010, and in 2011, a total of 63 000 deaths were directly attributed to hypertension. 1 Further, the impact of hypertension on financial resources is substantial. In 2011, the direct and indirect cost related to hypertension exceeded $46 billion US dollars. 1
Hypertension is generally regarded as a condition that is treatable, yet only 54% of patients diagnosed are being treated to their appropriate blood pressure (BP) goals. 1 The reasons for the suboptimal control are multifaceted and likely include factors related to the patient and provider, as well as issues within the US health system, such as fragmented care and lack of consistent clinical practices. 3 The volume of antihypertensive options also complicates hypertension management. More than 50 individual antihypertensive agents within 14 drug classes are available in the United States, increasing the risk of unsystematic medication selection. 4 Further, antihypertensive selection and titration is highly nuanced and requires clinicians to integrate nearly 50 years of clinical evidence with various patient factors and individual responses to therapy. Thus, application of evidence-based, comprehensive clinical practice recommendations plays an indispensable role in provision of optimal hypertension management. In fact, the American Heart Association (AHA), the American College of Cardiology (ACC), and the Centers for Disease Control and Prevention (CDC) published a scientific advisory statement in November 2013 calling for a system-wide approach to achieve BP control. 3 The authors of this statement assert that implementation of an effective practice guideline is a crucial ingredient to improving attainment of BP goals in the United States. 3
In spite of the recognition that hypertension guidelines are vital, the medical community recently experienced an extended season without updated hypertension recommendations. In 1977, The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC) began publishing hypertension guidelines, which evolved to become the authoritative resource for hypertension management in the United States. 5 The JNC recommendations were customarily updated every 4 to 6 years, a frequency that continued though JNC 7, which was published in 2003. 6 The update to JNC 7, however, was protracted. By early 2013, JNC 8 was still not published, marking the longest interval between JNC publications in the history of the program. Then, between July and December 2013, hypertension recommendations from multiple groups, including JNC 8, were disseminated, leading to an unprecedented volume of hypertension statements distributed virtually simultaneously. 3,4,7,8 Although the guidelines are from reputable organizations, they differ in their process for development, objectives, transparency, and several key recommendations, creating uncertainty rather than clarity with regard to hypertension management among the medical community.
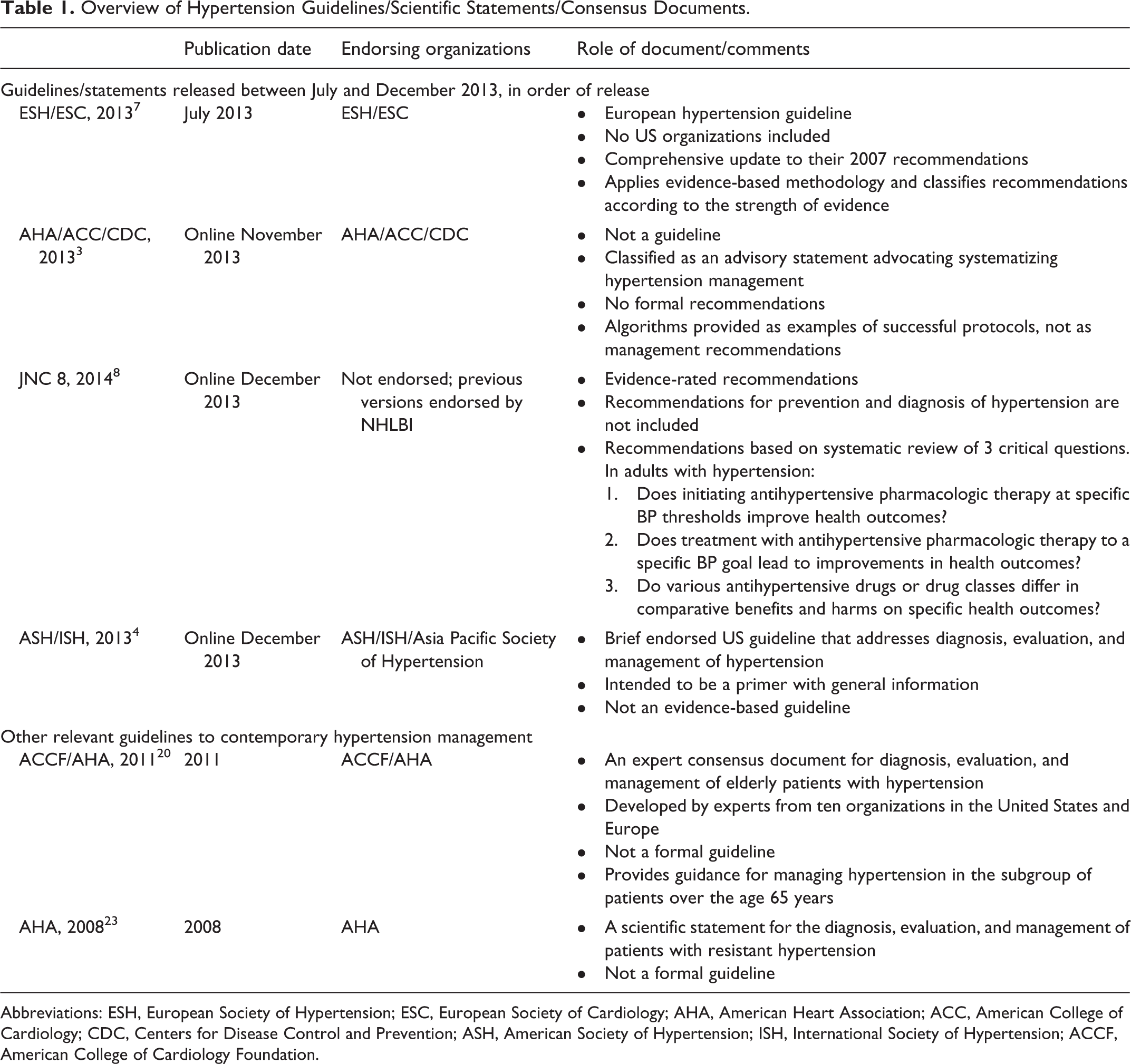
The objective of this article is to review the guidelines, scientific statements, and consensus documents influencing the debate surrounding contemporary hypertension management. The development method, intention of the authors, scope, and key recommendations will be summarized. The 4 hypertension guidelines or statements released in 2013 will be reviewed first (in order of release), followed by an overview of guidelines, documents, and statements in important subgroups to facilitate comparison, interpretation, and application of the various hypertension recommendations. Tables 1 to 3 provide an overview and comparison of these guidelines, scientific statements, and consensus documents.
Overview of Hypertension Guidelines/Scientific Statements/Consensus Documents.
Abbreviations: ESH, European Society of Hypertension; ESC, European Society of Cardiology; AHA, American Heart Association; ACC, American College of Cardiology; CDC, Centers for Disease Control and Prevention; ASH, American Society of Hypertension; ISH, International Society of Hypertension; ACCF, American College of Cardiology Foundation.
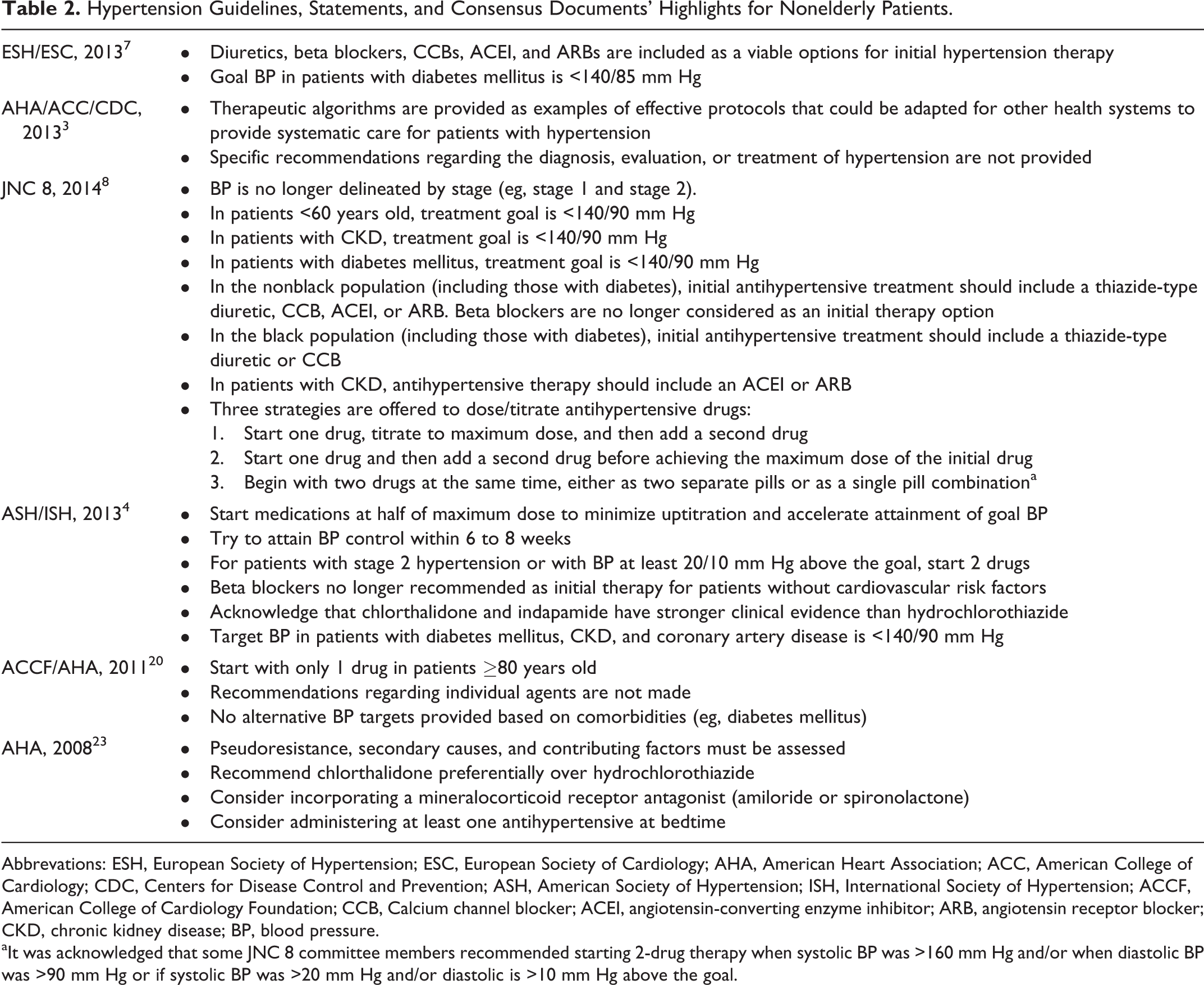
Hypertension Guidelines, Statements, and Consensus Documents’ Highlights for Nonelderly Patients.
Abbrevations: ESH, European Society of Hypertension; ESC, European Society of Cardiology; AHA, American Heart Association; ACC, American College of Cardiology; CDC, Centers for Disease Control and Prevention; ASH, American Society of Hypertension; ISH, International Society of Hypertension; ACCF, American College of Cardiology Foundation; CCB, Calcium channel blocker; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CKD, chronic kidney disease; BP, blood pressure.
aIt was acknowledged that some JNC 8 committee members recommended starting 2-drug therapy when systolic BP was >160 mm Hg and/or when diastolic BP was >90 mm Hg or if systolic BP was >20 mm Hg and/or diastolic is >10 mm Hg above the goal.
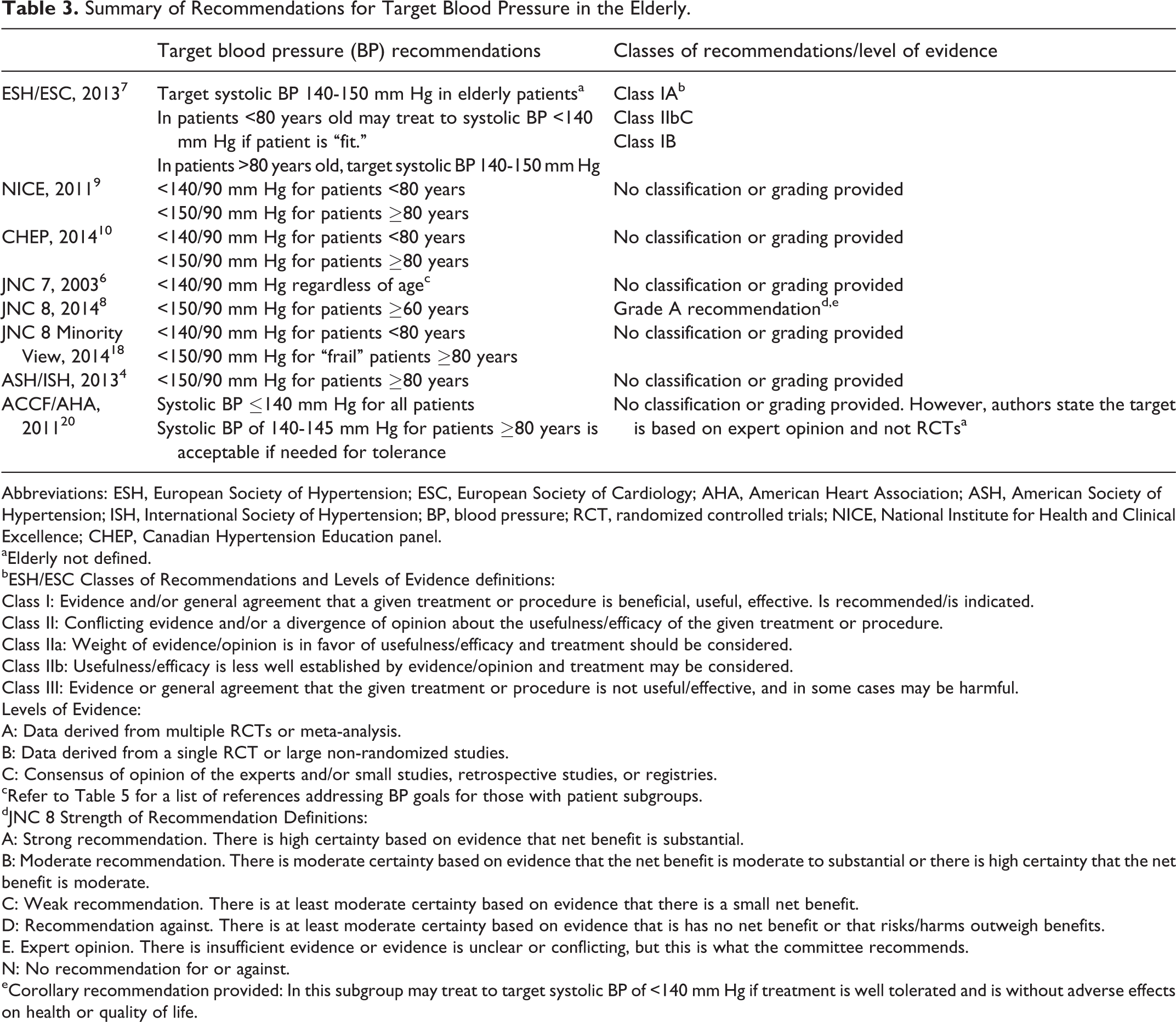
Summary of Recommendations for Target Blood Pressure in the Elderly.
Abbreviations: ESH, European Society of Hypertension; ESC, European Society of Cardiology; AHA, American Heart Association; ASH, American Society of Hypertension; ISH, International Society of Hypertension; BP, blood pressure; RCT, randomized controlled trials; NICE, National Institute for Health and Clinical Excellence; CHEP, Canadian Hypertension Education panel.
aElderly not defined.
bESH/ESC Classes of Recommendations and Levels of Evidence definitions:
Class I: Evidence and/or general agreement that a given treatment or procedure is beneficial, useful, effective. Is recommended/is indicated.
Class II: Conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of the given treatment or procedure.
Class IIa: Weight of evidence/opinion is in favor of usefulness/efficacy and treatment should be considered.
Class IIb: Usefulness/efficacy is less well established by evidence/opinion and treatment may be considered.
Class III: Evidence or general agreement that the given treatment or procedure is not useful/effective, and in some cases may be harmful.
Levels of Evidence:
A: Data derived from multiple RCTs or meta-analysis.
B: Data derived from a single RCT or large non-randomized studies.
C: Consensus of opinion of the experts and/or small studies, retrospective studies, or registries.
cRefer to Table 5 for a list of references addressing BP goals for those with patient subgroups.
dJNC 8 Strength of Recommendation Definitions:
A: Strong recommendation. There is high certainty based on evidence that net benefit is substantial.
B: Moderate recommendation. There is moderate certainty based on evidence that the net benefit is moderate to substantial or there is high certainty that the net benefit is moderate.
C: Weak recommendation. There is at least moderate certainty based on evidence that there is a small net benefit.
D: Recommendation against. There is at least moderate certainty based on evidence that is has no net benefit or that risks/harms outweigh benefits.
E. Expert opinion. There is insufficient evidence or evidence is unclear or conflicting, but this is what the committee recommends.
N: No recommendation for or against.
eCorollary recommendation provided: In this subgroup may treat to target systolic BP of <140 mm Hg if treatment is well tolerated and is without adverse effects on health or quality of life.
2013 European Society of Hypertension/European Society of Cardiology Guidelines for the Management of Arterial Hypertension
The European Society of Hypertension (ESH) and the European Society of Cardiology (ESC) published updated hypertension guidelines in July 2013. 7 Although no US organization participated in the development of these guidelines, the lack of up-to-date recommendations in the United States at the time of this publication rendered these guidelines significant to US clinicians. Thus, the European guidelines became a factor in the debate regarding the hypertension guidelines that ensued over the following months.
The ESH/ESC guidelines were developed with 3 overarching principles: (1) the recommendations were based on studies identified during an extensive review of the literature; (2) randomized controlled trials (RCTs) were given the highest priority from which they based recommendations, though other study designs (eg, meta-analyses and observational data) were not disregarded; and (3) evidence supporting the recommendations were classified and graded based on the level of scientific evidence (eg, Class I, Level of Evidence A is the strongest recommendation). These guidelines provide recommendations for comprehensive hypertension management (detection, evaluation, and treatment). Many of the recommendations found in the ESH/ESC guideline are concordant with other contemporary hypertension guidelines, with one notable exception. The ESH/ESC did not exclude beta blockers as one of the options for first-line antihypertensive treatment. Their justification for maintaining beta blockers as an initial treatment option, along with diuretics, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, and calcium antagonists, was that the evidence was mixed when comparing clinical outcomes to those of other antihypertensives. The authors also contend that the newer, vasodilating beta blockers (eg, carvedilol and nebivolol) do not appear to have the same pharmacodynamic limitations (eg, altered insulin sensitivity), as some of the older beta blockers used in the analyses that cast doubt on beta blockers’ clinical effects. Overall, the authors take the position that the data are not strong enough to exclude beta blockers from the list of initial options. Another recommendation that is noteworthy is in regard to systolic BP goals in elderly patients. In the opinion of the ESH/ECS panel, the goal systolic BP for elderly patients should be between 140 and 150 mm Hg. Importantly, the panel does not specifically define “elderly” but does make the concession that some elderly patients are more “fit,” in which case the systolic BP goal may be <140 mm Hg.
Overall, the ESH/ESC hypertension guidelines provide a meticulous and comprehensive review that can be edifying for clinicians, even if direct application is limited by different health systems, standards of care, or medication availability in Europe compared to the United States. Other non-US hypertension guidelines, including the National Institute for Health and Clinical Excellence (NICE, published 2011) and the Canadian Hypertension Education panel (CHEP, updated annually), can also serve as resources for providers, although a comprehensive assessment of international hypertension guidelines is beyond the scope of this article. 9,10 Nonetheless, the recommendations from both NICE and CHEP for target BP in the elderly with hypertension are included for reference in Table 3, since target BP in elderly patients is one of the recommendations at the forefront of the current hypertension debate.
An Effective Approach to High BP Control: A Science Advisory From the AHA, the ACC, and the CDC
In November 2013, the AHA, ACC, and CDC published an advisory statement to address the impact suboptimal BP control has on cardiovascular disease morbidity and mortality in the United States. 3 Since only 54% of those diagnosed with hypertension are being treated to their target BP goals, many patients are at risk of cardiovascular events and death. The AHA and CDC developed programs with specific nation-wide goals to reduce these events in the United States. The purpose of this AHA/ACC/CDC publication is to endorse standardized hypertension treatment to help achieve national goals defined by these programs. An important distinction of the AHA/ACC/CDC advisory statement is that it is not intended to be a clinical practice guideline, although it has been misinterpreted as such in the medical literature. 11,12
Although there are no specific hypertension management recommendations in this advisory, the authors provide 2 examples of management algorithms as well as a link to an online resource for additional treatment algorithms for the reader. An important distinction is that the provision of these hypertension management algorithms through this scientific advisory panel is not to offer hypertension recommendations, per se, but rather to provide tools and support to clinicians and/or health care systems to facilitate development of a standard and well-defined approach to hypertension management.
The timing from this advisory panel can add to the obfuscation that currently surrounds hypertension guidelines, since the AHA/ACC/CDC advisory statement was published 3 months after the National Heart, Lung, and Blood Institute (NHLBI) announced that the AHA and ACC would assume responsibility for creating and disseminating the future hypertension guidelines. 13 The difficulty with distinguishing the advisory statement from a bonafide guideline became clear when the authors of the statement were criticized for not adhering to guideline standards, requiring AHA and ACC leadership to reiterate that the AHA/ACC/CDC advisory statement is not a guideline for hypertension management. 11,12 The overall role of this scientific advisory statement is to support and endorse standardized care for hypertension management and to provide examples of protocols or algorithms that have been shown to be effective in real-world health care settings.
2014 Evidence-Based Guidelines for the Management of High BP in Adults: Report From the Panel Members Appointed to the Eighth Joint National Committee
In 2008, the Eighth JNC writing group was commissioned by the NHLBI to update JNC 7. 8 The JNC 8 committee introduced several changes to improve the guideline development process that ultimately led to a published document that is considerably different from prior JNC guidelines. Then, in 2013, after the JNC 8 committee had essentially completed their work, the NHLBI announced that they would transfer the mission of guideline development to external organizations so that the NHLBI could focus on their leadership role in health education. 14 The 5 pending guidelines commenced by the NHBLI (including hypertension) would be published as evidentiary reviews rather than as formally endorsed guidelines, in order to align with the NHLBI mission of knowledge generation and production of systematic reviews. 14 As such, the NHLBI no longer endorsed the JNC 8 panel as a guideline writing committee. Therefore, several important distinctions regarding JNC 8 are vital for proper application to clinical practice.
To begin, JNC 8, published online in December 2013, is not the hypertension guideline that comprehensively updates JNC 7. 13 –15 The AHA and ACC jointly accepted responsibility for developing and managing cardiovascular guidelines from the NHLBI, and are presently developing the official updated hypertension guideline, The American Society of Hypertension (ASH) subsequently agreed to collaborate with AHA and ACC after the initial announcement was made. 16 The JNC 8 panel chose to publish their work independent of NHLBI to provide timely, up-to-date, evidence-based hypertension recommendations, since it was recognized that the transfer of guideline writing responsibility could impart additional delays in guideline availability.
Another distinction of the JNC 8 publication is in regard to the methodology applied to developing their recommendations. The JNC 8 panel employed a systematic review process to develop their recommendations, while prior JNC panels used nonsystematic reviews. Since the JNC 8 group was the first to conduct a systematic review, the literature search and review was comprehensive and included studies from 1966 through 2009, which represents a time-intensive process that was a factor in the delay of their update. The use of a structured systematic review also provided the foundation for the JNC 8 committee to create standards to grade the evidence so that the strength of recommendations could be consistently articulated to the reader. Another important procedural difference applied by the JNC 8 committee was that the panel limited its review of evidence from which to base their recommendations to only RCTs, citing that RCTs are the gold standard for determining efficacy and effectiveness, in order to eliminate bias from uncontrolled studies. 8
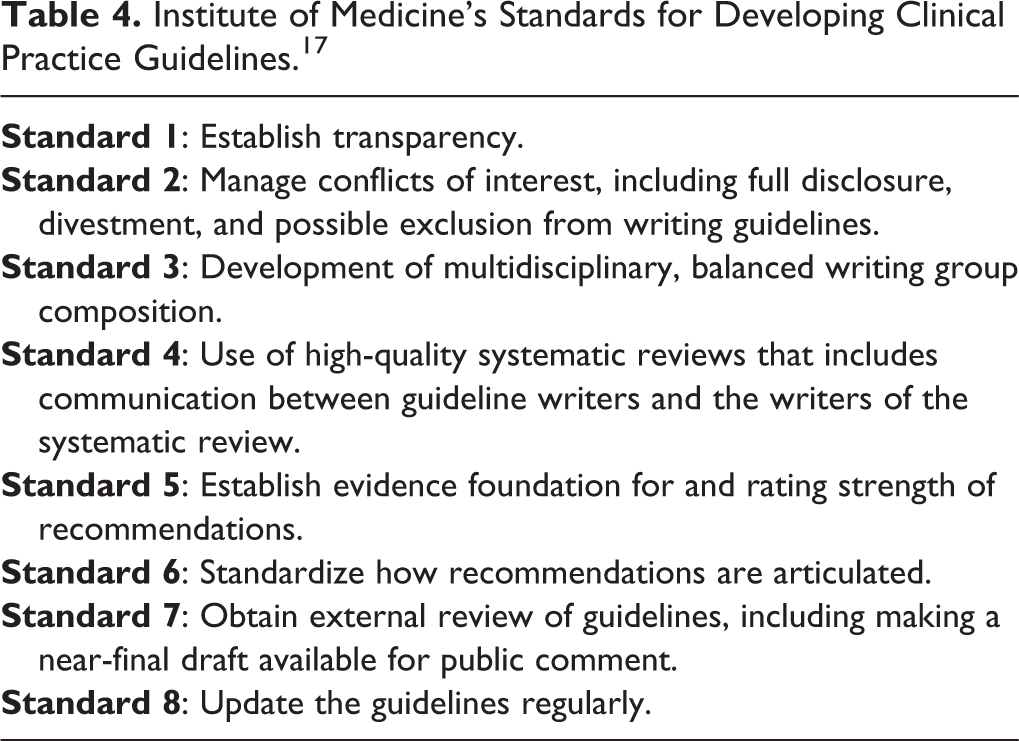
The methods used by the JNC 8 panel are closely aligned with the standards for development of clinical practice guidelines as recommended by the Institute of Medicine (IOM). In 2011, the IOM published 8 standards to define methods for developing trustworthy clinical practice guidelines (Table 4). 17 The JNC 8 panel attempted to comply with the standards, although JNC 8 development was well underway by 2011. Nonetheless, JNC 8 adheres to these standards to a greater degree than any other US hypertension statements released in 2013. 3,4,8 In particular, the panel committed to transparency with their process (including acknowledgement when consensus could not be achieved), inclusion of a multidisciplinary committee, use of a systematic review process for developing the recommendations, use of external peer review, and provision of a guideline draft to public organizations for review. The authors also provided details regarding how the evidence quality was rated and defined the standard language for communicating the recommendations.
Institute of Medicine’s Standards for Developing Clinical Practice Guidelines. 17
Importantly, although the JNC 8 committee applied a rigorous process, the guidelines are limited in scope and will not be sufficient as a stand-alone set of recommendations. Rather than providing a set of comprehensive recommendations for prevention, detection, evaluation, and treatment of high BPas done in prior JNC guidelines, the committee selected the 3 highest ranked clinical questions, as determined by the JNC 8 panel, which focus on the threshold and goals of pharmacologic treatment of hypertension to guide their systematic review (Table 1). The committee developed 9 recommendations within the scope of these three clinical questions (Tables 2 and 3).
Of the 9 recommendations provided in the 2014 JNC 8 guidelines, one recommendation has been the source of intense scrutiny and debate. According to the JNC 8 recommendations, clinicians should initiate pharmacologic treatment to lower BP when systolic BP is ≥150 mm Hg and/or diastolic BP is ≥ 90 mm Hg and treat to a goal of <150/90 mm Hg in the general population aged 60 years and older. The JNC 8 authors acknowledged that this recommendation was not unanimously supported and provided a corollary recommendation to not adjust therapy in those patients 60 years or older whose systolic BP is titrated to <140 mm Hg without adverse effects. The lack of consensus for this recommendation led to the publication of a “Minority View” from the 5 JNC 8 committee members who were not supportive of increasing the systolic BP goal to 150 mm Hg in patients over 60 years of age. 18 The minority group identified 3 reasons for not changing the target systolic BP of ≤140 mm Hg in patients aged 60 years or older. First, the panel cited concerns about the potential for loss of intense BP control in high-risk groups, including African American patients and those with multiple cardiovascular risk factors. Second, although the panel conceded that randomized controlled evidence was lacking to support the BP goal of ≤140 mm Hg in patients 60 years or older, they also argued that no evidence supported increasing the threshold in this population. Finally, the authors felt less intense BP control could reverse the declining rates of cardiovascular morbidity and mortality realized over the last 3 decades. The ensuing controversy was significant and included an unprecedented call to the Journal of the American Medical Association to retract the JNC 8 publication. 19 Critics of the controversial recommendation from JNC 8 assert that the totality of the evidence regarding BP goals in those aged 60 and older was not considered, since the panel chose to use only RCTs as the basis for their recommendations. 16,18 Importantly, although JNC 8 has been in the spotlight for their recommendation about the BP target in older patients, the debate is not relegated to only JNC 8 recommendations. Indeed, there is discordance among almost all of the hypertension guidelines or statements regarding BP goals in elderly patients with hypertension. A summary of the recommendations for BP goals among elderly patients from the major hypertension guidelines and statements can be found in Table 3.
Overall, the JNC 8 recommendations have a distinctive role in the milieu of hypertension guidelines. The guidelines are radically different from prior JNC publications, are not officially endorsed, and are not comprehensive. The merit of using only RCTs for developing clinical recommendations is controversial. On one hand, the use of RCTs exclusively provides a strong degree of confidence of recommendations provided by the guideline. Conversely, the exclusion of non-RCT data (eg, meta-analyses, observations studies) precludes development of recommendations based on the evidence in its entirety. The use of graded recommendations and level-of-evidence statements should provide guideline developers the latitude needed to make recommendations regarding the ambiguous areas of hypertension management and mitigate the need for such restriction. It is noteworthy that the most controversial recommendation from the JNC 8 writers was based on the “gold standard” clinical trial design and was given a grade A recommendation. One advantage of the exclusive approach taken by the JNC 8 committee is that it draws attention to the fact that recommendations that have been inculcated into hypertension management, such as target BP goals, have critical gaps and require additional investigation. Ultimately, the meticulous process, adherence to the standards for developing clinical practice guidelines, and transparency are noteworthy and represent several important advancements in the guideline development process.
Clinical Practice Guidelines for the Management of Hypertension in the Community. A Statement by the American Society of Hypertension and the International Society of Hypertension Clinical Practice Guidelines
Also in December 2013, ASH, in collaboration with the International Society of Hypertension (ISH), issued a clinical practice guideline for the management of hypertension. 4 In contrast to recommendations reviewed thus far, this publication is a hypertension guideline that is endorsed by ASH, ISH, and the Asia Pacific Society of Hypertension. However, the guideline, which included 3 authors who were also on the JNC 8 panel, was intended to be an international primer with general hypertension recommendations for an international audience rather than a comprehensive hypertension guideline. 16 The authors recommend that readers do not consider this guideline as an evidence-based set of recommendations.
In spite of these shortcomings, of all the hypertension recommendations released between July and December 2013, the ASH/ISH guideline is the only publication that is a formally endorsed guideline for managing hypertension in the United States. Several recommendations from these guidelines are noteworthy (Tables 2 and 3). Briefly, the authors state that hypertension is generally defined as systolic BP >140 mm Hg or diastolic BP >90 mm Hg but that a systolic BP up to 150 mm Hg is considered acceptable in patients 80 years of age or older. It is noteworthy that this age threshold for increasing the BP goal is 20 years older than what is recommended by the JNC 8 panel. The authors also advocate for a goal of <140/90 for most patients, including those with diabetes and chronic kidney disease (CKD), although it was acknowledged that many expert groups recommend a target BP of <130/80 in patients with albuminuria. The writers do not make a recommendation for a BP target explicitly in patients with albuminuria. This guideline is also more prescriptive than others regarding the intensity with which therapy should be selected and uptitrated. The writers of this guideline specify that the initial antihypertensive dose should be half of the maximum dose so as to reduce the number of dose adjustments and accelerate attainment of an effective regimen within 6 to 8 weeks of initiating therapy. Further, in contrast to many other guidelines that refrain from making recommendations about specific agents within medications classes, these guidelines advocate for indapamide and chlorthalidone over hydrochlorothiazide. Finally, the guidelines provide a treatment algorithm that is similar to the algorithm provided by JNC 7, and includes staging of hypertension (eg, stage 1 and stage 2), as well as the suggestion to start with 2 agents for those patients with stage 2 hypertension (defined as BP ≥160/100 mm Hg). This algorithm is in contrast to the one provided by JNC 8, which does not include staging of patients and offers the initiation of 2 agents as 1 of 3 viable options for medication titration for all patients with hypertension.
Overall, ASH/ISH is a brief, up-to-date hypertension guideline. Although these guidelines are not intended to be the evidence-based update to JNC 7, the recommendations address common hypertension management issues and provide sound guidance. This publication can serve as a resource for clinicians, while the panel from AHA/ACC/ASH develops the more in-depth, evidence-based hypertension guideline.
Management of Hypertension in Patient Subgroups
Hypertension in the Elderly
Since managing elderly patients with hypertension is the focus of much of the current hypertension debate, a review of the American College of Cardiology Foundation (ACCF)/AHA 2011 Expert Consensus Document on Hypertension in the Elderly is essential. 20 First, it must be recognized that this document is not an official guideline but rather an expert consensus statement. The distinction is important because expert consensus documents are created when there is insufficient evidence to develop clinical practice guidelines. Further, awareness of this distinction facilitates interpretation of the ACCF/AHA recommendations, and it also provides insight into the overall lack of congruency that exists among all the guidelines regarding BP management in elderly patients.
It is important to acknowledge that the methods applied to developing the ACCF/AHA consensus document are rigorous and closely aligned with the IOM recommendations for developing formal guidelines. In particular, the writing committee included experts from 10 multidisciplinary organizations across the United States and Europe. Further, members of the writing committee, as well as the external peer reviewers, fully disclosed any actual or potential conflicts of interest to maximize objectivity and transparency. The authors also performed a comprehensive literature review to develop their recommendations. Indeed, this consensus statement was systematically developed and represents the most comprehensive review for managing hypertension in the elderly available in the literature to date.
The ACCF/AHA writing committee provides guidance for managing patients 65 years of age and older. In the opinion of this expert panel, a target systolic BP of ≤140 mm Hg is appropriate for all elderly patients. However, a target of 140 to 145 mm Hg can be an alternative goal in patients 80 years of age or older if needed for improved tolerance. The authors also make some suggestions to mitigate adverse effects in elderly patients, including assessment of orthostatic BPs at each provider visit, more frequent follow-up, and suggest that providers avoid reducing BP below 130/65 mm Hg in this subgroup if possible. There are no specific recommendations in regard to antihypertensive agent selection, although there is considerable discussion about the Hypertension in the Very Elderly Trial, which demonstrated the benefit of indapamide and perindopril in patients 80 years and older. 21 The authors take the position that the evidence generally shows that BP lowering is the priority and that all drugs may be considered provided that the agents have a suitable safety profile.
To summarize, the authors of this consensus document applied a rigorous process to develop their recommendations and provide sound guidance for the management of hypertension in elderly patients. Importantly, although this consensus document was published 2 to 3 years before the debate about managing hypertension in the elderly reached its zenith, the clinical data underlying the recommendations are essentially unchanged, making the ACCF/AHA consensus document relevant in spite of the publication date.
Resistant Hypertension
Patients with resistant hypertension, defined as BP not controlled on at least 3 antihypertensive agents (ideally including a diuretic), represent approximately 9% of all patients with hypertension, according to recent data from the National Health and Nutrition Examination Survey, 2003 to 2008. 22 Yet, resistant hypertension is not comprehensively addressed in any of the guidelines published in 2013. A scientific statement from the AHA Professional Education Committee of the Council for High Blood Pressure Research was published in 2008 to assist clinicians with management of resistant hypertension. 23 Given the dearth of attention to resistant hypertension in the ASH/ISH and JNC 8 guidelines, the comprehensive review and recommendations provided by this panel for patients with resistant hypertension are valuable. Several recommendations provided by this publication are significant and are summarized in Table 2. Briefly, the authors place emphasis on assessing patients for pseudoresistance (eg, white coat hypertension), secondary hypertension, and contributing factors to the development of hypertension (eg, salt intake and weight). Also, the use of chlorthalidone over hydrochlorothiazide is advocated due to improved efficacy and more robust outcome data. The authors also suggest clinicians consider adding a mineralocorticoid receptor antagonist, as hyperaldosteronism is highly prevalent in resistant hypertension. Data supporting spironolactone and amiloride in resistant hypertension are summarized, and evidence substantiating spironolactone’s efficacy has been published since this 2008 review, although adequately powered RCTs evaluating clinical events are still lacking. 24,25 The authors also suggest that taking at least 1 antihypertensive at bedtime may be beneficial, although they caution that the increased frequency of administration could adversely impact adherence. The rationale for this dosing strategy is to target nighttime BP, which may better predict cardiovascular risk than daytime BP. Several small studies published more recently have corroborated the efficacy of this alternative administration method, but, again, large RCTs are still lacking. 26,27 Highlights from this statement are summarized in Table 2.
Other relevant subgroups
Another important deficiency among the recommendations released in the United States in 2013 is that fewer comorbidities and subgroups of patients with hypertension are addressed. In JNC 7, special considerations regarding various demographics (eg, ethnicity, age) and comorbidities (eg, heart failure, myocardial infarction) were summarized, and recommendations were provided for those subgroups that directed medication selection and treatment goals. 6 Conversely, JNC 8 only provides BP goals for black patients and those with CKD and diabetes. Therapeutic recommendations are only given for black patients and those with CKD. (Table 2) The guidelines from ASH/ISH provide an algorithm and table to guide management in some subgroups (eg, ethnicity, diabetes, heart failure), but the recommendations, again, are based on expert opinion. It is recognized by AHA/ACC that comorbidities are not adequately addressed among most cardiovascular guidelines in spite of the prevalence of multiple medical conditions among patients over age 65. 28 For this reason, the AHA/ACC will incorporate evidence-based recommendations about subgroups in future guidelines. 28 Since the AHA/ACC is developing the next comprehensive hypertension management guideline, it is reasonable to anticipate that the hypertension recommendations will address management within subgroups. In the meantime, there are a number of current guidelines that address hypertension management for subgroups (eg, diabetes, CKD) and must be included in the library of key references for clinicians managing hypertension, since no single US guideline provides evidence-based, complete, up-to-date recommendations that can be applied to important patient subgroups. A list of these guidelines, consensus statements, or position papers with their respective recommendations for BP targets is provided in Table 5. 29 –34
Other Relevant Clinical Practice Guidelines.
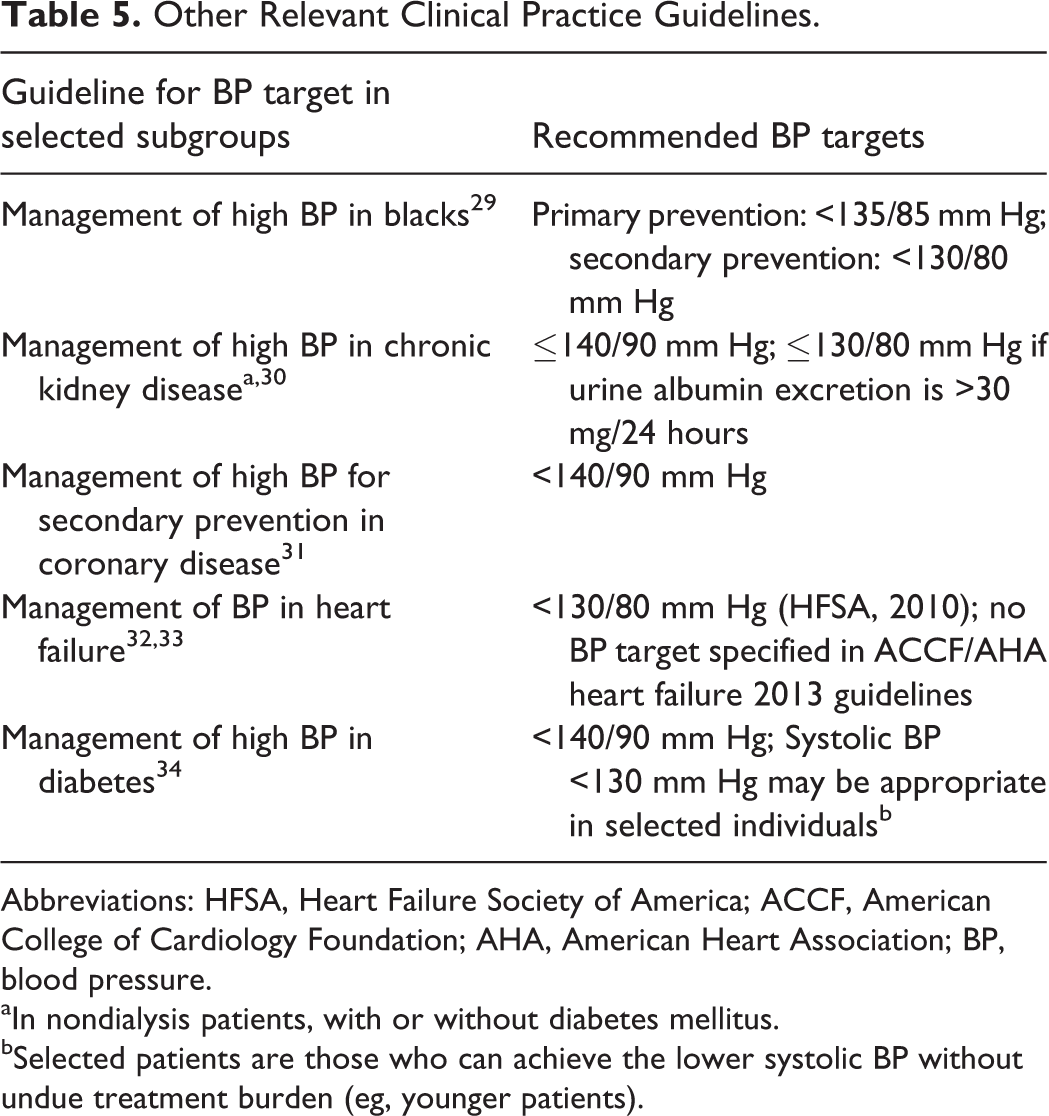
Abbreviations: HFSA, Heart Failure Society of America; ACCF, American College of Cardiology Foundation; AHA, American Heart Association; BP, blood pressure.
aIn nondialysis patients, with or without diabetes mellitus.
bSelected patients are those who can achieve the lower systolic BP without undue treatment burden (eg, younger patients).
Summary/Conclusion
A prolonged season without updated hypertension guidelines culminated in the release of numerous hypertension guidelines, documents, and scientific statements during 2013. The concurrent publication of multiple hypertension recommendations is unprecedented and creates a sense of “guideline overload,” but in actuality, none of these publications are the comprehensive, evidence-based guidelines that update the 2003 JNC 7 hypertension guidelines. Indeed, hypertension management in the United States continues to lack current, all-inclusive, evidence-based clinical practice guidelines.
To further complicate application of the guidelines released between July and December 2013 is that the recommendations lack congruence. There are several underlying reasons for the discordance, but perhaps the most impactful is that the methods for developing the recommendations vary. In particular, the evidence used to support the recommendations differs. The JNC 8 writing committee reviewed only RCTs, while other guidelines or statements included meta-analyses and/or observational data. Other methods differed as well, such as whether the recommendations were based on evidence, as with JNC 8, or based on opinion and consensus, as with ASH/ISH. It is, therefore, not surprising that the recommendations are incongruent.
The hypertension guideline that is intended to provide a comprehensive, evidence-based update to hypertension management is currently in development by the ACC, AHA, and ASH and is expected to be available as early as 2015. 16 In the meantime, since no current reference can be all inclusive for managing hypertension, examination of multiple resources may be necessary. One additional resource that may be helpful for clinicians, recently published by the Journal, is an annotated bibliography of key hypertension references that were released between 2008 and 2014. 35 Such a resource may allow for more expeditious review of primary literature and facilitate a clinician’s application of recommendations and contemporary evidence for hypertension management.
The landscape of hypertension guidelines has changed. The JNC guidelines that the medical community has relied on for 40 years are no longer going to be the authority for hypertension prevention, diagnosis, and management. The transition of guideline development from the NHLBI to ACC, AHA, and ASH has been done with the intent of improving the development process such that there is uniformity, transparency, and ultimately, enhanced reliability. Although this transition has been complicated by the concurrent publication of recommendations from multiple agencies, debate, and criticism, the pursuit of evolution of the guideline development process is commendable and has the potential to improve hypertension management in the United States.
Footnotes
Author’s note
At the time of this research the author was affiliated to Siouxland Community Health Center, University of Nebraska Medical Center, Omaha, NE, USA. Now the author is associated with Pender Medical Center Pender, Nebraska.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.