
Abstract
Strong cytochrome P450 (CYP) 3A4 inhibitors may induce Cushing syndrome and subsequent adrenal insufficiency when administered concurrently with corticosteroids. This drug–drug interaction has been well described with HIV protease inhibitors. A similar drug–drug interaction with corticosteroids and other strong CYP 3A4 inhibitors (antifungals [imidazoles]) has recently been reported but remains less well known. To our knowledge, we report the first case of probable drug-induced Cushing syndrome with subsequent adrenal insufficiency as a result of concomitant oral voriconazole with intranasal mometasone and inhaled fluticasone administration as well as a review of the current literature supporting this drug–drug interaction.
Introduction
Drug-induced Cushing syndrome and subsequent adrenal insufficiency as a result of the drug–drug interaction between concurrently administered corticosteroids (inhaled/intranasal/intra-articular) and HIV protease inhibitors have been well described. 1 –5 A similar drug–drug interaction with inhaled/intranasal corticosteroids and other strong cytochrome P450 (CYP) 3A4 inhibitors (antifungals [imidazoles]) has been reported but remains less well known. 6 –18 Voriconazole (VRC) is a strong CYP 3A4, 2C9, and 2C19 inhibitor, and drug–drug interactions with hepatically metabolized corticosteroids resulting in drug-induced Cushing syndrome would be expected. 19,20 Diagnosis of Cushing syndrome may pose a challenge to providers due to the wide array of nonspecific clinical signs and symptoms. 21 Patients may present with skin changes (acne, ecchymoses, and hirsutism), weight gain, cognitive impairment, or concurrent medical conditions (diabetes, hyperlipidemia, or hypertension), delaying a clinical diagnosis. Suboptimal diagnosis and treatment may result in significant clinical outcomes including cardio-/cerebrovascular disease, infection, and early mortality. Excess exogenous glucocorticoid administration leading to Cushing syndrome may subsequently result in adrenal insufficiency through decreased corticotropin-releasing hormone and corticotropin secretion. Similarly, adrenal insufficiency may present with vague symptoms (weight loss, hypotension, and dehydration) and, if left untreated, may be life threatening. 22 We report a probable case of drug-induced Cushing syndrome with subsequent adrenal insufficiency between concomitantly prescribed VRC, inhaled fluticasone, and nasal mometasone, with a review of the literature supporting this drug–drug interaction. 23
Case Report
A 61-year-old female with a past medical history significant for severe bullous emphysema, chronic obstructive pulmonary disease (40-year tobacco history with recent abstinence 5 months earlier), asthma, chronic sinusitis, gastroesophageal reflux disease, and necrotizing granulomatous Aspergillus pneumonia was hospitalized with methicillin-sensitive Staphylococcus aureus pneumonia. Home medications included oral VRC 200 mg twice daily (4.5 mg/kg for 5 months), oral esomeprazole 40 mg daily, inhaled fluticasone 500 μg/salmeterol 50 μg twice daily, nasal mometasone 50 μg daily, and inhaled tiotropium 18 μg daily. To our knowledge, the patient was adherent to her medication regimen and properly administered her inhaled and nasal steroids in compliance with the product instructions. On hospital admission, the patient was incidentally diagnosed with adrenal insufficiency (morning cortisol concentration <1.0 μg/dL [normal 6.2-22.0 μg /dL]). 22,24 A 9.7-kg weight gain (baseline weight 40.8-kg) with truncal obesity was documented since VRC initiation, but no other clinical findings to suggest Cushing syndrome were noted. As the morning cortisol concentration was undetectable, a cortisol stimulation test was deemed unnecessary to confirm a diagnosis of adrenal insufficiency. 22,24 The patient had no known adrenal abnormalities (tuberculosis, HIV, carcinoma, or primary adrenal insufficiency), was not critically ill at the time of presentation, and had no history of being on other medications known to cause adrenal insufficiency. As such, no alternative adrenal insufficiency etiologies were evaluated, and a probable drug interaction between VRC and inhaled/intranasal corticosteroids was suspected. 22,23 Due to her diagnosis of severe chronic obstructive pulmonary disease (COPD) and chronic sinusitis, the medical team decided the benefits of intranasal mometasone, and inhaled fluticasone outweighed the risk of discontinuing therapy. Physiologic cortisol repletion with oral hydrocortisone 20 mg every morning and 10 mg every evening was initiated. Of unknown clinical significance, a supratherapeutic VRC trough concentration of 8.1 μg/mL (therapeutic range 1-4 μg/mL) prompted a dose reduction to 100 mg (2.2 mg/kg) twice daily. 19,25 –27 At 3 weeks posthospitalization, the patient’s health status was improved with continued hydrocortisone repletion and no additional medication changes. At 6 weeks posthospitalization, the dose of hydrocortisone was decreased to 10 mg daily. VRC was discontinued 12 weeks after hospital discharge by the patient’s pulmonologist after computed tomography of the chest showed significant improvement. At 37 weeks postdischarge, the patient presented with an 11-kg weight gain and concerns for fat accumulation on the neck and upper chest. Hydrocortisone therapy was discontinued, and the patient was transitioned to an oral prednisone taper. At present, the patient is not on any oral corticosteroid therapy. To our knowledge, no repeat cortisol concentration was ever obtained.
Discussion
Within the normal dosage range, nasal and inhaled corticosteroids do not usually have systemic effects on the hypothalamic–pituitary–adrenal (HPA) axis. 2,28 –30 Cushing syndrome with subsequent adrenal insufficiency resulting from the negative feedback effects on the HPA axis is well known when HIV protease inhibitors (strong CYP 3A4 inhibitors) are used concurrently with corticosteroids due to increased systemic corticosteroid concentrations. 1 –5 Specifically, when nasal fluticasone (200 μg once daily) was administered with oral ritonavir (100 mg twice daily) to 18 healthy volunteers, the fluticasone maximum concentration (Cmax) and area under the concentration time curve (AUC) increased by 25- and 350-fold, respectively. 2,31 An 86% decline in serum cortisol AUC was additionally documented. 2
Recent reports demonstrate comparable results when inhaled/intranasal corticosteroids are administered with the similar strong CYP 3A4 inhibitors, such as itraconazole (ITC), posaconazole (PSC), fluconazole (FLC), and VRC (Table 1). 6 –18 Fourteen reports (including the current case) support the significance of this drug–drug interaction which may occur in pediatric or adult patients with significant comorbidities (HIV, lung transplant, cystic fibrosis, and chronic granulomatous disease). Further studies have indicated that Cushing syndrome with subsequent adrenal suppression is not related to treatment duration and may occur within the first 5 days and up to 2 years after therapy initiation with inhaled corticosteroids and a strong CYP 3A4 inhibitor. 6 –18 Similar to the drug–drug interaction with protease inhibitors and corticosteroids, adrenocorticotropic hormone (ACTH) stimulation tests are negatively affected when imidazoles and inhaled corticosteroids are concurrently administered. 6,8,10,13 In a recent report, patients with cystic fibrosis receiving inhaled fluticasone (500-1000 μg daily dose) with oral ITC (200 mg twice daily [N = 12]) or without a concurrent antifungal (N = 12) were evaluated. 8 A standard cortisol stimulation test was performed after 3 days of holding inhaled fluticasone. An abnormal ACTH stimulation test resulted in all patients receiving concurrent fluticasone and ITC compared to only 2 patients in the fluticasone-only group. Eighty-three percent of the patients receiving inhaled fluticasone with concomitant ITC had HPA axis suppression ranging from mild to severe in clinical significance. One of the patients with HPA axis suppression also presented with Cushing syndrome. Each of the cases was attributed to a probable drug–drug interaction between ITC and fluticasone, resulting in a significant increase in systemic fluticasone concentrations. Similar data exist with the concurrent administration of inhaled budesonide and oral ITC in healthy volunteers (N = 10). 15 Significant increases in the budesonide AUC, Cmax, and half-life were reported, with 43% of subjects having decreased cortisol concentrations.
Summary of Literature Regarding Inhaled/Intranasal Corticosteroids and Imidazole Antifungals.
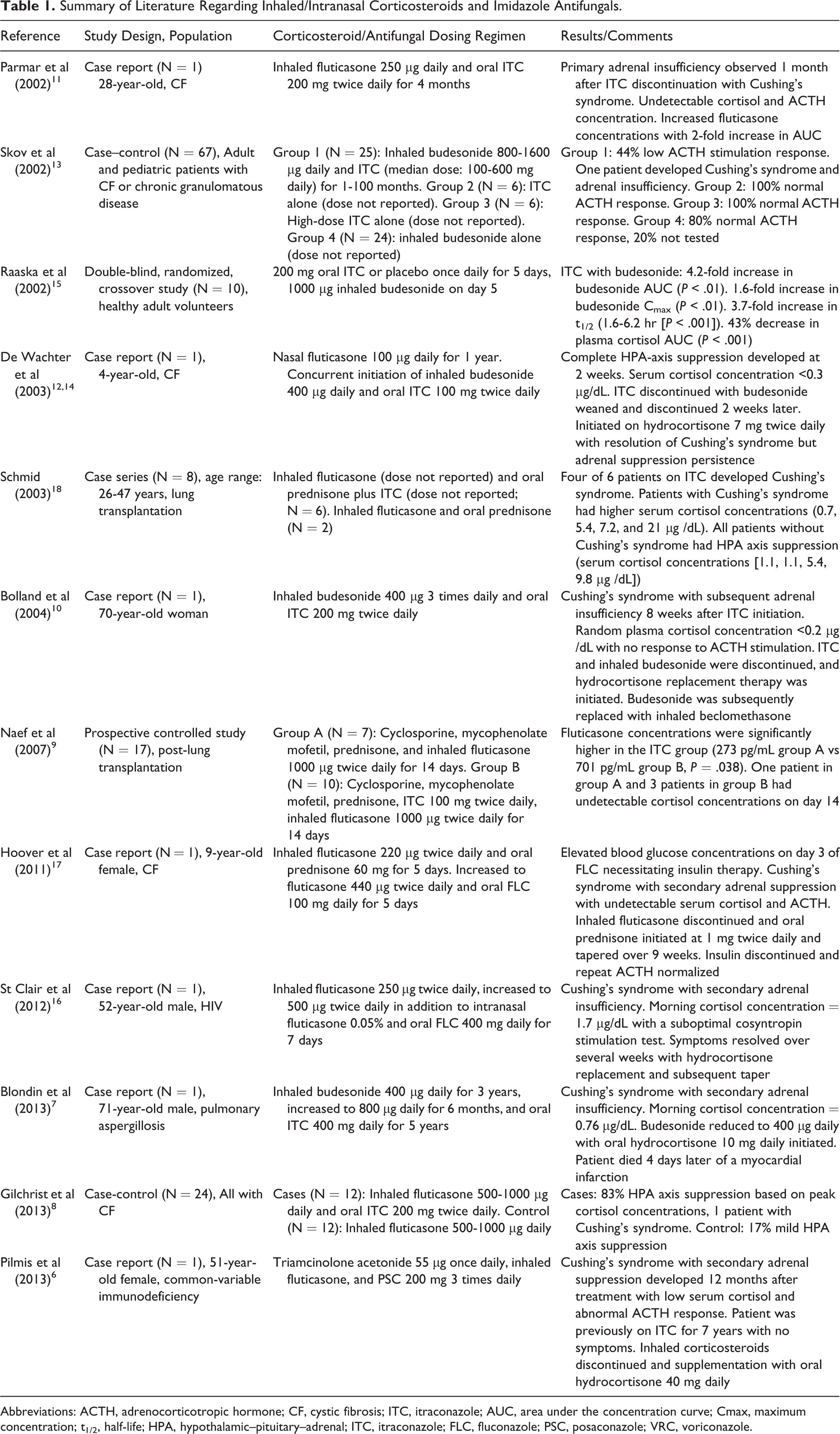
Abbreviations: ACTH, adrenocorticotropic hormone; CF, cystic fibrosis; ITC, itraconazole; AUC, area under the concentration curve; Cmax, maximum concentration; t1/2, half-life; HPA, hypothalamic–pituitary–adrenal; ITC, itraconazole; FLC, fluconazole; PSC, posaconazole; VRC, voriconazole.
Azole antifungals also directly inhibit cortisol synthesis, and this may be a contributing mechanism for decreasing systemic cortisol concentrations with resultant adrenal insufficiency. 10,12,20 Ketoconazole (KTC) has most commonly been associated with adrenal suppression, with more recent reports demonstrating similar effects with both FLC and ITC. 10,13,32,33 In order to determine whether the inhibitory effects of imidazoles on adrenal glucocorticoid synthesis is contributing to the interaction with inhaled/nasal corticosteroids, ACTH stimulation response was evaluated in patients with cystic fibrosis or chronic granulomatous disease receiving ITC alone (N = 12) or concurrently (N = 25) with inhaled budesonide (800-1600 μg daily). 13 Forty-four percent of the patients concurrently treated with budesonide and ITC had a documented low ACTH stimulation response. No patients receiving ITC alone had an abnormal ACTH response. These results provide further support for the possible causal association between imidazole antifungal CYP 3A4 inhibition of inhaled corticosteroid metabolism leading to Cushing syndrome with or without secondary adrenal suppression, irrespective of imidazole inhibition of cortisol production.
As with our patient, and similar to previously published reports, cortisol recovery may occur after VRC (or strong CYP 3A4) discontinuation. 4,10 –13,16,20,29 Patients on concomitant VRC and inhaled/nasal corticosteroids should be monitored at regular follow-up for Cushing syndrome and subsequent adrenal insufficiency with particular attention to fluctuations in weight (truncal obesity or moon facies) or blood pressure, reported myopathies, and electrolyte abnormalities. 21,22 The potential risks of this combination therapy should be carefully considered. 18,34 To our knowledge, there is no relationship between VRC plasma concentrations and degree of CYP 3A4 inhibition. 19 As such, while monitoring VRC concentrations may be of clinical value for assessing safety and efficacy, decreased metabolism of corticosteroids through the CYP 3A4 pathway may occur within any range of plasma concentrations. 19 Choosing an alternative corticosteroid with decreased CYP3A4 metabolism (beclomethasone or flunisolide) has been suggested as a reasonable alternative in patients who require treatment with an inhaled/nasal corticosteroid and strong CYP 3A4 inhibitors. 4,10,29 For patients whom corticosteroids are prescribed for asthma or allergic rhinitis, substituting a leukotriene inhibitor would be an additional alternative to avoid this drug–drug interaction. 4,10,29 No case reports currently exist between imidazoles and intra-articular corticosteroids. However, based on the reports with protease inhibitors and parenteral triamcinolone, a similar interaction would be expected and thus avoiding concurrent administration should be considered. 5 One additional concern is that intranasal corticosteroids have recently been given over-the-counter status. 2,35 Thus, patients may be at risk for this interaction without any prior screening of their pharmacotherapy profile by a direct provider.
Conclusion
The clinical evidence supports a probable drug–drug interaction between the imidazole antifungals and corticosteroids. While many providers may carefully weigh the risk versus benefit when prescribing imidazole antifungals with concurrent oral corticosteroids, consideration should also be given if inhaled/nasal/intra-articular corticosteroids are deemed necessary with meticulous monitoring for Cushing syndrome and/or adrenal insufficiency.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.