
Abstract
Background:
In-hospital venous thromboembolism (VTE) causes significant morbidity and mortality in hospitalized patients. The objective of our study is to determine the time to in-hospital VTE based on baseline risk stratification.
Methods:
All adult patients admitted to a 900-bed academic tertiary referral hospital who developed a VTE during hospital admission from September 1, 2011, to June 30, 2015, were retrospectively analyzed. Patients were excluded if they were younger than 18 years or if the VTE was present on admission.
Results:
The cohort included 400 patients, 224 (56%) males, median age 66 years. The median time to VTE was 8 days. Significant differences in time to VTE existed between the risk groups.
Conclusion:
Time to VTE in a broad hospitalized patient population differs based on admission risk group. This finding highlights the importance of performing risk assessment upon admission and subsequently with clinical changes to assess increases in risk scores.
Keywords
Background
In-hospital venous thromboembolism (VTE), comprised of deep vein thrombosis (DVT) and pulmonary embolism (PE), causes significant morbidity and mortality in hospitalized medical and surgical patients. 1 –3 Approximately 900,000 patients in the United States are affected by DVT and PE each year, with 50% of these events being hospital-acquired. 4,5 With appropriate prophylactic measures, as many as 70% of these hospital-acquired VTE events are preventable; however, fewer than half of hospitalized patients receive appropriate prophylactic measures. 6,7
Risk factors have been identified, which predispose patients to developing VTE while hospitalized. 8 These include, but are not limited to, hip or leg fracture, major general surgery, central venous lines, malignancy, and previous VTE. 9 Keeping these risk factors in mind, risk assessment models (RAMs) have been developed to identify patients at risk of VTE while hospitalized. 9 –11 It is recommended that providers assess patients using these RAMs upon admission and subsequently every 24 to 48 hours or with meaningful clinical changes to ensure appropriate prophylactic measures are being utilized. 12
Once a patient’s VTE risk has been established, appropriate prophylactic measures should be initiated. The American College of Chest Physicians (ACCP) provides guideline recommendations for the prevention of VTE in medical, orthopedic surgery, and nonorthopedic surgery patients. 13 –15 Options for VTE prevention include pharmacologic and mechanical methods, depending on the patient’s risk assessment. Mechanical methods, such as compression stockings or sequential compression devices (SCDs), increase venous blood flow and are generally utilized for patients with contraindications to pharmacologic prophylaxis or at low risk for VTE (0-1 risk factors). 16 Pharmacologic prophylaxis should be utilized for patients at moderate-high risk for VTE (2 or more risk factors) without risk factors for bleeding. 16 Clinical trials evaluated enoxaparin, dalteparin, and fondaparinux, respectively, for prevention of VTE in hospitalized patients and found that low doses of these agents reduced the VTE rate by half without increases in major bleeding complications. 17 –19 The risk of clotting must be balanced with the risk of bleeding, and scoring systems such as the International Medical Prevention Registry on Venous Thromboembolism (IMPROVE) assist clinicians in appropriately assessing these risks. 20 Providing appropriate prophylactic measures based on RAMs has led to significant reductions in hospital-acquired VTE rates. 21 –23 However, despite receiving prophylaxis while hospitalized, VTE events still occur. 24 To encourage widespread implementation of VTE prophylaxis measures, the Agency for Healthcare Research and Quality has published guidance for institutions to select between various risk assessment tools. 2
An important variable that has not been thoroughly explored in the literature is the time to VTE occurrence while patients are hospitalized. Examining this end point and determining when VTE events occur during hospitalization may lead to more targeted interventions to prevent these events from occurring. If health-care providers are able to identify at which point during hospitalization a patient is most likely to develop a VTE event, more effective and safer preventative measures can be implemented before the event occurs. This could potentially decrease hospital length of stay, total cost of hospital care, and increase patient satisfaction. One study has been published recently, examining the time to VTE occurrence in a specific spinal surgery population. 25 The objective of our study is to determine the time to in-hospital VTE development based on baseline risk stratification in a broad patient population.
Methods
A retrospective analysis was performed on all patients aged 18 years or older who were admitted to a 900-bed academic tertiary referral hospital and developed a VTE during their hospitalization from September 1, 2011, to June 30, 2015. Patients were identified via the University HealthSystem Consortium database using diagnosis codes for upper extremity DVT, lower extremity DVT, and PE not present on admission. Patients with a prior history of VTE were included in this study. This study was given a letter of exemption from the institutional review board after being deemed nonhuman subject research.
VTE events were defined as an acute DVT in the upper or lower extremities, diagnosed by venous Doppler ultrasound, or an acute PE diagnosed by computed tomography scan or a ventilation/perfusion scan. An institution-specific RAM was developed in 2011, modified from the Fifth ACCP Consensus Conference on Antithrombotic therapy, and was integrated into daily practice. 26 Due to the retrospective nature of the study and the fact that this RAM was not required to be utilized on all patients admitted to our institution, the RAM was documented as being used on some patients, but not all, based on provider discretion. Risk assessment was performed retrospectively by study investigators using the institution-specific RAM at the time of admission and at the time of VTE development (Figure 1). The RAM was intended to be used in a broad patient population; therefore, differing types of patients (ie, medical, surgical, oncologic) did not dictate the use of a separate RAM. The provider-documented history and physical was used to collect risk factors present on admission, and the provider-documented discharge summary was used for risk factors at the time of VTE development. Immobility was defined as medical patients who were hospitalized for >72 hours without any remarks in the discharge summary regarding the patient’s ambulatory status. Patients were divided into low (0-1 points), moderate (2 points), high (3-4 points), or highest (5 or more points) risk groups based on the number of risk factors present on admission and at the time of VTE development.
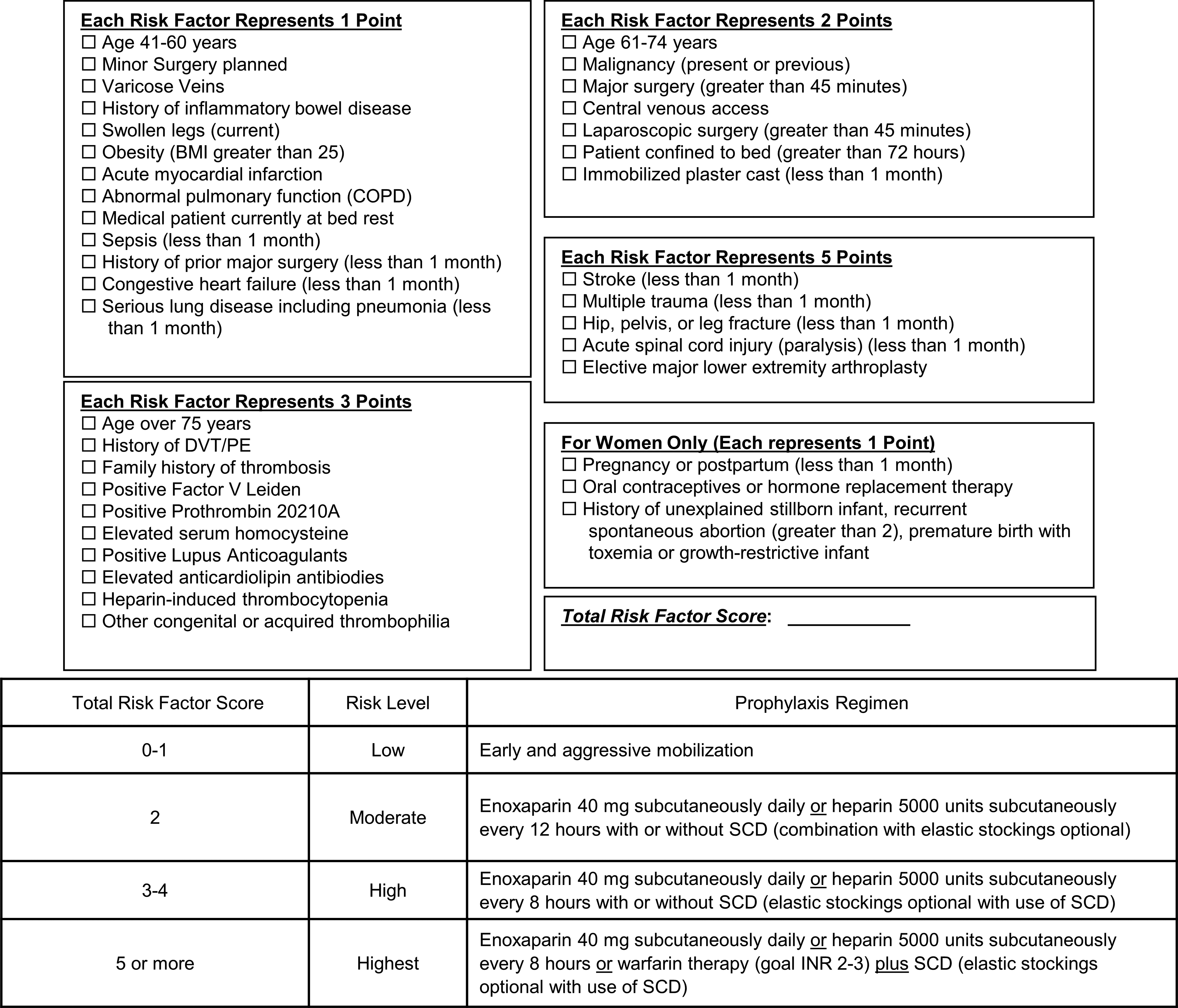
Institution-specific risk assessment model. BMI indicates body mass index (kg/m2); COPD, chronic obstructive pulmonary disease; DVT, deep vein thrombosis; PE, pulmonary embolism; SCD, sequential compression device.
VTE preventative measures were collected for all patients. For patients to qualify as having mechanical prophylaxis, they must have had an order for 1 of the following during their hospitalization prior to the VTE event: SCDs, compression stockings, or SCDs + compression stockings. For patients to qualify as having pharmacologic prophylaxis, they must have received 1 dose within 48 hours of admission of a prespecified agent, which must have continued for at least 80% of the time from admission to VTE development. 11 Nonsurgical patients could have received enoxaparin, heparin, or fondaparinux, while hip or knee replacement patients could have received these agents or apixaban 2.5 mg orally every 12 hours, aspirin 162 mg orally daily, rivaroxaban 10 mg orally daily, or warfarin. 13 –15
Patients with contraindications to pharmacologic prophylaxis were eligible to receive only mechanical prophylaxis. These contraindications included active hemorrhage, history of intracerebral hemorrhage, hemorrhage within the previous 6 months, pericardial effusion, heparin-induced thrombocytopenia, thrombocytopenia (platelets < 150,000), severe trauma to the head or spinal cord, extremity hemorrhage within 4 weeks, allergy to heparin products, epidural or indwelling spinal catheter, spinal tap, active intracranial lesions or neoplasms, proliferative retinopathy, or vascular access/biopsy sites inaccessible to hemostatic control. 13 –15
Appropriate prophylaxis was determined by 1 study investigator using the institution-specific RAM. Patients were classified as having appropriate prophylaxis if they were given the corresponding prophylaxis strategy based on their risk category according to our institution-specific RAM. If patients were, for example, moderate risk and given heparin 5000 units every 8 hours subcutaneously instead of every 12 hours, that was considered appropriate because it was more aggressive than what was recommended. Appropriate dosing per patients’ renal function was determined using estimated creatinine clearance, calculated with the Cockcroft-Gault equation and ideal body weight. For patients with end-stage renal disease on hemodialysis, appropriate dosing of pharmacologic agents included enoxaparin 30 mg subcutaneously once daily or heparin 5000 units subcutaneously every 12 hours. If patients had documented contraindications to pharmacologic prophylaxis, they were scored as having received appropriate prophylaxis if mechanical prophylaxis alone was utilized. Patients on treatment doses of anticoagulants were classified as having appropriate pharmacologic prophylaxis if the agents were started within 48 hours of hospital admission and present 80% of the time to VTE development. Patients who were receiving treatment doses of anticoagulants that did not meet our prespecified criteria for pharmacologic prophylaxis were coded as not receiving pharmacologic prophylaxis. Treatment doses were defined as receiving warfarin and having an international normalized ratio (INR) ≥2, heparin continuous infusion with anti-Xa 0.3 to 0.7, fondaparinux >2.5 mg/d, enoxaparin >40 mg/d, rivaroxaban >10 mg/d, dabigatran >220 mg/d, or apixaban >5 mg/d.
The primary end point of this study was the time to in-hospital VTE event based on baseline risk stratification. Secondary end points included the difference between VTE risk at the time of admission and at the time of VTE development, types of pharmacologic and mechanical prophylaxis utilized, patient populations (intensive care unit [ICU] vs non-ICU), whether or not appropriate prophylaxis was utilized, and the type of VTE event (DVT or PE).
Statistical Analysis
Normality was determined using the Ryan-Joiner normality test. Baseline characteristics were summarized using descriptive statistics, including median and interquartile range for continuous variables and frequency and percentage for categorical variables. Baseline statistics were compared between the risk groups using Kruskal-Wallis test and Mann-Whitney U test. The primary end point, time to in-hospital VTE based on risk stratification, was analyzed using a Kaplan-Meier curve with log-rank test to compare between the groups. Secondary end points were summarized using descriptive statistics and Kruskal-Wallis Test. Between high- and low-risk patients, if there was a difference in 2 days in time to VTE event using a β error of 20% and confidence level of 95%, an estimated sample size of 375 patients is necessary to determine outcomes. An α value of less than .05 was considered statistically significant. Microsoft Excel 2013 (Redmond, Washington) was used for collection of additional variables and database management. All data analyses were performed using Minitab® 16 (State College, Pennsylvania).
Results
The cohort included 400 patients, 224 (56%) males, with a median age of 66 years (Q1-Q3, 55-75) at the time of hospital admission (Table 1). Differences between the risk groups were seen at baseline for age, length of stay, type of VTE event, and estimated creatinine clearance. Types of patients included medical (n = 289, 72%) and surgical (n = 111, 28%) which represented abdominal, cardiac, orthopedic, and neurosurgical patients, among others. VTE events occurred in 22 patients (5.5%) at an INR greater than 2, which included patients with liver disease (n = 6), cancer (n = 7), active bleeding (n = 3), and other disease states (n = 6). Of these 22 patients, 5 were receiving warfarin therapy. Of the 75 patients who developed an upper extremity DVT, 32 (43%) had a central line at the time of VTE development. Upon admission, the median risk score was 5 (Q1-Q3, 3-7), with the majority of patients being classified as highest risk (n = 220, 73%). At the time of VTE event, the median risk score had increased to 8 (Q1-Q3, 7-10; P < .001 for the comparison between the admission risk score and time of VTE risk score). Several risk factors were acquired during hospitalization, accounting for the increase in risk score (Figure 2).
Baseline Characteristics.a
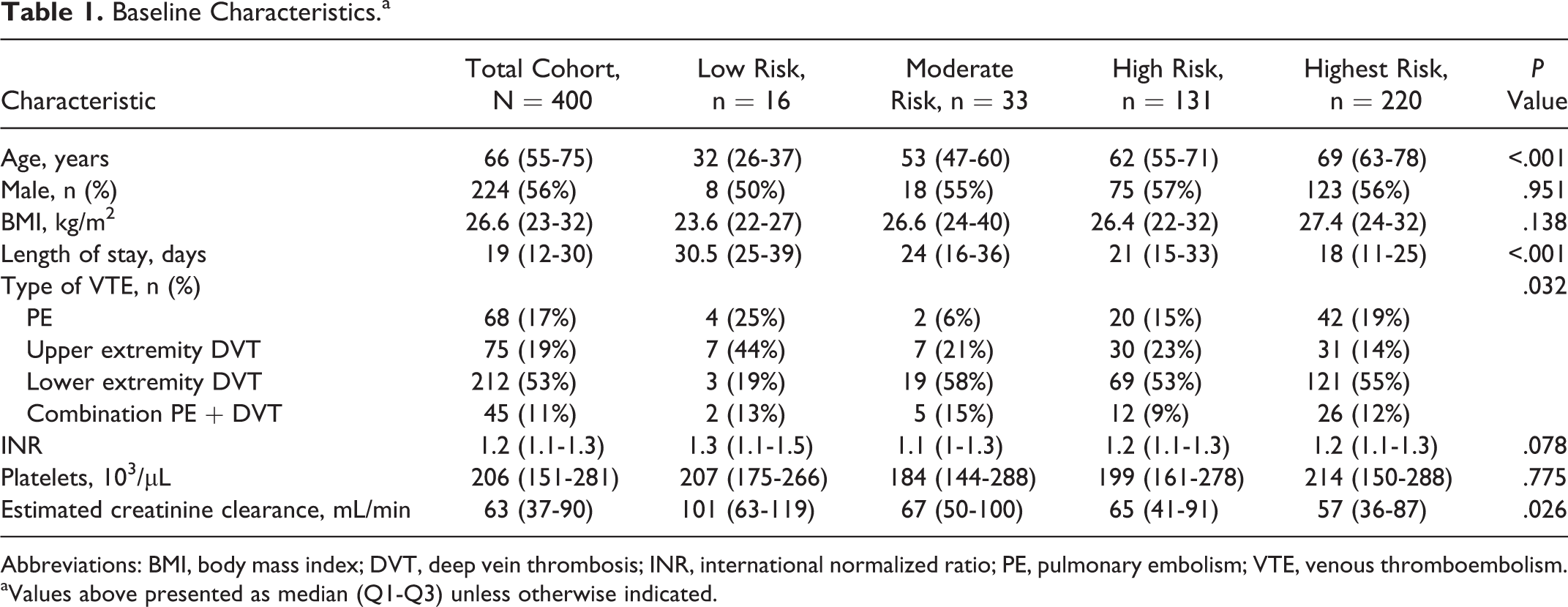
Abbreviations: BMI, body mass index; DVT, deep vein thrombosis; INR, international normalized ratio; PE, pulmonary embolism; VTE, venous thromboembolism.
aValues above presented as median (Q1-Q3) unless otherwise indicated.
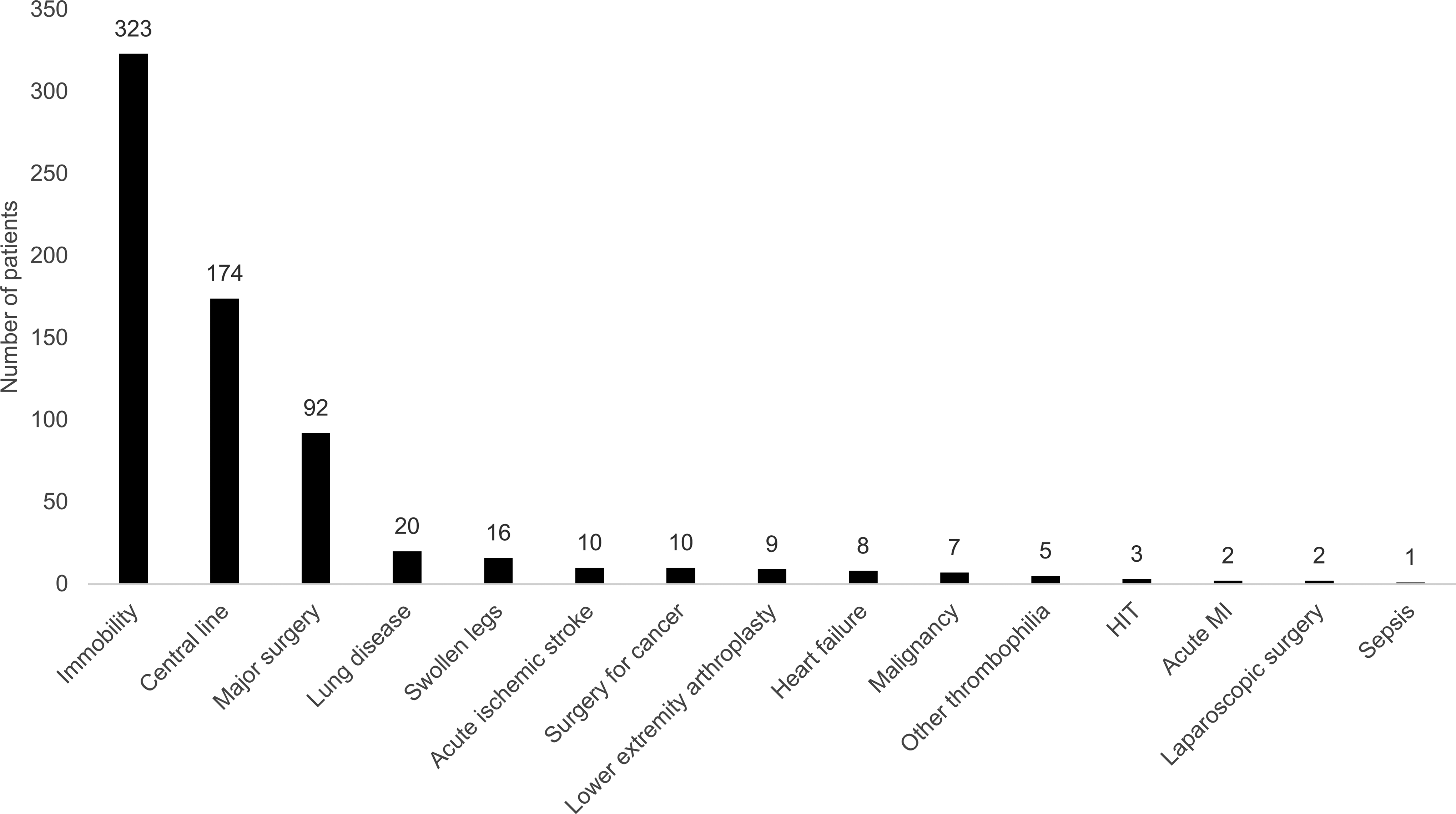
Risk factors acquired during hospitalization. HIT, indicates heparin-induced thrombocytopenia; MI, myocardial infarction.
VTE prophylaxis strategies included no prophylaxis (n = 73, 18%), mechanical prophylaxis alone (n = 235, 59%), pharmacologic prophylaxis alone (n = 50, 13%), and combined mechanical and pharmacologic prophylaxis (n = 42, 11%). Contraindications for pharmacologic prophylaxis were documented for 88 patients and included active hemorrhage (n = 52, 59%), history of intracerebral hemorrhage (n = 5, 5.7%), hemorrhage within previous 6 months (n = 4, 4.5%), spinal tap (n = 3, 3.4%), thrombocytopenia (n = 21, 24%), epidural or indwelling spinal catheter (n = 2, 2.2%), and pericardial effusion (n = 1, 1.1%). For patients who received pharmacologic prophylaxis, the most common medication used was enoxaparin (n = 58, 63%), followed by heparin (n = 27, 29%), warfarin (n = 4, 4%), aspirin (n = 2, 2%), and rivaroxaban (n = 1, 1%).
Mechanical prophylaxis strategies included SCDs (n = 242, 61%) and SCDs + compression stockings (n = 35, 9%). Inappropriate prophylaxis was documented in 140 patients (35%). Reasons for inappropriate prophylaxis included delayed pharmacologic initiation (n = 136, 52%), incomplete pharmacologic duration (n = 204, 78%), incorrect pharmacologic dose (n = 48, 18%), and no mechanical prophylaxis (n = 102, 39%). Some patients had more than 1 reason for inappropriate prophylaxis.
The median time to VTE event for the overall cohort was 8 days (Q1-Q3, 4-13). When subdivided between medical and surgical patients, there was no difference in the time to VTE (8 days vs 8 days; P = .8005). Analysis of the primary end point, time to VTE based on admission risk assessment, revealed a statistically significant difference between the risk groups (Figure 3).
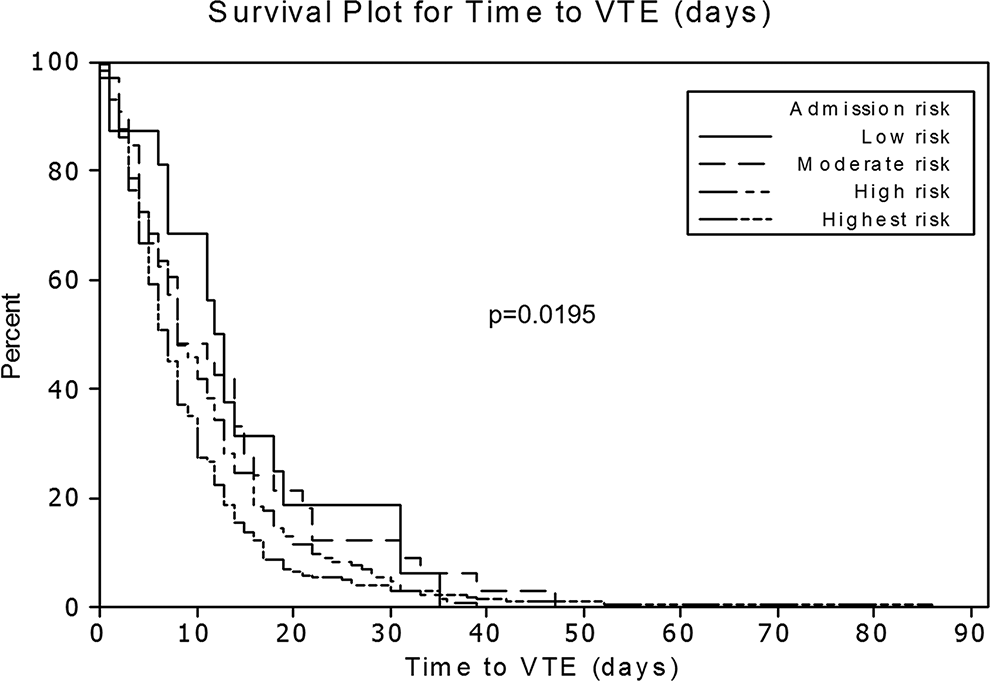
Time to VTE based on admission risk assessment. VTE indicates venous thromboembolism.
No difference was found when time to VTE was stratified based on the type of VTE prophylaxis given or if patients received appropriate prophylaxis prior to the VTE event. Patients located in a non-ICU setting at the time of VTE developed a VTE significantly faster than patients located in an ICU setting at the time of VTE (7 days vs 9.5 days; P = .001). In addition to patient location, PE occurred significantly faster than lower extremity DVT and upper extremity DVT (6 days vs 8 days vs 8.5 days; P = .001).
Discussion
To our knowledge, this study represents a novel contribution to the literature, exploring the time to in-hospital VTE event based on admission risk stratification in a broad patient population. Only 1 study has previously analyzed the time to in-hospital VTE event as the primary end point, though it was performed in a very specific patient population, spinal surgery. 25 This study by McClendon et al found that the median time to VTE event was 9.5 days, compared to our study which found that patients develop VTE events approximately 8 days into their hospitalization. Our time to VTE is slightly shorter than what was reported in the previous study which may be due to a number of factors, namely, a difference in patient population. In the McClendon study, all patients underwent spinal surgery and were given some form of VTE prophylaxis. In our study, we had a variety of medical and surgical patients, and not all patients received VTE prophylaxis.
The risk groups in which patients presented at baseline increased significantly by the time the VTE event occurred. Patients gained a number of risk factors during hospitalization, such as major surgery, placement of central venous access, and immobility. Additionally, the time to VTE differed significantly based on risk group stratification on admission. The fewer the risk factors patients had upon presentation, the more risk factors they gained while hospitalized and the longer it took for a VTE event to take place. This finding highlights the importance of performing risk assessment upon hospital admission and subsequently with clinical changes to assess increases in risk scores as risk factors are acquired.
Patient location and type of VTE event both showed significant differences in terms of time to VTE event. We found that patients located in an ICU setting took longer for a VTE event to occur compared to patients located in an acute care setting. One possible explanation for this finding is that the patients in the acute care setting were more likely to be in the high-risk group and highest risk group, which had a shorter time to VTE event in the overall cohort. Regarding the type of VTE event, patients who developed PE had a shorter time to VTE event compared to those who developed either type of DVT, upper or lower. The previous study performed in a spinal surgery population did not comment on the difference in time to PE versus DVT, but another study by Pateder et al found that the time to PE was 4.4 days after surgery, occurring early in the hospitalization. 27
This study has possible implications for clinical practice. Prescribers should perform risk assessment at baseline and repeat during the hospital stay to ensure adequate prophylaxis. While appropriate prophylaxis did not prevent some patients in our study from developing VTEs, our study did not include a control group who did not develop VTE while hospitalized, so we cannot adequately draw conclusions about the ability of appropriate prophylaxis to prevent VTE events. Additionally, patients who had contraindications to receiving pharmacologic prophylaxis were included as having received appropriate prophylaxis, because they were at high risk of bleeding and could not receive anticoagulants. These patients could be impacting the time to VTE findings between patients who received appropriate and inappropriate prophylaxis. By repeating risk assessment regularly throughout a patient’s hospitalization, perhaps some VTE events that occurred in our study could have been avoided. Some patients in our study still developed VTE despite being on appropriate prophylaxis, and this group should be explored further in future studies to determine which factors are unique and how to better tailor prophylaxis to this group. Additionally, it was certainly possible for patients to both gain and lose risk factors during the course of their hospitalization, but the net change that was found in this study throughout the entire patient population was an increase in risk score. More frequent risk assessments would be beneficial to identify patients who are in need of more aggressive prophylaxis and are at risk of developing a VTE and also patients who are receiving aggressive prophylaxis who are no longer eligible and are at an increased risk of bleeding. Because this risk/benefit must always be balanced on a patient-to-patient basis, repeating risk assessments during hospitalization would provide each patient with tailored prophylaxis strategies to meet their needs.
Strengths of this study include the large sample size, broad patient population, and generalizability to patient populations at other institutions. Limitations include the reliance on information documented in the medical chart collected retrospectively which may or may not be accurate, and inability to ensure that patients with orders for mechanical prophylaxis were wearing the devices during their hospitalization and could have possibly refused to wear them. Additional baseline patient information including comorbidities and ethnicity was not included in this study; therefore, conclusions cannot be drawn regarding the effects of these variables on our primary outcome. There may also be recall bias present in using discharge summaries to collect risk factors at the time of VTE development, if a substantial amount of time had passed between the VTE event and the patient’s discharge. Patients were identified using diagnosis codes for DVT and PE not present on admission, but patients were not universally scanned upon admission to ensure that the event had not occurred prior to hospitalization. Additionally, our RAM was modified from the Caprini model, which has only been validated in surgical patients and may not be representative of a broad patient population such as ours. Our RAM was also quite complex with numerous risk factors representing different point values. The RAM in itself was a limitation as the clinical utility was hindered by the sheer number of risk factors available to choose from to calculate an accurate risk score. Despite these limitations, this study demonstrates the importance of an initial and subsequent risk assessment and its impact on the time to VTE in a broad patient population.
There are several future directions and recommendations that come from our findings in this present study. One is to further explore our obese cohort of patients and the prophylaxis strategies utilized. There have not been concrete guidelines recommending specific doses of pharmacologic agents to prevent VTE events from occurring in our hospitalized obese patients, but only guidance from the primary literature. Additionally, although we saw that risk assessment was performed at baseline upon hospital admission and patients gained a significant number of risk factors during their stay, there are no recommendations for how frequently risk assessment should be repeated. The American Society of Health-System Pharmacists recommends repeating risk assessment every 24 to 48 hours or with clinical changes, but these recommendations have not been solidified by findings from primary literature. 12 By conducting further data analysis to find the optimal time point to repeat risk assessment during hospital admission, we can appropriately target patients who have gained enough risk factors to warrant changes in prophylaxis strategies. Due to the complexity of our RAM reported in this study, our institution recently implemented a new RAM which allows providers to allocate patients into 1 of 3 risk groups (low, medium, or high) upon admission. Future studies from our group may examine the time to VTE once the new RAM is in place to see if any improvements have been made from a quality-assurance perspective. Additionally, bleeding outcomes were not measured in our study, although this is an important consideration that must be balanced with the risk of VTE development. Future studies may incorporate the risk of bleeding to determine which appropriate prophylaxis measures should be implemented for specific patient populations.
Conclusion
This study shows that the time to VTE in a broad hospitalized patient population differs significantly based on the admission risk group. This may be due to patients gaining risk factors for VTE while hospitalized, many of which are interventions that patients receive during their hospital stay. This finding highlights the importance of performing risk assessment upon hospital admission and subsequently with clinical changes to assess increases in risk scores as risk factors are acquired.
Footnotes
Authors’ Note
Research materials related to this manuscript can be obtained by contacting the corresponding author directly.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.