
Abstract
Background:
Pneumococcal vaccination rates among high-risk patients (eg, diabetes, asthma, smoking) seen in 2 family medicine clinics are unknown.
Objectives:
To assess differences in pneumococcal polysaccharide vaccination rates and reasons for nonvaccination among patients with diabetes and asthma and patients who smoke.
Methods:
A chart review at 2 family medicine residency training clinics showed 425 patients with a medical indication for PPSV23 were seen between April 1, 2015, and April 30, 2015. One reviewer searched the electronic health records to assess reasons for nonvaccination.
Results:
Rates of nonvaccination were 29.8% in patients with diabetes, 58.7% in patients with asthma, and 62.5% in patients who smoke cigarettes. Patients were classified into 3 groups based on the reasons for nonvaccination: documented patient refusal, not being addressed by a provider, and being documented as low risk despite the presence of a medical indication.
Conclusion:
The 3 reasons for nonvaccination were vaccination not being addressed, misclassification of high-risk patients as low-risk patients for infection, and documented patient refusal. Providers overlooked vaccination more often in patients with asthma and cigarette use than in patients with diabetes. Patients seeing pharmacists were most likely to be vaccinated, whereas patients seeing physician assistants were least likely to be vaccinated. Pharmacists see patients to provide medication management and preventive care, whereas other providers treat more urgent conditions. Because indications are often overlooked and not addressed, pharmacists can play a larger role in identifying and vaccinating high-risk patients.
Background
Pneumococcal disease is caused by the bacteria Streptococcus pneumoniae, or pneumococcus, and infection results in a variety of illnesses including ear and sinus infections, meningitis, and pneumonia. 1,2 There are approximately 4 million illnesses, 445 000 hospitalizations, and 22 000 deaths in the United States each year as a result of pneumococcal disease. 3 Certain groups of people are at particular risk of pneumococcal illness including children younger than 2 years old; children in group care; adults 65 years and older; adults with chronic illnesses, cochlear implants, or cerebrospinal fluid (CSF) leak; adults with weakened immune systems; and adults living in nursing homes or in long-term care facilities. 2,4,5 The pneumococcal polysaccharide vaccine (PPSV23) helps protect against 23 strains of S pneumoniae and is indicated in adults aged 65 years and older, children 2 years and older at high risk, and in those aged 19 to 64 years who smoke or have asthma. 1,6 -10 High-risk medical indications include chronic heart, liver, or lung disease; diabetes mellitus; CSF leaks; cochlear implants; alcoholism; chronic obstructive pulmonary disease; sickle cell or other hemoglobinopathies; congenital or acquired asplenia; congenital or acquired immunodeficiencies; chronic renal failure; leukemia; lymphoma; generalized malignancy; multiple myeloma; and solid organ transplant. 6,10,11 Health-care providers have the opportunity to prevent pneumococcal disease by identifying high-risk patients and providing vaccination.
Objectives
Rates of PPSV23 vaccination are higher for those patients aged 65 years and older than in those aged 19 to 64 years who are at high risk of pneumococcal disease at 2 family medicine residency training clinics. The primary outcome of this study was to determine the differences in vaccination rates of the PPSV23 vaccine among patients with medical indications of diabetes mellitus, asthma, and cigarette smoking in clinics where family medicine faculty, residents, physician assistants, and ambulatory care pharmacists practice. Secondary outcomes assessed differences in vaccination rates based on provider type and reason for nonvaccination.
Methods
The institutional review board deemed this quality improvement project exempt. Two family medicine residency training clinics saw 425 patients between 19 and 64 years with any medical indication for PPSV23 between April 1, 2015, and April 30, 2015. Of the 425 patients, 319 had a documented diagnosis of diabetes mellitus, asthma, or cigarette use, and 146 did not receive the PPSV23. One reviewer evaluated the electronic medical record (EHR) to assess why these 146 patients did not receive the vaccine. The search tool within the EHR was used to look for any term related to pneumococcal vaccination at visits with providers during the month of April. The provider notes from each visit were then reviewed to assess why each patient was not vaccinated and which medical indication was present. Patients were then stratified into 3 groups based on the information available in the EHR as to why they were not vaccinated, which included documented refusal, not being addressed by the provider, or being classified as low risk of infection despite the presence of a vaccine indication. Table 1 describes the baseline characteristics of patients included in the analysis. Outcomes were analyzed using Minitab Express 1.3™. Nonparametric continuous data were compared using the Mann-Whitney U test, while discrete variables were compared using χ2 test. A Bonferroni correction adjusted the significance level to P < .017 when analyzing the primary outcome to avoid the introduction of type 1 error when performing multiple χ2 analyses.
Baseline Patient Characteristics.
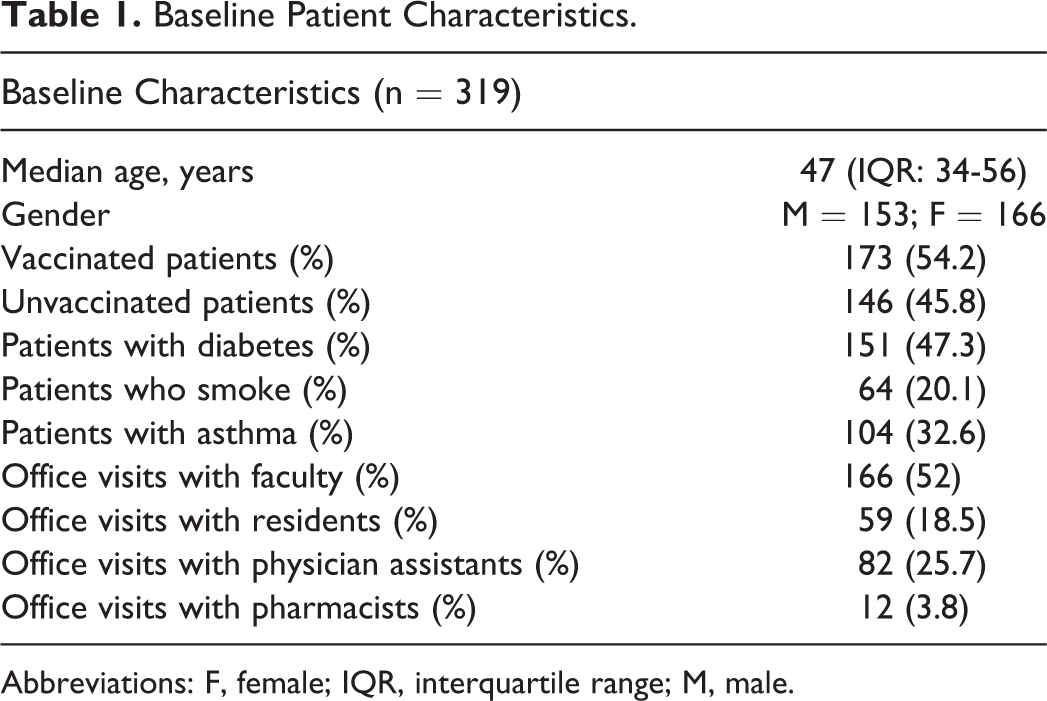
Abbreviations: F, female; IQR, interquartile range; M, male.
Results
There was no statistically significant difference between the number of male and female patients who were vaccinated (P = .9955). There was a statistically significant difference (P < .001) between the median age of vaccinated patients (51 years) and the median age of unvaccinated patients (40 years). The primary outcome assessed differences in PPSV23 vaccination rates among patients with diabetes and asthma and those who smoke. Rates of nonvaccination were 29.8% (n = 45) in those with diabetes, 58.7% (n = 61) in those with asthma, and 62.5% (n = 40) in those who smoke cigarettes. The difference in vaccination rates of patients with diabetes compared with those of patients with asthma and those who smoke was statistically significant (P < .001). There was no statistically significant difference in vaccination rates between those with asthma and those who smoke tobacco (P = .621).
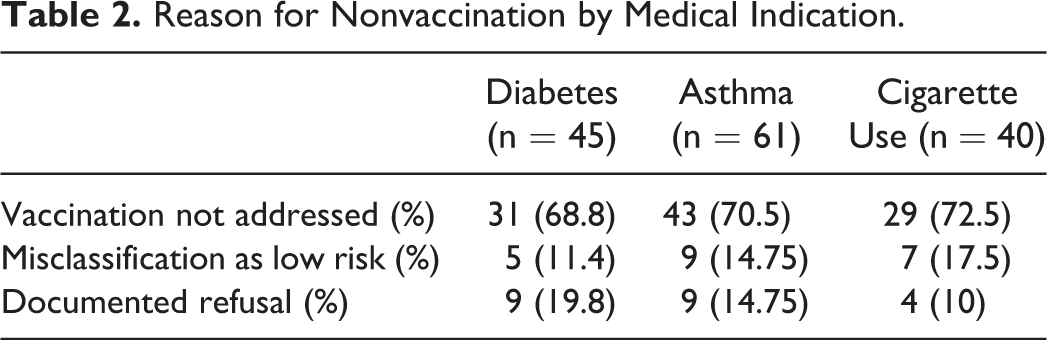
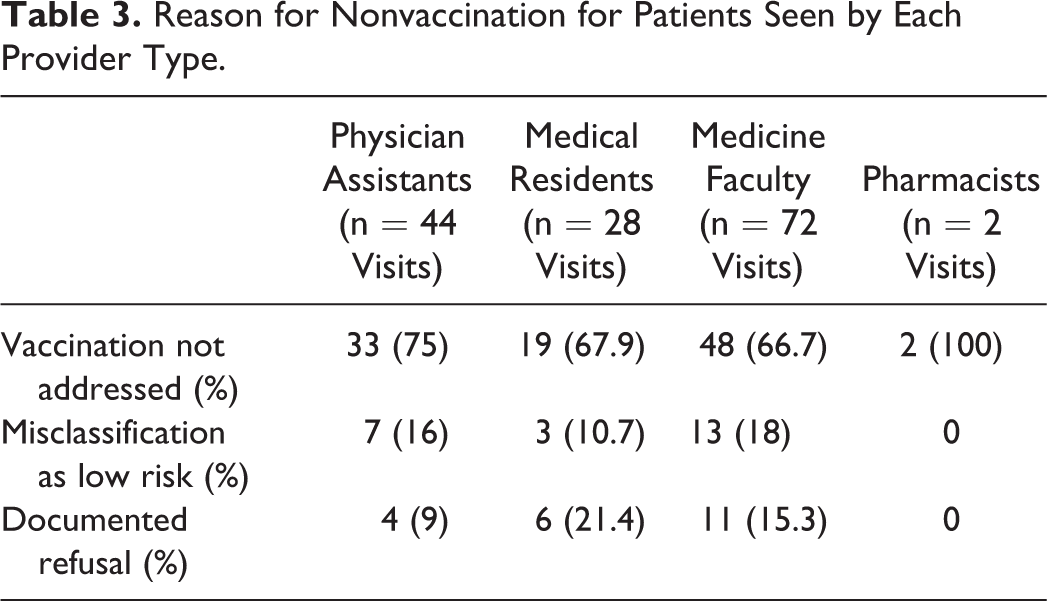
Secondary outcomes assessed rates of nonvaccination by medical indication and by the type of provider seen in the clinic based on the reason for nonvaccination. A total of 319 patients were seen who were eligible for vaccination. Nonvaccination rates by provider type were 53.7% (n = 44) in patients seen by physician assistants, 48.3% (n = 28) in patients seen by medical residents, 43% (n = 72) in patients seen by medicine faculty, and 16.7% (n = 2) in patients seen by pharmacists. The most common reason for nonvaccination was that it was not addressed during the visit. This was followed by misclassification as low risk of infection and documented refusal of vaccination. Table 2 describes the rates of nonvaccination for each medical indication based on the reason for nonvaccination. Table 3 describes the rates of nonvaccination based on the reason for nonvaccination by each provider type.
Reason for Nonvaccination by Medical Indication.
Reason for Nonvaccination for Patients Seen by Each Provider Type.
Discussion
Patients with asthma and patients who smoke were more likely to remain unvaccinated compared to patients with diabetes. The 3 reasons patients were not vaccinated at these clinics were vaccination not being addressed by a provider during a patient visit, documented refusal, and providers misclassifying patients with a medical indication for PPSV23 vaccination as low risk for infection. The median age of vaccinated patients was older than that of unvaccinated patients. Providers may have an easier time identifying patients closer to the age of 65 with medical indications for vaccination because they already acknowledge and adhere to the age-based vaccination at age 65 and older, or because disease severity increases with age, making indications easier to recognize. This may account for the difference in vaccination rates with age. Physician assistants were least likely to vaccinate patients, and pharmacists were most likely to vaccinate patients. Physician assistants and other providers at these clinics see more patients in a clinic session than pharmacists and may have less time to assess vaccination status. Pharmacists are able to spend more time with patients, often managing chronic conditions such as diabetes, asthma, and smoking cessation, which are associated with increased risk of developing pneumococcal disease. This could explain why patients seeing pharmacists had a higher chance of having vaccination addressed during the clinic visit. Lack of prompting in the EHR or lack of knowledge about what severity of asthma or what numbers of cigarettes smoked qualify patients for PPSV23 vaccination may explain why this occurred.
There are some limitations to consider as part of this study. Only one reviewer searched the EHRs of patients for 1 month at these family medicine clinics, and each patient chart was only accessed once. This provides consistent analysis of records but may introduce selection bias results due to lack of review from others. Data were collected using diagnosis codes in the EHR. Patients with diabetes or asthma and patients who smoke may have been excluded from analysis if a documented diagnosis was not present in the EHR. Patients may have had more than one of these medical indications for PPSV23 vaccination, but only the medical indication addressed specifically in the EHR in conjunction with vaccination status was included in the analysis. Data were collected during April 2015, and many patients were excluded from the analysis because they did not see a provider during that time period. Given the season chosen, we may have missed the time of the year when a larger number of patients are prompted to get their pneumococcal vaccines—that is, when they come in to get their influenza vaccine, despite there not being a seasonal need for the pneumococcal vaccine. We did not perform inferential statistics on secondary outcomes. Therefore, conclusions for secondary outcomes are based on descriptive statistics alone. The pharmacists practicing at this clinics are ambulatory care practitioners acting as health-care providers and have advanced training providing primary care. Rates of vaccination and level of pharmacist involvement in vaccine assessment may vary based on practice site.
Conclusions
From this small, time-limited study in 2 clinics, providers overlooked vaccination more commonly in patients with asthma and patients who smoked than in patients with diabetes. The most common reasons for nonvaccination were vaccination not being addressed, misclassification of high-risk patients as low-risk patients for infection, and documented refusal. More provider prompts in the EHR may help improve vaccination in patients at high risk of pneumococcal infection. Because medical indications are often overlooked or not addressed, pharmacists may be able to assist other providers in identifying patients with medical indications. This may help reduce missed opportunities for vaccination. Although pharmacists in this study were ambulatory care providers embedded in these family practice clinics, pharmacists in different practice settings may also help identify patients at high risk of infection and refer them to other health-care providers for vaccination or provide the vaccination. In addition to providing enhanced care, provision of vaccines by pharmacists is a billable service and may contribute to the justification to hire or expand pharmacist services.
Rates of documented refusal are low. Providers have a powerful voice when educating patients about vaccination but are often limited by time and may not address vaccination at each visit. Better quality health care and higher vaccination rates can be achieved by utilizing each type of provider in health-care teams. Although the numbers were small in this study, it does provide information that supports the idea that pharmacists can play a role on the health-care team by partnering with other providers and educating patients about the risk of pneumococcal disease and the benefits of vaccination and should be considered a valued member of the team.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.