
Abstract
Background:
Many studies have shown the positive impact that student pharmacists have on patients’ health; however, no studies have been published evaluating student pharmacists’ impact on direct patient outcomes (ie, readmission, emergency department [ED] visits, length of stay) related to the medication history process.
Objective:
To evaluate the impact of student pharmacist–obtained medication histories on identification of medication discrepancies and clinical outcomes.
Methods:
Student pharmacists obtained medication histories and then compared the history to that obtained by other health-care providers. Students documented discrepancies and interventions were completed. Control patients were identified and discharge medication list and 30-day readmissions were compared.
Results:
Seventeen students conducted 215 patient interviews, and 1848 modifications were made to documented home medications in the electronic medical record. Compared to controls (n = 148 student pharmacist, 149 controls), a nonsignificant improvement was found in discharge medication list completeness scores in patients seen by student pharmacists (3.94 vs 3.63; P = .06); but no difference was found in accuracy scores (0.92 vs 0.93; P = .41). Fewer ED visits at 30 days were found in the student pharmacist group (8 vs 18; P = .045), with no difference in readmissions.
Conclusions:
Student pharmacist–obtained medication histories improved the information available for identifying drug-related problems for inpatients, completeness of the discharge medication list, and ED visits within 30 days.
Introduction
Medication misadventures during transitions of care lead to poor outcomes and increased cost to the health-care system. 1,2 The transition between the inpatient and outpatient setting has been the most extensively studied, and poor communication between providers and the patient has been shown to create the most errors. 2 An accurate and complete medication history obtained at hospital admission provides the foundation for effective medication reconciliation and identification of drug-related problems (DRPs). The Joint Commission’s third National Patient Safety Goal states that health-care providers should “maintain and communicate accurate patient medication information.” 3(pp5,6) Within this goal, NPSG 3.06.01 directly focuses on the importance of maintaining accurate and complete medication information with a focus on medication reconciliation. The benefit of pharmacists performing medication histories include increased accuracy, increased information about herbal and over the counter medication use, and decreased pharmacist time spent in clarifications and physician interventions. 1,4 –7 In a 2012 American Society of Health-System Pharmacists (ASHP) survey, 27% of respondents stated that pharmacists are completing medication histories on admission and 5% utilize pharmacy technicians. 8 Increasing pharmacist involvement has been a slow, incomplete process due to competing priorities and the perception that a pharmacist’s time should be spent verifying and intervening on orders, therapeutic drug monitoring, and formulary management. 9,10
Many studies have attempted to quantify the benefit of pharmacists in the medication history and reconciliation process. 2 For example, Nester and Hale compared medication histories conducted by pharmacists and nurses and demonstrated that pharmacists identified more herbal and nonprescription home medications, true allergic reactions, and performed more clinical interventions. 5 A similar study demonstrated more medication discrepancies identified and dose schedule changes when pharmacists obtained histories compared to physicians. 7 Recently, Gilmore and colleagues described a collaborative effort of a pharmacy team to improve transitions of care and describe engagement of pharmacists, students, and technicians in the care model assisting with medication reconciliation and patient education. 11 Lastly, a systematic review demonstrated benefit from using pharmacy staff in medication reconciliation for patients at high risk of adverse events. 12 Despite the mounting evidence of the benefit offered by pharmacists, little consensus exists regarding the best strategies for engaging students in the medication reconciliation process to improve patient outcomes.
The benefit which students offer to the medication history and reconciliation process has been evaluated in at least 7 published reports. 13 –19 Each of these reports evaluated the number of discrepancies identified between medication histories obtained by nonpharmacy staff and one obtained by the student pharmacist. Each study demonstrated a significant impact on the accuracy of the documented home medication list and provided a rationale for extending the pharmacy departments’ ability to be involved in medication history taking and medication reconciliation by involving students.
The literature supporting pharmacist and student pharmacist involvement in completing medication histories has reported interventions performed and changes made to the patient record with limited impact on hospital readmission. There are numerous variables that may impact this outcome and make it difficult to either achieve or to ascribe benefit solely to a medication history process. A recent survey of hospital pharmacy directors showed that about 30% of departments were involved in medication reconciliation and 30% of that group incorporated student pharmacists as pharmacy extenders. 8 Another study that evaluated the impact of pharmacy students and residents in discharge counseling demonstrated cost savings, greater patient understanding of medications, and no change in readmission rates. 20 Institutions and health-care need to take a broader look at the pharmacist and student pharmacist role in transitions of care because touching the patient at only 1 point in the system has a limited impact. 2 Although student pharmacists have the potential to have a large, positive impact on patients’ health, there are currently no studies evaluating student pharmacists’ impact on direct patient outcomes (ie, readmission, emergency department [ED] visits, length of stay).
We studied student pharmacists performing medication histories and the impact that a more accurate medication history has on the clarity of the discharge list and hospital readmission.
Methods
This study was a retrospective comparison of the impact of student pharmacist–obtained medication histories compared to control patients. The study evaluated 3 primary outcomes: (1) to determine the impact of student pharmacist–obtained medication histories on the accuracy and completeness of the medications prior to admission documented in the electronic medical record (EMR), (2) to determine the impact of student pharmacist–obtained medication histories on the accuracy and completeness of the subsequent discharge medication list compared to control patients, and (3) to compare clinical outcomes (ED visits and hospital readmissions) in patients receiving a student pharmacist–obtained medication history compared to those without. Secondary outcomes included: (1) number of inpatient medication interventions related to DRPs found through the medication history process and (2) types of discrepancies identified between the documented medications prior to admission in EMR and the student pharmacists’ medication history. Outcomes described in this article are separated by outcomes related directly to interview process and those related to comparison of interviewed patients versus control patients. This study was submitted and approved by our university’s institutional review board.
General Process Description
Student pharmacists who were enrolled in their 6-week, Advanced Pharmacy Practice Experiences (APPEs) on a cardiology or internal medicine service participated in the process of obtaining medication histories and aided in medication reconciliation. All student pharmacists received standardized training on how to obtain the best possible medication history at the start of their APPE and were instructed to utilize a specific medication history-taking template (Appendix A). Students were provided with a review of the medication history template, trained on the EMR in order to understand how to interpret and execute documentation, and were observed by preceptors to demonstrate competence in completing medication histories before participating in this study.
Each student collected complete medication histories on patients which included a patient interview, making phone calls to the patient’s outpatient pharmacy, and talking to outpatient caregivers as needed. During the medication history process, students compared the information collected during their patient interview to the documented history in the EMR obtained by other health-care personnel (mainly nurses, physicians, and physician extenders who documented histories within the first 48 hours of admission). Due to the nature of the admission process at our institution, pharmacists were not incorporated into routine medication history documentation process at the time of the study. In this study, after interviewing patients, students then met with their pharmacy preceptor who manually updated the documented medications prior to admission list in the EMR because students lacked that level of EMR access. If the student identified any DRPs on the patient’s inpatient medication regimen based on the medication history, he or she discussed resolution of the problem with the preceptor and attempted to make interventions with the appropriate prescriber. These data were collected and evaluated for the first and second primary as well as secondary outcomes of the study.
Primary outcomes 2 and 3 were evaluated only in patients with a heart failure diagnosis. A discharge medication list was provided to each patient by the nurse upon discharge as part of the standard discharge process. This list was created by the prescriber and was a final reconciliation of the home medication list and the inpatient medications. This discharge medication list had 3 sections: (1) new medications, (2) home medications to continue, and (3) home medications to discontinue. A best possible medication list would include complete and accurate instructions for each medication; correct dose, and medications listed in only 1 of the 3 categories. Appendix B provides an example of best possible and modifiable discharge medication lists. For comparison of discharge medication lists, patients’ list were evaluated for clarity and against a “best possible” list, as in the study conducted by Wong and colleagues. 21
Patients included in the “interviewed group” for the study were interviewed by a student pharmacist on a medicine or cardiology APPE rotation and met the following criteria: greater than 18 years of age, spoke English or whose caregiver spoke English, had no underlying issues that impaired communication, were not transferred from a nursing home, and were admitted for less than 72 hours. If a patient met these criteria, they were assigned to the students for monitoring. Control patients were identified through the Heart Failure Core Quality Measures and were not interviewed by student pharmacists. Patients with a heart failure diagnosis were chosen for comparison of the discharge medication lists because of the high variability seen in the medicine patients on histograms in regard to age, number of disease states, and length of stay. Matching for controls consisted of service type (teaching team vs private physician) and complexity determined by number of medications and comorbid conditions. Control patients were selected during the months that student pharmacists were not on service. Clinical pharmacists at the institution were unit based and were responsible for protocol-based dosing of selected medications thus having equal chance of seeing patients in either group. These pharmacists would have interacted with the students while the students were on service. Patients included in the study were admitted during the calendar year of 2011.
Demographic data (age, gender, length of stay), number of disease states listed in the admitting past medical history, and type of admitting service were collected on all patients. Screenshots of the medication history prior to student interview, after student interview, and all discharge medication lists were gathered for evaluation by the primary investigators. Investigators utilized a Medication History Data Collection sheet to standardize evaluation of these documents for each patient.
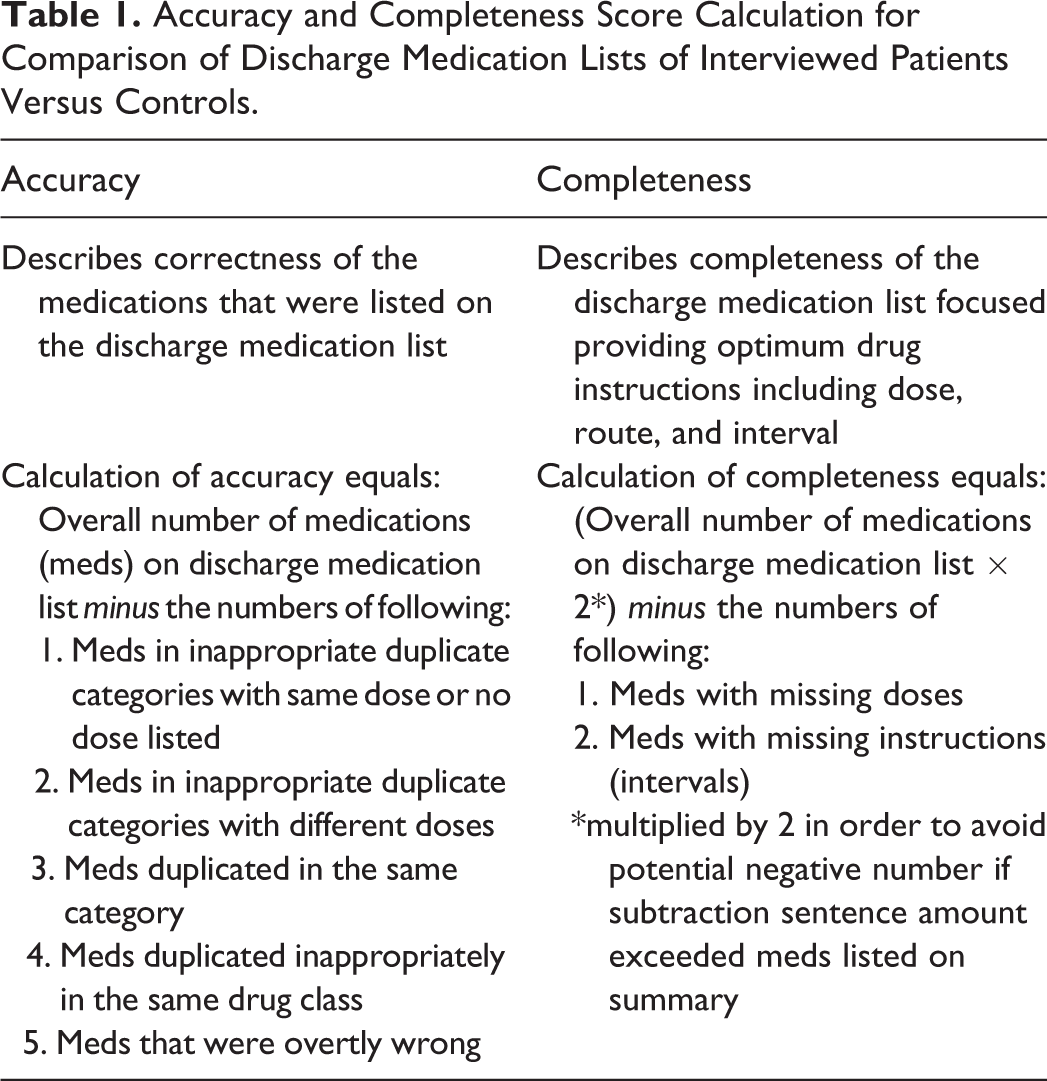
Due to lack of standardization of the previous literature describing accuracy and completeness, investigators worked with a local statistician to develop an accuracy and completeness calculation. Accuracy and completeness scores of the discharge medication list for all patients were determined using the calculations described in Table 1 by 2 of the investigators. If investigators disagreed on scores, the more conservative (lesser) number was chosen. Categories of data used for these calculations are shown in Table 2. Readmission and ED visit data were collected through the EMR and did not include visits to other health-care systems.
Accuracy and Completeness Score Calculation for Comparison of Discharge Medication Lists of Interviewed Patients Versus Controls.
Comparison of Types of Medication Errors Found on the Discharge Medication List Between Controls Patients and Patients Who Were Interviewed by a Student Pharmacist.
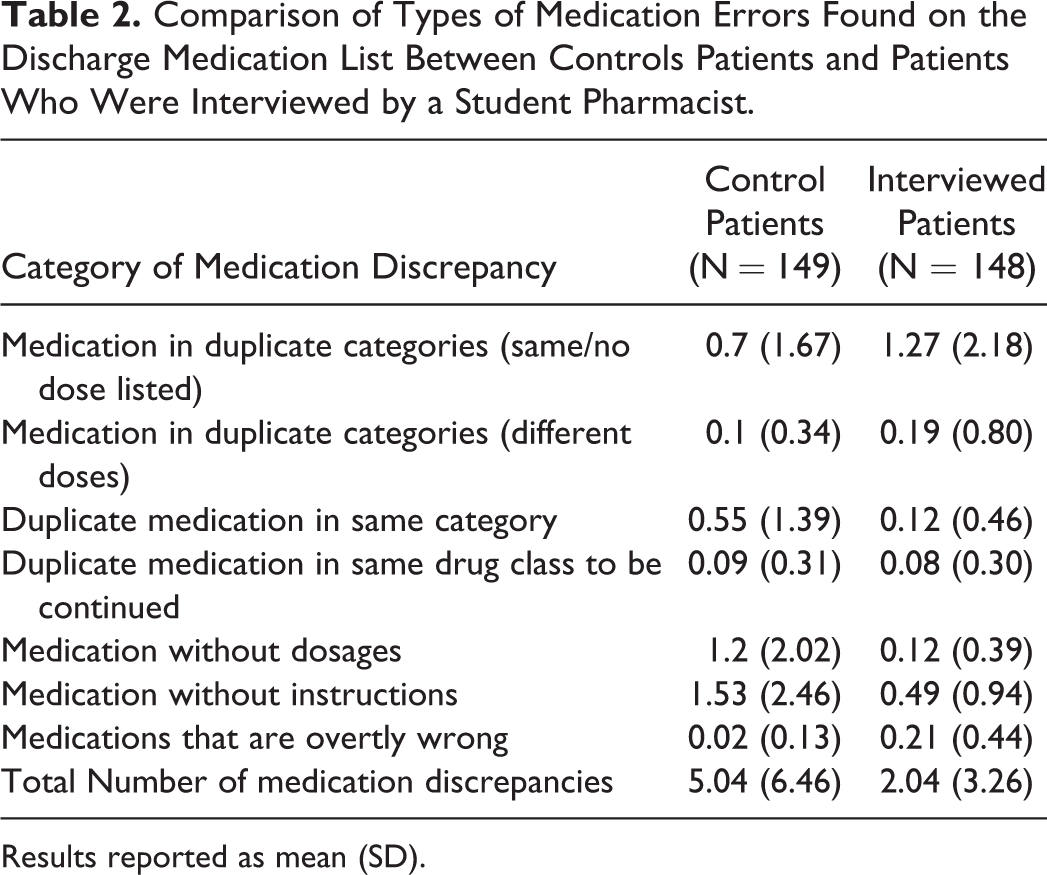
Results reported as mean (SD).
Data were evaluated using Microsoft Excel version 2013© to evaluate data for patients interviewed by student pharmacists and IBM SPSS Statistics version 22© to combine and evaluate data of matched interviewed and control patients. Descriptive statistics were used to characterize all quantitative variables including patient interview data regarding medication history changes. Data are presented as mean (standard deviation) for continuous variable and percentages for categorical variables, unless otherwise noted. For the patient groups, primary end points of accuracy and completeness scores were calculated as shown in Table 1 and then compared via analysis of variance, controlling for number of diseases stated per EMR. Emergency department visits and readmissions were evaluated via chi-square.
Results
A total of 215 patient medication histories were obtained by 17 student pharmacists over the 12-month period. The student pharmacists spent a mean of 19.2 (9) minutes interviewing patients and contacting outpatient pharmacies (170 pharmacies contacted). After comparing the patient’s home medication list in the EMR and the student pharmacist’s history, 96% of patient’s home medication lists required modification and the mean number of changes made per patient to the EMR medication history was 8.7 (5.6) changes. Types and quantities of modifications made to the patients’ EMR medication history are shown in Figures 1 and 2. As a direct result of information from the medication history, a total of 76 interventions to inpatient regimens, affecting 25% of patients, were completed by student pharmacists through communication with prescribers.
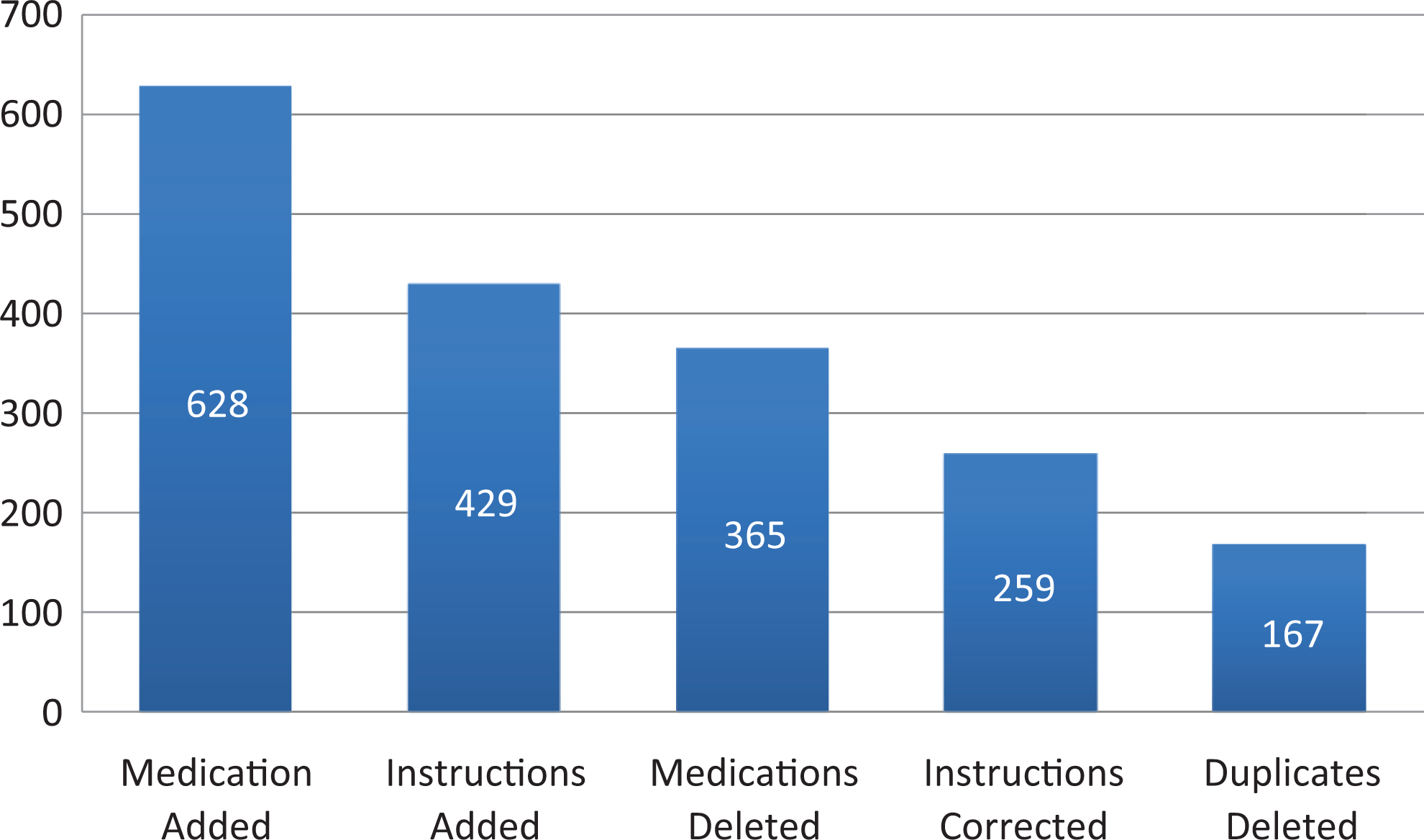
Types of changes made to the home medication list in the electronic medical record for 215 patients interviewed.
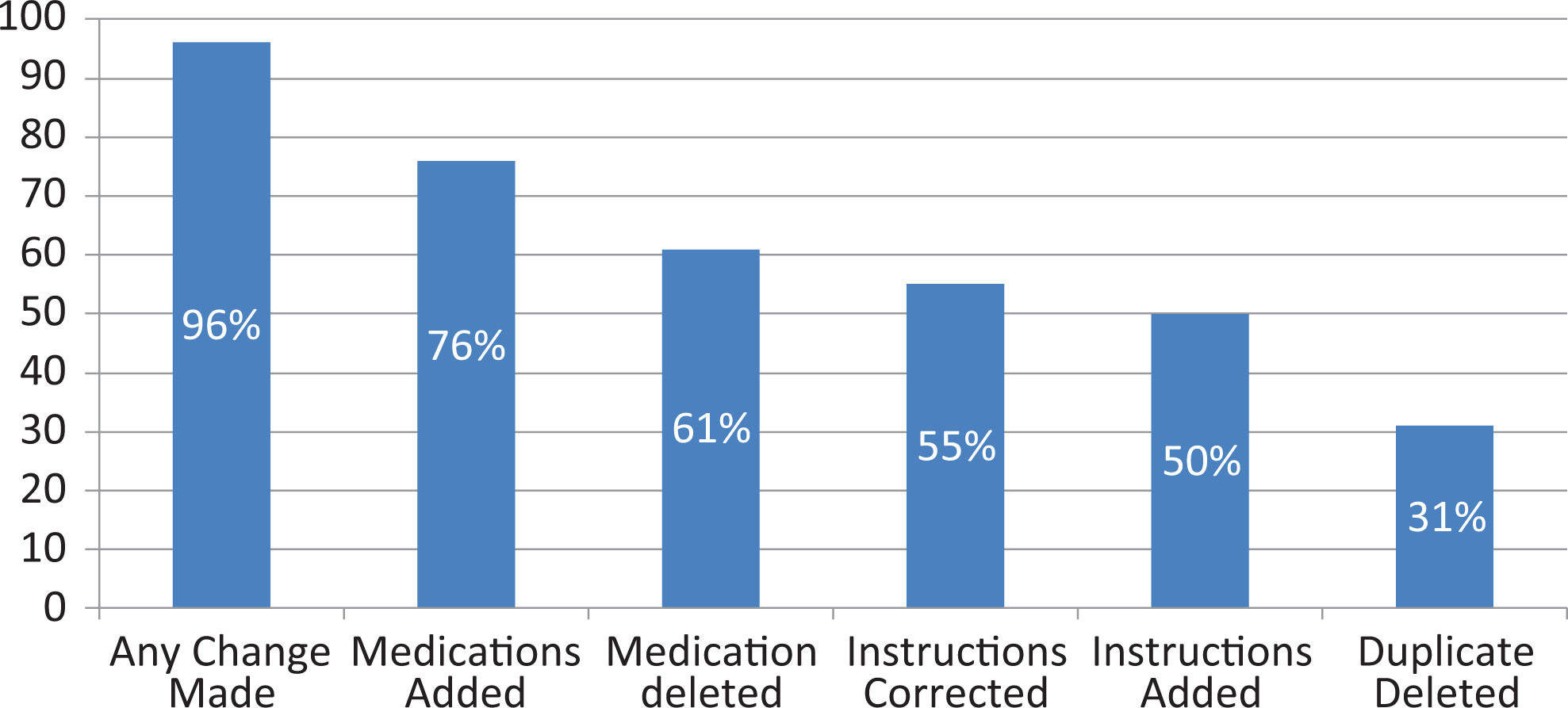
Percentage of patients (n = 215) who had changes made to their home medication list in the electronic medical record.
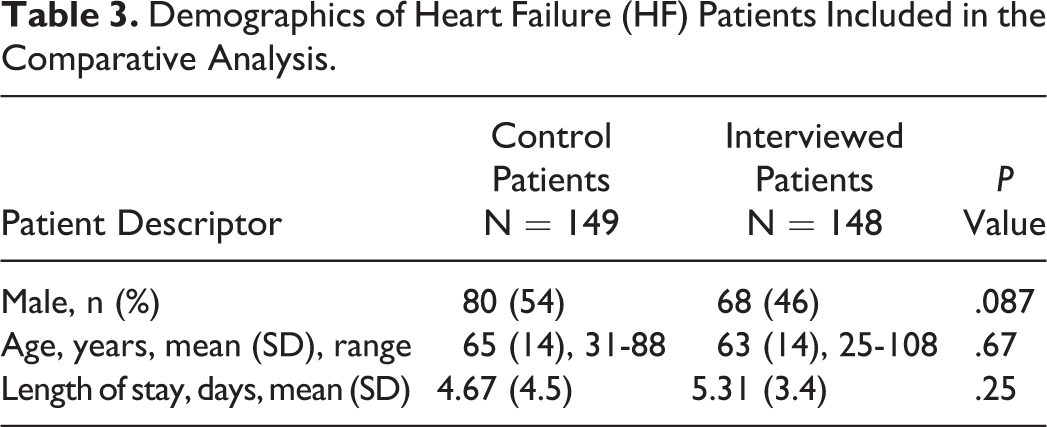
Among the 297 heart failure patients identified (n = 149 controls; 148 interviewed), no difference was seen in gender, length of stay, or age as shown in Table 3.
Demographics of Heart Failure (HF) Patients Included in the Comparative Analysis.
Variability was seen when comparing the discharge medication lists and patient outcomes for control heart failure patients versus heart failure patients interviewed by student pharmacists. Types of medication discrepancies found in the home medication list are described in Table 2. When calculating accuracy, there was no difference among heart failure controls and interviewed patients (scores of 0.93 [0.10] vs 0.92 [0.12]; P = .41). Control heart failure patients had lower completeness scores when compared to patients interviewed by student pharmacists but did not achieve statistical significance (3.63 [0.24] vs 3.94 [0.06]; P = .06). In addition, control heart failure patients had significantly more ED visits at 30 days than patients interviewed by student pharmacists (total visits per group: 18 vs 8; P = .045) but similar hospital readmission rates at 30 days (total visits per group: 34 vs 32; P = .85).
Discussion
To our knowledge, this is the first published study involving student pharmacist–directed medication histories that evaluates clinical impact and patient outcomes of readmission and ED visits. A significant difference was seen in ED visits at 30 days between the student pharmacist–interviewed patients and control patients, a result not found in previous studies. Multiple factors may have led to these results, but the number of student interventions performed, patient education, and the improved completeness of the discharge medication list may have played a role. Of note, in this study’s control group, the individual medication discrepancy of highest amount was “medications without instruction” followed by “medications without dosages.” Given this fact, it is possible that the interviewed patient group benefitted greatly from the improved completeness (score being primarily defined by writing of dosing and instructions) of discharge medication lists thus being a contributing factor to reduced ED visits. The focus and training of a student pharmacist in pharmacotherapy, order evaluation, and pharmacy law, likely encourages their attention to these critical details of dosage and instructions. 22
Similar to our study, Walker and colleagues studied the effects of pharmacist involvement in obtaining medication histories and aiding in the medication reconciliation process on rehospitalization rates at 14 and 30 days and ED visits within 72 hours after discharge. 6 While Walker and colleagues did not see a difference in groups related to readmissions or ED visits, they did find that postdischarge telephone calls reduced the 14-day readmission rate. Overall readmission rates were higher than the Walker study (our groups ranging 32 and 34%; Walker’s 20% at 30 days) but may be explained by our patient population being exclusively heart failure patients who have higher rates of readmissions. Results from our study support the growing data demonstrating the benefit of student pharmacist and pharmacist involvement in transition of care activities. 8
We identified 7 studies that describe the benefit of student pharmacist–obtained medication histories that have similarities in student training required and in the general patient interview process. 13 –19 Similar to our practice site, all of the previously published studies were at institutions without pharmacy services that were established in obtaining medication histories. 13 –19
Some similarities and differences existed between our results and those previously published when looking at patient types and intervention rates. When reported, the mean age (years) of patients were similar (Lubowski et al 66, Lancaster and Grgurich 67, ours 63-65 group dependent). 14,16 Similarly, several of the studies had greater than 75% of patients identified as having an inaccurate medication history (Padiyara 75%, Lubowski et al 75%, Procopio et al 76%, ours 96%). 13,16,18 Study by Mersfelder and Bickel stated that 67% of patient charts had a medication or dosage omitted but did not include clarifications for directions or frequency in this and therefore was lower than the other stated studies. 15 A high number of patients required additional pharmacy intervention of contacting their outpatient pharmacy to obtain a recent medication list (Padiyara 68%, ours 79%, Mersfelder and Bickel 99%). 13,15 The study by Mersfelder and Bickel required a medication history within 36 hours of admission. This may have increased the likelihood of contacting outpatient pharmacies because of increased patient acuity close to admission. 15 Lastly, differences existed in the average amount of time reported in taking the actual medication histories and ranged from about 5 to 22 minutes (Procopio et al 5.3, Lubowski et al 9.3, Pinelli et al 21.5, and ours 19.3 minutes). 16,18,19 These differences may be due to methods of data reporting. Student pharmacists in our study included all communications with pharmacies and caregivers and not just the time spent in the patient room in the time required for completing the medication history. Utilizing students to perform medication reconciliation is also an additional method in identifying medication errors or medication-related problems (MRPs) as was found in the study by Pinelli and colleagues. 19 Their student medication and reconciliation team (SMART) method identified 0.9 MRPs per patient.
One of the challenges in comparing these studies is that there is no standard method for quantifying medication discrepancy number, category, or accuracy. For example, a variety of numbers of medication discrepancies were found upon patient interview when comparing the other health-care provider’s medication history and the student pharmacists’ with the mean medication discrepancies ranging from about 1 to 9 (Pinelli 0.9, Procopio et al 2.9, Lubowski et al 3, Lancaster and Grgurich 5, ours 8.7). 14,16,18,19 The description of these discrepancies varied. For example, 3 of the studies reported combined “omissions” and “medications added” ranging from 27% to 66% of discrepancies, while we defined 34% of discrepancies as “medication added.” 14,17,18 One of the potential limitations of our study was our assessment of correctness accounting for medication discrepancies. We had developed and utilized a calculation formula for accuracy and completeness that had not been previously used.
The functionality and capability of the EMR at each institution is an essential tool in creating the home medication list (or medication history list). Each system is different and dynamic, creating difficulty in comparing studies and generalizing results. Since this study was completed, the EMR at our institution has been enhanced to include an “external medication history” which provides medication fill and refill data through an insurance database. Additionally, this study provided the impetus to allow students to participate more actively in updating the home medication list through changes made to student access, training, and preceptor supervision. In order to provide process improvements within the EMR, it is essential for the department of pharmacy to be involved with Information Technology Services and other health-care professionals as decisions are made and upgrades are implemented within the EMR. 23,24
A systematic review of medication reconciliation interventions did not demonstrate a decrease in rehospitalization but hypothesized that an impact would be seen if these activities were bundled with other interventions at the transitions of care. 25 The ASHP-American Pharmacists Association Medication Management in Care Transitions Best Practices supports this hypothesis, and as a result, 8 organizations were awarded the ASHP Best Practice Award secondary to demonstrating a decrease in hospital readmissions. 26 Each of these organizations intervened with the patient multiple times during the transition of care providing patient education, assistance with access to medications, and postdischarge follow-up. Four institutions were involved with admission reconciliation and 7 were involved with discharge reconciliation. The inclusion of students in each of these activities provides an additional means for improved patient care, expanded pharmacy services, and an enhanced educational experience. 27
In view of the competing priorities that pharmacists encounter on a daily basis, student pharmacists can provide a valuable resource for improving patient care. In addition, the Accreditation Council on Pharmacy Education’s 2016 standard expects students to be “practice ready” at the time of graduation which includes an emphasis on continuity of care, professional communication, and patient safety. 13 When students practice as pharmacist extenders by participating in consultant and dispensing roles, intravenous to oral switching, identifying and resolving DRPs, and participating in multidisciplinary patient care teams, health systems can provide improved patient care. 28 Initiating a student medication history program can expand the scope of pharmacy services and improve patient care without negatively impacting the pharmacist clinical service time and department resources. We recommend a thoughtful approach to this process that includes adequate and consistent training of students and evaluation and integration with the EMR. 29 In order to extract the maximal benefit from pharmacist involvement, patients should receive care from the pharmacist throughout the transitions of care and not at only one point.
Conclusion
Student pharmacist–obtained medication histories improve the information available for identifying DRPs for inpatients and may enhance the quality of the discharge medication list leading to improved patient outcomes.
Footnotes
Appendix A
Appendix B
Acknowledgments
The authors would like to thank Zeb Keehn at the Research Design and Analysis Unit at Wayne State for his assistance and the Advanced Pharmacy Practice Experience students for their engagement in patient care.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.