
Abstract
Background:
The 2013 Society of Critical Care Medicine guidelines for the management of pain, agitation, and delirium in adult intensive care unit (ICU) patients recommend intravenous opioids as first-line therapy to treat nonneuropathic pain. There is a paucity of literature describing possible benefits of utilizing specific opioids over others in ICU patients.
Objective:
The objective was to identify rationales for the transition from continuous infusion fentanyl to continuous infusion hydromorphone in critically ill patients.
Methods:
This was a single-center, prospective, observational analysis of adult ICU patients who were transitioned from fentanyl to hydromorphone. The major end point was to characterize the primary reason for transition. Minor end points included secondary reason(s) for transition, transition dosing, changes in continuous sedative requirements, and level of sedation.
Results:
Forty-six patients were included in the analysis. The primary rationale for transition was ventilator compliance (28.3%), followed by tachyphylaxis or better pain control (19.6%), and reduction in sedatives (13.0%). The most common secondary reason(s) for transition included reduction in sedatives (47.8%), opioid rotation (32.6%), and obesity (30.4). Median fentanyl rate of 100 µg/h was transitioned to 1 mg/h of hydromorphone. The percentage of patients requiring the use of continuous sedatives was decreased in the 24 hours following transition (P = .005); however, patients were more deeply sedated (P = .02).
Conclusion:
Rationales for transition were to improve ventilator compliance, optimize patient-specific pharmacokinetics, and limit overall sedative exposure.
Background
The 2013 Society of Critical Care Medicine (SCCM) guidelines for pain, agitation, and delirium (PAD) recommend intravenous (IV) opioids as first-line therapy to treat non-neuropathic pain in critically ill adult patients. 1 The use of analgesia first approach or analgosedation in mechanically ventilated patients has shown to reduce time on the ventilator and intensive care unit (ICU) length of stay. 1 -4 SCCM guidelines state all IV opioids, when titrated to similar pain intensity end points, are equally effective. However, this recommendation (Grade C) is based on a low quality of evidence. While there are limited data comparing IV opioids in critically ill patients, the guidelines do state that both medication- and patient-specific factors may lead to one opioid having benefits in certain populations over another. 1
Critically ill patients undergo many physiologic changes, which may result in significant alterations in drug absorption, distribution, metabolism, and excretion. 5 Fentanyl has been shown to have varying pharmacokinetics in critically ill populations, particularly in patients with a history of liver disease, congestive heart failure, and obesity. 6 -9 Hydromorphone may have favorable pharmacokinetic and pharmacodynamic properties in critically ill populations, as it is metabolized via glucuronidation instead of cytochrome P450 enzymes (CYP450), has minimal renal excretion of active drug, and is less lipophilic, limiting its distribution into tissues. 10
There is a paucity of literature describing possible differences between opioids in the critically ill. At our institution, fentanyl is the most commonly used opioid for continuous infusion administration in our ICUs. 11 However, patients are often transitioned to hydromorphone for various reasons. The objective of this analysis was to determine the patient-specific factors that led to a transition from fentanyl to hydromorphone and then to assess the clinical impact.
Methods
A single-center, prospective observational analysis was performed at Brigham and Women’s Hospital, a 793-bed acute, tertiary care, academic medical center in Boston, Massachusetts. Brigham and Women’s Hospital institutional review board approval was obtained prior to the start of this study. All adult patients admitted to an ICU between July 1, 2016, and January 31, 2017, who were transitioned from continuous infusion fentanyl to continuous infusion hydromorphone were eligible for inclusion in the study. Patients were excluded from the study if they met any of the following criteria: received less than 6 hours of continuous infusion fentanyl or less than 6 hours of continuous infusion hydromorphone, continued on both continuous infusion fentanyl and continuous infusion hydromorphone concomitantly for greater than 6 hours, if there was a period of greater than or equal to 3 hours between the transition where there were no infusion rates documented, or if the primary reason for transition was for comfort measures.
A hospital reporting system was used Monday through Friday to identify all adult patients in an ICU who were ordered for continuous infusion hydromorphone daily. For all patients who met inclusion criteria, the pharmacist managing the patient was interviewed within 24 hours of the transition from fentanyl to hydromorphone in order to determine the primary and secondary reason(s) for the change (please see supplementary material). The study group was responsible for conducting the interview within the appropriate time frame. The study group also independently reviewed the patient’s medical chart to confirm the proposed reasons for the transition.
Data collected included patient demographics, pertinent baseline laboratory results, pertinent past medical history, opioid requirements prior to admission (enteral morphine equivalents), admission Acute Physiology and Chronic Health Evaluation (APACHE) II and Sequential Organ Failure Assessment (SOFA) scores, liver function tests, Richmond Agitation and Sedation Scale (RASS) scores, patient reported or behavioral pain scores, and sedative and vasopressor requirements. Infusion rates of analgesics and sedatives, sedation and pain assessments, and vasopressor requirements were collected for 48 hours prior to and posttransition. Data collection was performed by the primary investigator and the members of the study team throughout the study.
The major end point of this analysis was to determine the primary reason for the transition from continuous infusion fentanyl to continuous infusion hydromorphone. Minor end points included secondary reason(s) for the transition from continuous infusion fentanyl to continuous infusion hydromorphone, along with the fentanyl to hydromorphone transition dosing. Overall sedation and opioid requirements (expressed in fentanyl equivalents) were compared by calculating each patient’s average rate over the total infusion time within the 24-hour period. The average rate was then calculated into a total daily requirement. The percentage of patients requiring continuous infusion sedatives and sedation level based on RASS assessments (deep sedation defined as RASS −4 to −5; light sedation defined as RASS −1 to −2) were compared 24 hours pre and posttransition. 12 Additionally, opioid, benzodiazepine, and antipsychotic use were also evaluated 24 hours pre and posttransition. To evaluate safety measures surrounding the transition to hydromorphone, changes in vasopressor requirements and positive pain assessment (defined as a critical-care pain observational tool greater than 2 or visual analog scale greater than or equal to 3), along with spontaneous breathing trial (SBT) success rates (defined by pass/fail documentation by respiratory therapist), were also evaluated in the 24 hours surrounding the transition. 13,14 An a priori subgroup analysis of patients in which the transition reason included ventilator compliance were also evaluated.
Continuous data were analyzed using paired t test (parametric data, expressed as mean [standard deviation]) or Mann-Whitney U test (nonparametric data, expressed as median and interquartile range [IQR]) when appropriate. Chi-square test, with the Yates correction, was used when appropriate for categorical data. Fisher’s exact test was used for categorical data with rare events.
Results
During the study period, 58 patients were evaluated for inclusion, of which 46 patients were included in this analysis. A majority of patients were excluded for receiving either fentanyl or hydromorphone infusions for less than 6 hours (n = 7). Patient baseline demographics are presented in Table 1. One patient was included in the analysis twice due to meeting inclusion criteria on separate occasions during the defined study period. The most common primary reasons selected for transition from continuous infusion fentanyl to continuous infusion hydromorphone were ventilator compliance with/without Acute Respiratory Distress Syndrome (ARDS), followed by improvement in pain control (tachyphylaxis or better pain control), opioid rotation, and reduction in sedatives. The most common secondary reason(s) for transition included reduction in sedatives, opioid rotation, obesity, and liver dysfunction. Additional primary and secondary reasons for transition are shown in Table 2.
Baseline Demographics.

Abbreviations: ALT, alanine aminotrasnerase; APACHE, Acute Physiology and Chronic Health Evaluation; ARDS, acute respiratory distress syndrome; AST, aspartate aminotransferase; BMI, body mass index; CHF, congestive heart failure; CPOT, critical-care pain observational tool; ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; INR, international normalized ratio; IQR, interquartile range; RASS, Richmond Agitation and Sedation Scale; SD, standard deviation; SOFA, Sequential Organ Failure Assessment; VA, veno-arterial; VV, veno-venous.
a Data presented as mean (SD).
b Data presented represents 45 patients.
c Data presented as median (IQR).
d Data compared found no statistically significant difference.
Major Outcomes.
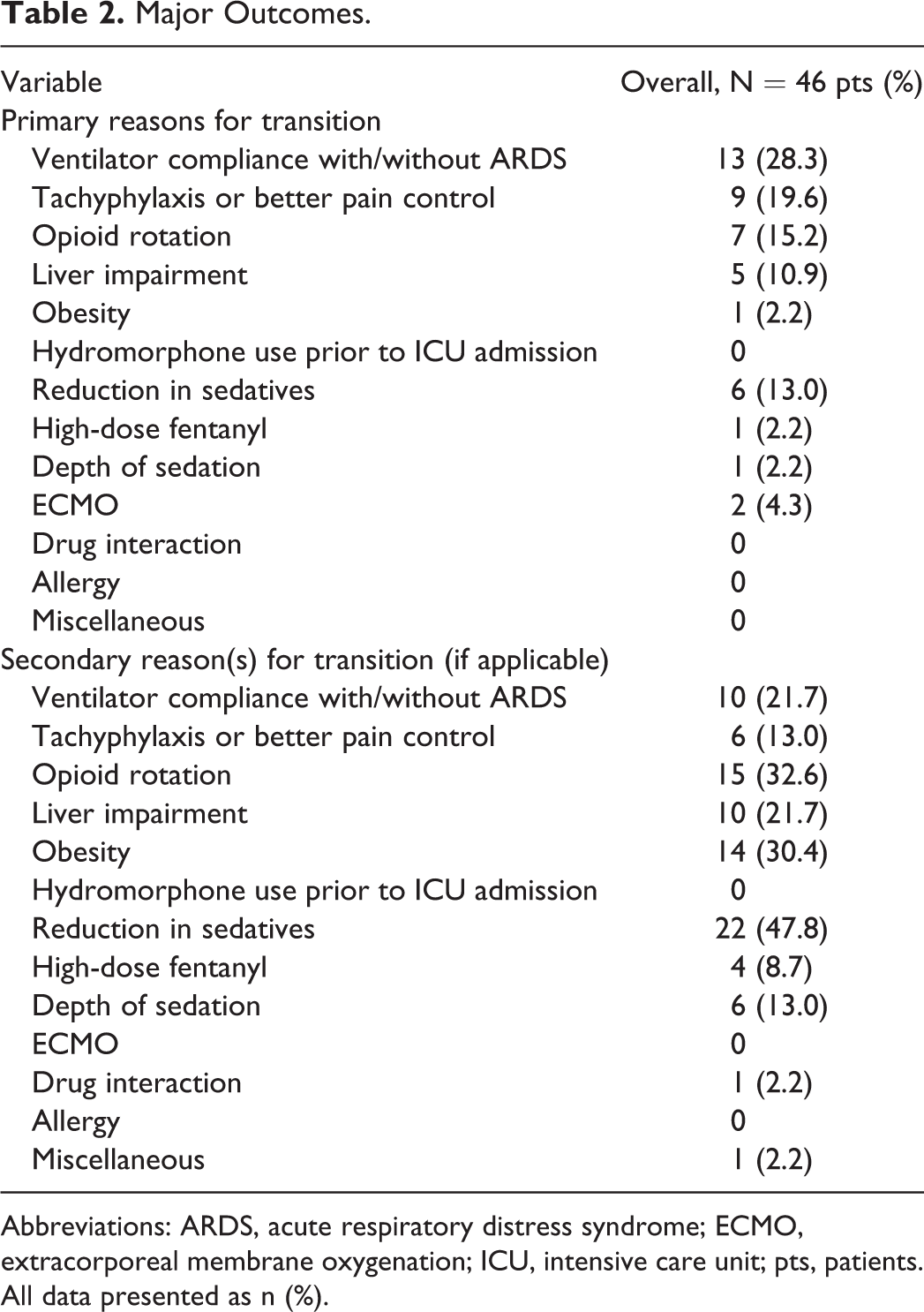
Abbreviations: ARDS, acute respiratory distress syndrome; ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; pts, patients.
All data presented as n (%).
The median duration of continuous infusion fentanyl prior to transition was 64.5 hours, with a median rate of 100 µg/h at transition. The median hydromorphone starting rate was 1 mg/h and was continued for a median of 96.5 hours. The amount of total opioid administered did not differ in the 24 hours surrounding transition (Table 3). In the 24 hours surrounding transition, there was no difference in positive pain scores as shown in Table 3.
Minor Outcomes.
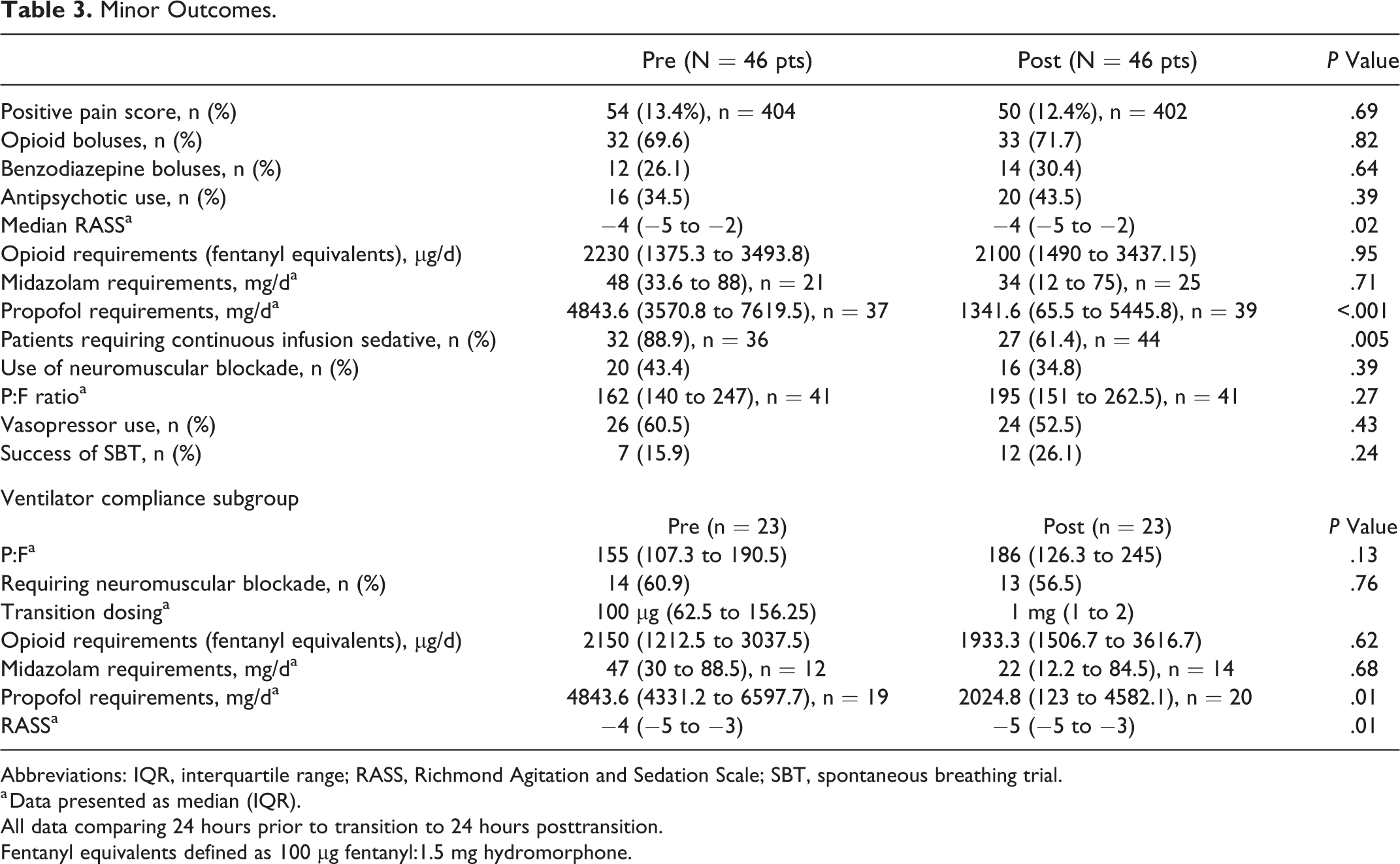
Abbreviations: IQR, interquartile range; RASS, Richmond Agitation and Sedation Scale; SBT, spontaneous breathing trial.
a Data presented as median (IQR).
All data comparing 24 hours prior to transition to 24 hours posttransition.
Fentanyl equivalents defined as 100 µg fentanyl:1.5 mg hydromorphone.
The median RASS scores were −4 during the 24 hours prior to and after transition. Despite median RASS values being the same in both the groups, this was found to be a significant difference (P = .02; Figure 1). The amount of propofol that was administered in the 24 hours following transition was significantly less than the 24 hours prior (P < .001). No difference was seen with midazolam (Table 3). The percentage of patients who required any continuous infusion sedative significantly decreased 24 hours posttransition compared to 24 hours prior to transition (P = .005; Figure 2). No significant differences were observed with regard to the administration of antipsychotics, paralytic agents, vasopressor agents, or boluses of benzodiazepines or analgesics (Table 3). A greater percentage of patients were able to successfully pass an SBT following transition (15.9% vs 26.1%); however, this was not found to be statistically significant (P = .24).
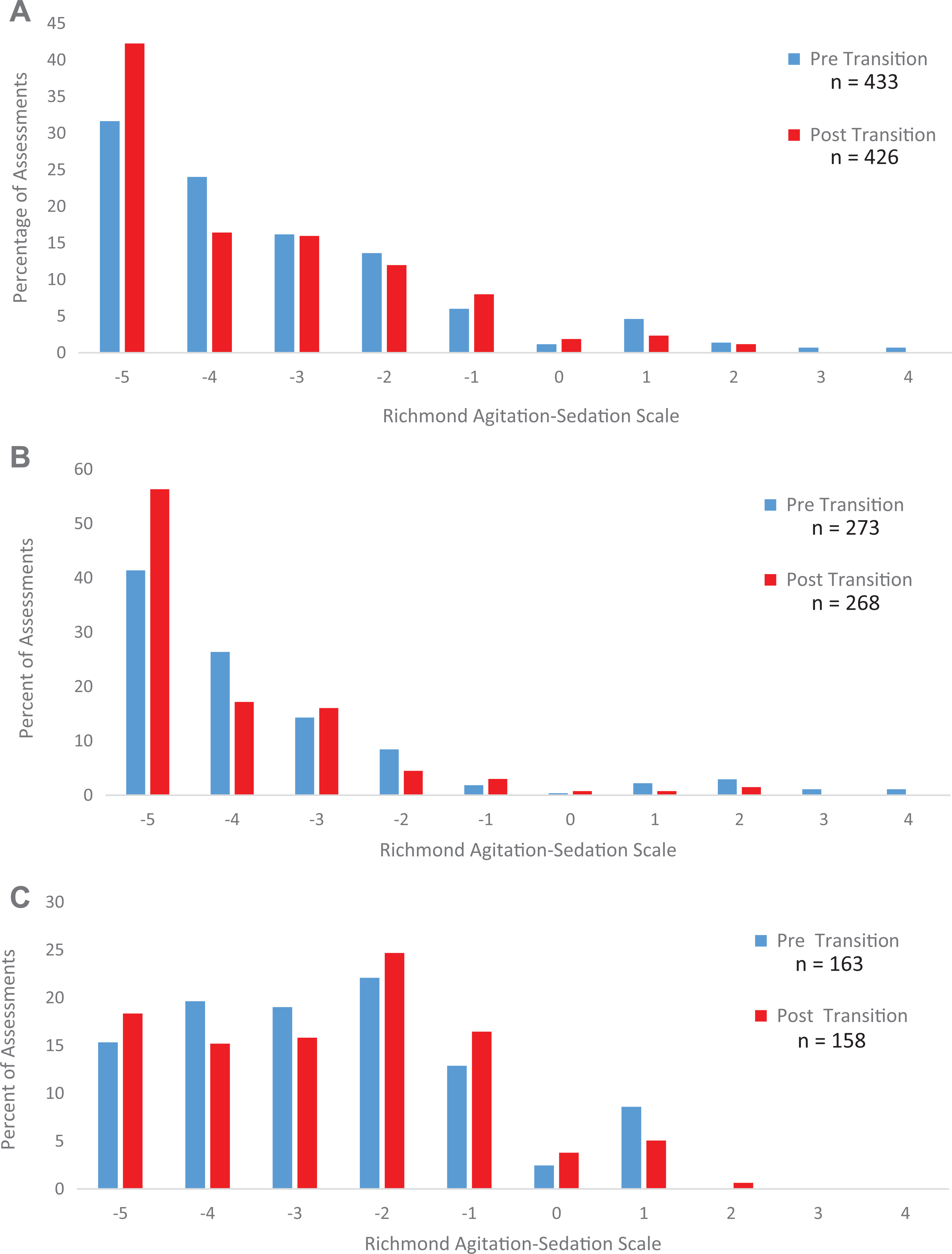
Median RASS scores in 24 hours surrounding transition. A, Represents the distribution of median RASS score 24 hours pre and posttransition for all patients in the cohort (N = 46 patients). B, Represents the distribution of median RASS scores for patients with ARDS (N = 30 patients). C, Represents the distribution of median RASS scores for all patients without ARDS (N = 16 patients).
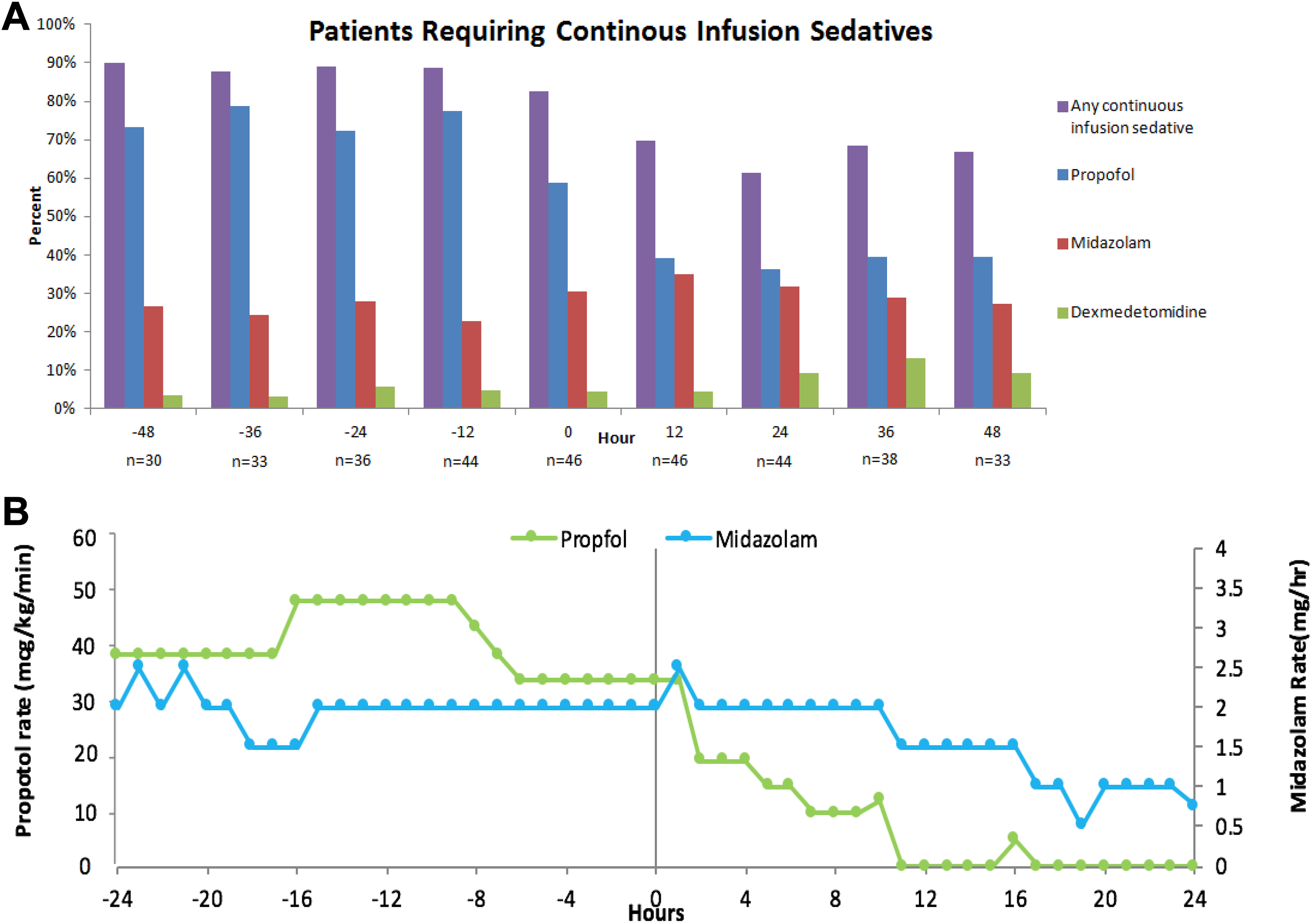
Continuous infusion sedatives. A, Represents the percentage of patients requiring any continuous infusion sedatives. B, Represents the median hourly rates of both propofol and midazolam 24 hours pre and posttransition.
Patients who were transitioned for the reason of ventilator compliance with or without ARDS made up the majority of the cohort. Following the transition, propofol requirements were still significantly reduced (P = .01), with no difference in midazolam requirements (P .68; Table 3). Median RASS assessment scores in patients with ARDS were significantly decreased following transition to hydromorphone (P = .002; Figure 1). There was no difference in patients requiring neuromuscular blockade (P = .76). Patient Pa
Discussion
To our knowledge, this is the first analysis to primarily evaluate the patient-specific factors that may impact clinical decision-making on IV opioid choice in critically ill patients. Patients included in this analysis were mostly middle-aged male medical ICU patients who were critically ill with a median APACHE II score of 29 and SOFA score of 12 upon admission. At the time of transition, these patients remained critically ill, as median SOFA scores were unchanged. Of these patients included, 30 (65.2%) patients had the diagnosis of ARDS during the time of their ICU stay.
Overall, half of the population in our analysis had a transition reason including improved patient ventilator compliance, and even more had a goal of reducing the amount of sedatives they were receiving. When analyzing overall sedative exposure, the transition from fentanyl to hydromorphone was associated with a reduction in sedatives. Daily propofol requirements were significantly reduced as was the percentage of patients who needed a continuous infusion of any sedative. Midazolam requirements were not reduced overall; however, patients with ARDS received about 50% less benzodiazepines in the 24 hours posttransition. Despite this large decrease in requirements, this finding may not have been significant due to the small number of patients receiving a midazolam infusion.
In the ARDS network studies, lung-protective ventilation strategies, mainly administration of low tidal volumes and high positive end-expiratory pressures, have been shown to decrease mortality in patients with ARDS. 15,16 Oftentimes it is necessary to utilize higher doses of sedatives and analgesics in patients with complex ventilator settings, resulting in deep sedation (RASS: −4 to −5). 17 These doses of sedatives and analgesics, and if necessary paralysis, are sometimes warranted for the tolerance of lung-protective ventilation strategies to limit patient–ventilator asynchrony, which may lead to further alveolar collapse and overdistention. 15 -20 Hydromorphone was shown to reduce overall sedative exposure. We also saw an increase in the number of successful SBTs 24 and 48 hours after transition, possibly due to the reduction in continuous sedation. In patients experiencing ventilator dyssynchrony, patient–ventilator compliance may be improved with the use of hydromorphone.
The 2013 SCCM PAD guidelines recommend targeting light sedation in most ICU patients utilizing analgosedation or analgesia first sedation. 1 Analgosedation has been shown in multiple studies to reduce time on mechanical ventilation, agitated delirium, and ICU length of stay. 1 -4
When evaluating patients without ARDS, there was no difference found in median RASS assessment scores. However, comparing this to the entire cohort, we believe the significant difference found between median RASS scores was based on the distribution, with a higher percentage of patients with RASS scores between −4 and −5 in the hydromorphone group. These findings suggest when titrating to light levels of sedation, hydromorphone may limit overall sedative exposure while still achieving goal level of sedation. Further investigation is warranted to confirm the signal suggesting the decreased need for sedatives in patients receiving hydromorphone.
In the tertiary literature, the dose equivalence of fentanyl and hydromorphone is 100 µg:1.5 mg. 1,10 Up to a 50% dose reduction is standard when converting from one opioid to another, and our analysis found a conversion equating to 100 µg: 1 mg (33% reduction). 21 We also found that patients were more deeply sedated, despite decreased sedative use after transitioned to hydromorphone. Further analysis may be warranted to evaluate fentanyl and hydromorphone equivalent dosing, especially when used as continuous infusions in the critical care setting.
Fentanyl is a highly protein bound (80%-85%) lipophilic agent with a large volume of distribution (VD: 3.2 to 5.9 L/kg), which is highly dependent on hepatic blood flow and synthetic function for metabolism via CYP3A4, due to a hepatic extraction ratio between 0.7 and 1.0. 6,7,22 Due to the anticipated pharmacokinetic and pharmacodynamic changes in certain critically ill patients, fentanyl may not be the optimal agent in all patients. 8,23 A pharmacokinetic study by Choi and colleagues determined severe liver disease, congestive heart failure, and weight strongly influenced clearance and plasma concentrations of fentanyl. 6 Hydromorphone, a less lipophilic and protein bound agent (10%-25%), has a smaller VD (2.9 L/kg) and does not depend as heavily on synthetic function or hepatic flow for metabolism. Hydromorphone goes through phase II metabolism via glucuronidation, thus, it may be impacted to a lesser degree by acute liver dysfunction as would fentanyl going through phase I metabolism. 5,24,25 In this analysis, pharmacokinetics played a role in opioid selection for critically ill patients. Important factors were patients with a history of hepatic disease or with shock liver, and alterations in VD, such as obesity or extracorporeal membrane oxygenation (ECMO) cannulation.
There are several limitations to this study. This was a single-center, observational study that evaluated primarily medical ICU patients. There was no comparison made between separate groups of patients receiving fentanyl versus those receiving hydromorphone. There was a possibility of the hospital reporting system incompletely capturing patients. Also, a risk of classification bias was present with the interview process. Finally, there may be other transition reasons, which were unable to be captured in this analysis. Our analysis also does not evaluate patients who were initiated on hydromorphone in the place of fentanyl, such as during the time of drug shortages.
Conclusion
Our analysis found the most common rationale for the transition from fentanyl to hydromorphone was to improve patient ventilator compliance, to reduce overall sedative requirements, and to optimize pharmacokinetics and pharmacodynamics in particular critically ill patients. Hydromorphone may be associated with a reduction in overall sedative requirements without negatively impacting the success rate of SBT or overall level of sedation when compared to fentanyl. A prospective, head-to-head study is warranted to explore possible benefits or differences in outcomes associated with hydromorphone compared to other continuous infusion opioids.
Supplemental Material
Supplemental Material, Interview_Template_supplemental - Transition From Continuous Infusion Fentanyl to Hydromorphone in Critically Ill Patients
Supplemental Material, Interview_Template_supplemental for Transition From Continuous Infusion Fentanyl to Hydromorphone in Critically Ill Patients by Mary P. Kovacevic, Paul M. Szumita, Kevin M. Dube and Jeremy R. DeGrado in Journal of Pharmacy Practice
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.