
Abstract
Purpose
To review the effects of statin use in patients at risk for or diagnosed with Clostridium difficile infection (CDI) on CDI incidence, treatment success, and mortality.
Methods
A literature search was performed through January 2019 using the following terms: statins, HMG-CoA inhibitors, Clostridium difficile, Clostridium difficile associated diarrhea, and Clostridium difficile infection. Additional references were identified from a review of literature citations. Studies evaluating statin effects on C difficile-related outcomes were included.
Results
A total of 8 studies were identified for inclusion in this review. All studies were retrospective. Five studies reported the association between statin use and the development of CDI, suggesting that statins may decrease risk of CDI development in patients already on statin. In one study, there was an improved treatment response against CDI with the use of statin. Three retrospective studies evaluated statin use and mortality from CDI and only one study found significant mortality benefit in statin users.
Conclusions
Statin use may have a protective effect against the development of CDI and improve CDI treatment success; however, it is unclear if use confers a mortality benefit. Current data remain sparse and larger, prospective studies are needed to confirm current results and identify the specific population that may benefit the most from this intervention.
Introduction
Clostridium difficile, a gram-positive, spore-forming, anaerobic bacterium, is one of the leading causes of hospital-acquired illness in the United States with a financial burden estimated at US$6.3 billion annually. 1,2 A surveillance study from 2011 identified approximately 453 000 cases in the United States, with an estimated 83 000 cases of infection recurrence and 29 300 C difficile-related deaths occurring during the year-long study. 3 Additionally, the case fatality rates due to C difficile infections (CDI) have increased from 1.5% to 16.7% during epidemic periods. 4 The clinical presentation of CDI primarily includes diarrhea but may range from symptomless carriage, as is seen in healthy infants, to serious complications such as pseudomembranous colitis and toxic megacolon. C difficile causes disease through the release of exotoxins that cause colitis in susceptible patients. 5,6 While the complete mode of action of these exotoxins is not yet fully elucidated, it is suggested that they may lead to complete inactivation of Rho guanosine triphosphates (GTPases) pathways, which may have downstream immunomodulatory effects. 7 -9 Studies of CDI have identified multiple factors associated with increased risk of infection, including advanced age, duration of hospitalization, exposure to chemotherapy, gastrointestinal surgery, prior antimicrobial use, and use of gastric acid suppressing agents. 10 -19 Systematic CDI prevention has largely focused on infection control and antibiotic stewardship. 20,21 Additional prevention options for CDI include probiotics, tetracyclines, and, more recently, potentially statins. 22,23
Inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA), more commonly known as statins, are a class of drug indicated for the treatment of dyslipidemia and prevention of atherosclerosis. Statins are increasingly prescribed in the United States, with the percentage of statin users in patients over 40 years old rising from 17.9% in 2002 to 27.8% in 2012. 24 In addition to their cholesterol-lowering effects, statins also exhibit anti-inflammatory, immunomodulatory, and other pleiotropic effects. 25 -27 The significance of these secondary effects have been studied in a variety of disease states, including sepsis, pneumonia, and bacteremia. 28 -30 In short, the pleiotropic effects of statins may also inhibit Rho GTPase pathways leading to immunomodulatory effects that may affect CDI-related outcomes. 31
The burden of disease C difficile places on the health-care system, coupled with plausible mechanisms for statin benefits, has led to several studies investigating the link between the two. We have conducted a systematic review of published studies of statin use to summarize available information and facilitate a better understanding of the possible associations and benefits that statins may play in CDI.
Methods
An English-language MEDLINE search was conducted from 1964 through January 2019 using the following terms: statins, HMG-CoA inhibitors, Clostridium difficile, Clostridium difficile associated diarrhea, and Clostridium difficile infection. Results were limited to clinical studies evaluating statin effects on CDI-related outcomes, such as effect on CDI development, severity, treatment success, and so on. Studies that failed to report CDI-related outcomes were excluded. References of relevant articles were reviewed for qualifying studies. Articles identified were evaluated for study inclusion by at least 2 reviewers to eliminate the possibility of selection bias. Additionally, references from published articles were reviewed for citations for study inclusion. Figure 1 highlights the inclusion and exclusion of literature.
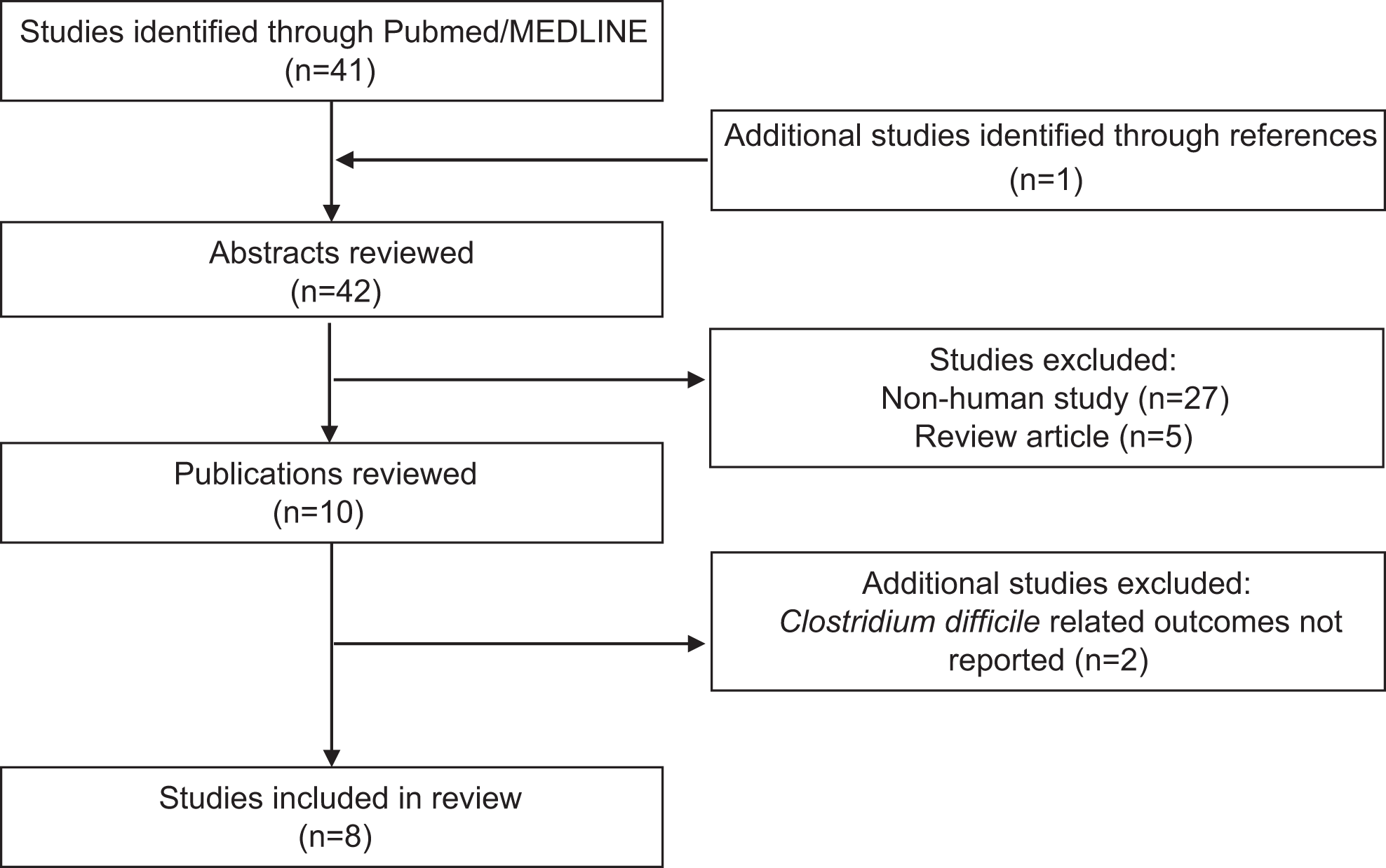
Flowchart of study inclusion.
Results
A total of 8 studies were identified for inclusion in this review. All studies were retrospective in nature and a summary of results can be found in Table 1. 32 -38
Studies Evaluating Clostridium difficile-Related Outcomes Related to Statin Use.
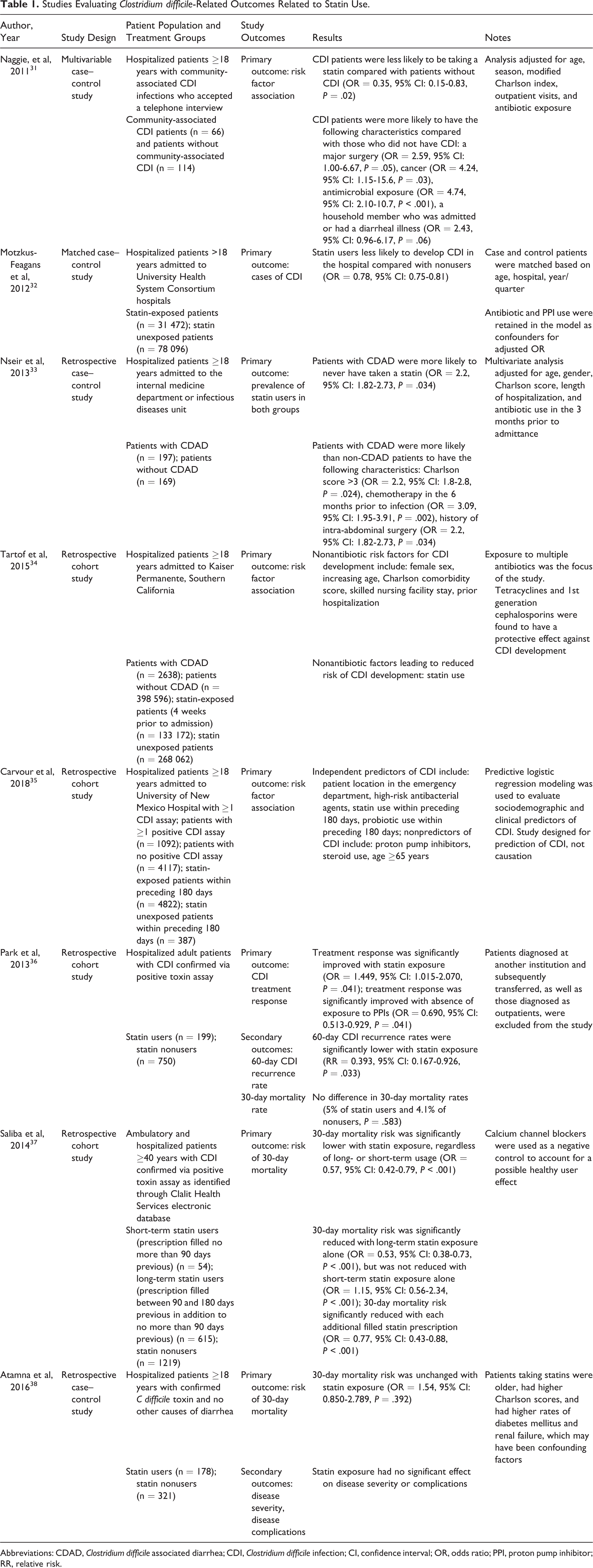
Abbreviations: CDAD, Clostridium difficile associated diarrhea; CDI, Clostridium difficile infection; CI, confidence interval; OR, odds ratio; PPI, proton pump inhibitor; RR, relative risk.
Effect on CDI Development
A 2011 case–control study published by Naggie et al of 180 patients from 5 medical centers and affiliated clinics in the United States sought to identify novel risk factors for the development of community-associated CDI (CA-CDI). 32 Patients were included if they had a diagnosis of CDI based on symptomatic diarrhea with no other etiology and a positive C difficile toxin assay. Symptom onset occurred in the community or within 72 hours of admission to a health-care facility to be considered CA-CDI. The controls were recruited in a 2:1 ratio and were geographically matched to cases. Significant risk factors for the development of CA-CDI were bowel surgery, antimicrobial use, and exposure to a household member admitted to a health-care facility or with recent diarrheal illness. Statin use was found to have a protective effect against the development of CA-CDI, while proton pump inhibitors (PPIs) showed no significant harmful effect to patients.
Another case–control study by Motzkus-Feagans et al published in 2012 evaluated the association between statins and other cholesterol-lowering drugs and the development of health-care facility-onset CDI (HCF-CDI) in patients admitted to US academic medical centers. 33 Patients admitted to the hospital with a primary International Classification of Disease, version 9, Clinical Modification code for CDI and who received at least 3 days of CDI treatment initiated on or after the fifth day of admission were included in the study as cases, while controls were patients with at least 8 days of hospital stay who did not have a diagnosis of CDI. Cases were matched 5:1 to controls based on age, hospital, and quarter/year of admission. Statin exposure was defined as the administration of atorvastatin, fluvastatin, lovastatin, or pravastatin prior to the index date which was defined as postadmission date of CDI diagnosis in cases or postadmission day 5 in controls. Between the 2 groups, an estimated 20% of patients used statins, with atorvastatin and simvastatin being the most commonly used medication. Overall, there was a protective effect found with the use of statins against the development of HCF-CDI. Subgroup analysis showed this protective effect persists regardless of the statin used. This protective effect was not seen in patients who only received nonstatin cholesterol-lowering agents, and instead, an increased risk of infection was seen in patients who received resins. However, it should be noted that a minority of patients received these medications (0.36%).
A similar retrospective case–control study by Nseir et al evaluated the risk of CDI in hospitalized patients in Israel between those who were and who were not taking statins. 34 All consecutive patients diagnosed with CDI over a 1-year timespan were included. Cases of CDI were defined as diarrhea (3 or more unformed stools per day for the past 2 days) not attributed to any other cause and positive CDI test (endoscopy revealing pseudomembranes or stool enzyme immunoassay [EIA] for C difficile toxins). Cases were matched to controls based on age, gender, comorbidity, length of hospitalization, and antibiotic use. Cases differed from controls in terms of statin, PPI, chemotherapy, and nasogastric tube use as well as history of intra-abdominal surgery. A total of 366 patients were included, 197 diagnosed with CDI and 166 served as controls. Multivariate analysis revealed that the absence of statin use increased the risk of CDI. Similar to the study by Naggie et al, there was no significant effect seen with the use of PPIs.
In 2015, Tartof et al published a study on a comprehensive assessment of factors associated with hospital-associated CDI. 35 They conducted a retrospective cohort study of adult Kaiser Permanente Southern California members with a hospital admission between January 2011 and December 2012. Cases were defined as patients with positive polymerase chain reaction (PCR) assay results 72 hours following hospital admission. A total of 401 234 patients were included, with 2638 (0.7%) patients testing positive for CDI. Crude analysis found a higher incidence of CDI in patients with statin exposure. However, a multivariate Poisson regression model demonstrated a lower risk of CDI among statin users.
The most recent of these studies was published in 2018 by Carvour et al. 36 This study was a retrospective cohort study of patients over the age of 18 who were admitted to the University of New Mexico Hospital with CDI between May 2011 and August 2016. This study sought to determine predictors of CDI development among hospitalized patients. Patients with any type of CDI assay, including EIA or nucleic acid amplification/PCR, were included to serve as cases (positive assay result) or controls (negative assay result). A multivariate analysis identified multiple independent predictors for CDI development, including statin use. There was not a predictive association of CDI with PPI or steroid use or in those 65 years or older.
Effect on Treatment Success
A Korean retrospective cohort study of 949 patients by Park et al evaluated characteristics of treatment success among hospitalized CDI-positive patients. 37 Patients were included if they had a positive diagnosis for CDI and no prior episode of CDI. Statin users were defined as patients with use of a statin prior to the study index date. If statin therapy was initiated in a patient within 12 weeks of the index date, they were excluded. Overall, there were several differences in baseline characteristics between statin users and nonusers including that statin users were significantly younger (62.5 ± 16.1 years vs 65.9 ± 14.2 years), had a lower Charlson score (2.9 ± 1.7 vs 3.2 ± 1.8), and less had exposure to PPIs (29.2% vs 52.8%). The primary outcome of successful treatment response, defined as symptom resolution within 6 days of treatment, was significantly associated with exposure to statins. Other characteristics which were significantly associated with treatment response included absence of a nasogastric tube, higher serum albumin levels, lower serum creatinine levels, lower severity scores, and absence of exposure to PPIs. Recurrence rates of CDI at 60 days were significantly lower in statin nonusers.
Effect on Mortality
CDI is not only a major cause of morbidity, but also mortality, with high mortality rates due to CDI on the rise. Three studies identified evaluated mortality end points. Saliba et al conducted a retrospective cohort study of 1888 Israeli patients positive for CDI to evaluate the effect of statin use on risk of 30-day all-cause mortality. 38 All study subjects with CDI were included and evaluated for statin use, defined as current users (further stratified by short-term use within 90 days only and long-term use over the course of 180 days) or nonusers. A centralized electronic database which included prescription information was utilized. Notable baseline characteristics that differed included that higher percentages of statin users also used PPIs or antibiotics within the previous 90 days. Overall, 18% (n = 340) of patients in the cohort died within 30 days of CDI diagnosis. Of statin users, 13.3% died compared with 20.6% of nonusers, resulting in a 43% decreased risk of 30-day mortality with statin use as revealed by multivariate analysis.
Atamna et al also investigated the impact of statin use on mortality in a retrospective, case–control study of 499 hospitalized patients with CDI in Israel. 39 All patients who tested positive for C difficile via toxin testing were included and categorized into either statin users or nonusers. Overall, 36% of patients were statin users. Statin users had significantly higher Charlson scores, were older, and were more likely to have diabetes. Regarding the primary end point of 30-day all-cause mortality, there was no significant difference between statin users and nonusers by univariate analysis, or by multivariate analysis. When patients were evaluated for factors predicting CDI severity, statins had no effect with the exception of an association with higher serum creatinine levels. Statins also had no impact on CDI complications or transfers to the intensive care unit.
The study by Park et al as described above evaluated statin effects on mortality as a secondary end point. 37 There was no significant difference in all-cause mortality within 30 days of CDI diagnosis between statin users and nonusers. In addition, there was no significant difference in severe complications of CDI between groups.
Discussion
Although many risks for the development of CDI have been identified, there is sparse data on pharmacologic protective factors that may decrease the development and severity of this infection. Statins, with their multitude of uses, relative tolerability, and pleotropic effects, provide an attractive option for adjunctive treatment and prevention of CDI. The current body of evidence has identified protective effects (potential reduction in incidence, improved treatment success, improved mortality); however, there is a wide range of heterogeneity between the retrospective trials identified and discussed.
A growing body of evidence exists supporting statin use for various mechanisms outside of cholesterol-lowering activity, including for the prevention and treatment of infections via anti-inflammatory and immunomodulatory properties. 25 -31,40,41 One such mechanism is through statin-induced inhibition of isoprenylation of Rho GTPase proteins. The Rho pathway acts as a signaling switch for downstream cell cycle changes and can affect the functions of endothelial, vascular smooth muscle, inflammatory cells, and platelets. 42,43 In patients with sepsis, statins have been associated with less marked elevation of inflammatory markers, leading to decreased cellular injury. 40–41 It is reasonable to consider that these statin effects might also provide protective benefits for patients with CDI. Statins can reduce cytokine production and decrease the ability of neutrophils to sense and migrate toward areas of inflammation, both of which could reduce CDI disease severity. 44,45 Paradoxically, Rho inhibition decreases the inflammatory effects caused by CDI; however, presence of C difficile toxins may also stimulate cytokine-induced inflammation as part of the immune process. 7 -9 Since C difficile toxins and statins both affect Rho GTPase proteins, among others, there might also be unspecified interactions that may affect the toxigenic effects of CDI.
One retrospective study found statins had a protective effect in patients with severe sepsis, which led to a reduction in mortality when compared to patients not receiving statins. 28 However, in a post hoc analysis of the study, they found an increased rate of CDI in statin users (n = 12/19) versus nonstatin users (n = 7/19). 46 Inhibition of the Rho pathway may lead to negative cell cycle effects including cell apoptosis based on cell type affected, presence of other protein modulators, intensity of inhibition, and varying pathways of inhibition. 42,43 Specific statins, such as simvastatin, may also potentiate the cytotoxic effect of C difficile toxins by inhibiting CD40-mediated immunologic functions. 47 This is a potential explanation for the reported increased incidence of CDI in statin users; however, this was an incidental finding in a relatively small retrospective cohort study and was contradicted by a number of studies since. The most recent study included in this review by Carvour et al suggests similar results. 36 As mentioned above, the interaction of statins and C difficile toxins within the Rho pathway remains uncertain.
Although mechanisms tying statins to CDI protective effects are plausible and suggest statin benefits, the existing data reviewed are limited by its retrospective nature and wide array of outcomes. Multiple studies showed statins have several protective effects in reducing development of CDI; however, there are several aspects of the trials to consider. Regarding impact on CA-CDI development, the study by Naggie et al included only CDI occurring early in patients’ hospitalizations and excluded patients with risk factors for health-care facility-associated disease. This study, therefore, was able to minimize confounding effects of hospitalization duration and other associated risks. 32 In addition, they were able to identify patients who received antimicrobials in the past 90 days, allowing them to adjust for antimicrobial effects on CDI development rates. In terms of disease severity, there were no reported complications of CDI such as colectomy or death in the patients included in the study. The small sample size of the study, along with the relatively low disease severity of patients included, may have masked potentially significant risk factors. In addition, because the study was conducted in an outpatient setting and relied on patient interviews, it is difficult to assess and ascertain patient adherence to the medications of interest. In contrast, Motzkus-Feagans et al sought to answer the same question but in terms of HCF-CDI using billing information. 33 They, too, found that all statins were associated with a decreased development of CDI. However, the lack of patient-level data could have confounded the results. Since only instances of medication use were tracked, instead of doses and administration information, continuity of statin administration could not be assessed. No patient-level data were analyzed for this study, and thus, prior to admission, medications could not be evaluated. This study, along with the previous trial, was not able to assess whether timing of statin administration may impact effects. Nseir et al also found a protective effect with statin use in hospitalized patients with CDI. 34 However, this multicenter study was conducted in Israel and it is hard to ascertain whether diagnostic, infection control, and treatment procedures are generalizable to practices in the United States.
In contrast to the above trials, Carvour et al found that statin use may be a predictor for CDI development among hospitalized patients in New Mexico. 36 This study found that probiotic use was associated with CDI development, also contrasting with data from prior studies. 22 Although multivariate regression was used, other confounders may include statin use as a measure of patients more likely to utilize the health-care system or to present to the hospital with symptoms. Finally, this study only identified predictors, not causality based on its observational nature.
Trials associating statins with improved treatment success and reductions in mortality also have factors to consider. In the study by Park et al, improvements in treatment success in patients exposed to statins were limited by large differences in baseline characteristic between statin users and nonusers. 37 This may have led to statin users being slightly healthier or lower risk. This study also evaluated and discovered many other factors which were associated with successful treatment response, in addition to solely statin use. Finally, like many of the studies discussed, there was no way to evaluate statin adherence given the retrospective nature. Regarding mortality data, Park et al, Saliba et al, and Atamna et al investigated outcomes including risk of all-cause mortality at 30 days. 37 -39 In these trials, cause of death was not available, making interpretation of CDI outcomes difficult to deduce as there was no indication whether mortality was due to CDI or complication, cardiovascular mortality, or another cause. In these trials, statin type and adherence was also difficult to determine. Interestingly, one trial further stratified statin use by short- or long-term use and found that statin use greater than 90 days conferred mortality benefit, suggesting a potential mechanism requiring long-term use. 38 Of note, similar to other trials, mortality trials were also limited by differences in baseline characteristics possibly confounding results.
Another consideration is that identification of cases differed between the mentioned studies evaluating statins and CDI-related outcomes. The study by Motzkus-Feagans used billing information to identify cases, while the studies by Naggie and Nseir used toxin EIA for case identification. 32 -34 Diagnosis via EIA have been shown to have substantially reduced sensitivities when compared to other assays. 48 It is, however, important to note that the studies by Naggie and Nseir used EIAs to test for exotoxins, which minimizes the risk of missing patients infected with a pathogenic strain of C difficile producing only toxin B. 32,34 Carvour used both EIA and PCR but did not specify any assay specifics. 36 The study by Tartof et al used a PCR assay detecting the toxin B gene alone. 35 Diagnostic testing for CDI using PCR assays have lower specificity than sequential testing, which may lead to an inflated infection rate as asymptomatic cases are mistakenly included in the analysis. 49 Park et al, on the other hand, conducted chart reviews for any positive C difficile toxin (A or B), C difficile cultures, or pseudomembranous colitis on imaging, possibly including patients without a true CDI. 37 Finally, studies by Saliba and Atamna utilized the 2-step approach of glutamate dehydrogenase and toxin A/B EIA testing followed by a PCR assay for the toxin B gene if initial results contained discrepancies, as now recommended by the European Society of Clinical Microbiology and Infectious Disease for CDI diagnosis. 38,39,50 This strategy limits the chance of false-positive results while quickly ruling out CDI if initial testing is negative.
When interpreting this statin data, a question remains as to the impact the statin regimen may play. It is difficult to assess how dose, statin selection, or changes in regimen might affect CDI development and outcomes as studies only stratified patients as statin users or nonusers. Thus, studies only evaluated various statins at unreported doses. Additionally, the studies included in this review cannot account for the environmental risks of CDI infections. The role of infection control and surveillance plays a large part in risk and development of contagious diseases such as CDI, especially when considering non-community-acquired subtypes. Facilities and hospitals have a wide array of sanitation and quarantine protocols that might impact patients staying in spaces with prior CDI contact.
Globally, presented statin data in the setting of CDI were analyzed in a meta-analysis which found statin use may be associated with a 20% risk reduction of CDI. 51 As discussed above, available evidence has a high level of heterogeneity and must be interpreted with caution. Statin use, in general, has risen in the past several years and may continue to do so with aging populations. 24 Guidelines on the use of statins for primary and secondary reduction of cardiovascular risk affect the number of patients treated with statins and may change the landscape of statin use as updates are made. 52 Regarding statin use in the setting of CDI, presently, no randomized controlled trials have been identified evaluating statins for prevention or treatment. From a practical standpoint, the development of such a trial evaluating statin effects on CDI would be difficult and possibly unethical (ie withholding statins from patients who may benefit from treatment for cardiovascular risk for the sake of a control group) to design. Large cohort studies will likely to provide the best evidence for statins as protective agents against CDI. Conversely, prospective randomized controlled trials are warranted to address deficiencies in the current literature and provide evidence that statins improve treatment response or mortality in patients who have developed CDI, as current retrospective studies provide encouraging results.
Conclusions
The protective mechanism of statins in CDI is a novel concept; to date, no prospective trials evaluating statin effects in the setting of CDI exist. Although there remains a paucity of data, we have presented preliminary evidence reviewing the impact of statins on CDI development, treatment success, and mortality, which suggest some benefit to statin use in terms of CDI development and treatment success. Overall, statins may provide benefit in reducing the risk of both CA-CDI and HCF-CDI development, improve treatment response, and decrease recurrence rates. Effects on mortality remain unclear. Currently, no evidence supports initiating a statin in statin-naive patients who develop CDI or in patients at high risk of developing CDI, but statins may prove to be an attractive adjunctive treatment in addition to standard therapy. Larger, prospective studies are needed to confirm current results and identify the specific population that may benefit the most from this intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.