
Abstract
Methadone is frequently used to prevent withdrawal symptoms secondary to intended therapeutic opiate exposure. Absence of a standardized dose weaning strategy potentially results in increased exposure to narcotics and/or withdrawal symptoms. We sought to quantify the effect of implementing a standardized methadone weaning protocol and withdrawal assessment tool on methadone exposure and opiate withdrawal in pediatric patients receiving 5 or more days of continuous morphine or fentanyl infusions. The preintervention phase included patients weaned off of opiate infusions before implementation of a standardized weaning protocol and withdrawal symptom scoring tool. Patients in the postintervention phase were started on a standardized methadone wean based on total duration and dose of continuous opiate infusion exposure in the 24 hours preceding methadone initiation. Patients received either a 5- or 10-day wean, with the total daily methadone dose reduced by 20% daily or every other day, respectively. Patients in the postintervention phase were monitored for withdrawal using the withdrawal assessment tool (WAT-1). Postintervention patients were compared to preintervention patients treated with methadone. Total methadone duration decreased significantly from a median of 17 (13-22 interquartile range [IQR]) to 5 (5-10 IQR) days (P = .00001) after implementation of the methadone weaning protocol. Number of morphine boluses administered increased from a median of 3 (0-6 IQR) to 4 (0-5 IQR) doses per patient (P = .45). Demographic data were similar between both groups. Patients in the postintervention phase had significant reductions in methadone exposure after implementation of a standardized methadone weaning protocol and assessment tool.
Introduction
Pediatric patients in the intensive care unit often require administration of intravenous opiate infusions for pain management and as an adjunct for sedation. Adequate pain control reduces stress and has been shown to decrease recovery time in critically ill patients but carries the risk of developing physical dependence. 1 Abrupt discontinuation of a fentanyl infusion when used for more than 5 days or at a total cumulative dose greater than 1.5 mg/kg has been associated with a 57% incidence of developing withdrawal. Incidence of withdrawal approaches 100% after greater than 9 days of exposure. 2-3 Withdrawal symptoms include neurologic, autonomic, and gastrointestinal dysfunction potentially causing increased morbidity and length of stay in the pediatric intensive care unit (PICU). Prevention of withdrawal is achieved by weaning the opiate slowly over time. Methadone is an ideal choice for weaning due to its long half-life, high oral bioavailability (85%) allowing for 1:1 intravenous to oral dose conversions, and lack of euphoria. 4,5
The use of methadone for opiate weaning in pediatric patients (less than 18 years of age) has been reported in the literature, but there is wide variability and lack of standardized weaning strategies. 6 -11 The equipotent dose conversion from morphine or fentanyl continuous infusions to intermittent methadone can be challenging in pediatric patients due to opiate cross-tolerance and pharmacokinetic differences across age ranges. The optimal weaning duration has varied as well, ranging from days to weeks. 6 -11 Assessment of iatrogenic withdrawal in pediatric patients has also proven difficult with variable strategies reported in the literature and a lack of an accepted standard. Further complicating withdrawal assessment is the concomitant use of other sedatives, including benzodiazepines and alpha-2 agonists, which can also cause withdrawal symptoms after their discontinuation.
Methadone is frequently used to prevent withdrawal symptoms secondary to intended therapeutic opiate exposure. Absence of a standardized dose weaning strategy potentially results in increased exposure to narcotics and/or withdrawal symptoms. Also, assessing the effectiveness of any weaning strategy is difficult without a standardized approach to withdrawal assessment.
An evidence-based methadone wean protocol was then utilized to delineate dosing and treatment duration and a validated withdrawal symptom scoring tool implemented to standardize assessment. The objective of this study was to compare the duration of methadone exposure and the incidence of withdrawal symptoms pre- and postprotocol implementation.
Materials and Methods
This single-center, retrospective cohort quality analysis compared patients before and after protocol implementation. Electronic health records were used to identify patients under 18 years of age who were prescribed methadone. Patients included in the study received continuous morphine or fentanyl infusions in the PICU for 5 days or more prior to the methadone wean. Patients were excluded if they were born at less than 36 weeks gestational age, experienced an acute central nervous system injury, had an overlap of methadone and continuous morphine or fentanyl infusion greater than 48 hours, discontinued methadone prior to completing the wean (ie, patient transfer to another facility, allergy, or side effect), or did not adhere to the methadone wean protocol in the postintervention phase. The institutional review board reviewed this quality improvement project and granted a waiver for informed consent.
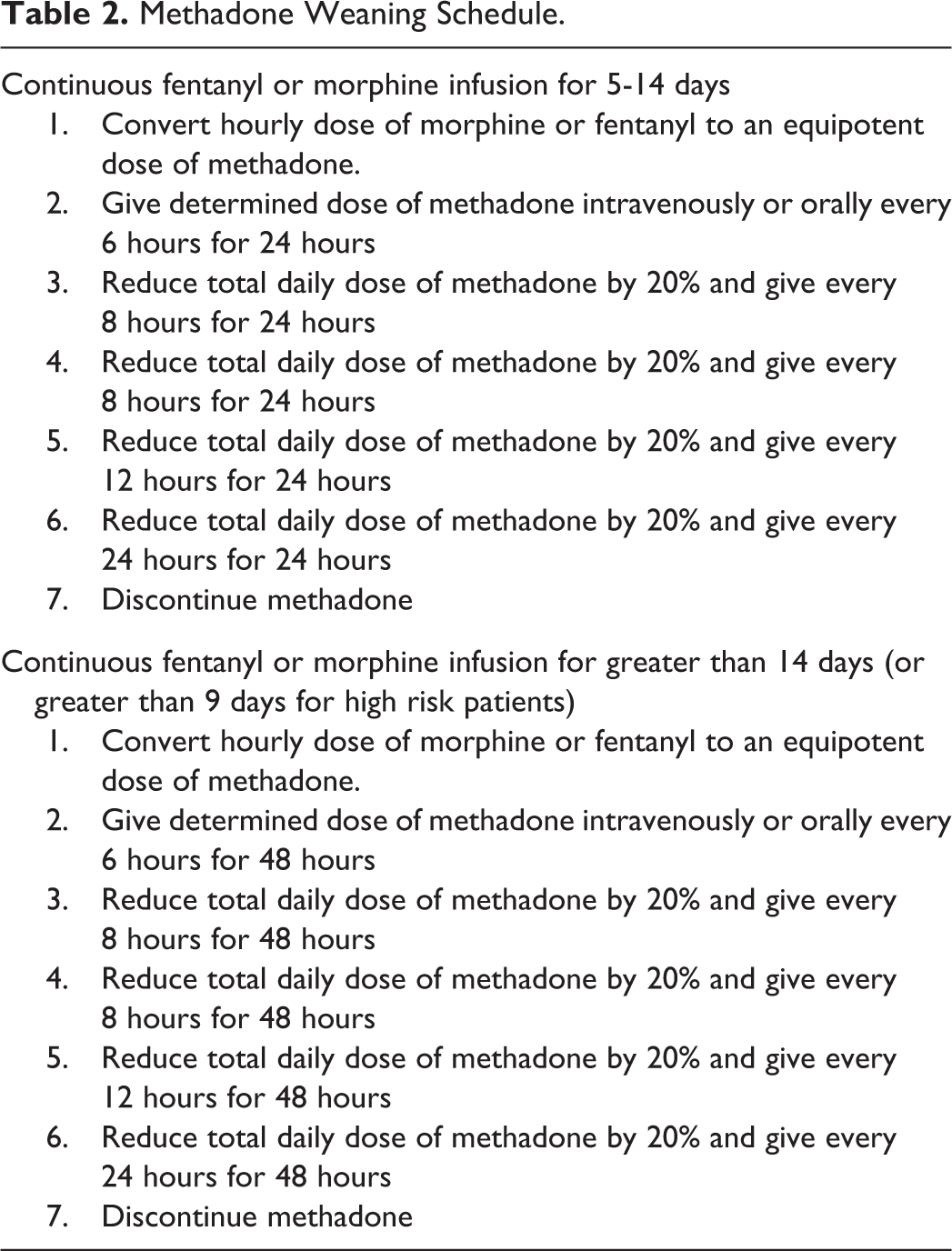
Patients in the preintervention phase were weaned off of methadone on a case-by-case basis, with dose adjustments made at the discretion of the critical care physician. Patients in the postintervention phase were started on the standardized methadone opiate weaning protocol. The protocol was based on previous weaning strategies reported in the literature by Robertson et al. 9 The initial methadone dose in mg/kg was calculated based on the average hourly dose of the continuous opiate infusion over the previous 24 hours (Table 1). Morphine infusions were converted and rounded to either a 0.05 mg/kg or 0.1 mg/kg dose of methadone in order to simplify order entry in the electronic health record (EHR). This daily dose was administered orally or intravenously based on the patient’s status every 6 hours for the first 24 to 48 hours of the methadone taper, for patients receiving a 5-day and 10-day wean, respectively. The continuous opiate infusion the patient was receiving was reduced by 50% after the third dose of methadone and then discontinued after the fourth dose. Patients who had been exposed to continuous opiate infusions for 5 to 14 days received a 5-day wean, and patients exposed greater than 14 days received a 10-day wean. High-risk patients, defined as patients with hemodynamically significant congenital heart disease or previously failing a methadone taper, were weaned over 10 days if the patient was exposed for greater than 9 days (Table 2). The protocol was then incorporated into an order set in the EHR to promote compliance and facilitate implementation.
Initial Methadone Dose Calculation.a
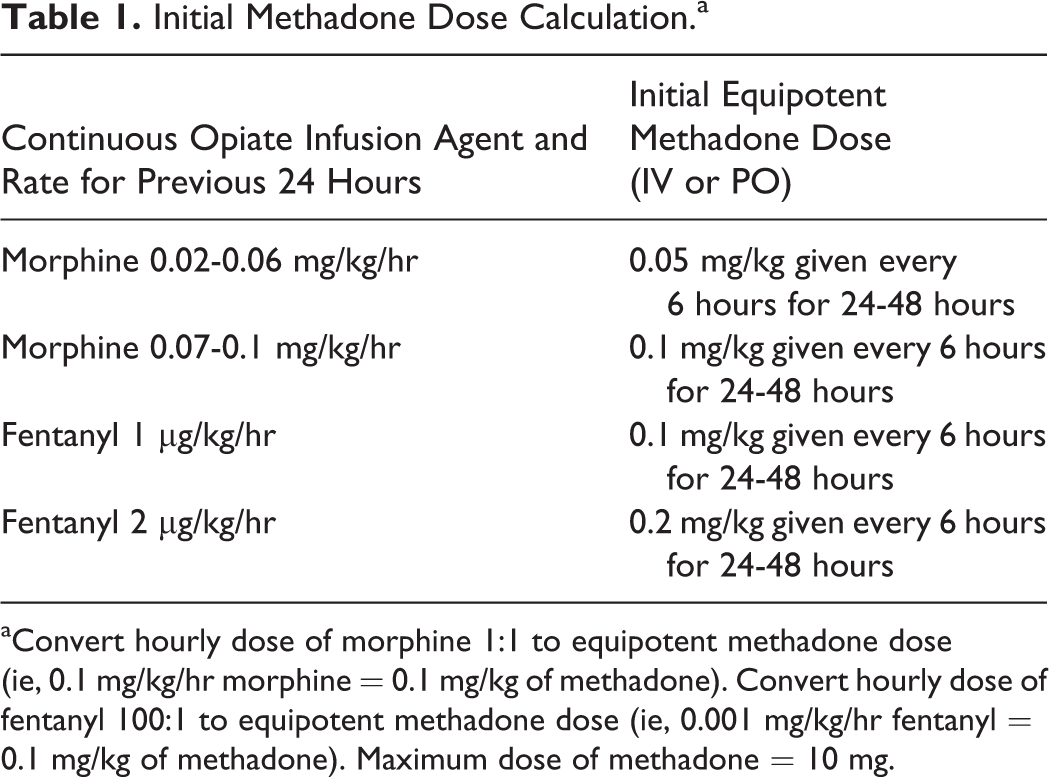
aConvert hourly dose of morphine 1:1 to equipotent methadone dose (ie, 0.1 mg/kg/hr morphine = 0.1 mg/kg of methadone). Convert hourly dose of fentanyl 100:1 to equipotent methadone dose (ie, 0.001 mg/kg/hr fentanyl = 0.1 mg/kg of methadone). Maximum dose of methadone = 10 mg.
Methadone Weaning Schedule.
Withdrawal in the postintervention phase was assessed using the withdrawal assessment tool (WAT-1). 12 Nurses utilized the tool to score patients’ symptoms once per shift (every 12 hours) during the weaning phase. 12 Scoring was initiated after the first decrease in opiate infusion rate and continued for 48 hours after completing the wean. Scores greater than or equal to 3 indicated clinically significant withdrawal. Intravenous morphine 0.05 mg/kg was available to manage symptoms of withdrawal; if administered, the patient was reassessed in 30 minutes, then once every hour for 2 hours. If the patient required more than 2 rescue doses of morphine in 24 hours, the protocol directed the nurse to contact the physician to revise the tapering schedule. The as-needed morphine order was available for 48 hours after the end of the wean. Nursing staff also monitored for oversedation and were instructed to hold the next methadone dose and contact the physician for further orders if identified.
The primary study outcome was to calculate the difference in duration of the methadone wean between the preintervention phase and the postintervention of the standardized methadone weaning protocol and withdrawal assessment tool. The secondary outcome measure was to compare the number of as-needed morphine bolus doses per patient for the management of withdrawal symptoms between the 2 groups; this was used as a surrogate marker of withdrawal due to the lack of the WAT-1 tool in the preintervention phase.
Additional outcomes measured included concomitant sedative administration, initial methadone dose, peak opiate infusion rate and duration, and PICU length of stay. Data collected included patient demographic data, peak fentanyl or morphine infusion rate (µg/kg/hr), duration of fentanyl or morphine infusion administration (days), WAT-1 scores, initial methadone doses, wean duration, boluses of morphine administered, and concomitant administration of dexmedetomidine or clonidine (alpha-2 agonists) and lorazepam during wean. Fisher exact tests were used for categorical data and the Mann-Whitney U test for continuous data. For all tests, P values < 0.05 were considered significant.
Results
One hundred two patients administered methadone and continuous infusions of morphine or fentanyl were reviewed, 50 in the preintervention phase and 52 in the postintervention phase. A total of 25 patients in the preintervention phase and 21 patients in the postintervention phase were included for analysis after applying exclusion criteria (Figure 1). Pre- and postintervention groups were similar with respect to age, gender, and admitting diagnoses (Table 3).
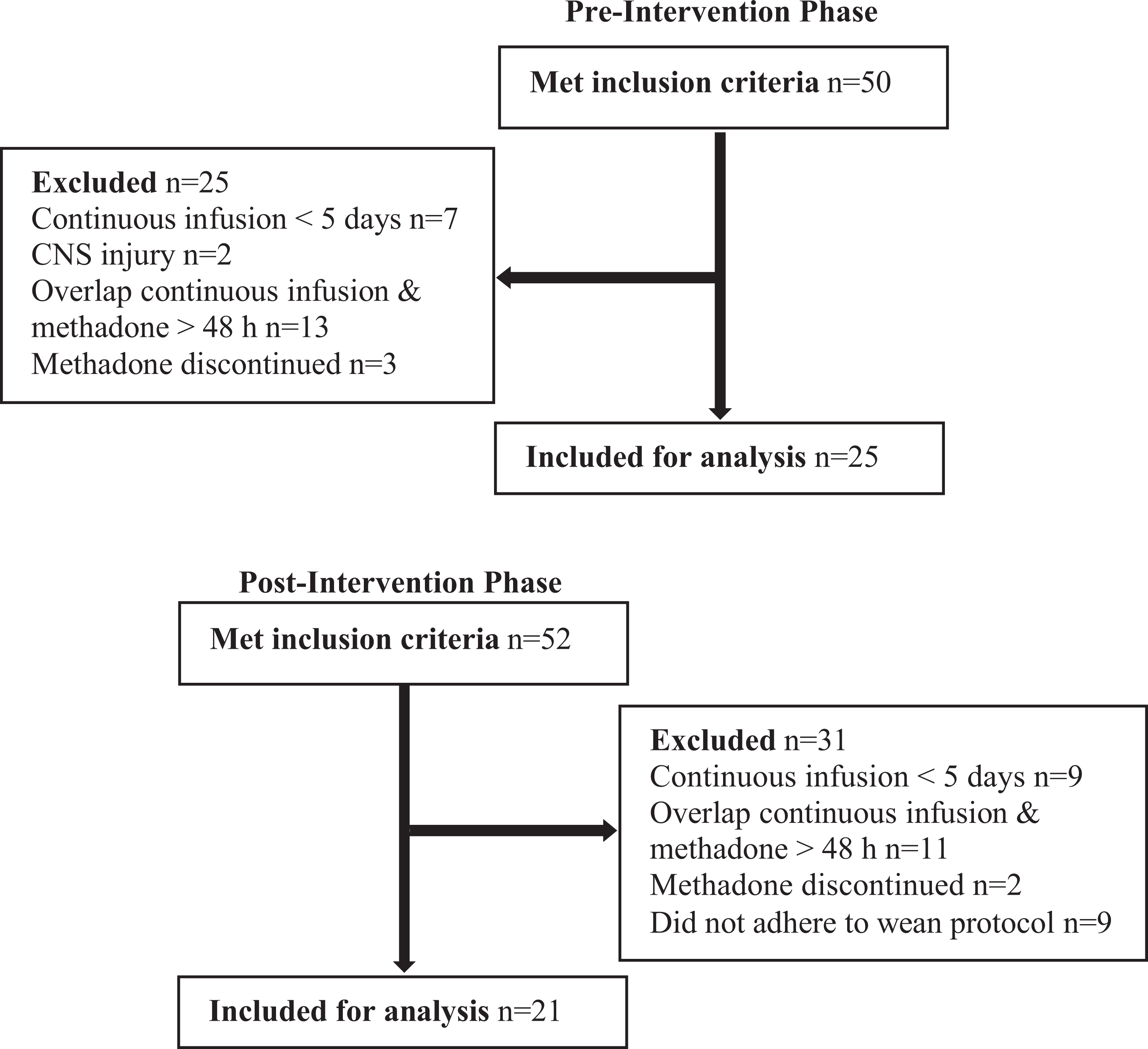
Patient enrollment.
Baseline Demographic Data.a
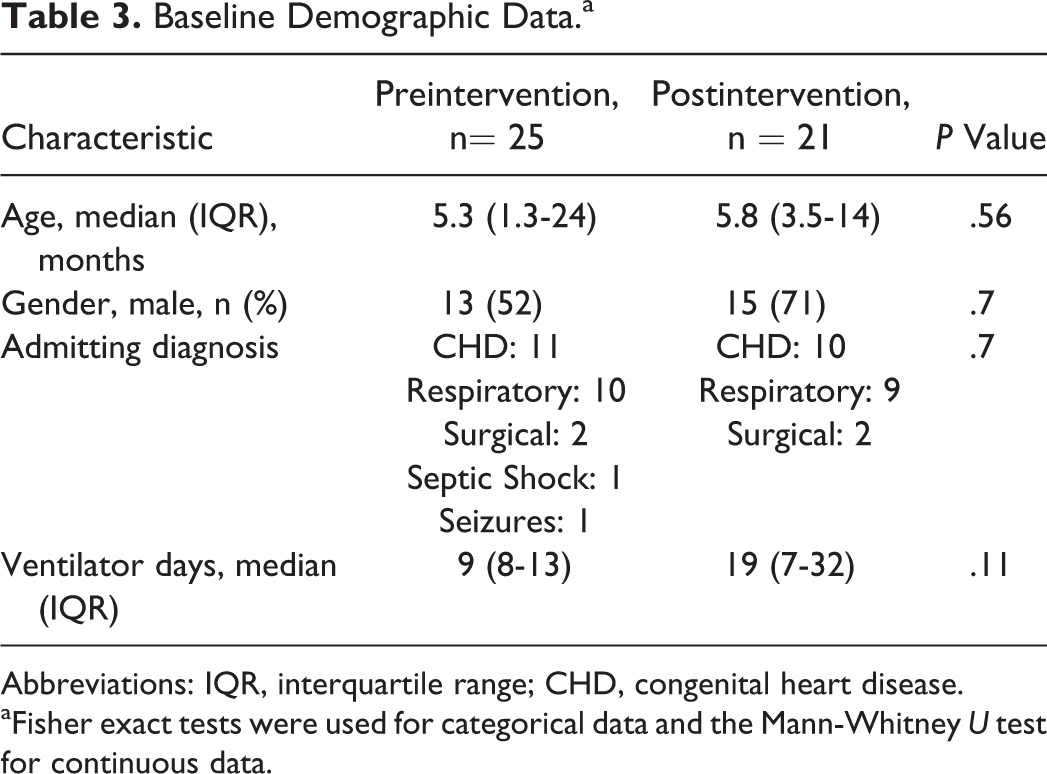
Abbreviations: IQR, interquartile range; CHD, congenital heart disease.
aFisher exact tests were used for categorical data and the Mann-Whitney U test for continuous data.
Total methadone exposure significantly decreased from a median of 17 (interquartile range [IQR] 13-22) to 5 (IQR 5-10) days (P = .00001) after implementation of the methadone weaning protocol and the WAT-1 scoring tool despite a longer opiate infusion duration and higher peak opiate infusion rate in the postintervention group. Number of morphine boluses administered increased from a median of 3 (IQR 0-6) to 4 (IQR 0-5 IQR) doses per patient (P = .45). Initial daily methadone dose increased from a median of 0.3 (IQR 0.2-0.4) mg/kg/day to 0.4 (IQR 0.2-0.4) mg/kg/day (P = .42; Table 4).
Methadone Exposure, Concomitant Sedatives, and PICU Length of Stay Pre- and Postintervention.
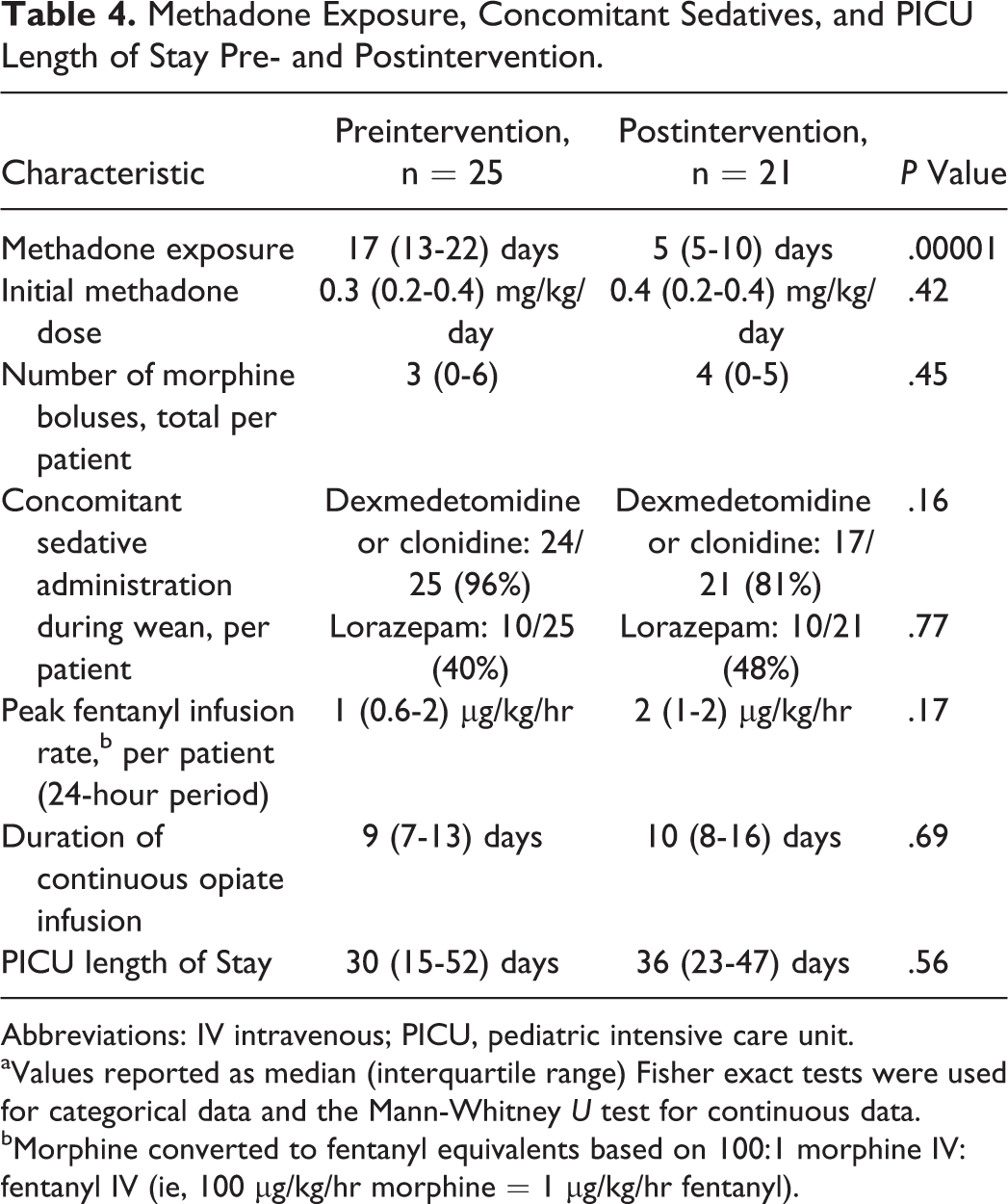
Abbreviations: IV intravenous; PICU, pediatric intensive care unit.
aValues reported as median (interquartile range) Fisher exact tests were used for categorical data and the Mann-Whitney U test for continuous data.
bMorphine converted to fentanyl equivalents based on 100:1 morphine IV: fentanyl IV (ie, 100 µg/kg/hr morphine = 1 µg/kg/hr fentanyl).
Concomitant sedative exposure and duration and PICU length of stay were similar in both groups (Table 4). Three weaning courses required revision due to excessive withdrawal symptoms postintervention. The percentage of patients experiencing withdrawal (WAT-1 scores ≥ 3) for the 5-day wean and 10-day wean are illustrated in Figure 2. WAT-1 scores were recorded for 48 hours after the completion of the wean.
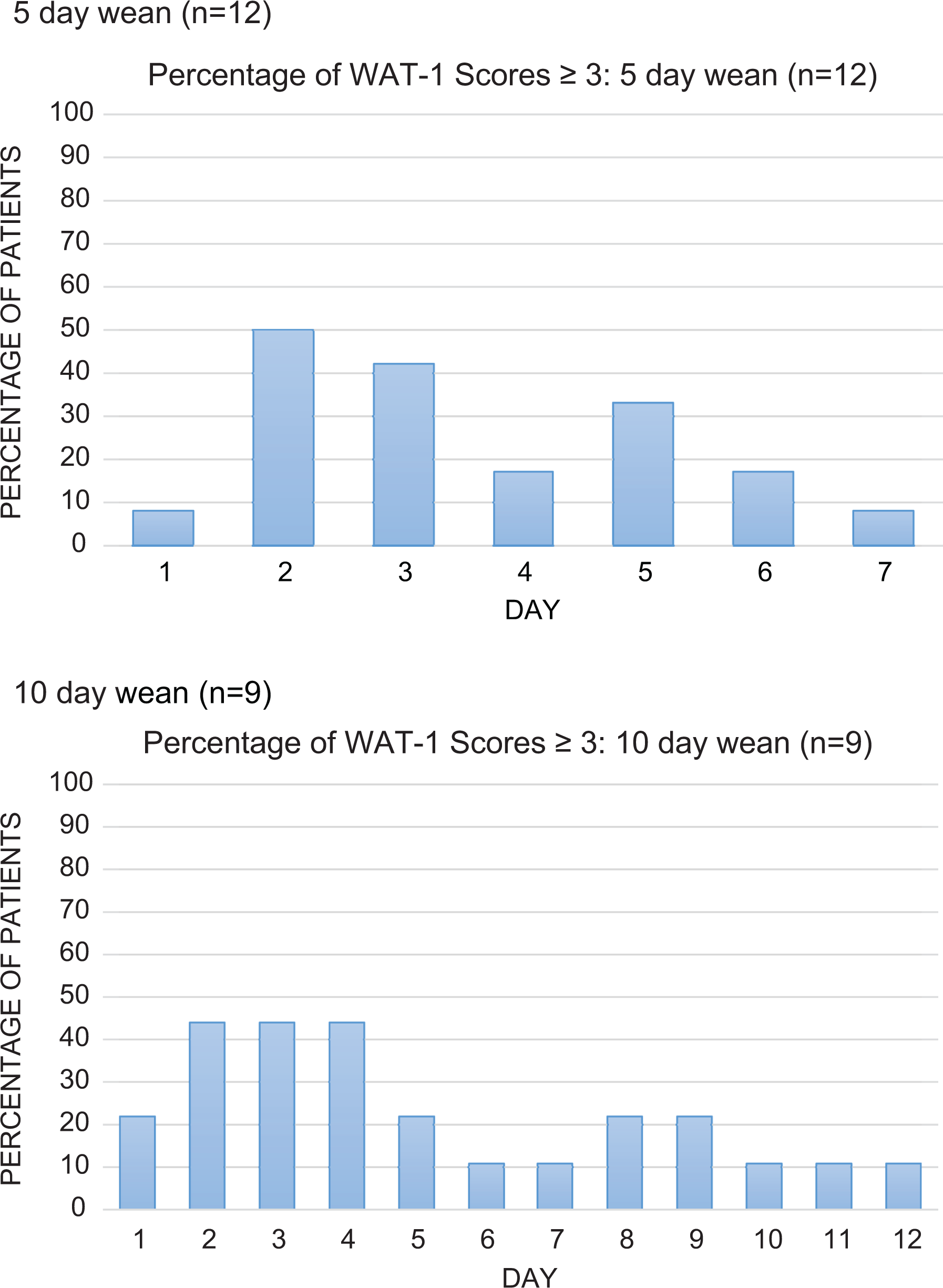
Percentage of withdrawal assessment tool (WAT-1) scores ≥3. Day 1 of wean = first day on methadone. WAT scores continued to be recorded for 48 hours after completion of the methadone wean. WAT scores ≥ 3 indicate clinically significant withdrawal.
Discussion
Implementation of the wean protocol standardized methadone dosing methodology for iatrogenic opiate withdrawal in pediatric patients at our institution. Total methadone exposure was significantly reduced in the postintervention phase although initial daily methadone doses were higher and opiate infusion duration prior to the methadone wean was longer in this group. The number of morphine boluses administered to each patient increased in the postintervention group, although these results were not statistically significant. This could be attributed to the increased peak opiate infusion dose and extended duration relative to the preintervention phase. Also, heightened awareness to withdrawal symptoms after receiving education on the WAT-1 tool and an “as-needed” order for morphine were only consistently present in the postintervention phase.
Previous studies have attempted to find the optimal weaning strategy for iatrogenic opiate withdrawal. Siddappa et al used 3 times the dose of fentanyl per day as equivalent methadone dose per day given in 3 divided doses then weaned by 3% to 10% daily depending on the dose and duration of fentanyl infusion. The authors found that 80% of their suggested methadone dose had the highest sensitivity and specificity in preventing withdrawal symptoms. 8 Berens et al compared a 5-day versus 10-day wean using 10 times the dose of fentanyl per day as equivalent methadone dose per day, resulting in no statistically significant difference in neonatal abstinence scores ( ) scores between the groups. 11 Bowens et al compared a fixed dose of methadone (0.1 mg/kg/dose given 4 times daily) versus using 10 times the dose of fentanyl per day as equivalent methadone dose per day weaned over 10 days, with no statistically significant differences in wean completion between the groups. 7 This study added that a standardized dosing approach using an order set incorporated into the EHR made a significant reduction in total methadone exposure. Abdouni et al reported similar results with regard to implementing a standardized methadone wean protocol, with reduced methadone exposure in the postintervention phase. 6 In addition, they were able to reduce the number of opiate boluses administered for withdrawal symptoms after protocol implementation. However, their study used a modified NAS scale for the duration of their study, whereas the present study implemented the WAT-1 scoring tool, which was specifically developed to detect iatrogenic withdrawal, in the postintervention phase only.
It is possible that methadone itself is not enough to prevent withdrawal due to incomplete cross-tolerance between opiates. 13 Opiate tolerance develops mainly as a result of downregulation of opiate receptors and increased cyclic adenosine monophosphate production. 14 These changes are caused by a variety of different mechanisms, including G-protein uncoupling, N-methyl-D-aspartate (NMDA) receptor activation, and protein kinase system activation. 15-16 Different opiates produce different effects on these systems, potentially contributing to cross-tolerance. Methadone as a weaning agent has the advantage over other opiates of attenuating the effect of NMDA receptor activation on opiate withdrawal. 17
Similar to opiate withdrawal, benzodiazepines and alpha-2 agonists are known to cause withdrawal symptoms when weaned. 13,18,19 Several patients in our study were exposed to and subsequently weaned off of 1 or both of these drug classes; this could have contributed toward additional symptoms of agitation and irritability, undistinguishable from opiate withdrawal symptoms. Patients administered prolonged infusions of midazolam were prescribed a lorazepam taper to prevent benzodiazepine withdrawal. Similar numbers of patients in both groups were exposed to both benzodiazepines and dexmedetomidine or clonidine (alpha-2 agonists) during the weaning period; therefore, the contribution of these medications to overall withdrawal events is uncertain.
The Finnegan scoring tool has been utilized to assess iatrogenic opiate withdrawal, although this tool was developed to assess neonatal abstinence syndrome. 10,13,20 Prior to the WAT-1 scoring tool, the Finnegan scoring tool was modified to better assess iatrogenic opiate withdrawal. 7 However, the WAT-1 is preferred and has been validated for monitoring opiate and benzodiazepine withdrawal symptoms in pediatric patients (2 weeks-18 years of age) with a reported high degree of sensitivity (0.872) and specificity (0.88). 12 Implementation of the WAT-1 scoring tool made recognition and management of withdrawal symptoms less subjective. Patients in the postintervention phase seemed to have increased withdrawal symptoms during day 2 to 3 of the methadone wean. This corresponds with the time that the continuous infusion was stopped (24 hours after the first dose of methadone), and the patient transitioned to scheduled methadone only (Figure 2). The incidence of withdrawal steadily decreased as the wean progressed, which may indicate that the initial methadone doses were insufficient to prevent withdrawal in our patient population or that the continuous opiate infusion should have been weaned over a longer period of time (ie, over 48 hours instead of 24 hours). This could also be attributed to concomitant sedative medications being weaned simultaneously or incomplete cross-tolerance between methadone and fentanyl and/or morphine.
There were several limitations to our study. This was a retrospective cohort study that did not allow for control of confounding factors such as concomitant sedative exposure which may have influenced outcomes. Also, our limited sample size may have prevented us in detecting a difference between the groups. In addition, the majority of our patients were 2 years of age or younger, making it difficult to generalize this protocol to older children and adolescents. Finally, our institution did not utilize a standardized scoring tool to assess withdrawal in the preintervention phase; during this phase, withdrawal assessment was dependent on the nurses’ interpretation of opiate withdrawal symptoms and not on a standardized scale. This negated the opportunity for direct comparison of withdrawal incidence between the groups using a validated tool and led to the use of breakthrough morphine doses as a surrogate marker for estimating withdrawal incidence. The complex medical conditions affecting the patients in the cohort made it challenging to conclusively measure the impact of the implemented interventions on PICU length of stay. Patients remained hospitalized for prolonged periods after being weaned off of opiates due to factors, such as feeding intolerance, multiple comorbidities, complex social issues, and/or awaiting cardiac transplantation.
Conclusions
The implemented opiate wean protocol and WAT-1 scoring tool reduced total methadone exposure in the postintervention group. The results support continuation of the protocol and scoring tool at our institution. However, larger prospective studies are needed to determine the ideal weaning strategy for pediatric patients exposed to continuous opiate infusions.
Footnotes
Acknowledgments
Special thank you to the pediatric critical care nurses, critical care physicians, and clinical pharmacists for all of their hard work to make this endeavor possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.