
Abstract
Background:
Argatroban, a synthetic, parenteral, nonheparin anticoagulant, is a direct thrombin inhibitor indicated for the prophylaxis or treatment of venous thromboembolism (VTE) in patients with heparin-induced thrombocytopenia with thrombosis (HITT) and for use during percutaneous coronary intervention (PCI) in patients who have or are at risk for developing HITT. Although heparin resistance occurs in approximately 0.5% to 5% of heparin-treated patients and is well documented in the literature, argatroban resistance is limited to a single case report. The objective of this case is to describe a case in which argatroban resistance was suspected in a patient with critical limb ischemia.
Methods:
This is a case report of a single patient.
Results:
A 68-year-old female admitted for critical limb ischemia requiring vascular intervention was treated for presumed HITT with argatroban. A therapeutic activated partial thromboplastin time (aPTT) was not attained (31 seconds) despite multiple uptitrations of the dose to 2.8 μg/kg/min (adjusted based on the institutional protocol and with consideration of organ dysfunction). A coagulopathy workup revealed a high level of factor VIII (265%).
Conclusion:
This case supports early assessment of factor VIII levels and the consideration of argatroban resistance and in patients who have a subtherapeutic aPTT, despite multiple increases in dose with an elevated factor VIII level. Early identification should prompt the use of an alternative anticoagulant to ensure efficacy.
Background
Argatroban, a synthetic, parenteral, nonheparin anticoagulant, is a direct thrombin inhibitor indicated for the prophylaxis or treatment of venous thromboembolism in patients with heparin-induced thrombocytopenia with thrombosis (HITT) and for use during percutaneous coronary intervention in patients who have or are at risk for developing HITT. 1 Argatroban is in the same pharmaceutical class as bivalirudin; however, it is metabolized predominantly in the liver and has a half-life of about 39 to 51 minutes and it can be prolonged in patients with acute renal failure and liver dysfunction. 2 Monitoring parameters include the activated partial thromboplastin time (aPTT), hemoglobin, and hematocrit. As with other anticoagulants, the major side effect is bleeding. Tests of anticoagulant effects (including the aPTT) typically attain steady-state levels within 1 to 3 hours following initiation in a patient with normal liver function. Although heparin resistance occurs in approximately 0.5% to 5% of heparin-treated patients and is well documented in the literature, argatroban resistance is limited to a single case report. 3 –6 We herein describe a case of a lack of aPTT correlation with uptitration of argatroban doses in treatment of presumed rapid onset HITT in which early identification of resistance and consideration of elevated factor VIII levels may have ensured therapeutic anticoagulation more quickly.
Case Description
A 68-year-old female (weight, 60 kg) with a past medical history of diabetes mellitus, hypertension, chronic kidney disease (stage III), peripheral artery disease, and multiple left lower extremity stents was transferred from an outside hospital to our surgical trauma intensive care unit (ICU) for right lower extremity Rutherford 2B critical limb ischemia. The patient emergently underwent a right femoral endarterectomy and patch angioplasty, graft thrombectomy, diagnostic angiogram, catheter-directed thrombolysis, tibial embolectomy, infrageniculate popliteal artery angioplasty and stenting, and 4-compartment fasciotomy. This was complicated by postoperative bleeding and required reexploration. The patient was transferred the surgical ICU postoperatively for hemodynamic monitoring, frequent vascular exams, and reinitiation of systemic anticoagulation.
Intravenous heparin was initiated at 15 U/kg/h (900 U/h) for critical limb ischemia, with a target aPTT 60 to 90 seconds (baseline aPTT prior to heparin initiation: 32.3 seconds [normal range: 25.7-35.7 seconds]) or target anti-Xa goal 0.3 to 0.7 IU/mL. The patient was transitioned from therapeutic intravenous heparin after 12 hours of therapy to argatroban due to the concern for rapid-onset HITT, given previous exposure less than 100 days prior. The patient’s 4 T score was 6, indicating a high probability of HITT (∼64%) due to the platelet count fall in ≤1 day that was >50% and nadir ≥20 K/μL, progressive thrombosis, and no other apparent causes for thrombocytopenia. 7,8 An immunoassay and a functional assay for HITT antibodies were sent and argatroban was promptly initiated at 1 μg/kg/min (3600 μg/h). At this time, the patient’s serum creatinine level was 2 mg/dL, correlating to an estimated creatinine clearance of ∼26 mL/min/1.73 m2. Liver function tests were not ordered but were presumed to be normal at the time of initiation.
Despite running at the appropriate rate via a medication infusion pump and through a dedicated intravenous line for the entirety of treatment, aPTT levels were subtherapeutic (targeted range: 50-75 seconds) and increased appropriately per protocol (see Table 1). Drug–drug interactions that could have diminished the anticoagulant effect of argatroban were assessed for and were not present. Other laboratory values at this time revealed a factor VIII level of 265% (normal value: 55%-145%). The PF4 antibody optical density came back grossly negative at 0.019 (normal value: ≤0.3), and the patient was immediately switched back to a heparin infusion without any issues and with appropriate platelet recovery. The rest of the patient’s hospital course was uneventful and she was discharged on hospital day 11 to a rehabilitation facility on apixaban therapy.
Argatroban Monitoring and Dose Adjustment.
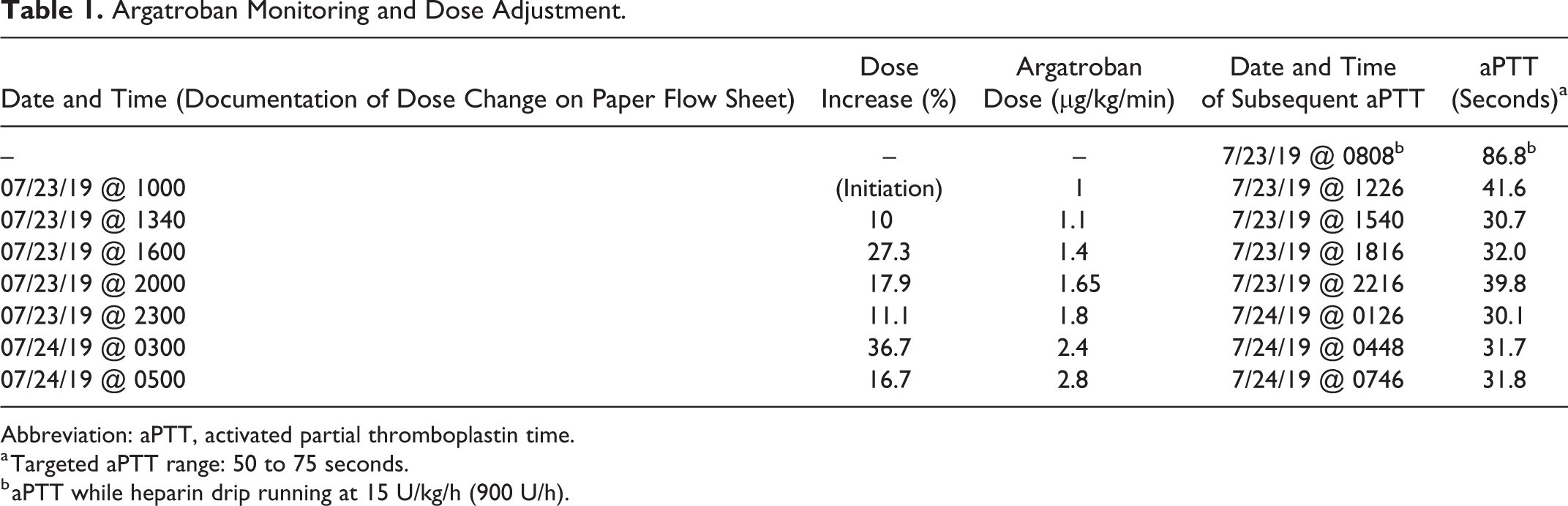
Abbreviation: aPTT, activated partial thromboplastin time.
a Targeted aPTT range: 50 to 75 seconds.
b aPTT while heparin drip running at 15 U/kg/h (900 U/h).
Discussion
Argatroban exerts its anticoagulant effects by inhibiting thrombin-catalyzed or thrombin-induced reactions, including fibrin formation; activation of coagulation factors V, VIII, and XIII; activation of protein C; and platelet aggregation. 1 The package insert recommends a starting dose of argatroban of 2 μg/kg/min administered as a continuous infusion in patients without hepatic impairment. However, the protocol at our institution recommends a starting dose of 1 μg/kg/min, consistent with the guidelines for HITT management. 1 To our knowledge, only one other case of possible argatroban resistance has been described in the literature in which a 59-year-old female reached doses of argatroban up to 7 μg/kg/min with a corresponding argatroban level of 2.2 μg/mL (therapeutic range: 0.4-1.2 μg/mL) and an aPTT of 53.1 seconds. Notably, the patient had an elevated factor VIII level of 276%. 7 In the preceding case, further therapy was titrated to argatroban levels. Evaluation of argatroban levels was not completed in our patient case.
The use of aPTT has been challenged as the accepted coagulation parameter for anticoagulant monitoring, most recently for heparin. The response varies with the reagent used. For use in HITT, therapy with argatroban is monitored using the aPTT, with a target range of 1.5 to 3 times the initial baseline value (not to exceed 100 seconds). 1 The Ecarin clotting time may be a more specific monitoring parameter for argatroban; however, it is not commercially available. Thrombin time, a measurement of the conversion of fibrinogen to fibrin, may also be prolonged by the presence of argatroban; however, it is not used routinely. Tests of anticoagulant effects (including the aPTT) typically attain steady-state levels within 1 to 3 hours following initiation of argatroban in patients without hepatic impairment, which was not seen in our patient. 1
The patient was therapeutic on a heparin drip (dose = ∼15 U/kg/h) before and after the use of argatroban therapy in the setting of suspected HITT. However, we were unable to achieve a therapeutic aPTT, despite aggressive argatroban dosing in a patient with an elevated factor VIII level of 265%. When a patient is administered a direct thrombin inhibitor, the clot-based factor VIII will be falsely decreased. Therefore, the actual factor VIII level was most likely higher. Factor VIII is a cofactor of factor IXa, which in the presence of calcium and phospholipid form a complex that activates factor X. Factor VIII is also involved in the formation of tissue thromboplastin (intrinsic prothrombin activation). Elevated factor VIII levels have been described as an acute-phase reactant and can be increased in other acquired disorders, including late normal pregnancy, liver disease, postoperative period, and rebound activity after sudden cessation of a coumarin-type drug. 9 In vitro blunting of aPTT has been described in the setting of elevated factor VIII levels during heparin therapy, necessitating the use of anti-Xa monitoring. 9,10
When initiating argatroban therapy, close monitoring of aPTT is needed to ensure adequate anticoagulation and to prevent life-threatening bleeding complications. Excessive argatroban dosing requirements or a prolonged time to reach a therapeutic aPTT should prompt further investigation into potential confounders such as elevated factor VIII levels and a switch to a different anticoagulant. This case elucidates the importance of early identification of argatroban resistance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.