
Abstract
Background:
Most antibiotic prescriptions originate in the outpatient setting and an estimated 30% are unnecessary. Pharmacists are well positioned to positively impact antibiotic prescribing habits; the role of the community pharmacist in outpatient antibiotic stewardship programs is not well defined.
Objectives:
The objectives of this study were to (1) assess the knowledge of the general public regarding appropriate antibiotic use, and (2) assess the experiences of the general public regarding delayed antibiotic prescriptions.
Methods:
A cross-sectional survey was administered at community pharmacies in Kansas from September 2018 to January 2019. Eligible individuals were older than 18 years and self-reported their ability to speak and read English. The 22-item survey collected demographics, knowledge regarding appropriate antibiotic use, and participant understanding and experiences of delayed antibiotic prescribing. Descriptive statistics assessed demographics and chi-square compared responses between demographics.
Results:
Of 347 surveys completed, respondents were mainly Caucasian (91.6%), female (58.2%), and aged 60 years or older (59.1%). Those with high school education or below were more likely to believe antibiotics kill viruses (43.1% vs 20.9%, respectively; p < 0.01) and that antibiotics work on most coughs and colds (31.4% vs 16.2%, respectively; p = 0.01). Delayed antibiotic prescriptions were more frequently offered to those who had received an antibiotic prescription in the last year compared to those who had not (36.1% vs 15%, p < 0.001).
Conclusion:
Gaps in patient knowledge about appropriate antibiotic use and delayed prescribing present an opportunity for community pharmacists to educate patients and become involved in outpatient antibiotic stewardship.
Introduction
According to the Centers for Disease Control and Prevention (CDC), approximately two million individuals develop antimicrobial-resistant infections each year in the United States. 1 Antibiotic-resistant pathogens may require the use of alternative, more toxic treatment, often leading to poorer health outcomes, increased rates of adverse events, and higher health care costs. 1 Inappropriate antibiotic use is an imperative and modifiable contributor to antimicrobial-resistant bacterial pathogens. The vast majority of antibiotic prescriptions originate in the outpatient setting, and an estimated 30% of these prescriptions are deemed unnecessary. 2 Determining whether to prescribe an antibiotic can be difficult for health care practitioners, and patient demand is frequently cited as an influential decision-making factor. 3 Patients may falsely believe that antibiotics are needed to relieve symptoms caused by viral infections such as a fever, sore throat, or cough. 4 Therefore, understanding the foundation of patient education gaps that lead to antibiotic misuse is essential.
The Infectious Diseases Society of America defines antibiotic stewardship as “coordinated interventions designed to improve and measure the appropriate use of antimicrobials by promoting the selection of the optimal antimicrobial drug regimen, dose, duration of therapy, and route of administration.” 5 Although the role of the pharmacist in health system–based antibiotic stewardship programs has been shown to decrease inappropriate prescribing of antibiotics by up to 31%, current best practices and the role of the community pharmacist in outpatient antibiotic stewardship are not as clearly defined. 6,7
Strategies to change current antibiotic prescribing trends are needed to prevent circumstances in which serious infections no longer respond to available treatment options. One strategy recommended by the CDC Core Elements of Outpatient Antibiotic Stewardship is to delay prescribing when appropriate. 6 Clinicians utilizing delayed antibiotic prescribing issue an antibiotic prescription for use at a designated later date if patient symptoms worsen or do not resolve. This practice has previously demonstrated a 58% reduction in antibiotic use when compared with immediate prescribing. 8 Additionally, the CDC Core Elements of Outpatient Antibiotic Stewardship calls upon community-based pharmacists, one of the most accessible health-care professionals, to provide patient education on the appropriate use of antibiotics. 6 These pharmacists are well positioned to educate patients on appropriate antibiotic use and are qualified to recommend appropriate over-the-counter (OTC) medications for the self-treatment of minor symptoms related to common viral illnesses.
The purpose of this study was to assess the knowledge of the general public regarding appropriate antibiotic use and to assess the experiences of the general public regarding delayed antibiotic prescriptions.
Methods
Study Design
The 22-item prospective, cross-sectional questionnaire (Online Appendix A) was a modified version of a questionnaire taken from a previously published study. 9 The written questionnaire included six questions for participant demographics, nine questions that evaluated knowledge regarding appropriate antibiotic use, six questions that measured participant understanding and experiences of delayed antibiotic prescribing, and one free response question to address any additional comments regarding the questionnaire. Questions were presented in multiple-choice single answer, true/false, and free-response formats. The “University of Kansas Medical Center” Human Subjects Committee granted this study exempt status prior to commencement.
Inclusion and Exclusion Criteria
Participants were eligible if they were 18 years or older. Participants were excluded from the study if they were unable to read or speak English or unwilling to complete the questionnaire while at the pharmacy.
Approach
Questionnaire administration and collection occurred between September 2018 and January 2019 at four pharmacies operated by Balls Food Stores, a grocery store chain located in the Kansas City metropolitan area. The pharmacies selected are located within the same county and serve a diverse patient population relative to income, age, and education. If an individual presented to one of the participating pharmacies for an influenza vaccine, he or she was given the option of completing the questionnaire if the inclusion criteria were met. Upon consent, the questionnaire was completed while the individual waited for administration of the influenza vaccine. Targeting those receiving their annual influenza vaccine avoided duplicate questionnaire responses. A cover letter was provided to explain the purpose of the questionnaire and instructions for completion (Online Appendix A). To ensure anonymity, participants immediately placed the completed questionnaire into a tamper-resistant collection box only accessible to the primary investigator. Upon receipt of a completed questionnaire, a nonmonetary incentive was added to the participant’s grocery store rewards card. Questionnaires were retrieved at regular intervals throughout the data collection period by the primary investigator and securely stored in a locked office.
Statistical Analysis
Descriptive statistics were used to evaluate participant demographics. Knowledge and experiences with antibiotic use and delayed antibiotic prescribing were evaluated using chi-square between different demographic groups, with an a priori alpha of 0.05. SPSS version 25 (Chicago, Illinois) was used for quantitative analyses.
Results
Study Population
Three hundred forty-seven participants answered the questionnaire and were included in data analysis. Of these participants, 20.7% did not answer one or more questions. The majority of respondents were Caucasian (91.6%), female (58.2%), and aged 60 years or older (59.1%). Additionally, nearly two-thirds (61.6%) of respondents reported completion of a college education or higher (Table 1).
Questionnaire Participant Demographics.
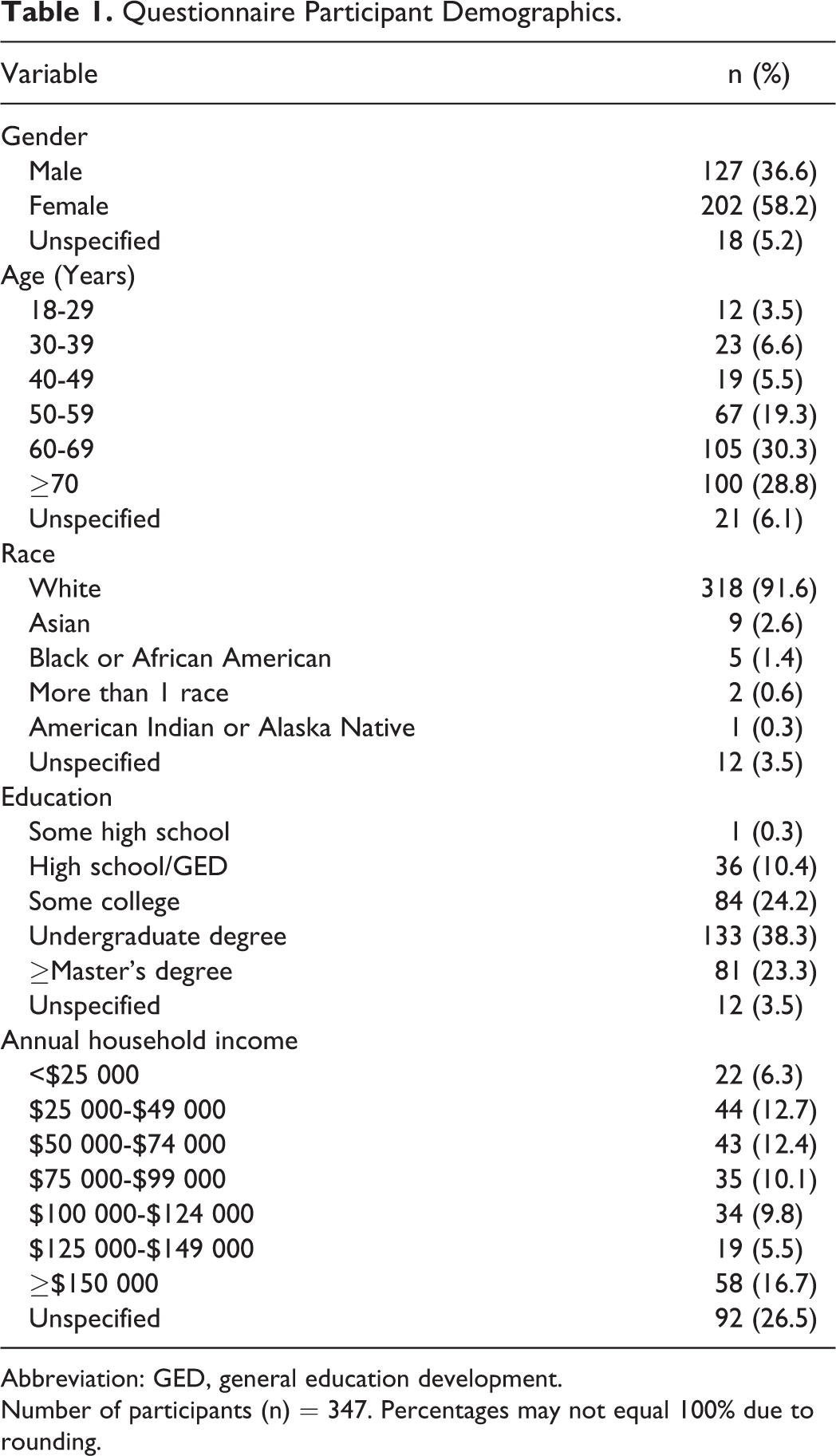
Abbreviation: GED, general education development.
Number of participants (n) = 347. Percentages may not equal 100% due to rounding.
Questionnaire Results
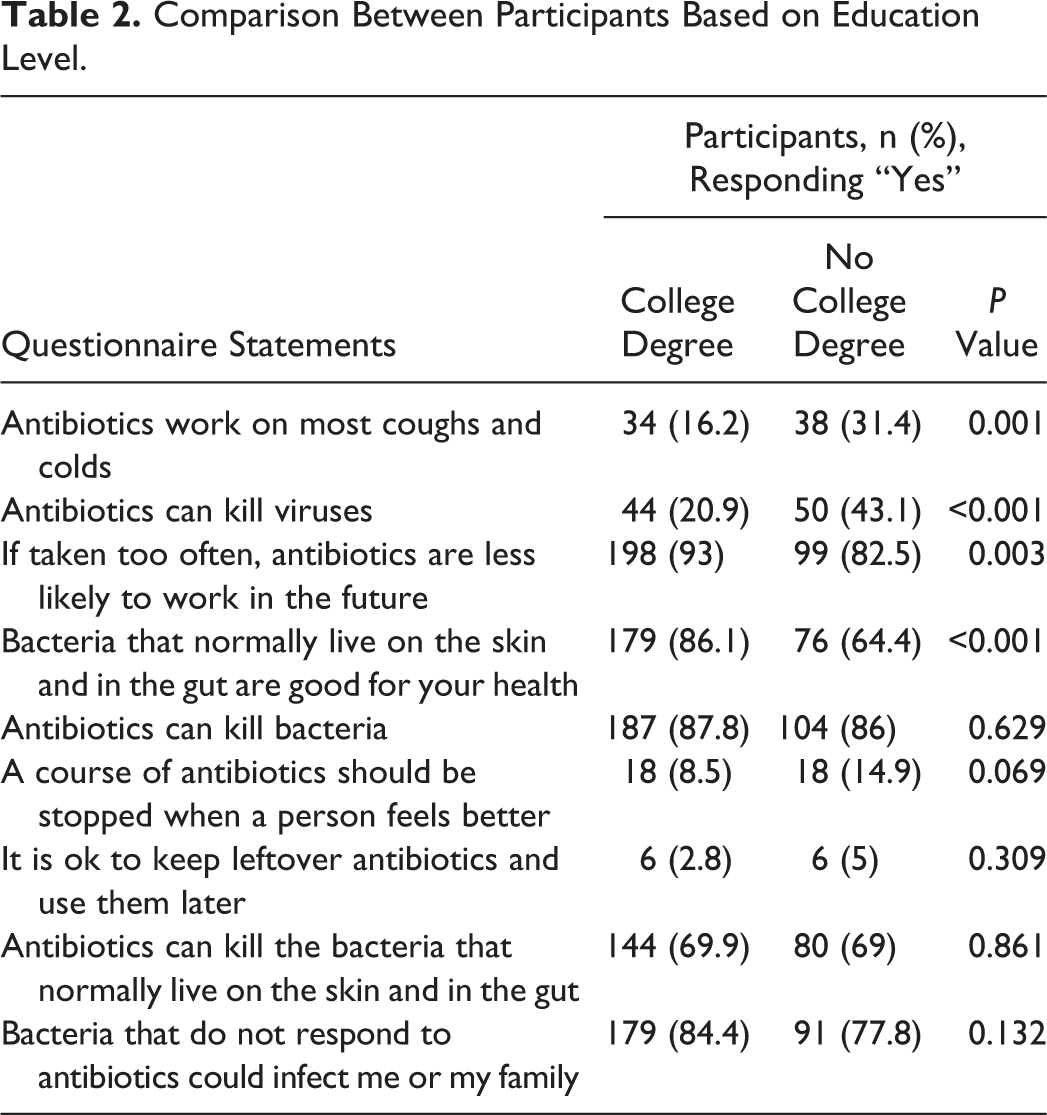
Four comparisons of questionnaire statements between participants based on education level reached statistical significance (Table 2). Questionnaire items were also compared between participants based on prior antibiotic use (Figure 1). Delayed antibiotic prescriptions were more frequently offered to those who reported receiving an antibiotic prescription in the last year compared to those who did not (36.1% vs 15%, respectively; p < 0.001). Of the questionnaire respondents, nearly half of those who reported antibiotic use within the past year reported presenting to a doctor or nurse for a respiratory infection. Additionally, 36% of participants who reported the use of an antibiotic within the past year were offered an antibiotic if symptoms did not improve, and 25% of those participants were offered to return to the prescriber’s office if there was no symptom improvement.
Comparison Between Participants Based on Education Level.
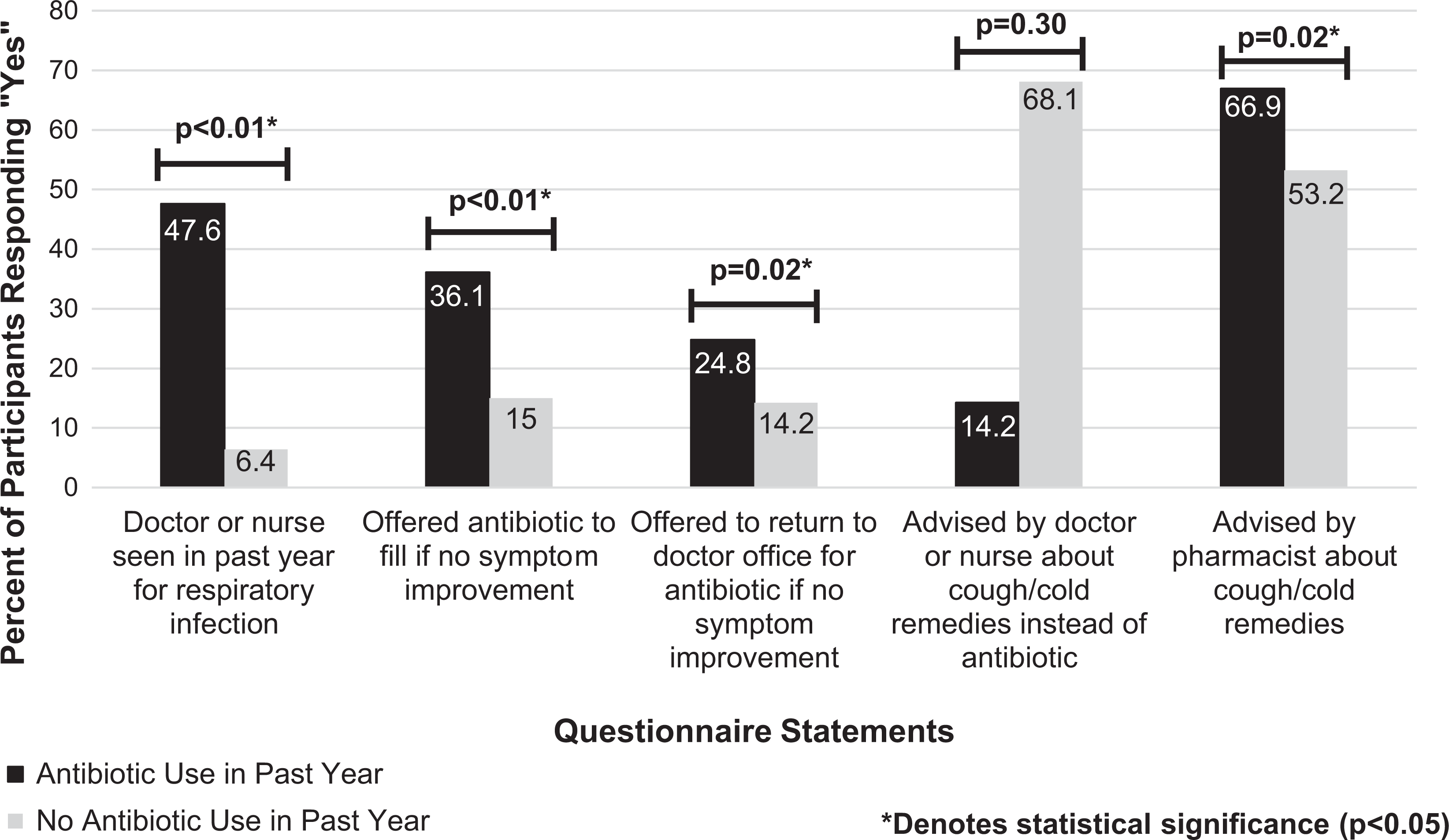
Comparison between participants based on reported prior antibiotic use.
Discussion
To the authors’ knowledge, this is the first study to assess the knowledge and experiences of the general public regarding appropriate antibiotic use and delayed antibiotic prescribing in the community pharmacy setting. Since the majority of antibiotic prescribing occurs in the outpatient setting, pharmacists are increasingly called upon to design and implement strategies for antibiotic stewardship in the outpatient setting. 10 Although not directly addressed in the study, the results suggest a number of opportunities for community pharmacists to engage in antimicrobial stewardship initiatives. However, the body of evidence concerning the role of the community pharmacist in outpatient antibiotic stewardship programs is limited.
Higher levels of education were associated with increased knowledge about appropriate antibiotic use, which is congruent with results obtained from previous studies. 11 -13 In the current study, those with high school education or below were nearly twice as likely to believe antibiotics are effective in treating the common cold (31.4% vs 16.2%). Similarly, the World Health Organization (WHO) conducted an international survey in 2015 to determine public awareness and attitudes toward antibiotic use across a variety of countries and found that respondents with less education were more likely to believe antibiotics are beneficial in the treatment of the common cold and flu (71% vs 61%). 11 Although knowledge of appropriate antibiotic use was influenced by education level in both studies, more respondents understood which medical conditions can be treated with antibiotics in the current study. This may be attributed to a less diverse patient population surveyed in comparison to the WHO Multi-Country Public Awareness Survey or may suggest that health care providers in the same geographic area in which the study pharmacies were located provided enhanced communication and education about appropriate antibiotic use during patient encounters. Additionally, those with a higher level of education in the current study were significantly more likely to believe the effectiveness of antibiotics decreases if taken too often compared to those with less education (93% vs 82.5%). This was consistent with Davis and colleagues, who surveyed 190 participants from primary care clinics and urgent care locations in the eastern United States. Their survey found that those with a college degree or higher were significantly more likely to believe that an antibiotic may not be effective in treating an individual’s illness if taken unnecessarily versus those with lower education levels (72.4% vs 55.4%). 12 The higher percentage of correct responses reported by participants in the current study may indicate health care providers in the area in which the current study was conducted have educated patients about the harms of antibiotics more frequently than health care providers at other outpatient locations.
This study found that nearly 30% of questionnaire participants believed that antibiotics are effective in the treatment of viral infections, although this percentage is lower than the 55% reported in a large survey completed in a British population by McNulty et al. 14 The current study included a larger percentage of respondents with a college degree or higher compared to McNulty et al (61.6% vs 18%). 14 The higher education level may have led to a lower percentage of participants incorrectly believing that antibiotics can effectively treat viral infections. The current study utilized a modified version of a questionnaire previously used in a study published by McNulty et al in 2010. The McNulty study found that 13% of questionnaire respondents reporting antibiotic use within the past year had been offered an antibiotic prescription by a provider to be filled if symptoms worsened or did not improve after several days. 9 This finding is lower than the results of the current study (36%). However, these low percentages indicate there are still additional opportunities to increase delayed antibiotic prescribing habits among providers to better align with the best practices outlined in the CDC Core Elements of Outpatient Antibiotic Stewardship. 6 One example of best practices included in the CDC Core Elements document is to identify conditions in which delayed antibiotic prescribing is appropriate but underused and implement at least one policy or practice to improve delayed antibiotic prescribing habits, assess whether the intervention is effective, and modify as needed. 6 The differences among participants observed between the studies conducted by McNulty et al in 2010 and the current study may be attributed to an increased awareness among the general public and health care providers regarding appropriate antibiotic use between the two study periods. The United States government initiated a nationwide strategy aimed to take action against antibiotic resistance in 2014 and subsequently an action plan for combating antibiotic-resistant bacteria was implemented in 2015. 15,16 As a result of these initiatives, certain state health departments have enacted educational programs with the intention of decreasing inappropriate antibiotic use by modifying the attitudes and behaviors of consumers and health care providers, as well as increasing awareness of the general public regarding appropriate antibiotic use and resistance. 17
In the current study, nearly half (47.6%) of individuals who reported using an antibiotic within the past year presented to their prescriber’s office for a respiratory tract infection, a condition commonly of viral etiology. Previous data indicate that practitioners may inappropriately prescribe antibiotics for viral infections for several reasons including patient satisfaction, time constraints, diagnostic uncertainty, and externalized responsibility. 4 Sanches and colleagues similarly reported that the most commonly perceived reasons among primary care providers for inappropriate antibiotic prescribing were pressure from patients or caregivers and concern for patient satisfaction as a result of the visit. 18 However, additional studies indicate that patients prefer antibiotic prescriptions less frequently than health care providers perceive and inappropriate antibiotic prescribing often results from this misperception. 19,20
In this study, slightly over two-thirds (66.9%) of individuals who reported the use of an antibiotic within the past year sought advice from a pharmacist regarding cough or cold remedies. These findings indicate that community pharmacists are perceived as easily accessible to the general public and are well positioned to influence the management of acute illnesses. Additionally, the gaps in knowledge identified among the general public regarding appropriate antibiotic use in this study indicate an opportunity for community pharmacists to better educate consumers about antibiotic use such as indication for use, duration of therapy, and risks associated with unnecessary use. Since community pharmacists are among the most accessible health care providers and often serve as the last point of contact prior to a patient beginning antibiotic therapy, it is imperative they are adequately exposed to the information and training necessary to implement and sustain outpatient antibiotic stewardship interventions. In 2018, a study conducted by Kufel and colleagues reported that greater than two-thirds (68.1%) of Doctor of Pharmacy (PharmD) programs in the United States have incorporated antibiotic stewardship education into the didactic curriculum. 21 Additionally, in a survey conducted in 2014 by Justo and colleagues among graduating student pharmacists, over half (54%) of respondents agreed their education was “good or very good” in the preparation of streamlining or de-escalating antibiotic therapy. 22 As discussed by Kufel and colleagues, incorporating outpatient antibiotic stewardship into pharmacy school curricula will better prepare the next generation of pharmacists as antibiotic stewards. 21 The findings of the current study and ease of patient access to community pharmacists highlight the importance of educating student pharmacists regarding the application of outpatient antibiotic stewardship principles and pharmacotherapy optimization in addition to traditional approaches to teaching infectious diseases pharmacotherapy. However, while Kufel and colleagues reported approximately 84% of PharmD programs in the United States incorporate antibiotic stewardship education into experiential education, this was primarily related to health system–based experiential rotations versus community pharmacy practice. 21 By incorporating outpatient antibiotic stewardship efforts into pharmacy school curricula, community pharmacists are more likely to feel confident in implementing strategies to reduce current antibiotic resistance patterns. In order to accomplish this, it may be beneficial to allow student pharmacists the opportunity to apply antibiotic stewardship principles within different pharmacy practice settings. Examples of approaches to enhance education on outpatient antibiotic stewardship within the pharmacy school curricula include modifying inpatient-based pharmacotherapy cases focused on antibiotic stewardship principles to include longitudinal scenarios and training student pharmacists to effectively evaluate the safety and efficacy of antibiotics via patient consultation when access to objective laboratory data is unavailable. This type of education may prepare student pharmacists pursuing postgraduate community pharmacy residency training in assisting with the development and sustainability of outpatient antibiotic stewardship programs.
According to the most recent Bureau of Labor statistics, community pharmacists account for approximately 58% of the pharmacy profession. 23 However, the majority of antibiotic stewardship efforts have been directed toward health system–based pharmacists. 23,24 The results of a survey conducted by the Minnesota Department of Health reported that about three-fourths (76%) of pharmacists with prior history of implementing a pharmacy-based antibiotic stewardship policy were associated with a hospital or outpatient clinic. 24 However, an official position statement of the Society of Infectious Diseases Pharmacists released in 2018 emphasizes the value of community pharmacists in outpatient antibiotic stewardship efforts due to their frequent interaction with patients and their ability to influence the continuity of care. 10 Over time, antibiotic stewardship initiatives have been implemented to increase immunization rates, develop disease state–based antibiotic treatment guidelines, and educate the general public regarding appropriate antibiotic use. For example, the American Academy of Pediatrics partnered with pediatric practices in Virginia to decrease antibiotic prescription use for children with viral upper respiratory tract infections and improve antibiotic prescribing for bacterial acute otitis media, sinusitis, and pharyngitis. In-person meetings and monthly webinars aimed to change provider behaviors and beliefs about appropriate antibiotic use resulted in decreased prescription fill rates for acute otitis media through the use of delayed antibiotic prescribing. Also, education was provided more frequently to families about appropriate antibiotic use and symptom management following antibiotic stewardship interventions. 25 However, despite these efforts, inappropriate antibiotic prescribing rates remain high in the United States. 26 Therefore, involving community pharmacists in outpatient antibiotic stewardship interventions may be useful in improving coordination of care, encouraging the judicious use of antibiotics, and increasing patient satisfaction. For example, community pharmacists could partner with a nearby health care provider to establish a collaborative practice agreement (CPA) outlining appropriate antibiotic initiation in patients with confirmed group A streptococcal infections. CPAs can enhance team-based care by enabling each member of the health care team to augment the knowledge and abilities of one another to more effectively provide patient-centered care, which often leads to improved patient outcomes. 27 Under such a CPA, community pharmacists could perform a rapid diagnostic point-of-care test and initiate appropriate therapy in a timely manner based on the results. As demonstrated with the current study, patients often seek advice from community pharmacists regarding symptomatic relief with OTC remedies. Therefore, if an antibiotic is not indicated to treat an individual’s acute illness based on a negative rapid diagnostic point-of-care test result, community pharmacists could direct the patient toward appropriate OTC medications for symptomatic relief. Additionally, the development of CPAs focused on the management of specific infectious diseases in the community pharmacy setting may reduce the number of visits to a health care prescriber for certain illnesses. Also, community pharmacists are well positioned to provide proper education to patients regarding the difference between a bacterial versus a viral infection, explaining when antibiotics are not necessary, and recommending when to seek medical care if symptoms worsen or fail to improve. Other outpatient antibiotic stewardship interventions community pharmacists could be involved with include following up with patients two to three days after dispensing an antibiotic prescription to evaluate for adverse reactions and verify adherence, delivering continuing education presentations on appropriate antibiotic use to health care prescribers and patients, and collaborating with health care providers to develop evidence-based algorithms for the appropriate management of infectious diseases. Also, community pharmacists can potentially utilize medication therapy management services to evaluate and educate on drug–drug interactions between antibiotics and chronic medications and clarify and update any allergies to antibiotics reported. Further exploration is necessary to better understand the effectiveness of such initiatives.
Limitations identified with this study include that the study was completed in a limited geographic area with all study pharmacies located in an urban area, so it is uncertain if the study results are generalizable to antibiotic prescribing habits in other geographic areas or rural populations. The study sample lacked ethnic and gender diversity; therefore, it is uncertain if the study results are generalizable to other populations. Another limitation of this study is the large percentage of respondents (61.6%) with a college degree or higher. When compared with the distributions described by the US 2017 census data, the respondents of the current study reported a higher level of education than the general public (61.6 vs 33.4). 28 Also, some participants did not complete the questionnaire in its entirety. Responses to questions included on the questionnaire were not required and unanswered items may have impacted results of this study. However, responses from incomplete questionnaires were included in data analysis. Lastly, the reliance on self-reported behavior from questionnaire respondents may have led to recall bias. Due to the anonymity of the questionnaire, the primary investigator was unable to objectively verify history of prior antibiotic use among participants.
Future research is needed to determine which outpatient stewardship interventions are most effective in the community pharmacy setting. One suggestion to accomplish this would be to measure antibiotic prescribing habits of local health care providers before and after a community pharmacist-led educational outreach program is delivered. The purpose of the community pharmacist-led educational outreach program to health care providers would be to discuss appropriate antibiotic use in order to encourage evidence-based prescribing. Specifically, it may be beneficial to evaluate the effectiveness of community pharmacist-led communications training in which health care providers are educated on how to appropriately assess patient expectations and understanding of the information discussed to further reduce inappropriate antibiotic prescribing habits. Another area of interest would be to survey the general public before and after a community pharmacist-led public health campaign on appropriate antibiotic use and antibiotic resistance. Also, surveying community pharmacists regarding their perceptions and attitudes toward the implementation of outpatient antibiotic stewardship programs may be useful to develop strategies to overcome potential barriers identified. Additionally, community pharmacies could consider partnering with a Quality Innovation Network/Quality Improvement Organization in the area to develop a local antibiogram to identify antibiotic resistance patterns. With this information, community pharmacies could use their prescription data to compare antibiotic use in their area to resistance patterns in order to potentially establish opportunities for improvement.
Conclusion
Overall, knowledge of appropriate antibiotic use among participants surveyed in the community pharmacy setting was influenced by education level. Additionally, knowledge and experiences of delayed antibiotic prescribing among questionnaire participants was influenced by receipt of an antibiotic prescription within the past year. Gaps in patient knowledge about appropriate antibiotic use and delayed prescribing present an opportunity for community pharmacists to educate patients and to become involved in outpatient antibiotic stewardship. The involvement of community pharmacists in outpatient antibiotic stewardship initiatives may be useful in improving knowledge of appropriate antibiotic use among consumers. Further evaluation is necessary to determine which outpatient antibiotic stewardship interventions are most effective in the community pharmacy setting.
Supplemental Material
Supplemental Material, Manuscript_Appendix_A - Patient Knowledge and Experiences With Antibiotic Use and Delayed Antibiotic Prescribing in the Outpatient Setting
Supplemental Material, Manuscript_Appendix_A for Patient Knowledge and Experiences With Antibiotic Use and Delayed Antibiotic Prescribing in the Outpatient Setting by Mary Beth A. Seipel, Emily S. Prohaska, Janelle F. Ruisinger and Brittany L. Melton in Journal of Pharmacy Practice
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.