
Abstract
Background:
Ketamine, an N-methyl-
Methods:
We conducted a single center, retrospective cohort study of patients admitted to the medical intensive care unit (MICU) between 2013 and 2018. Patients who received continuous infusion ketamine or nonketamine sedatives (NKS) including dexmedetomidine, fentanyl, midazolam, or propofol were identified. The primary outcome was percentage of Richmond Agitation-Sedation Scale (RASS) scores at goal in patients receiving ketamine as adjunct to NKS compared to those on NKS alone.
Results:
A total of 172 patients were included (n = 86 ketamine, n = 86 NKS). Baseline characteristics were similar with the exception of antipsychotic use, which was higher in the ketamine group (P = .008). Percentage of RASS scores at goal was not different between groups (78.7% vs 81.4%, P = .29). Fewer patients in the ketamine group received continuous infusion fentanyl (76.7% vs 94.2%, P = .002). Patients on adjunctive ketamine required fewer days of intermittent benzodiazepines (0 [0-1] vs 1 [1-2], P < .0001). Patients receiving ketamine required less norepinephrine, receiving a median of 6.32 mg (2.4-20) versus 11.7 mg (5.2-45.2; P = .03). There was no difference in receipt of new antipsychotics or occurrence of arrhythmias.
Conclusion:
Addition of ketamine did not increase the percentage of RASS scores at goal versus NKS but was well tolerated. Ketamine was associated with reductions in norepinephrine requirements, days of intermittent benzodiazepine administration, and number of patients receiving continuous infusion fentanyl. Continuous infusion ketamine appears safe and effective for sedation in the MICU.
Background
Appropriate sedation and analgesia are cornerstones of care of mechanically ventilated patients. Opioids such as fentanyl are often the backbone of both pain and sedation management but are associated with respiratory depression, hypotension, and decreased gut motility. 1 Benzodiazepines have been associated with intensive care unit (ICU) delirium, prolonged mechanical ventilation, and increased mortality, and are therefore not routinely recommended.2-5 Other agents, such as propofol and dexmedetomidine, are not associated with these negative outcomes but may cause adverse hemodynamic effects, including hypotension and bradycardia. 1
Ketamine is an old sedative that has recently seen a resurgence in use due to its unique mechanisms of action and side effect profile. The primary mechanism of action is antagonism of the N-methyl-
Currently, ketamine is only approved for induction and maintenance of anesthesia. The 2018 Clinical Practice Guideline for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Insomnia and Sleep Disruption (PADIS) recommends ketamine for reduction of opioid use in postsurgical ICU patients but does not include a broad recommendation for ketamine use in other ICU populations. 7 In practice, continuous infusion ketamine is becoming increasingly popular as an adjunctive sedative for ICU patients, in part due to its quick onset and preservation of spontaneous respirations and airway reflexes. Limitations to use are unfamiliarity among practitioners and concerns about potential side effects, including hypertension, tachycardia, and emergence reactions. 8
Evidence for continuous infusion ketamine for sedation of critically ill patients is limited. There are a few studies evaluating ketamine as an alternative analgesic in critically ill traumatic brain injury patients; however, the focus of these studies was evaluating safety and concomitant sedative/analgesics.9-11 Previous studies of continuous infusion ketamine have evaluated single cohorts of mixed medical and surgical ICU patients before and after the addition of adjunctive ketamine. These studies suggest ketamine improves time at goal sedation and/or allows for reduced doses of concomitant sedatives.12,13 However, these outcomes may have been influenced by the inclusion of surgical ICU patients, a population more likely to derive benefit from the analgesic and opioid-sparing effects of ketamine. To our knowledge, there are no studies evaluating attainment of goal sedation specifically in medical ICU (MICU) patients who received adjunctive ketamine compared to a separate cohort who received traditional sedatives only. The objective of this study was to evaluate the effectiveness and safety of continuous infusion ketamine as adjunct to nonketamine sedatives (NKS) in mechanically ventilated critically ill patients in the MICU compared to patients who received NKS alone.
Methods
We performed a retrospective cohort study comparing mechanically ventilated patients receiving adjunctive continuous infusion ketamine to those receiving continuous infusion (NKS) only in the MICU at University Hospital, a large, academic, tertiary care medical center in San Antonio, Texas. This study was approved by the institutional review board at University of Texas Health Science Center, San Antonio, and the University Health System research department. Pharmacy billing records were used to identify patients admitted to the MICU from January 2013 to December 2018 who received continuous infusion ketamine as adjunctive sedation or those who received NKS only, including dexmedetomidine, fentanyl, midazolam, or propofol. Patients 18 years and older who were mechanically ventilated for at least 24 hours with a goal Richmond Agitation-Sedation Scale (RASS) score of 0 to −3 were included. Patients were required to receive at least 6 hours of ketamine or comparator NKS infusion to be included. Patients on intermittent sedative or analgesic agents alone were not included. Patients were excluded if they were pregnant, prisoners, received a concomitant neuromuscular blocker (NMB) infusion, or if it was specified in the chart that the patient had a deeper goal level of sedation (RASS: −4 or −5). In the ketamine cohort, patients were excluded if ketamine was ordered for a nonsedation indication such as seizure management or analgesia alone.
At our institution, sedative and analgesic medications are selected by the medical team and titrated by nursing staff per protocol to achieve goal pain score and RASS of 0 to −3. All patients receive daily awakening trials where sedation is held unless there is a contraindication such as status epilepticus, neuromuscular blockade, targeted temperature management, or active alcohol withdrawal. Spontaneous breathing trials are also performed during spontaneous awakening trials. Standard interventions to prevent delirium include minimizing sleep interruption, avoiding benzodiazepines, and early mobility.
Patients receiving ketamine were screened first. The initial report of NKS patients included 367 items, with some individuals who received multiple continuous infusion NKS appearing more than once on the list. For these patients on NKS only, the list of billed medication charges was randomized in Excel, and patients who received multiple continuous infusion sedatives were limited to their first appearance on the list. Patients on the NKS list were screened in order and screening ended after 86 unique patients meeting inclusion criteria were identified. Based on a median time from ICU admission to initiation of ketamine of 1.3 days in the ketamine group, NKS patients were only included if on the NKS at 24 hours after initial ICU admission. This was done in order to evaluate the 2 groups at the same time in their hospital course to limit confounders. For the ketamine group, data were collected for the 6-hour period prior to ketamine initiation and for the duration of the ketamine infusion or 7 days, whichever came first. In the NKS group, data were collected from 24 hours after initial ICU admission through the duration of the primary NKS infusion or 7 days, whichever came first.
The primary analysis compared patients on ketamine versus NKS. The primary outcome was percentage of RASS scores at goal in the ketamine group versus the NKS group. Goal RASS was 0 to −3, with zero defined as alert and calm and −3 defined as moderate sedation. This goal was selected to be consistent with our institutional protocol. Patients were considered to have this goal RASS unless an alternative light sedation goal within this range was noted in the chart. This outcome was reported as number of RASS scores at goal (0 to −3) divided by number of RASS scores included in the collection period, multiplied by 100%.
Secondary outcomes included percentage of pain scores at goal, ICU length of stay, and in-hospital mortality, as well as concomitant sedative requirements, concomitant vasopressor requirements, and “as needed” analgosedation requirements. A secondary intrapatient analysis was performed to evaluate the ketamine group pre- and postketamine initiation. The first 24 to 48 hours of data after ketamine initiation was used for the paired comparison.
Baseline data collected for both groups included demographic information, past medical history, primary admit diagnosis, and Sequential Organ Failure Assessment (SOFA) score. The SOFA score recorded was calculated using the worst value for each criterion in the 24 hours prior to the start of ketamine or NKS, or if data for the 24 hours prior were not complete, the 24 hours following was used. RASS scores and pain scores were collected every 2 hours for all patients. Pain scores reported included both self-reported pain scores and scores derived from the nonverbal pain scale. The goal pain score was defined as 0 to 4.
Cumulative vasopressor and concomitant sedative requirements were recorded for the collection period. Intermittent benzodiazepine and opioid use were assessed by number of days on which any dose of benzodiazepine or opioid was received. Enteral nutrition (EN) tolerance was evaluated by number of days it was received and on which it was held; holding EN for a procedure was not counted. EN was assessed to determine if ketamine’s potential opioid-sparing effects would affect bowel motility and tolerance of feeding.
Confusion Assessment Method for the ICU (CAM-ICU) scores were collected to assess delirium. At our institution, CAM-ICU scores are recorded once per nursing shift. If CAM-ICU scores were missing for a 24-hour period, that day was not included in analysis. Any day on which a CAM-ICU score was positive was counted as a day of delirium. New scheduled antipsychotic use (defined as aripiprazole, quetiapine, and olanzapine) and intermittent antipsychotic use (primarily haloperidol) were also collected. Scheduled antipsychotics were considered new if the patient was not on an antipsychotic at home or prior to the start of ketamine or NKS infusion. For hemodynamic variables, we assessed mean arterial pressure (MAP), heart rate (HR), and arrhythmias. Maximum MAP and HR were collected for each 24-hour period. Arrhythmia occurrences were noted in the vital signs flowsheet. Tachycardia was defined as an HR > 120 beats per minute. Receipt of antihypertensive agents (defined as hydralazine, labetalol, and continuous infusion esmolol or nicardipine) was also collected.
Statistical Analysis
A sample size of 61 patients per group was needed to detect a 20% difference in the primary outcome of percentage of RASS scores at goal with an 80% power and alpha of 0.05. This effect size was determined based on previous data demonstrating an approximately 20% higher rate of RASS scores within goal with adjunctive ketamine sedation. 13 Categorical variables were compared using Fisher’s exact or chi-square test. Continuous data were tested for normality using the Shapiro-Wilk test. Continuous data that were normally distributed were reported as mean and standard deviation and analyzed using the student’s t test. Nonparametric continuous data were reported as median and interquartile range and analyzed using the Wilcoxon rank-sum test. The Wilcoxon signed-rank test was used for paired comparisons in the ketamine group. A 2-sided a priori α level ≤ 0.05 was used to determine statistical significance. JMP software version 11.0 (SAS Institute Inc) was used for data analysis.
Results
We identified 152 MICU patients who received continuous infusion ketamine for adjunct sedation during the study period. Of these patients, 66 were excluded for the following reasons: ketamine infusion < 6 hours (n = 25), mechanically ventilated < 24 hours (n = 7), ketamine indication other than sedation (n = 10), RASS goal not 0 to −3 (n = 1), pregnant (n = 1), prisoner (n = 3), concomitant NMB continuous infusion (n = 7), and ketamine administration not charted (n = 12). The remaining 86 patients who received ketamine were included for analysis. To identify the NKS group, we screened 282 patients in the MICU who received continuous infusion propofol, dexmedetomidine, midazolam, or fentanyl. We excluded 196 patients, of which 123 were excluded for not being on the identified sedative at 24 hours from ICU admission, with the remainder being primarily excluded for receiving ketamine, being mechanically ventilated <24 hours or being a prisoner.
Baseline characteristics were similar between groups (Table 1). In the overall population, the median age was approximately 55 years, and over half of patients were Hispanic (55.8%) and male (61.6%). Past medical history and primary admit diagnoses were also similar. Both groups had a median baseline SOFA score of 10 in the 24 hours prior to the collection period. The only significant difference at baseline was antipsychotic use (25.6% in ketamine group vs 9.3% in NKS group, P = .008).
Demographics.a
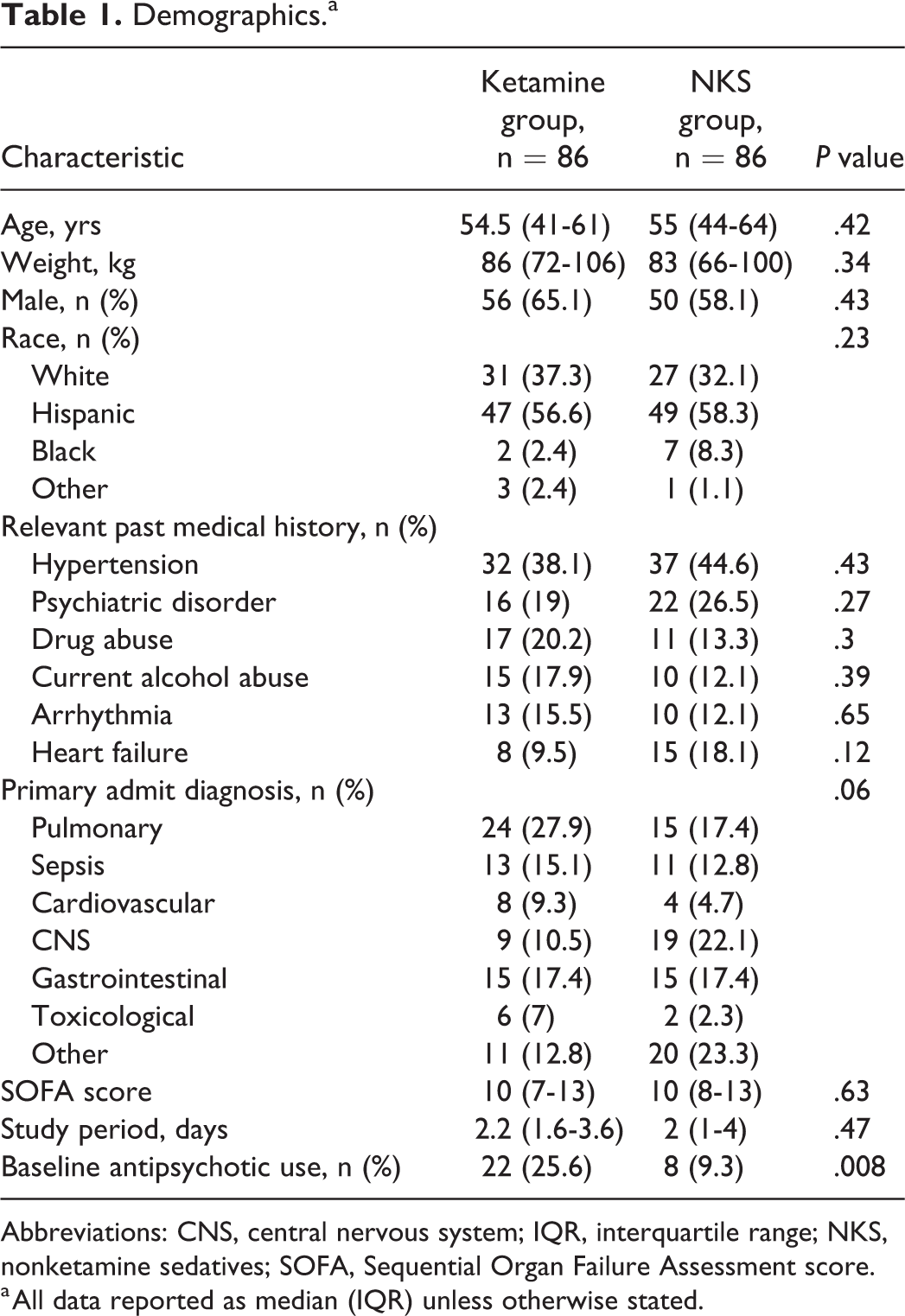
Abbreviations: CNS, central nervous system; IQR, interquartile range; NKS, nonketamine sedatives; SOFA, Sequential Organ Failure Assessment score.
a All data reported as median (IQR) unless otherwise stated.
Results of the ketamine versus NKS analysis are presented in Tables 2 and 3. There was no significant difference in the primary outcome of percentage of RASS scores at goal between ketamine and the NKS groups (78.7% vs 81.4%, P = .29). There was also no significant difference in the percentage of pain scores at goal, with both groups having a median of 100% at goal (P = .53). Median maximum MAP was not significantly different (103.2 vs 102.5 mm Hg, P = .71) nor was median maximum HR (103.8 vs 100 bpm, P = .34). Patients receiving ketamine had a longer ICU length of stay than patients on NKS (8.8 vs 5.2 days, P < .001).
Ketamine Versus NKS Outcomes.a
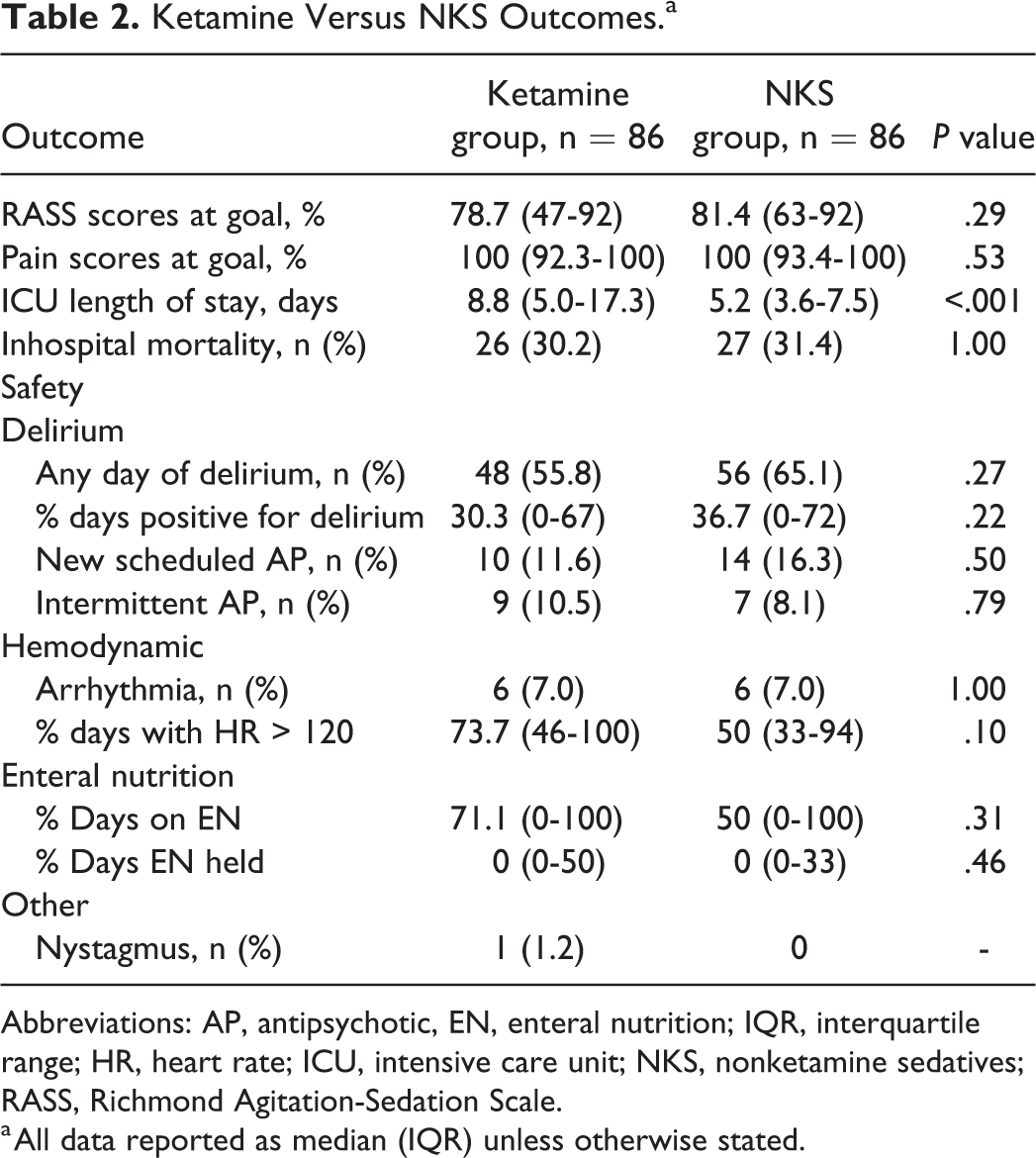
Abbreviations: AP, antipsychotic, EN, enteral nutrition; IQR, interquartile range; HR, heart rate; ICU, intensive care unit; NKS, nonketamine sedatives; RASS, Richmond Agitation-Sedation Scale.
a All data reported as median (IQR) unless otherwise stated.
Ketamine Versus NKS Concomitant Medications.a
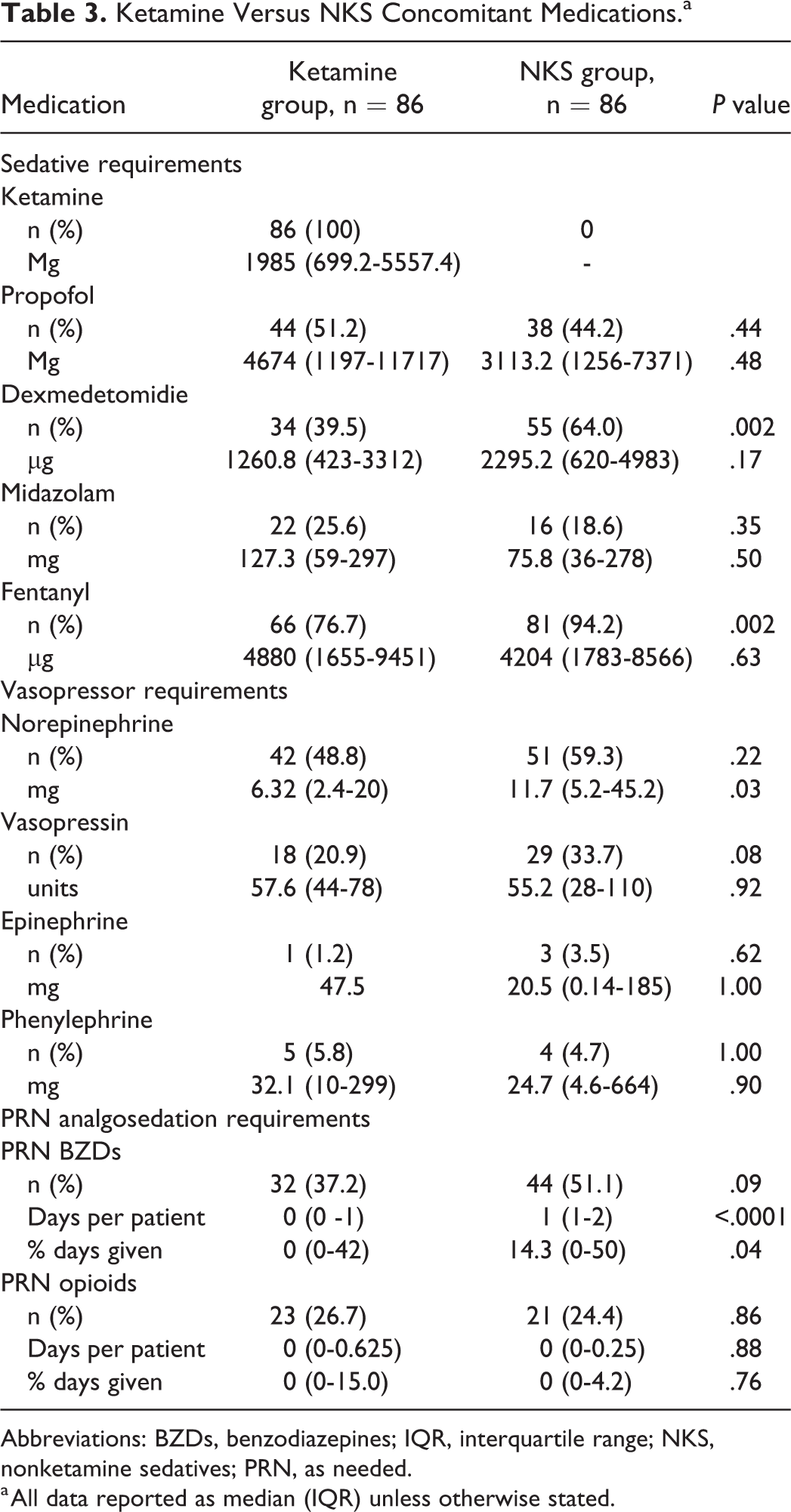
Abbreviations: BZDs, benzodiazepines; IQR, interquartile range; NKS, nonketamine sedatives; PRN, as needed.
a All data reported as median (IQR) unless otherwise stated.
Differences in concomitant sedative doses between groups were not statistically significant (Table 3). Ketamine was infused at a median rate of 7.9 μg/kg/min (interquartile range, 3.7-15.5 μg/kg/min) for a median of 2.25 days (interquartile range, 1.6-3.6 days). This median ketamine infusion rate was calculated as an average of the cumulative ketamine dose per patient over the duration infused. Fentanyl was the agent used most often in conjunction with ketamine. Though the ketamine group received higher fentanyl doses, only 76.7% of the ketamine group was on fentanyl compared to 94.2% in the NKS group (P = .002). Dexmedetomidine was more commonly used in the NKS group (39.5% vs 64%, P = .002), while a similar number of patients in both groups received midazolam and propofol. In all, 49% of the ketamine group and 59% of the NKS group received norepinephrine. The NKS group received almost double the norepinephrine in total (6.32 vs 11.7 mg, P = .03). Eighteen patients in the ketamine group and 29 in the NKS group received vasopressin, while only 4 and 9 in total received epinephrine and phenylephrine, respectively. The ketamine group received fewer days of intermittent benzodiazepines (0 vs 1 day, P < .0001).
Ketamine was not associated with an increase in number of patients with at least 1 day of delirium (56% vs 65%, P = .27); 12% of the ketamine group and 16% of the NKS group required new antipsychotic medications (P = .5). There was no difference in patients requiring intermittent antipsychotic medications (10% vs 8%, P = .79). Ketamine was not associated with an increase in the rate of arrhythmias, with 6 (7%) patients in both groups experiencing atrial fibrillation or atrial flutter. The percentage of days on which patients experienced tachycardia was also similar (74% vs 50%, P = .10). Patients on ketamine received EN on 71.1% of days compared to 50% in the comparator NKS group (P = .31) and there was no difference in the percentage of days on which EN was held. One patient in the ketamine group experienced nystagmus. Due to the retrospective nature of the study, we were unable to determine if adverse events were directly related to the sedatives used.
In the intrapatient analysis, percentage of RASS scores at goal increased from 66.7% to 72.1% following ketamine initiation but was not statistically significant (P = .43; Table 4). There was, however, a statistically significant improvement in pain scores at goal, though the median was 100% before and after ketamine initiation. Median maximum MAP was significantly higher following ketamine initiation (93 vs 100 mm Hg, P = .005). There was no significant difference in the doses of concomitant sedatives required.
Ketamine Group Baseline Versus on Ketamine.a
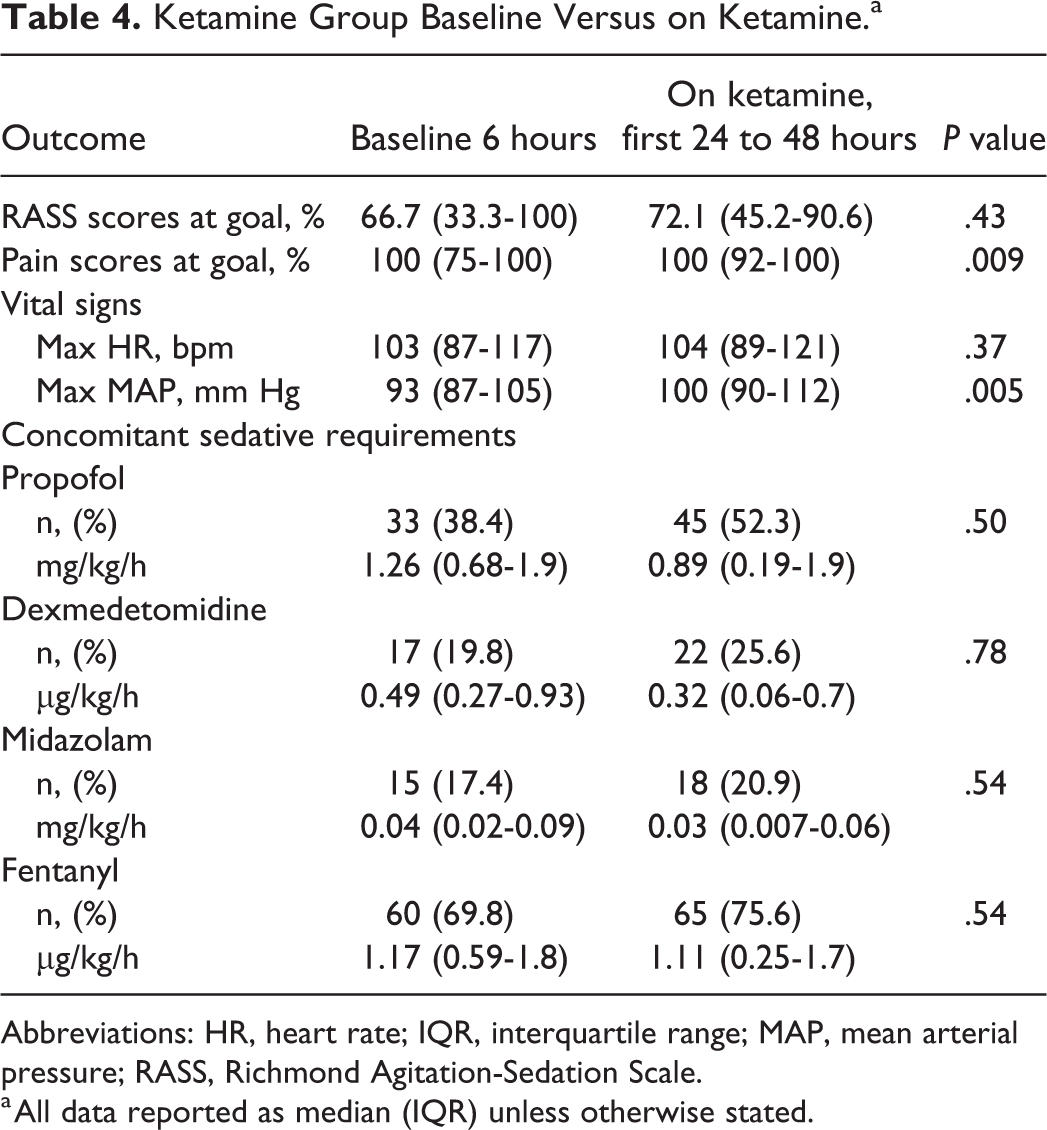
Abbreviations: HR, heart rate; IQR, interquartile range; MAP, mean arterial pressure; RASS, Richmond Agitation-Sedation Scale.
a All data reported as median (IQR) unless otherwise stated.
Though the reason for ketamine discontinuation was not consistently documented, the most common reason was extubation (n = 23), followed by weaning sedation (n = 21). No patients required discontinuation due to a tachyarrhythmia. Ketamine was discontinued for sinus tachycardia and hypertension in 2 and 3 patients, respectively. In 1 patient, ketamine was stopped due to psychosis. The most common reasons for discontinuation of the primary sedative in the NKS group were extubation (n = 44) and death (n = 20).
Discussion
Our study is the first to compare continuous infusion ketamine to alternative sedatives in MICU patients. In accordance with the 2018 PADIS guidelines, the majority of patients in both groups received fentanyl analgosedation, with propofol and dexmedetomidine being the next most commonly used agents. Relatively few patients overall received continuous infusion midazolam.
Ketamine did not improve the percentage of RASS scores at goal versus NKS or in the intrapatient analysis, though the intrapatient analysis was not powered to detect this difference. In our study, 72% of RASS scores were at goal (0 to −3) after ketamine initiation, which is consistent with major randomized controlled trials evaluating sedation and higher than seen in other ketamine studies.12-15 This may be explained by a broader goal RASS range in our study, which would make it easier to be within the specified goal before initiation of ketamine and more difficult for addition of ketamine to affect change. Our result aligns with a single-arm study of ketamine in trauma patients in which time at goal RASS (0 to −2 for most patients) was not significantly different before and after ketamine initiation. 16 In contrast, Garber and colleagues found time within goal RASS of −1 to +1 increased from 7.1% to 25% after ketamine initiation; however, this result may have been affected by the small percentage of patients at goal at baseline. 12
There was no significant difference in concomitant sedative doses between groups. However, fentanyl was used in almost 20% fewer patients in the ketamine group—a statistically and clinically significant difference. In our study, prescribing bias for use of ketamine in patients not adequately sedated with standard agents may have contributed to lack of difference found in concomitant sedative doses. Garber et al found a 20% relative decrease in concomitant analgesic and sedative doses at 24 hours following ketamine initiation, while Groetzinger et al found the addition of ketamine was associated with reduction or discontinuation of adjunctive sedatives in 63% of patients.12,13 In our study, the ketamine group received fewer overall days of benzodiazepines per patient. This reduction occurred despite a similar number of patients in both groups receiving continuous infusion benzodiazepines. These results were not seen in our intrapatient analysis, potentially due to the short 24 to 48 hours of follow-up period used for this comparison.
Ketamine is an attractive sedative due to favorable hemodynamic effects. The ketamine group required approximately half the norepinephrine amount during the treatment period. This result supports ketamine use in patients requiring vasopressors. Despite ketamine’s association with lower norepinephrine doses, there was no difference between groups in the median maximum MAP or HR. In the intrapatient analysis, there was a statistically significant, albeit not clinically significant, increase in maximum MAP from 93 to 100 mm Hg. Previous studies found ketamine may increase MAP and HR, but this effect was not consistent across all days of ketamine therapy.9,11
Ketamine has been associated with visual and auditory hallucinations, psychosis, and other psychomimetic effects as patients “emerge” from sedation. 6 Concern for psychosis and delirium has led to avoidance of ketamine in patients with a history of psychiatric disorders. 17 Ketamine was well tolerated in the 16 patients with psychiatric disorders included in the ketamine group. Only 1 patient with a history of posttraumatic stress disorder, major depressive disorder, and anxiety required discontinuation of ketamine secondary to severe agitation. While there are concerns ketamine may exacerbate delirium, Perbet et al found low-dose ketamine added to remifentanil significantly reduced incidence and duration of delirium compared to remifentanil plus placebo. 18 In the current study, ketamine did not increase the number of patients with delirium or number of days of delirium compared to nonketamine sedation. There was no difference between groups in use of new scheduled or intermittent antipsychotic medications. However, the ketamine group had significantly higher use of antipsychotics at baseline, which may have modified their risk of delirium. These medications were frequently continued during ICU admission but were not included in our assessment of “new” antipsychotics in order to better evaluate antipsychotic requirements secondary to ketamine effects.
A single-center retrospective study of 30 patients receiving ketamine sedation found a 13% rate of adverse events including arrhythmias and agitation. 19 In comparison, the overall adverse event rate in the ketamine group was 9.3% in our study. Six patients in both groups experienced arrhythmias. In the ketamine group, 5 patients had atrial fibrillation and 1 had narrow complex supraventricular tachycardia during the study period. All patients in the ketamine group who experienced an arrhythmia had a prior history of atrial fibrillation. There was no significant difference in the number of patients who experienced tachycardia or required antihypertensive medications.
One strength of this study is the evaluation of adjunctive ketamine sedation compared to a primarily nonbenzodiazepine comparator group, as avoidance of benzodiazepines for sedation is considered best practice. 7 Additional strengths include the focus on an MICU population with various comorbidities, similarity of groups at baseline, use of objective scoring systems for level of sedation and delirium assessment, and the comparison of patients at a similar time from ICU admission. Limitations include the retrospective design, small sample size, potential for missing documentation, and a broad goal RASS range. Confounding effects of concomitant sedatives and analgesics, including propofol and dexmedetomidine, may have decreased hemodynamic adverse effects, such as tachycardia and hypertension, that may occur with ketamine. In addition, we collected only 6 hours before ketamine infusion to serve as a baseline for current sedation and hemodynamics; this window could have been extended to 24 hours to allow for comparison of the same time period before and after ketamine initiation. While EN tolerance has been frequently evaluated in previous studies assessing ketamine use, we were not able to account for other reasons EN was held, including hemodynamic instability and gastrointestinal bleeding. We hypothesized that use of ketamine may improve EN tolerance due to decreased opiate requirements; however, this was not seen. An additional limitation is selection bias due to inability to control who received ketamine versus NKS only. At the study institution, ketamine is more commonly used in patients who are difficult to sedate due to underlying comorbidities or severity of illness. This may explain the difference in baseline antipsychotic use and overall ICU length of stay.
Conclusions
Addition of adjunctive ketamine to other continuous infusion sedatives was not associated with an increase in the percentage of RASS scores at goal. In comparison to patients on nonketamine sedation, there was an association between ketamine use and a lower requirement for continuous infusion fentanyl, dexmedetomidine, and intermittent benzodiazepines. Ketamine was well tolerated and not associated with an increase in delirium, arrhythmias, or tachycardia. Based on the results of this study, continuous infusion ketamine has potential as an adjunct for sedation in MICU patients, particularly in those who require vasopressor support. However, prospective randomized, controlled trials are needed to determine its optimal place in therapy for this patient population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.