
Abstract
Invasive fungal rhinosinusitis (IFRS) is a serious illness requiring early diagnosis, surgical debridement, and administration of antifungals. We report a case of an acute IFRS caused by Curvularia in a patient with diabetes mellitus. An 18-year-old female presented to the emergency department with an acute onset of fever, headache, facial discomfort, and a blood glucose reading of 500 mg/dL. The patient was admitted for the management of hyperosmolar hyperglycemia. Her past medical history includes uncontrolled type 1 diabetes mellitus and a recent toothache. A computed tomography scan of the facial maxillary region revealed sinus disease with bony erosion. Empiric therapy with liposomal amphotericin B 400 mg i.v. every 24 hours, piperacillin/tazobactam 4.5 g i.v. every 6 hours and vancomycin 1 g i.v. every 12 hours was started. A functional endoscopic sinus surgery revealed invasive rhinosinusitis and cultures were positive for fungal elements. The patient was discharged on liposomal amphotericin B 400 mg i.v. daily and cefuroxime 500 mg orally twice daily. However, she was readmitted for the management of acute kidney injury and was discharged on itraconazole capsules 200 mg orally twice daily. Sinus cultures grew Curvularia and itraconazole was prescribed for 6 weeks, but the patient discontinued treatment after 3 weeks and had no signs or symptoms of rhinosinusitis when she was last seen in the clinic. The possibility of IFRS should be explored in patients with diabetes and signs and symptoms of rhinosinusitis.
Introduction
Fungal rhinosinusitis encompasses a wide spectrum of immune and pathological responses, including invasive, chronic, granulomatous, and allergic disease. 1 Allergic fungal rhinosinusitis (AFRS) involves a hypersensitivity response to colonizing fungi and invasive fungal rhinosinusitis (IFRS) involves an aggressive infection. 2 IFRS is increasing in frequency due to the rise in the number of patients with altered immunocompetence. 2 IFRS can be classified as acute or chronic. 2 Acute IFRS has a rapid onset of signs and symptoms and usually occurs in patients with profound immunosuppression, whereas chronic IFRS has a more insidious onset and usually occurs in patients with a mild degree of immunosuppression. 2 The most common causative organisms are molds. 2 Acute infections are usually caused by Aspergillus, Fusarium, and the Mucorales such as Rhizopus and Mucor. 2 Chronic infections are usually caused by Aspergillus, Scedosporium, and the dematiaceous fungi such as Alternaria, Bipolaris, and Curvularia. 2 Diagnosis is based on histopathologic findings demonstrating fungal invasion of the tissues. 2 Treatment of IFRS involves surgical debridement and administration of antifungals targeted against the invading organism. 2
Curvularia belongs to a group of dark-walled fungi known as dematiaceous mold commonly found worldwide in the environment, particularly in soil and on plants in tropical and subtropical regions.3,4 Curvularia can cause a variety of human infections known as phaeohyphomycoses that can manifest as cutaneous and subcutaneous lesions, brain abscesses, AFRS, and IFRS.3-5 When these dematiaceous fungi infect tissues, they produce hyphae, pseudohyphae, or yeast-like elements. 6 While these infections have been reported in the immunocompetent host, fungemia and disseminated infections are more likely to occur in the immunocompromised host. 3 Risk factors for acquiring Curvularia infections include trauma, allergic rhinitis, diabetes mellitus, and altered immunocompetence. 3 IFRS caused by Curvularia is uncommon. 3 Diagnosis requires observation of the fungi invading tissue or recovery of the fungi from an otherwise sterile site. 3 Treatment usually involves surgical debridement and administration of antifungals such as amphotericin B deoxycholate, lipid preparations of amphotericin B, itraconazole, and voriconazole. 3 There are no universally accepted treatment options or clinical practice guidelines to guide clinicians in managing patients with this condition. Nonetheless, there have been some case reports in the literature describing successful treatment of fungal rhinosinusitis caused by Curvularia. If antifungal therapy is warranted, amphotericin B seems to be the agent of choice for life-threatening infections, whereas itraconazole is used for mild to moderate disease. 3 Voriconazole, posaconazole, isavuconazole, and caspofungin have shown in vitro activity against many of the dark-walled dematacious fungi and may be potential treatment options.3,7 We present the case of an 18-year-old woman with type 1 diabetes mellitus and IFRS caused by Curvularia and we reviewed similar cases published in the literature to assist pharmacists and other healthcare professionals in recognizing and managing this condition.
Case report
An 18-year-old African American female presented to the emergency department with an acute onset of fever (2 days), headache, facial discomfort, congestion, and a home blood glucose reading greater than 500 mg/dL. She denies sinus discharge and any prior episode of rhinosinusitis. Her past medical history is significant for type 1 diabetes mellitus and a recent toothache. The patient states that her type 1 diabetes mellitus is uncontrolled although she is taking insulin lispro 15 units subcutaneously 3 times a day before meals and metformin 500 mg by mouth twice daily to assist in weight management. Her height is 168 cm and her weight is 80 kg resulting in a body mass index of 28.3 kg/m2. She was admitted to the hospital for the management of hyperosmolar hyperglycemia, fever, and altered mental status changes. Her temperature upon arrival was 103°F, her other vital signs were stable, and her white blood cell count was 13,000 cells/mm3 (neutrophil 61%, lymphocyte 29%, monocytes 5%, eosinophils 4%, and basophils 1%). A urine drug screen was negative. A computed tomography (CT) scan of the facial maxillary region revealed complete opacification of the anterior and mid right ethmoid sinus air cells with osseous destruction, sinus disease, and bony erosion. Figure 1A shows an axial view demonstrating an opacified right maxillary sinus filled with thick material, focally invading the nasal septum. Figure 1B shows a coronal view of the aforementioned opacified sinus focally destroying the nasal septum. Blood cultures were obtained and empiric broad-spectrum antimicrobial therapy was initiated with liposomal amphotericin B (5 mg/kg) 400 mg i.v. every 24 hours, piperacillin/tazobactam 4.5 g i.v. every 6 hours, and vancomycin 1 g i.v. every 12 hours. Due to the abnormal findings on the CT scan, the patient underwent functional endoscopic sinus surgery (FESS) and a specimen was collected for pathology examination and microbiology cultures. Figure 2 shows the results of the histologic section of the right sinus contents demonstrating broad, irregular, septated, branching filamentous fungal hyphae. Blood cultures were negative, but preliminary sinus cultures were positive for coagulase negative staphylococci and negative for fungal elements. Liposomal amphotericin B and piperacillin/tazobactam were discontinued after 4 days of therapy. Vancomycin was continued to cover coagulase negative staphylococci and ceftriaxone 2 g i.v. every 24 hours was initiated to cover common upper respiratory tract infection organisms. Five days after collection, the sinus cultures revealed fungal hyphae. Intravenous antibiotics were discontinued and the patient was discharged on liposomal amphotericin B (5 mg/kg) 400 mg i.v. every 24 hours and cefuroxime 500 mg by mouth twice daily. However, 3 days later, the patient was readmitted for the management of acute kidney injury as evidenced by a rise in serum creatinine from 0.9 mg/dL to 1.8 mg/dL, and liposomal amphotericin B was discontinued as it was most likely the cause of the injury. Once the acute kidney injury resolved, liposomal amphotericin B was reinitiated in the hospital for 3 days and the patient was discharged home on itraconazole capsules 200 mg by mouth twice daily for 6 weeks.
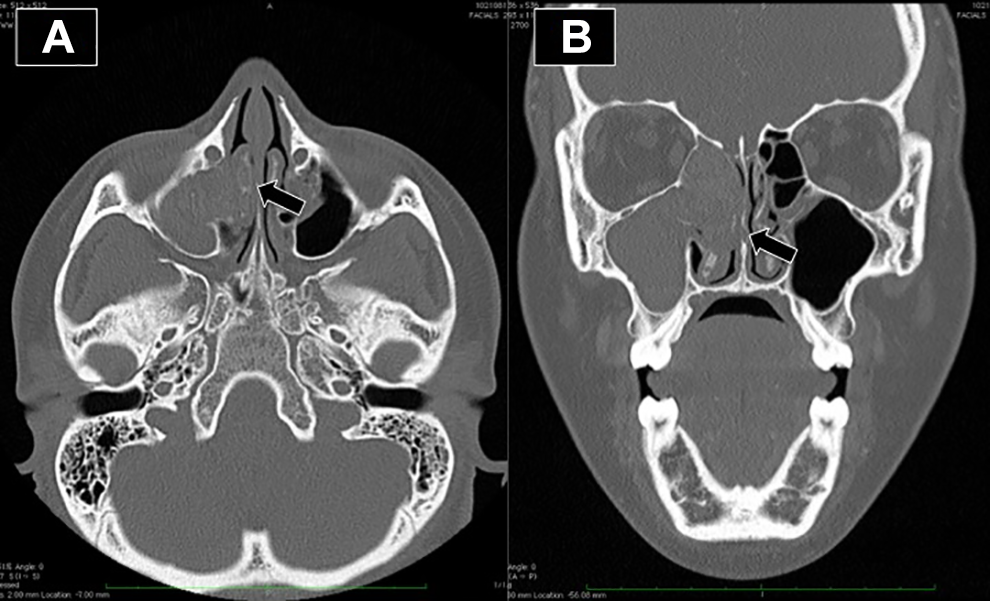
A. CT axial view demonstrating an opacified right maxillary sinus filled with thick material, focally invading the nasal septum (arrow). B. CT coronal view of the aforementioned opacified sinus focally destroying the nasal septum (arrow).
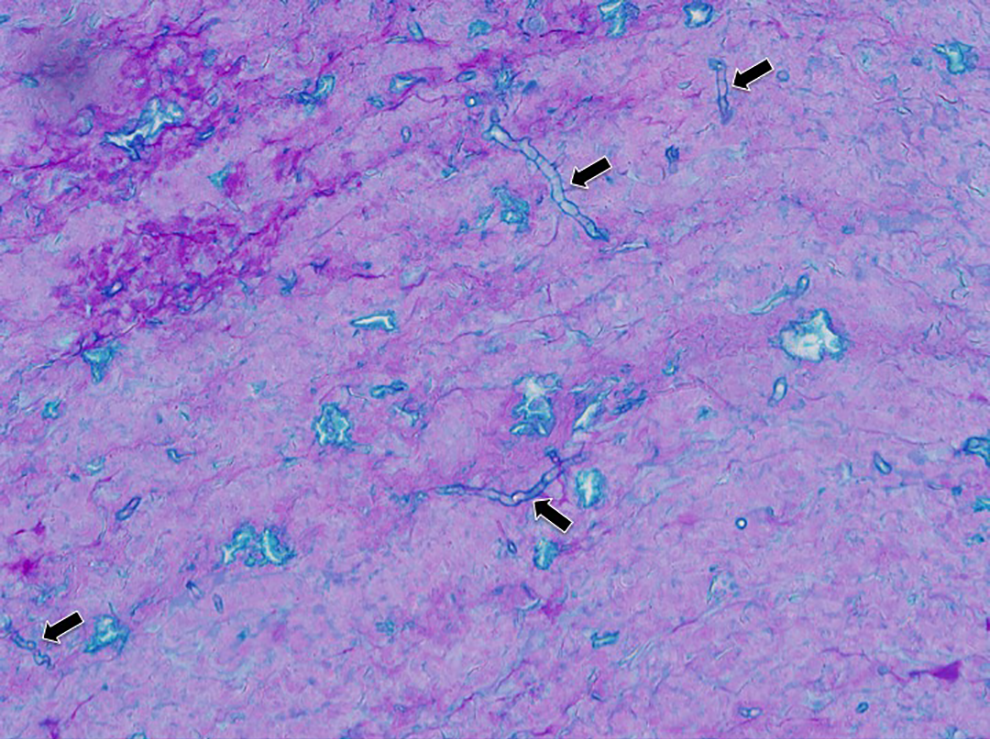
Histologic section of the right sinus contents demonstrating broad, irregular, septated, branching filamentous fungal hyphae (arrows), identified as Curvularia species on fungal culture (Periodic-Acid Schiff fungal stain, original magnification 200x).
Three weeks later, sinus cultures finally grew Curvularia, but the species was never identified. The patient was diagnosed with acute IFRS and was instructed to follow up with the infectious diseases physician in the outpatient clinic 1 week after discharge and until resolution of signs and symptoms. During the second visit, the patient revealed that she has stopped taking itraconazole after 3 weeks because of nausea and resolution of signs and symptoms of rhinosinusitis. The physician determined that the patient has significantly improved and itraconazole was no longer needed. There was no clear indication for repeat imaging.
Discussion
Curvularia can cause AFRS and IFRS.3-5 Diagnosis is based on imaging, pathology, and cultures. A CT scan or magnetic resonance imaging (MRI) usually displays sinuses filled with fluid and outward pressure on the bony sinus walls. 3 CT scans have higher sensitivity than MRI for detecting bony erosions, whereas MRI has higher sensitivity for soft tissue abnormalities. 8 Sinuses typically involved are the maxillary, ethmoid, sphenoid, and frontal. 3 When these molds are present in the culture, but not invading sinus tissues, surgical removal alone can be curative and antifungal therapy is not necessary. However, when there is evidence of tissue invasion, antifungal therapy is indicated in addition to surgery. 3 Although treatment options for Curvularia infections have not been universally accepted, surgical debridement is necessary to cure most patients and FESS is the most common surgical procedure in the case of rhinosinusitis.3,9 Table 1 is a summary of published case reports of invasive and allergic fungal rhinosinusitis caused by Curvularia.5,6,10-20 In the most recent published case of AFRS, a CT scan showed a heterogenous expansile mass in the right sphenoid sinus. 11 The patient underwent endoscopic sphenoidotomy and sinus cultures grew Curvularia. The patient was cured with surgical debridement and budesonide irrigation without antifungal therapy. This is an acceptable treatment strategy because the patient did not have IFRS like our patient and therefore did not require antifungal therapy. Topical corticosteroids are recommended for patients with AFRS. 21 In another recently published case of AFRS caused by Curvularia, the patient was treated with oral itraconazole 200 mg twice daily for 4 weeks, intranasal mometasone furoate spray 100 mcg twice daily for 6 months, and normal saline irrigation. 5 The patient was free of signs and symptoms of the disease after 2 months of treatment. This is an acceptable treatment strategy because the patient described, like our patient, had mild to moderate disease which can be successfully treated with itraconazole. In the most recent published case report of IFRS caused by Curvularia, the patient was immunocompetent. 6 The CT scan showed bilateral opacification of the maxillary sinuses and bony destruction of the lateral wall of the maxillary sinus. The patient underwent surgical debridement and was given amphotericin B 1.0 mg/kg i.v. daily; however, treatment was discontinued after 6 weeks due to lack of resolution of symptoms. The patient then received oral itraconazole 600 mg daily for 1 week followed by 400 mg daily. After 4 weeks of treatment, the patient reported improvement and was scheduled for facial reconstruction but did not show up to scheduled appointments and was further lost to follow up. This case report had the most similar treatment approach to our case as the patient underwent surgical debridement and received amphotericin B initially followed by oral itraconazole. Most case reports included in our search describe the use of amphotericin B, itraconazole, and terbinafine as treatment options, but the more recent case reports have shown improvement of signs and symptoms of rhinosinusitis with itraconazole. Although bone infections usually require a long duration of therapy, the patient described in our case report seemed to have responded to surgical debridement and a relatively short course of antifungal therapy. Repeat imaging and monitoring of inflammatory biomarkers would have been beneficial to document clinical cure.
Summary of Published Cases of Invasive and Allergic Fungal Infections Caused by Curvularia.
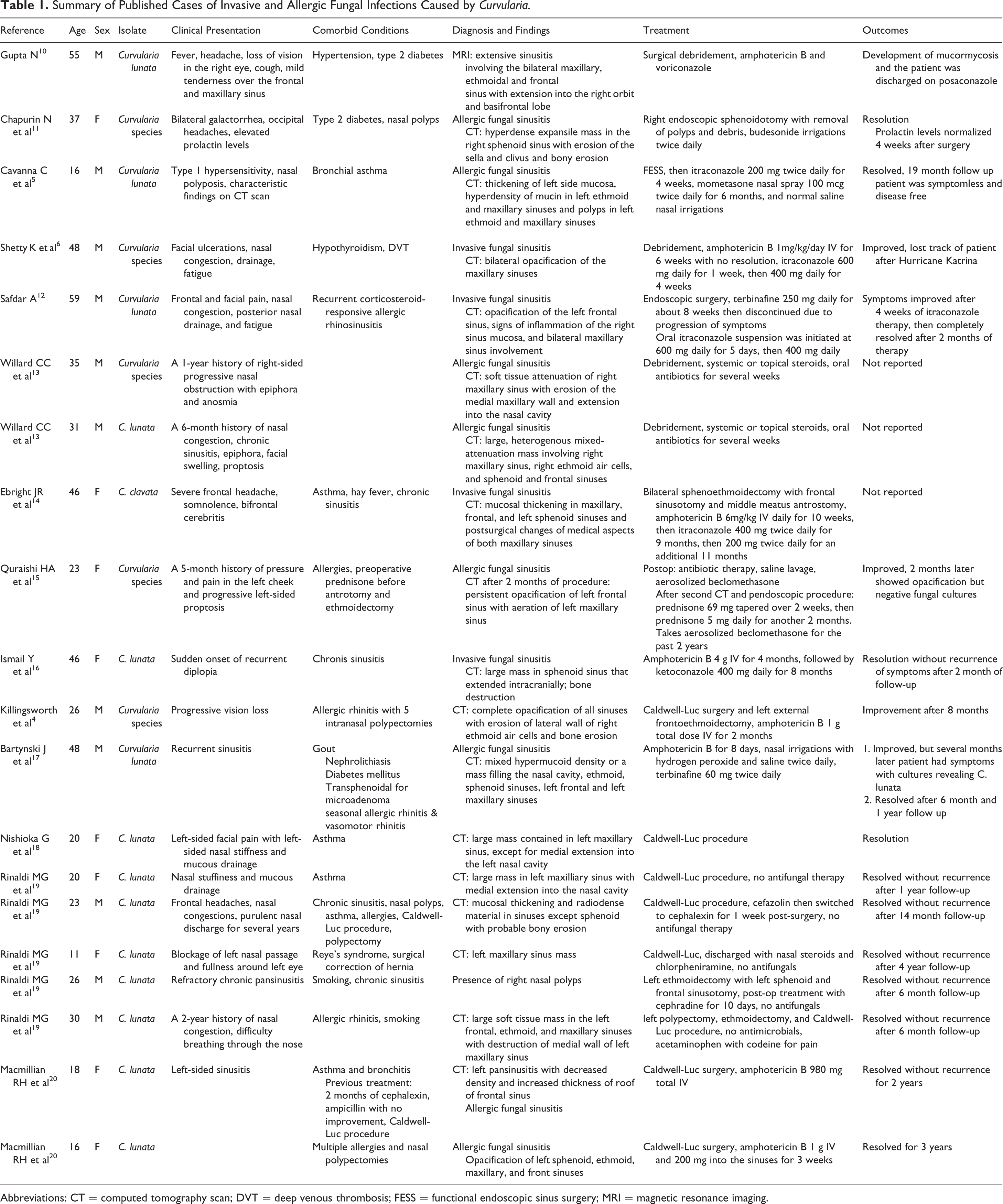
Abbreviations: CT = computed tomography scan; DVT = deep venous thrombosis; FESS = functional endoscopic sinus surgery; MRI = magnetic resonance imaging.
Conclusion
An 18-year-old woman with type 1 diabetes mellitus and IFRS was successfully treated with surgical debridement and intravenous liposomal amphotericin B for 1 week, followed by oral itraconazole for 3 weeks. The existing evidence supports this treatment strategy in immunocompetent patients with mild to moderate disease who respond quickly to oral azole antifungals. However, most patients require a longer duration of therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr. Chahine serves on the speakers’ bureaus of Merck & Co, Inc. and Paratek Pharmaceuticals, Inc. Drs. Marinucci and Bush have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.