
Abstract
Background:
Cannabidiol (CBD) serves as a promising medicine, with few known adverse effects apart from the potential of drug interactions with the cytochrome P450 system. It has been hypothesized drug interactions may occur with chemotherapeutic agents, but no supporting evidence has been published to date.
Case:
A 58-year-old female with a history of bilateral breast carcinoma in remission, was treated with tamoxifen for breast cancer prevention for over 6 years. CBD was instituted to treat persistent postsurgical pain, inadequately managed by alternate analgesics. It was postulated that CBD may diminish tamoxifen metabolism by CYP3A4 and 2D6 to form active metabolite endoxifen, which exerts the anticancer benefits. Endoxifen, tamoxifen, N-desmetyltamoxifen and 4-hydroxytamoxifen levels were collected while the patient chronically received CBD 40 mg/day, and after a 60-day washout. Upon discontinuation of CBD 40 mg/day, it was observed that endoxifen levels increased by 18.75% and N-desmethyltamoxifen by 9.24%, while 4-hydroxytamoxifen remained unchanged.
Conclusion:
CBD at a low dose of 40 mg/day resulted in the potential inhibition of CYP3A4 and/or CYP2D6. Patients receiving CBD and interacting chemotherapeutic drugs, such as tamoxifen, require monitoring to identify possible subtherapeutic response to treatment. Further pharmacokinetic studies are required to ascertain the dynamics of this drug interaction.
Introduction
Cannabis has gained increased acceptance as a medicine over the past few decades in Europe and North America, in particular for the treatment of symptoms stemming from gastrointestinal, neurological and psychological disorders.1-3 It has been theorized that tetrahydrocannabinol (THC) and cannabidiol (CBD) have the potential for significant drug interactions, complicating drug therapy in conditions such as cancer. 4
Unlike THC, CBD interacts more extensively with the cytochrome P450 system. As noted in several in vitro studies, CBD acts as an inhibitor of enzymes 2C9, 2C19, 2D6, 3A4 and also potentially inhibits or induces CYP 1A2 and 2B6 respectively.5-9 Here we present a case of a post-menopausal woman with a history of bilateral breast carcinoma on long term therapy with tamoxifen for breast cancer prevention. In this case, a reduction in metabolite N-desmethyltamoxifen and active metabolite endoxifen with chronic CBD use was observed. To our knowledge, this is the only clinical report in humans that potentially demonstrates a CYP3A4/5 and 2D6 drug interaction with chronic CBD administration with a chemotherapeutic agent.
Case Report
The case report involves a 58 year old Caucasian female with a history of fibromyalgia since the age of 21, bilateral wrist pain due to repetitive strain disorder since the age of 35, and a prolonged history of anxiety and depression for a period of more than 20 years.
At the age of 50, she was diagnosed with cancer of the right breast, with a grade 2, ER/PR (+), HER-2 (-) tumor without lymph node involvement (Stage IIA-T2, N0, M0). Shortly after adjuvant chemotherapy with dose dense doxorubicin-cyclophosphamide and paclitaxel [AC-PACL(DD)] for the right breast, left sided breast cancer was detected upon MRI, which showed a grade 2 invasive ductal carcinoma that was ER/PR (+), HER-2 (-) (Stage IIA-T1, N1, M0). Due to the close temporal proximity to which the left sided breast cancer was detected after detection of the right sided breast cancer, the originally scheduled course of adjuvant AC-PACL(DD) chemotherapy remained the same. Upon completion of adjuvant chemotherapy, the patient underwent double mastectomy with reconstruction. After these treatments, she remained in remission, however she developed persistent post-surgical pain in her chest after reconstructive surgery. The patient was placed on tamoxifen 20 mg daily for 5 years from 2011-2016 for breast cancer prevention, with a subsequent switch to letrozole in 2016. Letrozole was not tolerated due to adverse effects, therefore tamoxifen therapy was re-initiated for an additional 5-year course.
The patient’s pain management regimen traditionally consisted of opioid therapy, and her total morphine equivalent dose was at or above 690 mg/day for several years. Previous attempts at adding other non-opioid analgesics had failed, which included gabapentinoids and tricyclic antidepressants. A trial with duloxetine was not initiated, due to a relative contraindication with tamoxifen therapy, as duloxetine is a CYP2D6 inhibitor capable of reducing the production of active metabolite endoxifen.
A trial with medical cannabis was considered to reduce overall opioid drug burden and neuropathic pain symptoms. A medical prescription was sent to a licensed Canadian medical producer of cannabis, which issued a concentrated oil consisting of approximately 20 mg/mL of cannabidiol (CBD) and 2 mg/mL of tetrahydrocannabinol (THC). The dose was gradually up titrated weekly starting in February 2018 by 0.1 mL (2 mg of CBD and 0.2 mg of THC), to a dose of 1 mL (20 mg of CBD and 2 mg of THC) twice daily over the course of several months. The patient used a total of approximately 40 mg of CBD and 4 mg of THC orally per day from March 2018 to July 2018.
In July 2018, upon a medication review by the clinic pharmacist, a potential interaction was noted in literature, whereby CBD may act as a strong CYP2D6 inhibitor. 9 The patient was informed that the use of CBD may lower the degree to which tamoxifen is metabolized to active metabolite endoxifen, thereby potentially reducing its anticancer benefits. The patient consented to have lab work performed, and blood levels were drawn a week later in the early afternoon and sent to Quest Diagnostics ™ in San Juan Capistrano, California for analysis. The blood draw revealed that her serum endoxifen level was 16.00 ng/mL (6.01-43.19 ng/mL), N-desmethyltamoxifen 119.00 ng/mL (2.59-373.96 ng/mL), 4-hydroxytamoxifen level was 1.00 ng/mL (0.24-5.05 ng/mL) and tamoxifen 70.00 ng/mL (12.54-233.07 ng/mL); Table 1.
Impact of Cannabidiol on Tamoxifen Metabolism.

Despite demonstrating a therapeutic level of endoxifen, the clinical team wished to explore the impact of CBD on tamoxifen metabolism further and evaluate whether discontinuation of CBD would increase endoxifen levels. As the half-life of CBD and their metabolites range from approximately 41-113 hours, 10 the patient was advised and consented to go through a thorough washout of at least 25-30 days (5 to 6 half-lives) and have tamoxifen and endoxifen levels repeated. During this time, she primarily used acetaminophen, ibuprofen and opioids for pain management.
At follow-up in February 2019, the patient discontinued her cannabis oil and went through a washout for a period of 67 days. A repeat serum blood sample was taken at the same time of day as the previous blood sample, and sent to Quest Diagnostics™. The resulting blood sample revealed increased serum levels of endoxifen 19.00 ng/mL (6.01-43.19 ng/mL), N-desmethyltamoxifen 130.00 ng/mL (2.59-373.96 ng/mL), and tamoxifen level of 75.00 ng/mL (12.54-233.07 ng/mL), but an unchanged level of 4-hydroxytamoxifen 1.00 ng/mL (0.24-5.05 ng/mL), as compared to when the patient was receiving CBD 40 mg/day. The withdrawal of CBD 40 mg/day resulted in an 18.75% increase in endoxifen, 9.24% increase in N-desmethyltamoxifen whereas no discernable increase or decrease was found with 4-hydroxytamoxifen (Table 1).
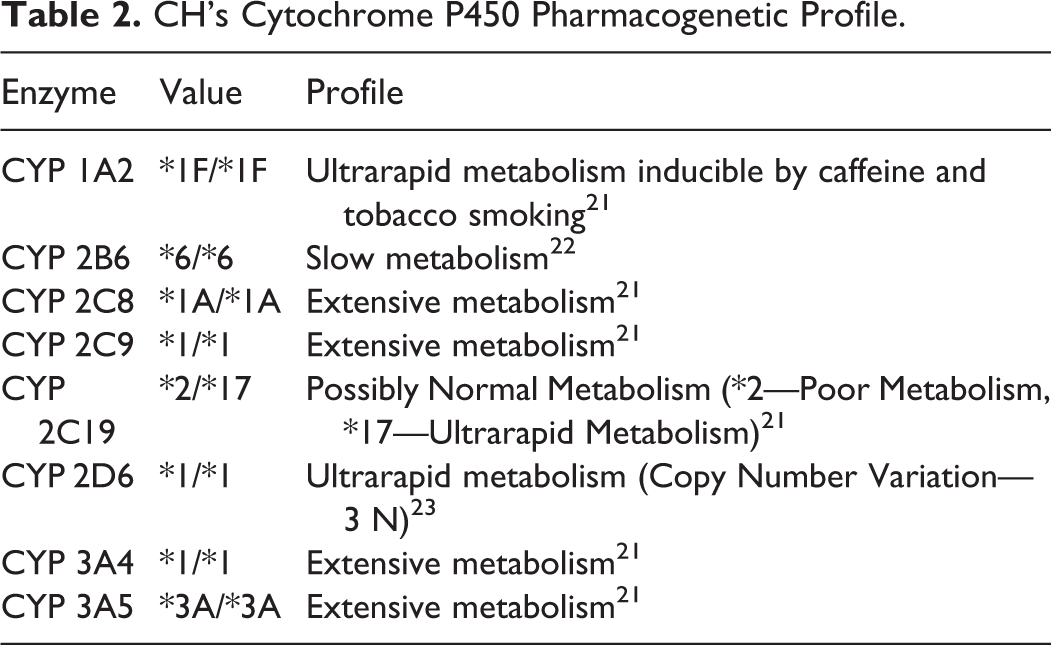
As the patient’s endoxifen level was still above its respective therapeutic thresholds for efficacy, the supervising physician re-initiated the prescription for medical cannabis. In order to determine the patient’s intrinsic CYP2D6 enzyme function and its influence on the drawn serum samples, a pharmacogenetic test was ordered using a cheek swab kit from Geneyouin® Inc, Toronto, Canada. It was determined from this pharmacogenetic test, that the patient is an ultra-rapid metabolizer for CYP 2D6 (*1/*1), as she possessed a copy number variation (multiple copies of this gene), and is an extensive metabolizer for CYP 3A4 (*1/*1). Table 2 lists the patient’s complete pharmacogenetic profile of cytochrome P450 enzymes measured.
CH’s Cytochrome P450 Pharmacogenetic Profile.
After disclosure of the pharmacogenetic report to the patient, she was approached and provided written consent to have her medical information utilized, in the publication of this case report.
Discussion
The metabolism of tamoxifen undergoes 2 pathways involving 2 separate steps to formulate endoxifen (Figure 1). The major metabolic pathway, which accounts for approximately 90% of tamoxifen metabolism, involves a first step by CYP3A4/5 which metabolizes tamoxifen to N-desmethyltamoxifen.11,12 The patient’s levels of N-desmethyltamoxifen increased by 9.24% when CBD was withdrawn, indicating CBD had an inhibitory effect on CYP3A4/5. This finding has been validated with a recent pharmacokinetic study of CBD on clobazam metabolism. 13
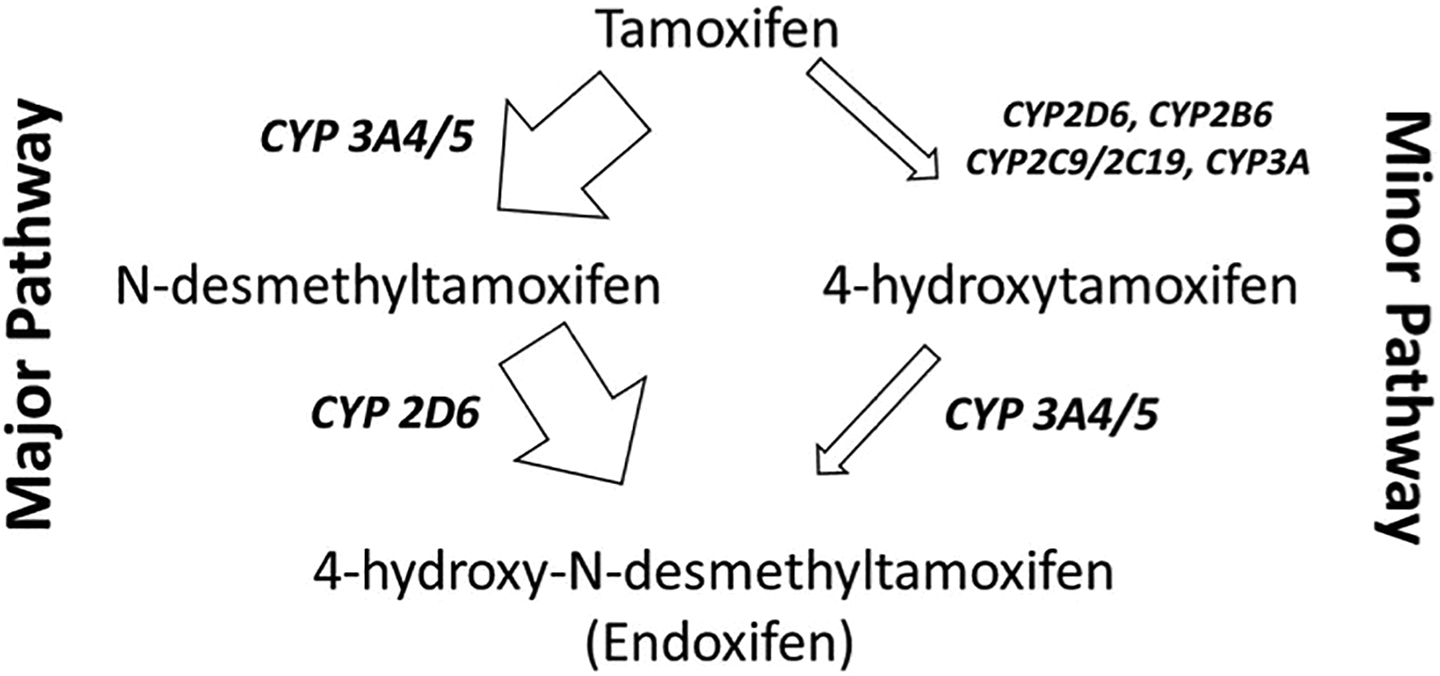
Major and Minor Pathways of Tamoxifen Metabolism by Cytochrome P450 Enzymes.
The second step of this major pathway involves metabolism of N-desmethyltamoxifen to endoxifen by CYP2D6, which increased by 18.75% upon withdrawal of CBD, indicating a potential inhibitory role of CBD on CYP2D6 activity. This result potentially validates a previous theoretical study, that demonstrated that CBD is a CYP2D6 inhibitor. 9
The minor pathway’s first step involves CYP2D6 metabolism (along with lesser contribution of other CYP P450 enzymes), metabolizing tamoxifen to 4-hydroxytamoxifen. Regardless of CBD exposure, no apparent changes were noted in 4-hydroxytamoxifen levels. This may partly be explained by the fragmented contribution that both CYP2D6 and CYP3A4/5 have in metabolizing tamoxifen to 4-hydroxytamoxifen, as other CYP P450 enzymes are involved in this process as well. 12 The second step of this minor pathway involving CYP3A4/5 may have been influenced by CBD, as upon withdrawal of CBD, greater endoxifen levels were noted, however the exact contribution of this reaction is confounded by the influence of the major pathway.
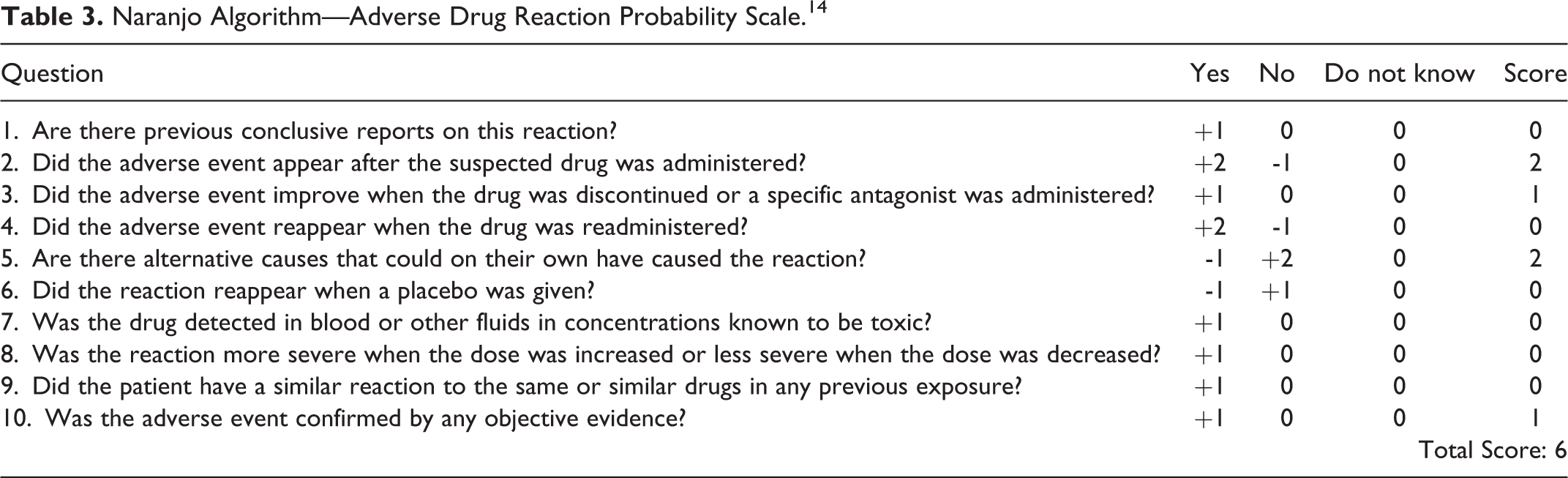
A Naranjo adverse drug reaction probability scale score of 6 was obtained, indicating a probable role that CBD contributed to CYP3A4/5 and CYP2D6 inhibition and resulting decreased endoxifen production (Table 3). 14 For CBD to have been categorized as having a definitive role (score been greater than 8) in this drug interaction, re-exposure to either a higher dose of CBD with corresponding greater inhibition of endoxifen production, or lower dose of CBD with corresponding lesser inhibition of endoxifen production, would need to occur.
Naranjo Algorithm—Adverse Drug Reaction Probability Scale. 14
It cannot be ascertained from these results, the strength of CYP3A4/5 or CYP2D6 inhibition. A strong CYP 3A4/5 inhibitory effect would have resulted in a bottleneck in the first step of the major pathway, with elevated tamoxifen levels with exposure to CBD. Paradoxically, tamoxifen levels were slightly greater after CBD withdrawal. Similarly, an accumulation of N-desmethyltamoxifen would have occurred if there was strong CYP2D6 inhibition by CBD, however this was not observed as well. Based on these results, it is possible that the inhibitory effect of CBD on both CYP3A4/5 and CYP2D6 is either weak at this current dose and/or relatively equal as compared to one another, resulting in a lack of observed bottlenecking effect of parent drug and intermediate metabolite.
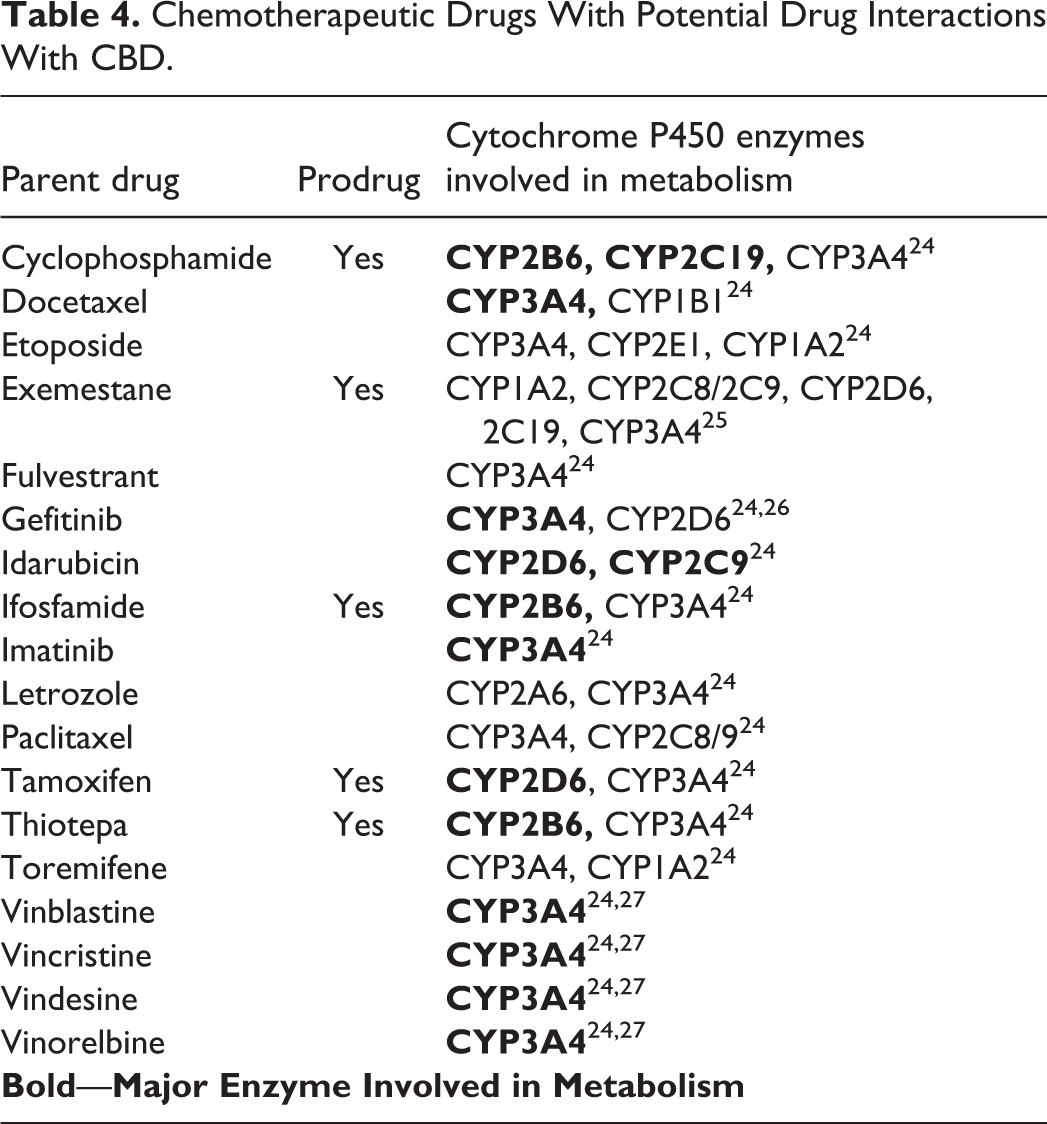
As CBD is being utilized more commonly as a therapeutic agent to treat cancer pain, the potential for drug interactions with other anticancer agents is highly probable. 4 In the case of this patient, the significance of this interaction was not clinically relevant, as the patient possessed an ultra-rapid metabolic profile (CYP 2D6 *1/*1 copy number variation—3 N), which resulted in therapeutic endoxifen levels despite the presence of CBD inhibition of CYP2D6 and 3A4/5. However, the potential for a CYP2D6 interaction with CBD may be particularly meaningful if a patient possesses an intermediate or poor CYP2D6 metabolic profile. A patient with this profile would intrinsically have a greater risk of subtherapeutic endoxifen levels. Adding CBD in such a case, would further reduce tamoxifen metabolism, which may lead to an enhanced risk of breast cancer recurrence. 15 It is noteworthy that the total daily of dose of 40 mg per day of CBD that this patient was using was considerably smaller than that which is administered for the treatment of pediatric epilepsy disorders, which can exceed >750-1500 mg/day.16-19 It is conceivable that with markedly greater CBD exposure, a greater degree of CYP2D6 and CYP3A4/5 inhibition would be observed resulting in potential therapeutic failure with tamoxifen treatment. In addition to tamoxifen, a series of other chemotherapeutic agents may be influenced by CBD induced CYP 3A4/5 or CYP 2D6 inhibition (summarized in Table 4). With CBD exposure, it is conceivable that active chemotherapeutic parent drugs metabolized by these enzymes to inactive compounds, would lead to accumulation of active drug and thus cause a supratherapeutic response and/or toxicity. Similarly, for inactive parent drugs that require CYP 3A4/5 or CYP 2D6 for metabolism into active metabolites, the possibility of decreased biotransformation would potentially lead to therapeutic failure at standard doses.
Chemotherapeutic Drugs With Potential Drug Interactions With CBD.
There were several limitations to this case report. In particular, medical cannabis products in Canada do not possess CBD alone, but possess many other cannabinoids as they are whole plant extracts from the cannabis plant. 20 Therefore the presence of these other cannabinoids may have had an interaction potential with tamoxifen as well, confounding our findings. Additionally, this case report assessed one individual with a collection of only 2 serum samples. In order to validate these findings, ideally a pharmacokinetic study involving several participants receiving tamoxifen, prior to and after exposure to variable doses (low, medium and high) of CBD would be required to assess the reproducibility of these findings as well as the dose response relationship between CBD and CYP3A4/5 and CYP2D6 inhibition.
Conclusion
Cannabidiol has the potential to inhibit CYP3A4 and CYP2D6, when administered long term orally in small doses (<50 mg/day). If CBD is utilized concurrently with chemotherapeutic agents, careful consideration should be given regarding appropriateness of instituting CBD therapy in light of other unknown clinical drug interactions that may impact treatment course and enhance adverse effects. Further pharmacokinetic studies are warranted to evaluate the inhibitory role CBD has on CYP2D6 and CYP3A4 to validate the findings presented in this case.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.