
Abstract
Drug-induced liver injury has been reported to cause up to 10% of adverse drug reactions in the United States. Risk factors for druginduced liver injury include female gender, older age, interacting medications and drugs that are metabolized by the liver. This case report describes a patient who was newly initiated on tizanidine, an alpha2 adrenergic agonist used for muscle spasm and musculoskeletal pain, and bortezomib, a proteasome inhibitor used for multiple myeloma. Both medications are metabolized by cytochrome P450 isoenzyme 1A2. The medications were suspected of causing acute hepatitis based on the timing of their initiation and evidence to suggest that they can cause acute hepatitis. The Naranjo adverse drug reaction scale was scored as possible. In addition, the drugs’ blood levels may have been increased by acyclovir and hydralazine, both inhibitors of cytochrome P450 isoenzyme 1A2. A dilemma for the team was how to best manage bortezomib. It is part of first line treatment for multiple myeloma when combined with lenalidomide and dexamethasone. Other proteasome inhibitors are available for multiple myeloma treatment. When starting chemotherapy, it is important to be aware of medications that cause a rise in liver enzymes, potential drug interactions, and how best to manage the clinical consequences.
Introduction
Drug-induced liver injury (DILI) has been reported to cause up to 10% of adverse drug reactions in the United States. 1 Risk factors for DILI include female gender, older age, interacting medications, and drugs that are metabolized by the liver. DILI, including drug-induced hepatitis, is challenging to diagnose and identify the causative agent. 1 Most importantly, DILI can result in severe toxicity and complications if not managed appropriately. Many medications have been linked to drug-induced hepatitis, including over-the-counter medications such as acetaminophen, 3-hydroxy-3-methyl-glutaryl-CoA reductase inhibitors, antibiotics including sulfonamides and amoxicillin-clavulanate, and chemotherapy medications. 2 This case report describes an adverse event of acute hepatitis that occurred post-administration of the newly initiated medications bortezomib and tizanidine. Bortezomib is a proteasome inhibitor utilized as a first line treatment of multiple myeloma (MM).3,4 Tizanidine is an alpha2 adrenergic agonist used for muscle spasm and musculoskeletal pain. 5 Both drugs are metabolized hepatically via several cytochrome P450 (CYP) pathways including isoenzyme CYP1A2.3,5
A 74-year-old black female, height 173 centimeters, weight 63.6 kilograms, body surface area 1.75 kg/m2 was admitted to the hospital with ongoing back pain and a past medical history of hypertension, atrial fibrillation, and vertigo. Medical problems and medications prior to and during hospitalization are described in Table 1. A computed tomography scan showed a superior endplate fracture of T12, as well as at L2 and T11, and evidence of central stenosis at L4-5, where end-stage lumbar degenerative disc disease and a grade 1 spondylolisthesis were present. Kappa and lambda light chains were normal with only a slightly decreased kappa/lambda ratio. The patient’s clinical picture of anemia, mild chronic kidney disease, diffuse osteopenia with compression fracture, slightly elevated total protein in her serum and rouleaux formation on peripheral blood smear was consistent with the diagnosis of MM. Bone marrow aspirate and biopsy were completed confirming MM. The patient was subsequently ordered bortezomib, lenalidomide, and dexamethasone (VRd). The patient was administered bortezomib for the MM starting on day 16 of the hospitalization (bortezomib 1.3 mg/m2 subcutaneously on days 1,4, and 8). Dexamethasone was administered starting on day 16. Lenalidomide was delayed and subsequently not administered due to patient’s reduced renal function and risk evaluation and mitigation strategy program requirements. Tizanidine 2 mg, by mouth, dosed 3 times daily was initiated on day 14 of hospitalization. Lab results during the hospitalization included normal iron levels, normal vitamin B12 and folate levels, mildly elevated creatinine on admission (estimated creatinine clearance between 35-40 mL/minute) that improved during the hospitalization, and normal liver enzymes during the initial part of the hospitalization that increased on day 19 (Table 2). On Day 19, increased alanine aminotransferase (ALT) (23 units/L to 806 units/L) and aspartate aminotransferase (AST) (22 units/L to 579 units/L) levels (Figure 1) were reported with a normal total bilirubin. The patient’s INR was slightly elevated from the normal range but decreased from admission. The albumin level was not significantly changed from the patient’s admission level (Table 2). Patient did not have any symptoms of acute hepatitis, such as nausea and vomiting, except for fatigue. During physical exam, the patient’s abdomen was non-tender, non-distended with normal bowel sounds with no evidence of guarding, hepatosplenomegaly, and rebound. A liver ultrasound showed hepatitis steatosis. Bortezomib was given 1-time 3 days prior to the rise in liver enzymes and was not administered again because of the increase in ALT and AST levels. Tizanidine was started 5 days prior to the rise in liver enzymes and stopped on Day 19. After the discontinuation of the bortezomib and tizanidine, the AST and ALT subsequently trended toward the upper range of their normal limits over the next week. Additional laboratory tests were completed to rule out other causes of increased liver enzymes (Table 2).
Medical Problems and Medications Prior to and Upon Admission to the Hospital.
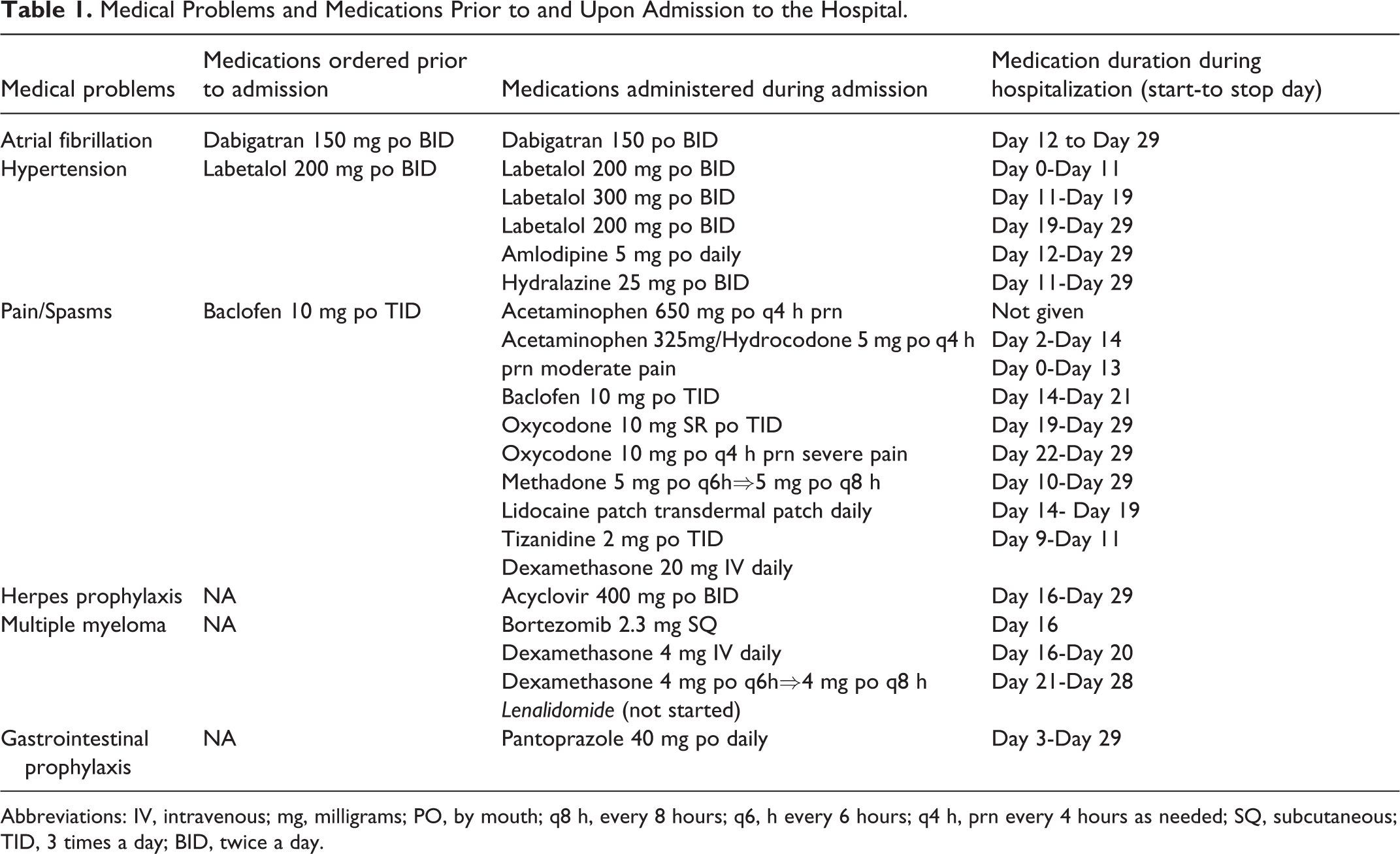
Abbreviations: IV, intravenous; mg, milligrams; PO, by mouth; q8 h, every 8 hours; q6, h every 6 hours; q4 h, prn every 4 hours as needed; SQ, subcutaneous; TID, 3 times a day; BID, twice a day.
Critical Laboratory Values.
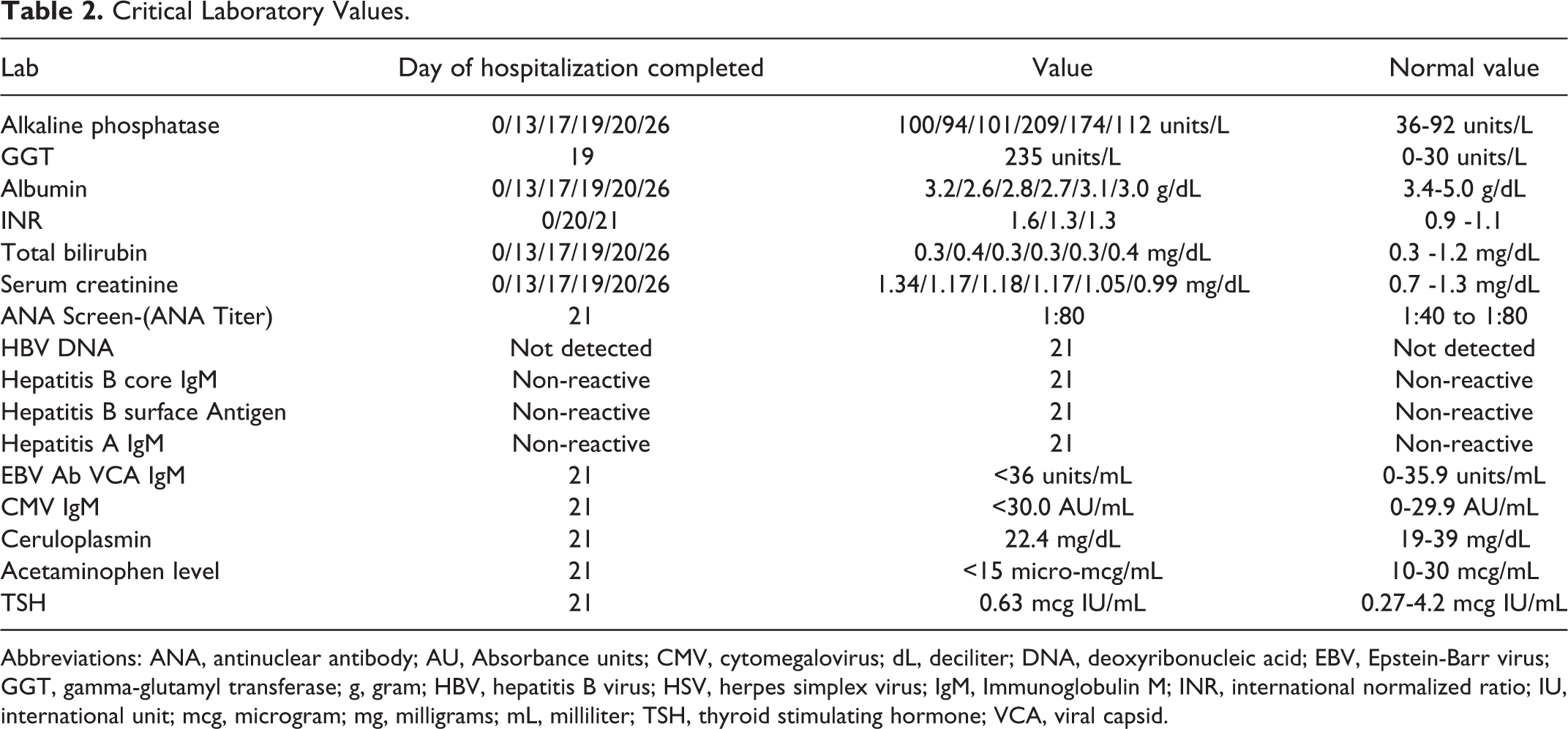
Abbreviations: ANA, antinuclear antibody; AU, Absorbance units; CMV, cytomegalovirus; dL, deciliter; DNA, deoxyribonucleic acid; EBV, Epstein-Barr virus; GGT, gamma-glutamyl transferase; g, gram; HBV, hepatitis B virus; HSV, herpes simplex virus; IgM, Immunoglobulin M; INR, international normalized ratio; IU, international unit; mcg, microgram; mg, milligrams; mL, milliliter; TSH, thyroid stimulating hormone; VCA, viral capsid.
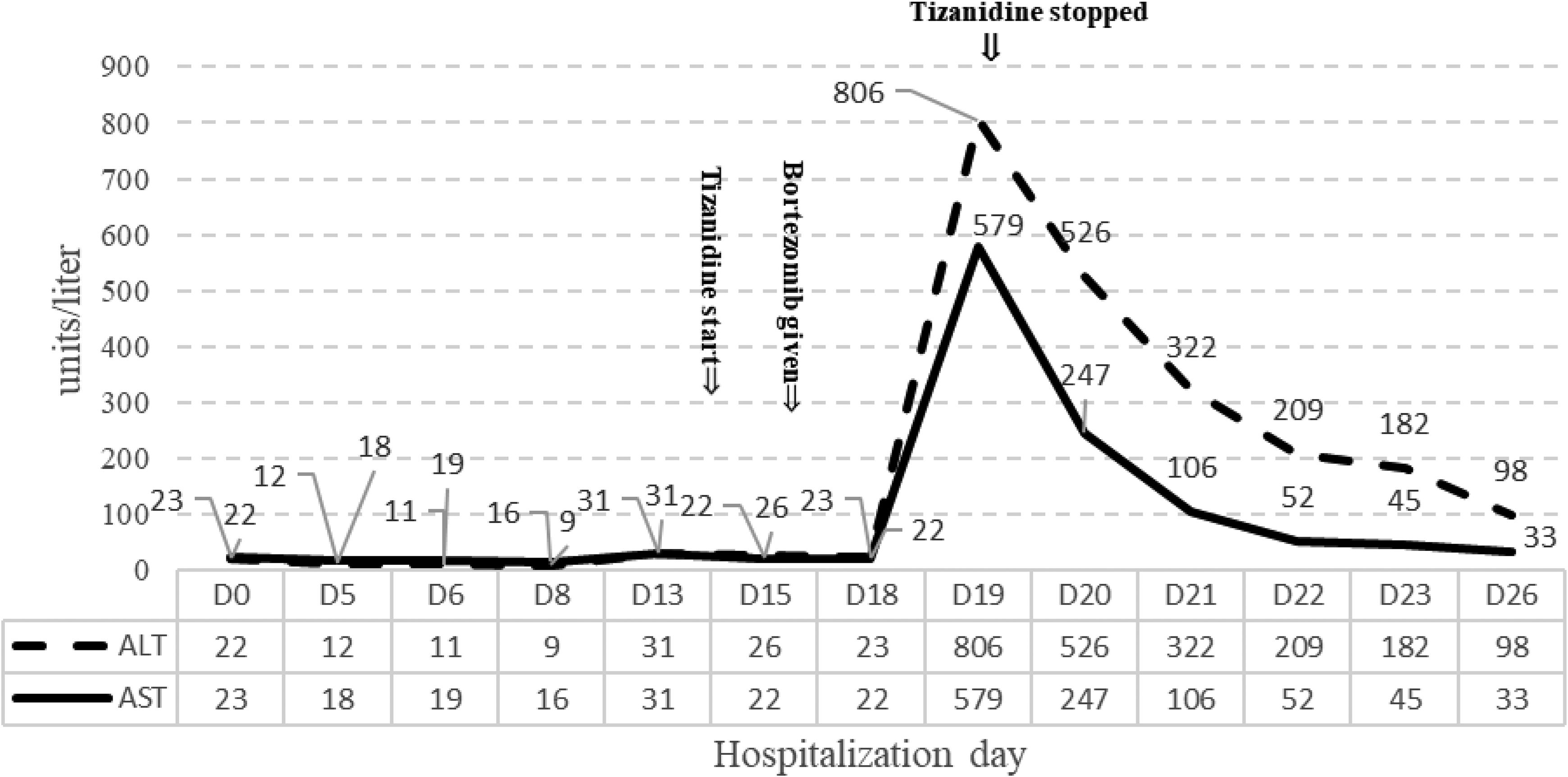
Change in ALT, AST (units/liter).
Discussion
Tizanidine’s common adverse effects are dry mouth (49%), somnolence (48%), and asthenia (16%). 5 The central nervous system (30-40%), hematological system (30-40%), and gastrointestinal tract (20-30%) are the organ systems with the most common adverse effects from bortezomib. Other adverse effects for bortezomib include fatigue (25%), rash (11%), and pyrexia (16%). 3 There is evidence that both tizanidine6-8 and bortezomib9-11 increase liver enzymes. Significant increases in serum ALT 3 times the normal limit has been documented for tizanidine in ∼5% of patients taking the drug. 8 Previous tizanidine and bortezomib case reports show that the patient had an increase in AST and ALT within 5-7 days.6-8,10,11 A patient who was accidentally re-challenged with 1 dose of tizanidine 4 mg, weeks after tizanidine had been discontinued because of an increase in LFTs, had a rise in ALT to greater than 3 times the normal limit within 6 days. 8 The patient in this case had a rise in liver enzymes 3 days post administration of bortezomib and 5 days after starting tizanidine (Figure 1). Tizanidine was discontinued on the day the liver enzymes began rising. Many of the medications the patient was receiving have been documented to cause increased liver enzymes including amlodipine, baclofen, dabigatran, hydralazine, labetalol, and pantoprazole.12-20 As noted in Table 1, the patient was taking baclofen, dabigatran, and labetalol at home prior to admission. The baclofen was discontinued 6 days prior to the rise in liver enzymes. Thus, it was unlikely to be the cause of the increase in the liver enzymes. In addition, amlodipine, dabigatran, hydralazine, and labetalol were not considered a primary cause in the rise of the liver enzymes since these medications were continued until the patient was discharged, which was after there was a decline in ALT and AST levels. After the elevation on Day 19, the ALT and AST levels gradually decreased over the next 7 days and were trending towards normal limits. Based on the timeline of events and clinical course, tizanidine seems to be the most likely cause of the rise in liver enzymes, although bortezomib cannot be ruled out. In addition, both tizanidine and bortezomib are metabolized by CYP 1A2 and may have had their levels increased by inhibition of their metabolism by acyclovir (a weak CYP1A2 inhibitor) and/or hydralazine (a moderate to strong CYP1A2 inhibitor).21-23 There are potential alternative causes of increased liver enzymes including herbal products, over the counter agents including acetaminophen, prescription medications, alcohol, viral hepatitis (B, C, D), Epstein Barr virus, autoimmune disease, Wilson’s disease, alpha-1 antitrypsin deficiency, celiac disease, and thyroid disease. 24 Each of the other potential causes of acute hepatitis were excluded by physical exam, patient history, an imaging study and laboratory values (Table 2). Applying the Naranjo adverse drug probability scale to this case, a score of 4 was obtained, indicating possible reaction of tizanidine and/or bortezomib causing the increased liver enzymes. 25 Risk factors that may have contributed to the risk in liver enzymes in this patient include female gender and advanced age. 1 Interacting medications that inhibit the metabolism of tizanidine and bortezomib may have been another contributing factor. 1
Management of the patient’s increased liver enzymes involved several treatment decisions. Bortezomib and tizanidine were discontinued because they represented the most likely causes of the patient’s elevated liver enzymes. Removing bortezomib and treating the patient with a 2-drug regimen such as lenalidomide and dexamethasone (Rd) was an option. However, this regimen was suboptimal in clinical trials, with VRd being superior to Rd in MM patients.4,26 Ideally, it was best to try and maintain this patient on a 3-drug regimen. There was a discussion concerning the use of other proteasome inhibitors to replace bortezomib. Carfilzomib is a second generation proteasome inhibitor with minimal CYP kinetic pathway interaction as well as minimal reports of hepatic toxicity.27,28 Ixazomib is metabolized by CYP1A2 and has reports of hepatotoxicity in clinical trials.4,29 Daratumumab has no known hepatic issues or toxicities and is now recommended as a first-line treatment for MM in combination with lenalidomide and dexamethasone.4,30 Lastly, the patient described in the case had good performance status, but was 74 years old which may make stem-cell transplant difficult to tolerate. 4 The medical team’s decision was to discontinue bortezomib and change the regimen to include carfilzomib. Renal and hepatic function was closely assessed to ensure carfilzomib and lenalidomide was dosed appropriately. 31 This medication adjustment provided improved safety from a hepatic toxicity standpoint without compromising efficacy in the first line setting for MM.
Conclusion
It is important to understand the risk factors associated with a rise in liver enzymes and how best to manage the clinical consequences when starting new medications. Elderly female patients that are prescribed medications that are metabolized through the liver are especially at risk of DILI. This patient most likely had an increase in liver enzymes from the administration of tizanidine and potentially bortezomib. Administration of acyclovir and hydralazine may have contributed to a rise in tizanidine and bortezomib concentrations. Close monitoring of liver function tests following initiation of bortezomib and tizanidine, particularly in patients with risk factors for liver toxicity, is prudent.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.