
Abstract
BACKGROUND
The burden of prescription drug prices affects patients and health system, creating a need for pharmacists to use their medication expertise to recommend the most cost-effective treatment for patients.
OBJECTIVE
The study aimed to analyze the cost avoidance for medication conversions related to GERD from an integrated medication therapy management call center.
METHODS
A quasi-experimental study was conducted at a call center during a 12-month intervention. Adult patients aged ≥18 years who received highercost PPIs were included. The pharmacists provided MTM services to patients telephonically to review all aspects of the patients’ medication regimen as well as conversion recommendation to lower-cost PPIs. The cost avoidance analysis and sensitivity analysis were conducted.
RESULTS
Of 40 eligible patients, 9 patients accepted the medication conversion, resulting in a 22.5% acceptance rate. The total cost avoidance from medication conversions was $19,937.1 per year, which equated to $2,215.2 per patient. The adjusted cost avoidance of medication conversion was estimated by assuming the patients who accepted the conversion continued taking the medication for 365 days and resulted in a total savings of $40,370.7 per year, which equated to $4,485.6 per patient. There were no significant association between the acceptance of medication conversions and patient’s age(P = 0.15), gender(P = 0.73), and insurance status(P = 0.96).
CONCLUSION
The study results showed that the call-center MTM with medicationconversion interventions successfully demonstrated an economically advantageous impact from a budgetary perspective. Further studies should explore methods to increase acceptance of MTM services and promote awareness of the profound effect on public health and well-being.
Introduction
Sontents are refluxed back into the esophagus, causing esophageal damage over time. 1 GERD is a common disorder in the United States (US) and it is estimated that the prevalence of GERD is 18.1-27.8%, making it the most common gastrointestinal disorder diagnosed in outpatient clinics. 2 The 2016 National Ambulatory Medical Care Survey (NAMCS) revealed that 4.3 million Americans were diagnosed with GERD in 2016. 3 Roughly $15-20 billion health care dollars are spent every year on GERD, with the majority of the costs spent on medications which is likely due to the chronic nature of the disease. 4 In addition to these direct health care costs, GERD accrues indirect health care costs through interference with patients’ quality of life. 5 Proton pump inhibitors (PPIs) are commonly used to treat GERD because they reduce the amount of hydrochloric acid produced in the stomach, thereby decreasing the likelihood of strong acid refluxing and eroding the esophagus. 6 With the high prevalence of GERD in the US population, it is no surprise that PPIs are one of the top 20 prescribed drug classes as seen in the 2016 NAMCS. 3 Studies have shown that PPIs have similar efficacy and safety in the treatment of GERD and other gastric acid related disorders.7,8 However, the cost gap between higher-cost PPIs and lower-cost PPIs is significant. Higher-cost PPIs include dexlansoprazole, esomeprazole, and omeprazole-sodium bicarbonate combination therapy. Lower-cost PPIs include omeprazole and pantoprazole. The average wholesale prices (AWP) for higher-cost PPIs are $11.30 for one capsule of dexlansoprazole brand capsules(30mg or 60mg DR), $1.02 for one capsule of esomeprazole generic capsules(20mg or 40mg DR), $10.04 for one capsule of esomeprazole brand capsules(20 mg or 40mg DR), and $13.34 for one capsule of omeprazole-sodium bicarbonate brand capsules(20-1100 mg or 40-1100 mg).9,10,11 In comparison, the AWP for lower-cost PPIs are $0.62(20 mg or 40mg EC) for one tablet of omeprazole generic tablets and $0.43 (20mg or 40mg EC) for one tablet of pantoprazole generic tablets. 12
In the ever-changing world of healthcare, pharmacists are a crucial member of interdisciplinary teams. Pharmacists are in a unique position to provide medication therapy management (MTM) services to help patients get the best benefits from their medication by actively intervening and managing drug therapy. Previous studies have shown the positive effect of pharmacist-driven MTM interventions on health outcomes. 13 Sanchez et al performed a retrospective review that demonstrated patients who received a telephonic pharmacist intervention within 30 days of hospital discharge were less likely to be readmitted. 14 A systematic reviewed study performed by Omboni and Caserini showed that pharmacists were able to control risk factors of cardiovascular disease such as high blood pressure, smoking, high cholesterol, and alcohol use through various types of MTM interventions. 15 Although several studies have shown the positive effects of MTM services, very few studies have evaluated its impact on economic outcomes, especially on medication conversions.16,17
While there is a growing interest in the cost containment of health care delivery, there is also a clear motivation for examining costs from a payer and systems perspective. Pharmacists can taper the growing costs in prescription drug spending by facilitating patients’ transition from higher-cost to lower-cost medications that attain similar therapeutic outomces. 18 The objective of this study is to analyze the cost avoidance for medication conversions related to GERD at an integrated medication therapy management call center from a budgetary perspective.
Methods
Study Setting and Design
This quasi-experimental study was conducted at a medication therapy management call center located in Fort Lauderdale, Florida. Nova Southeastern University’s College of Pharmacy (NSUCOP) developed a comprehensive and state of the art MTM pharmacy services call center in partnership with Independent Colleges and Universities Benefits Association (ICUBA) and OptumRx Pharmacy Care Services. The medication conversion intervention is included in the collaborative practice agreement. The call center is staffed by the clinical pharmacist who has supervision over pharmacy residents (licensed pharmacists) and pharmacy interns working in the call center. Services that pharmacists provide through the program include (1) serving as a liaison between primary care physicians, the pharmacy, and the insurance company (2) answering questions about medications (3) providing information on side effects and drug interactions (4) discussing medication options that are cost effective and (5) providing assistance with procuring prior authorizations from physicians. The pharmacists typically make outbound calls to members who are identified by ICUBA or physicians as needing specific services or assistance. Members are encouraged to contact the call center with any questions or concerns using the phone number located on the back of their prescription drug ID card.
Subjects
Adult patients aged ≥18 years who filled at least one prescription between January 1, 2017 and December 31, 2017 for any of the following 4 higher-cost PPIs were included in the study: dexlansoprazole, esomeprazole brand, esomeprazole generic, and omeprazole-sodium bicarbonate generic. Eligible members were defined as ICUBA members with active member status during the intervention and 1 year after the intervention implanted. The ICUBA members are employees and employees’ immediate family of the universities contracted with ICUBA commercial health insurance plans and OptumRx prescription drug program. The Institutional Review Board (IRB) at Nova Southeastern University approved this study. All study subjects completed the informed consent process.
Interventions and Data Collection
Pharmacists at the MTM call center provided medication therapy management telephonically to ensure that the medication is right for the patient and his or her health conditions and that the best possible outcomes from treatment are achieved. All data were retrieved from ICUBA electronic claim detail reports. These reports were extracted directly from ICUBA claims history and list all the members who took higher-cost PPIs between January 1, 2017 to December 31, 2017. Although the study is targeted on PPIs conversion, the individual patient’s medications were evaluated in the context of the patient, taking into consideration all of the patient’s conditions and medication therapy. Pharmacists first conducted the intervention protocol according to the MTM strategies recommended from the American Pharmacists Association. 19 A series of standard trainings were performed to provide a systematic process of implementing services, collecting patient-specific information and assessing medication therapies to identify medication-related problems. After completing the medication reviews from the eligible subjects’ electronic records, the pharmacy interns called and inquired patients whether to participate in the study. Each subject was called up to 3 times and each call was recorded. The cost differences between higher-cost PPI and lower-cost PPI were mentioned to patients in the telephone conversion. Pharmacist further verified the completion of the informed consent process and consulted patients if they agreed to change to lower-cost PPI. All medication conversion and dosage adjustment were consulted and informed prescriber via written facsimile (fax) to discontinue former PPI & initiate new PPI order to patients’ pharmacy of choice. Prescriber fax contained patient’s pharmacy of choice name, address, phone, and fax number for prescriber/office staff ease and options to discontinue or initiate new prescription. Pharmacy information provided allowed prescriber/office staff options in placing new prescription order via electronic prescription, telephone, or fax. Pharmacists then initiated follow up phone call to prescribers’ office to ensure successful transmission. Further follow up included several days later view via prescription carrier claims software for PPI claims, if successful retrieve plan pays prices and member pays prices, and document. If unsuccessful claim, review rejection reasons and follow up accordingly. In addition to recommending the switch from the higher-cost medication to the lower-cost medication, our pharmacists played an important role for communicating among patient, physician, patient’s primary pharmacist, and third-party payer to facilitate and assure the lower-cost medication filled.
All data collected in this study were securely stored on the ICUBA Claim Detail Reports system on a password protected site on the University server. The pharmacists used these claim detail reports to document 3 telephonic contact attempts for each eligible member. The documentation notes for each member were assessed to determine if the member accepted the recommended switch to the lower-cost medication. If the member accepted the switch, OptumRx, a third-party pharmacy services administrator that maintains a history of all prescriptions filled by the member, was checked to verify that the lower-cost medication was filled. The first fill date of the lower-cost medication was logged as the conversion date. The medication history was further reviewed for 12 months after the conversion date to check for consistency to the lower-cost medication.
Cost Avoidance Analysis of Medication Conversion
The cost avoidance of medication conversion (CAMA) was calculated using the cost of the lower-cost medication minus the cost of higher-cost medication, then multiplied by the actual days filled during the study period.
The cost figures were derived from the actual prescription claim data with consideration of real-world refill persistence for prescriptions. The medication conversions were classified as persistency if the patient has taken the medication for at least 12 months after the first day of conversion. The medication cost figures were based on the actual number of days the lower-cost PPI was filled. All data were retrieved from the electronic prescription drugs claim data.
Furthermore, the adjusted cost avoidance of medication conversion (ACAMC) was calculated to estimate the amount of money that could be saved every year if the member continues to fill the recommended new medication. This was calculated by taking the difference in the daily cost of the higher-cost and lower-cost medications and multiplying it by 365 days.

Statistical Analyses
A series of descriptive measures associated with medication costs avoidance were computed from the electronic prescription claim data. Differences in age between acceptance and non-acceptance of medication conversion intervention were compared using t-test. Chi-square tests were used to assess the statistical significance of differences for gender and insurance status. A sensitivity analysis was conducted to assess the sensitivity of acceptance rate to the projection of cost avoidance from the medication conversion. Data were analyzed using IBM SPSS software version 24 and a p-value of 0.05 was considered significant. 20
Results
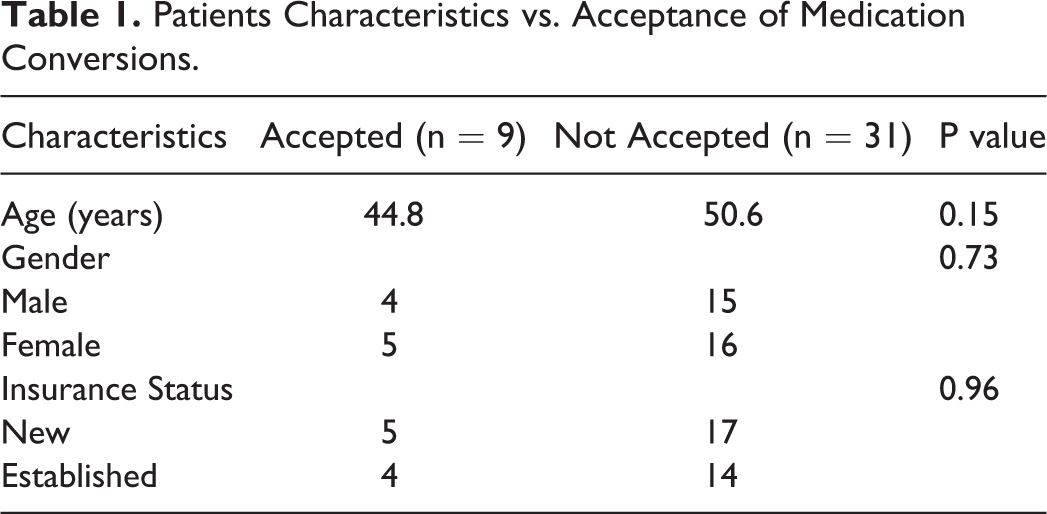
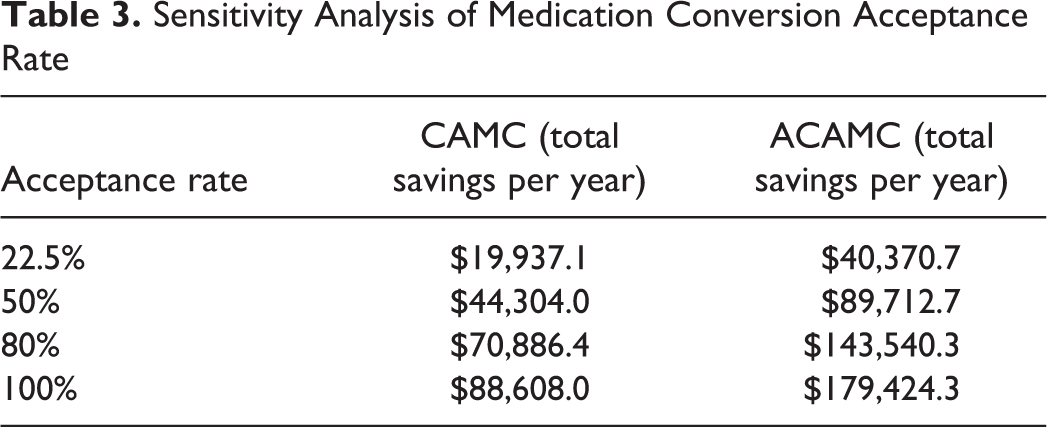
There were 175 total patients included in the study who were active members in ICUBA and taking a high-cost PPI during the study period. There were 74 members who were not called due to various reasons, such as the member not having a phone number available or the switch to the lower-cost PPI was not recommended. The pharmacists were able to call the remaining 101 members. However, only 40 patients who were identified as potential long-term PPI users and agreed to participate this project by telephone consent. A standard phone “script” that addresses the key elements of informed consent were used and all phone calls were recorded with permission. In this study, the potential Long-term use was defined as longer than 8 weeks of PPI claims data or per patient interview, including 1) Patient experiencing laryngopharyngeal reflux (LPR) symptoms sometimes referred to as silent reflux; 2) Per patient interview, patient experiencing ‘persistent GERD symptoms’ post recommended 8 weeks of therapy; 3) 1 years’ worth of PPI was seen in patients that had bariatric surgery (post surgery 1 year). The pharmacists further performed the medication therapy management (MTM) telephonically and recommended the switch from the higher-cost medication to the lower-cost medication. Out of the 40 members contacted, 9 members accepted the conversion to the lower-cost PPI, resulting in a 22.5% acceptance rate. Table 1 presents patients’ demographic information and the significance in influencing the acceptance of medication conversion. The mean age for the accepted and rejected groups were 44.8 years and 50.6 years, respectively. Yet, age (p = 0.15) was not statistically significant for acceptance rate, nor were gender (p = 0.73) and insurance status (p = 0.96), respectively. Figure 1 shows patient’s persistency for medication conversion. 66.7% of patients persisted using the recommended lower-cost PPIs throughout 12 months of follow-up. Non-persistent patients either discontinued PPI drug therapy (22.2%) or switched to other non-recommended PPIs (11.1%). There is no patient reverted to original higher-cost PPIs. The cost avoidance analysis found that total cost avoidance of all accepted medication conversion (CAMC) made by pharmacy call center interventions was $19,937.1 per year, which equates to $2,215.2 per member per year. Further, the adjusted cost avoidance of medication conversion (ACAMC) was estimated by assuming the patients who accepted the conversion continued taking the medication for 365 days and resulted in a total savings of $40,370.7 per year, which equated to $4,485.6 per member per year (Table 2). Based on the prescription claim data, there was an actual cost avoidance of $2,215.2 per member per year from the medication conversion from the plan budgetary perspective. We further conducted a sensitivity analysis to project the cost avoidance if the acceptance rate were to increase, with a 100% acceptance rate resulting in a projected CAMC of $88,608.0 and ACAMC of $179,424.3 saved per year if all eligible study subjects converted from a higher-cost PPI to a lower-cost PPI (Table 3).
Patients Characteristics vs. Acceptance of Medication Conversions.
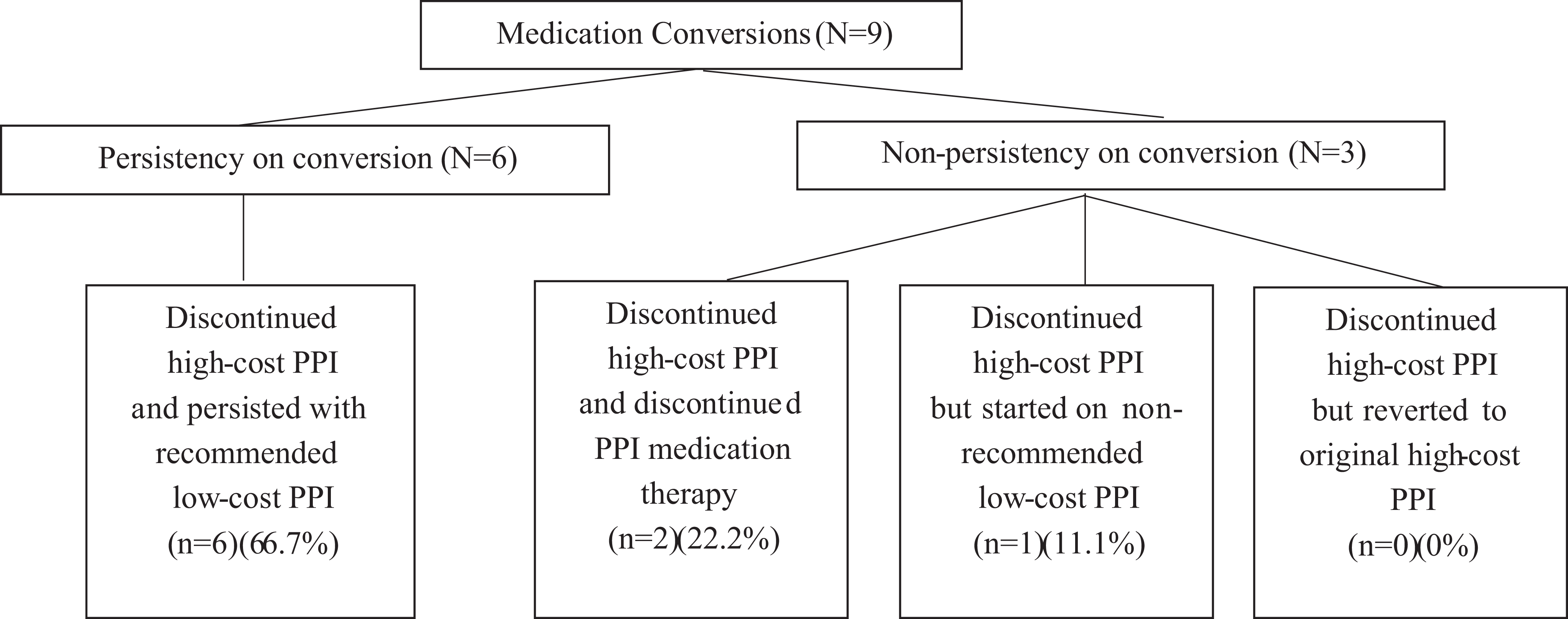
Medication conversions diagram.
Cost Avoidance Analysis (CAMC1 vs. ACAMC2).
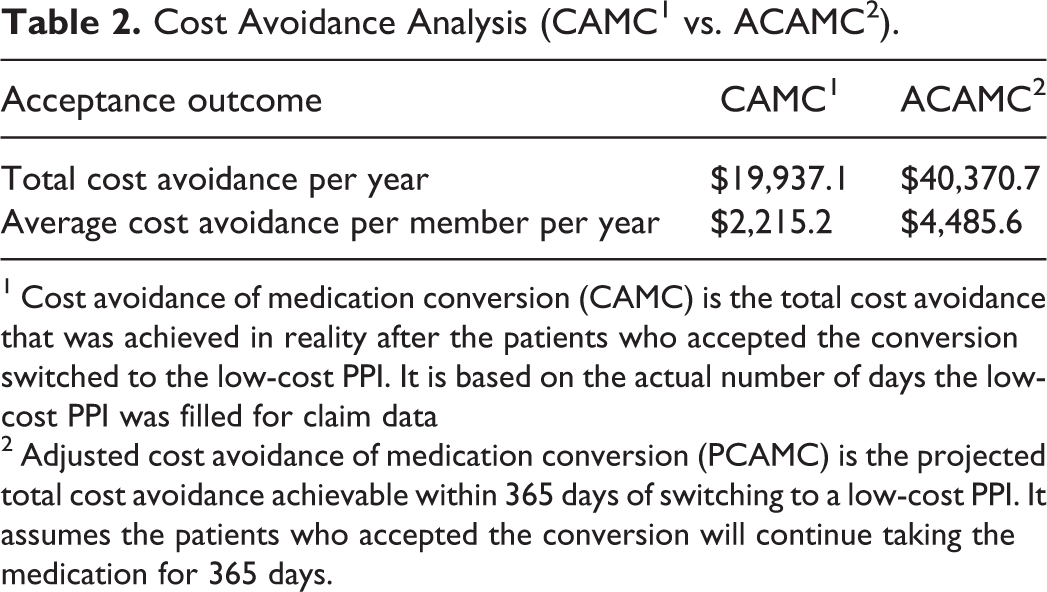
1 Cost avoidance of medication conversion (CAMC) is the total cost avoidance that was achieved in reality after the patients who accepted the conversion switched to the low-cost PPI. It is based on the actual number of days the low-cost PPI was filled for claim data
2 Adjusted cost avoidance of medication conversion (PCAMC) is the projected total cost avoidance achievable within 365 days of switching to a low-cost PPI. It assumes the patients who accepted the conversion will continue taking the medication for 365 days.
Sensitivity Analysis of Medication Conversion Acceptance Rate.
Discussion
The present study makes a valuable contribution to the field of pharmacy practice because it demonstrates economic evaluation techniques and processes that will be able to apply to other MTM interventions. Our study results showed that call-center MTM with medication-conversion interventions successfully demonstrated an economically advantageous impact from a budgetary perspective. Through these interventions, there was an actual cost avoidance of $2,215.2 per member per year from the medication conversion. Previous studies have shown similar positive effects on cost avoidance from pharmacist-initiated medication conversions. For example, it has been shown that pharmacy services involving converting brand medications to generics can save Medicare patients more than $2,900 per year in medication costs. 16 In addition, a 2016 study showed that brand-to-generic conversions in combination with other MTM interventions helped save Medicare patients on annual drug costs from $3,144 to $2,239 or less. 17 Kroner et al compared projected versus actual medication conversion related cost avoidance for 4 different pharmacotherapies (i.e. hypertension, dyslipidemia, depression, pain). The average projected medication cost avoidance for patients who persisted with their medication conversions was about $599 per conversion per year. 18 Our study results showed notable effects on cost avoidance compare with other studies, probably because our targeted medications (high cost PPIs) are relatively much more expensive medications. And, this study only investigated on single class of medication that was able to avoid clinical and methodological challenges arising from differences across different diseases and their MTM intervention strategies. Although the economic benefits of medication conversions were discussed in various therapeutic classes and study settings, to our knowledge, the present study is the first to evaluate cost avoidance on the treatment of gastroesophageal reflux disease from an MTM call center.
With respect to the limitations of prescription claim data, our study did not include the other potential cost avoidance such as decreases in health care expenditures related to avoided adverse drug reactions, emergency room visits, hospital admission, etc. However, these potential cost savings could be difficult to attribute all monetary benefit of indirect cost avoidance solely from the pharmacy services intervention. We attempted to overcome these limitations with a conservative approach for cost avoidance estimation. This conservative approach may underestimate values of MTM, but the results obtained here can be viewed as being close to the minimum benefit expected from medication conversions. An additional limitation of the study is that patients were not enthusiastic about the MTM medication conversion intervention, which introduces a potential bias in cost avoidance estimation. A systematic review of patient’s and the public’s view of community pharmacies showed that patients had a low awareness of the services pharmacists provide in the United Kingdom. 21 Another survey study in Canada had similar results, with most participants citing unawareness of the pharmacy services that pharmacists can provide. 22 However, most participants indicated they would take advantage of pharmacy services if they were aware such services existed. In our study, the possible reasons for low acceptance rate may vary; for example, lack of awareness of pharmacy services, fear of telemarketing scams or the issues of privacy, reluctance to change without doctor’s approval on the spot, uncertain of insurance coverage for new drugs, concern about therapeutic failure, and the need to complete more urgent tasks, etc. Although there is financial incentive for patients to pay less copayment for switching to lower-cost PPIs, the amount of cost saving was not a factor for our patients to accept medication conversion. This may be because this study population was from a commercial insurance that had some income busy work life and didn’t desire to spend time in the logistics of obtaining a new prescription (e.g., head to pharmacy, potentially prescriber’s office could call them and spend time discussing symptoms and treatments availability). Noted the public’s perceptions of pharmacists and pharmacy services may play a big role in the large number of patients who did not respond to the pharmacists’ call attempts in our study. Thus, this will be a significant next step to evaluate the effectiveness of different methods of increasing public awareness of pharmacy services that would have a profound effect on public health and well-being. One final consideration is the study subjects are with private health insurance, limiting generalization of our results to the patients with public health insurance such as Medicaid and Medicare.
Conclusion
Prescription drug spending has sky-rocketed over the past decade and only continues to climb. The burden of prescription drug prices affects patients and the economy alike, creating a need for pharmacists to use their medication expertise to decrease unnecessary spending on prescription drugs. In spite of the fact that our study only demonstrated the economic benefits from medication conversion on proton pump inhibitors for gastroesophageal reflux disease, it developed a widely applicable MTM platform and generated novel cost containment strategies that can be applied to different drug classes. As health care system was forced to adjust care delivery during the COVID-19 crisis, our call-center MTM interventions can be expanded to the telehealth model of care that will be perfectly suited to this pandemic situation- giving people in remote locations access to healthcare services without increasing risk of infection. Although this study has encouraging results on the cost avoidance potential of pharmacist interventions, there is still a need to discover avenues to reach more patients. Further studies should explore different approaches to increase awareness and acceptance from patients, in order to fully maximize cost avoidance while providing the most cost-effective patient care.
Footnotes
Acknowledgment
The authors acknowledge Dr. Mark Weinstein, the Independent Colleges and Universities Benefits Association, and OptumRx Pharmacy Care Services for technical support of this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.