
Abstract
Background:
Patients living in rural communities often experience pronounced health disparities, have a higher prevalence of diabetes and hypertension, and poorer access to care compared to urban areas. To address these unmet healthcare service needs, an established, academic-based MTM provider created a novel, collaborative program to provide comprehensive, telephonic services to patients living in rural Arizona counties.
Objective:
This study assessed the program effectiveness and described differences in health process and outcome measures (e.g., clinical outcomes, gaps in care for prescribed medications, medication-related problems) between individuals residing in different rural-urban commuting area (RUCA) groups (urban, micropolitan, and small town) in rural Arizona counties.
Methods:
Subjects eligible for inclusion were 18 years or older with diabetes and/or hypertension, living in rural Arizona counties. Data were collected on: demographic characteristics, medical conditions, clinical values, gaps in care, medication-related problems (MRPs), and health promotion guidance. Subjects were analyzed using 3 intra-county RUCA levels (i.e., urban, micropolitan, and small town).
Results:
A total of 384 patients were included from: urban (36.7%), micropolitan (19.3%) and small town (44.0%) areas. Positive trends were observed for clinical values, gaps in care, and MRPs between initial and follow-up consultations. Urban dwellers had significantly lower average SBP values at follow-up than those from small towns (p < 0.05). A total of 192 MRPs were identified; 75.0% were resolved immediately or referred to providers and 16.7% were accepted by prescribers.
Conclusion:
This academic-community partnership highlights the benefits of innovative collaborative programs, such as this, for individuals living in underserved, rural areas.
Background
Patients living in rural communities often experience pronounced health disparities. These communities also have a higher proportion of older adults and impoverished residents. 1 Additionally, their demographic, environmental, economic and social characteristics differ from urban centers, contributing to health problems. 2 Moreover, the prevalence of diabetes and hypertension is higher in rural areas compared to urban areas. Individuals living in rural areas have a greater likelihood of having diabetes than those in urban areas. 3 For example, estimates from the 2013 Behavioral Risk Factor Surveillance System (BRFSS) reported a prevalence of 12.0% for diabetes in rural areas versus 10.4% in urban areas; and the prevalence for hypertension was 38.1% in rural areas versus 32.6% in urban areas. 4 Rural health stakeholders recently ranked diabetes as one of the top 3 healthcare challenges facing rural areas in the United States (US). 5 Often these residents are at a higher risk for chronic diseases, face health workforce recruitment and retention challenges, have decreased access to hospitals and other medical facilities, and experience shorter overall life expectancies.2,6,7 Furthermore, rural patients are at increased risk for adherence-related treatment issues due to geographic barriers, lack of transportation to healthcare facilities, and lack of healthcare providers.8,9 Concentrated efforts are needed to address this gap in access to and provision of healthcare services for rural-dwelling patients.
The definition of the term “rural” varies as individuals, government agencies, and funders often define the term differently when setting thresholds for program eligibility. Rural may be defined using legal definitions, such as that provided by the Arizona state statute. 10 Another method is the rural-urban commuting area (RUCA) codes, using census data to classify each zip code. RUCA codes can be aggregated in many different ways, depending on the needs of the user, and have been widely used for health policy and research. Categorizing individuals by RUCA code is useful in identifying differences in trends between urban- and rural-dwelling patients regarding their medication optimization, healthcare utilization and health outcomes.11-13
Medication therapy management (MTM), defined by the American Pharmacists Association, is “a service or group of services that optimize therapeutic outcomes for individual patients.” 14 Medicare Part D sponsors must offer MTM services to all eligible beneficiaries, 15 yet each sponsor can determine how these services are provided to patients (e.g., telephonic, face-to-face, or both). 16
While MTM services improve patients’ health measures and reduce healthcare costs,17-20 challenges remain that limit their scope, reach and effectiveness. 21
While somewhat indirect, patients and prescribers play critical roles in the acceptance and provision of MTM services. Many patients have reservations about pharmacists performing roles other than dispensing medications, i.e. providing MTM services. 22 This may explain why only about 11% of eligible beneficiaries accept MTM services. 23 Moreover, completion rates for comprehensive medication reviews (CMRs), the initial step in this multi-step MTM process, 14 are low (23.8%-49.8%). 24 Furthermore, prescriber acceptance rates of pharmacists’ MTM recommendations vary widely (14.1%-60%),25-27 perhaps due to their lack of awareness regarding these services. 28 To address the challenges surrounding MTM acceptance, other researchers have evaluated: improving strategies or promotional approaches, establishing stricter eligibility criteria, varying levels of MTM services to improve efficacy, or integrating more targeted programs into clinics.24,29-31
To address this gap in unmet healthcare service needs, an established, academic-based MTM sponsor created a novel, collaborative program with independent retail and community health center pharmacies to provide comprehensive, telephonic services to patients living in rural Arizona counties (as defined by Arizona state statutes). 10 The use of 3 intra-county RUCA levels (i.e., urban, micropolitan, and small town) allowed for comparisons between degrees of rurality within population centers in counties designated as rural by the state of Arizona. The objective of this study was to describe differences in health process and outcome measures (e.g., clinical outcomes, gaps in care for prescribed medications, medication-related problems) between individuals residing in different RUCA groups (urban, micropolitan, and small town) in rural Arizona counties, and to assess the program effectiveness.
Methods
Study Design and Collaborators
This study used a pre-post design to assess the effect of this collaborative MTM program on the health process and outcome measures of rural Arizona patients. An academic-based MTM provider partnered with 5 rural community sites: 3 independent retail pharmacies; one pharmacy at a Federally Qualified Health Center; and one Rural Health Clinic pharmacy. The participating sites signed formal agreements with the MTM provider that outlined their specific roles and responsibilities for the project. The selected pharmacy sites were located in rural Arizona counties, as defined by the Arizona statute (A.R.S.§ 11-806). These specific pharmacy partners were selected given their long-standing relationships with the academic institution as well as their ability to target socioeconomically underserved areas to address health disparities as defined by the Centers for Disease Control and Prevention. 32 The University of Arizona Institutional Review Board approved this study.
Patient Eligibility and Enrollment
Eligible participants included those: receiving care at one of the community partner sites; aged 18 years or older; diagnosed with diabetes mellitus and/or hypertension; and living in rural Arizona counties. Participants were recruited and enrolled by personnel at the community partner sites in person or via telephone. The MTM provider also furnished flyers for dissemination via mail and e-mail and periodically conducted telephonic recruitment. Once a patient agreed to participate in the program, community site personnel completed a patient registration form and sent it to the MTM provider. The MTM pharmacist then contacted the patient to provide telephonic services from a centralized, academic site. The same board-certified pharmacist provided the MTM service to all study participants. All participants were informed of the program and given the option to participate or not.
MTM Services
The university-based provider integrated the American Pharmacists Association’s Core Elements of an MTM Service Model 14 during service provision. The MTM pharmacist provided comprehensive services, including an initial patient consultation and a CMR, during which patients were always asked about all prescribed, non-prescription, and complementary medications as well as medications recommended/prescribed by all of their other providers. Thereafter, the MTM pharmacist sent patient recommendations or referrals to the community partner sites (i.e., community pharmacist and/or prescriber).
Patients were deemed high risk, for study purposes, if they had any of the following: Hemoglobin A1c >7%, average fasting blood glucose (FBG) level >130mg/dL, ≥2 episodes of hypoglycemia, presence of diabetic complications, missing preventive screenings, blood pressure above individualized goal, uncontrolled respiratory symptoms, confusion regarding inhaler use, fluid overload symptoms, missing a fluid management plan, and medication non-adherence.33-39 Based on patient risk level, MTM pharmacists conducted follow-up consultations, at 30-days (high-risk patients) or at 90-days (all other patients), to ensure that their recommendations were addressed appropriately by the retail pharmacists or prescribers. MTM pharmacists conducted additional follow-up consultations as necessary. If the patient was unreachable, the MTM pharmacist made recommendations directly to community partner site staff, based on available information (e.g., site-provided medication list, or data review from electronic health record).
Staff at the community partner sites included medical assistants, pharmacists, or prescribers, depending on the site. Their role was to discuss recommendations made by the MTM pharmacist with the patients and conduct periodic reviews of medication history to assess recommendation outcomes. Community health workers (CHWs), were utilized at one site. Their role was to make a home visit during the initial consultation and CMR to: assist with the medication reconciliation, ensure patient understanding, and document any recommendations made.
Data Collection
Demographic information was collected for: gender, age, ethnicity, race, and medical conditions. Patients who had a CHW present at the initial consultation and individuals who were deemed high risk also were recorded.
Clinical data, including laboratory results and self-monitoring information, were collected at the initial and follow-up consultations for: systolic and diastolic blood pressure (SBP and DBP), hemoglobin A1c (HbA1c), fasting blood glucose (FBG), and postprandial glucose (PPG). Laboratory results (when available) were obtained from the medical record by the MTM pharmacist or community partner site staff, or directly from patients in the remaining situations.
Gaps in care were identified dichotomously (i.e., gap or no gap) as cases where an individual should have had a prescription for certain drug classes (statins, beta blockers, rescue inhalers, and inhaled corticosteroids) based on respective national consensus guidelines, yet did not (i.e., the individuals needed additional therapy).33-39 Presence of a statin (3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitor) was assessed for patients with diabetes and atherosclerotic cardiovascular disease while presence of a beta-adrenergic blocker was assessed for patients with reduced ejection fraction heart failure and in post-myocardial infarction patients. Inhaled beta-2 adrenergic agonist presence (such as an albuterol inhaler) was assessed for patients with asthma and those with chronic obstructive disease while presence of an inhaled corticosteroid was assessed in patients with asthma. These 4 classes were chosen as they represent treatments for common prevalent chronic conditions and have clinical guidelines to support their appropriate use. If an individual had a gap in recommended care, after taking into account the holistic needs of the patient e.g. medication history, allergies, comorbidities, etc. a facsimile was sent to the prescriber to alert them where appropriate. At the follow-up consult, the pharmacist assessed if the gap in care had been rectified.
Data also were collected on medication-related problems (MRPs) whereby the patient’s entire medication profile was taken into account including: unnecessary drug therapy (therapy duplications) identified and resolved; different drugs needed (drug-disease and drug-drug interactions), as well as dose-related safety concerns identified, referred, and accepted by the prescriber; adverse drug reactions identified and referred to prescriber; and high-risk medications (e.g., Beers list of medications to avoid in the elderly) identified, referred, and accepted by the prescriber for seniors (>65 years). 40 The MTM pharmacist followed a protocol delineating various actionable items and the criteria that deemed it as appropriate or inappropriate to take action.
Data collected on health promotion guideline adherence included reporting of: hypoglycemic event education; missing preventative screenings (e.g., daily foot exams and finger-stick fasting blood sugar for diabetic patients); medication utilization concerns (open text for any medication utilization concern reported, e.g. not taking medication as prescribed, inappropriate use or dosing of medications, delays in refilling medications); adherence issues (defined according to responses to the self-report question: do you miss a dose more than 6 times in 30 days?); administration errors identified and corrected; referrals made to various healthcare professionals or programs (e.g., diabetes education, dietary consultation, smoking cessation program, and use of CHWs); and vaccination recommendations (i.e., for influenza, pneumococcal, shingles).
Finally, data were collected for: the initial and follow-up consultation dates and time spent on the initial, pre- and post-CMR. Additionally, patient-reported levels of comfort managing their chronic diseases was collected before and after the CMR using the following question: “How comfortable are you with management of your chronic diseases?” Response options included: “very comfortable,” somewhat comfortable,” somewhat uncomfortable,” very uncomfortable.”
Data Analysis
Study subjects were organized into 1 of 3 intra-county RUCA groups: urban (RUCA codes 1-3; Metropolitan area core with high or low commuting), micropolitan (RUCA codes 4-6; primary traffic flow through an urban cluster or low or high commuting), or small town (RUCA codes 7-10; small town core with flow within an urban cluster or high or low commuting to a small urban cluster). The most recently available RUCA codes were employed for this study, based on the 2010 census data. That is, all subjects lived in rural Arizona counties as defined by the Arizona statute (A.R.S.§ 11-806). 10 However, within these counties there were urban, micropolitan and small town areas per the RUCA code definition. 41
Participants who were lost to follow-up were excluded from the analysis. Differences between initial and follow-up clinical values (laboratory results and self-monitoring data) were calculated by subtracting one value from the other. Differences between the initial and follow-up consultation dates were calculated, and the mean follow-up time was calculated for each group.
Chi-square or Fisher’s exact tests were used to compare unpaired nominal data. Post-hoc tests were conducted where necessary and Bonferroni corrections were applied in cases of multiple tests to decrease the possibility of type I errors. ANOVA and Tukey’s honestly significant difference tests were used as appropriate to evaluate changes in interval level data. An alpha of 0.05 was selected a priori. All analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Results
Demographic Characteristics
A total of 384 individuals were included in this study. The majority of subjects were female (n = 252, 65.6%), white (n = 280, 72.9%) and non-Hispanic (n = 201, 52.3%). The most common age category observed was for 65-74 years old (n = 127, 33.1%). Most patients had hypertension (n = 358, 93.2%) or diabetes mellitus type II (n = 286, 74.5%) or both (n = 265, 69.0%), based on the eligibility criteria. Post-hoc testing indicated that there were several instances of significant differences between the 3 RUCA groups for certain age groups, ethnicity status, and all medical conditions except hypertension. Almost half of the patients were considered high risk (n = 186, 48.4%), with significantly fewer of these individuals residing in urban versus micropolitan areas (p < 0.001) within rural counties. CHWs were present at the initial consultation for 45 subjects, all of whom were residing in urban areas (RUCA codes 1-3) within the rural counties. Further details are provided in Table 1.
Demographic Characteristics of Study Participants by Rural-Urban Commuter Area (RUCA) Code.
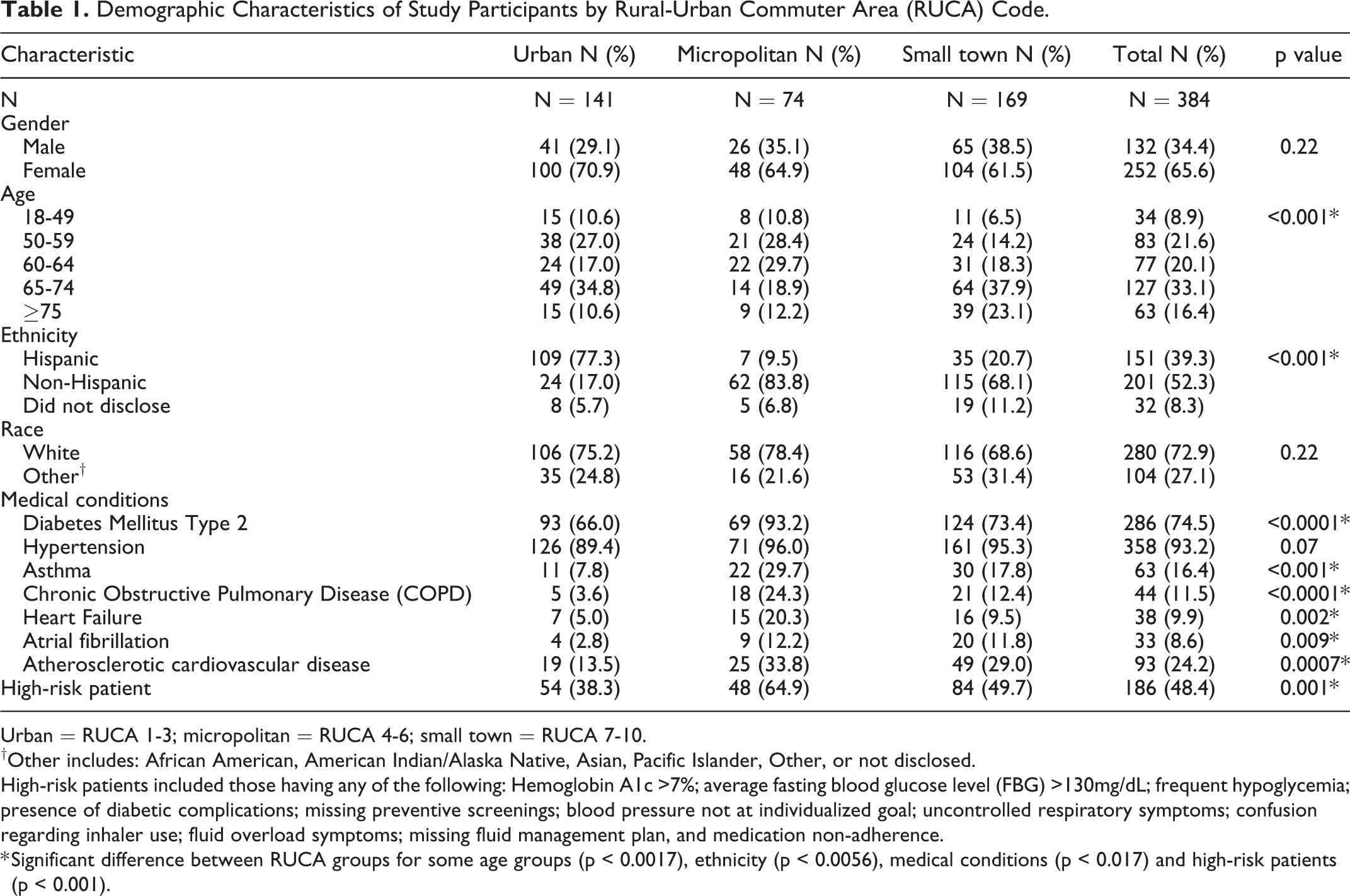
Urban = RUCA 1-3; micropolitan = RUCA 4-6; small town = RUCA 7-10.
†Other includes: African American, American Indian/Alaska Native, Asian, Pacific Islander, Other, or not disclosed.
High-risk patients included those having any of the following: Hemoglobin A1c >7%; average fasting blood glucose level (FBG) >130mg/dL; frequent hypoglycemia; presence of diabetic complications; missing preventive screenings; blood pressure not at individualized goal; uncontrolled respiratory symptoms; confusion regarding inhaler use; fluid overload symptoms; missing fluid management plan, and medication non-adherence.
* Significant difference between RUCA groups for some age groups (p < 0.0017), ethnicity (p < 0.0056), medical conditions (p < 0.017) and high-risk patients (p < 0.001).
Clinical Data
Mean follow-up laboratory values and self-monitoring data were typically lower than those documented at the initial consultation. However, the only statistically significant difference was for the mean average SBP value (p = 0.0263); urban-residing individuals had significantly lower mean average SBP values at follow-up compared to those living in small towns (p < 0.05) within the rural counties. See Table 2 for further details.
Clinical Values (Laboratory Results and Self-Report Data) at Baseline, 30- or 90-Day Follow-Up by Rural-Urban Commuter Area (RUCA) Code.
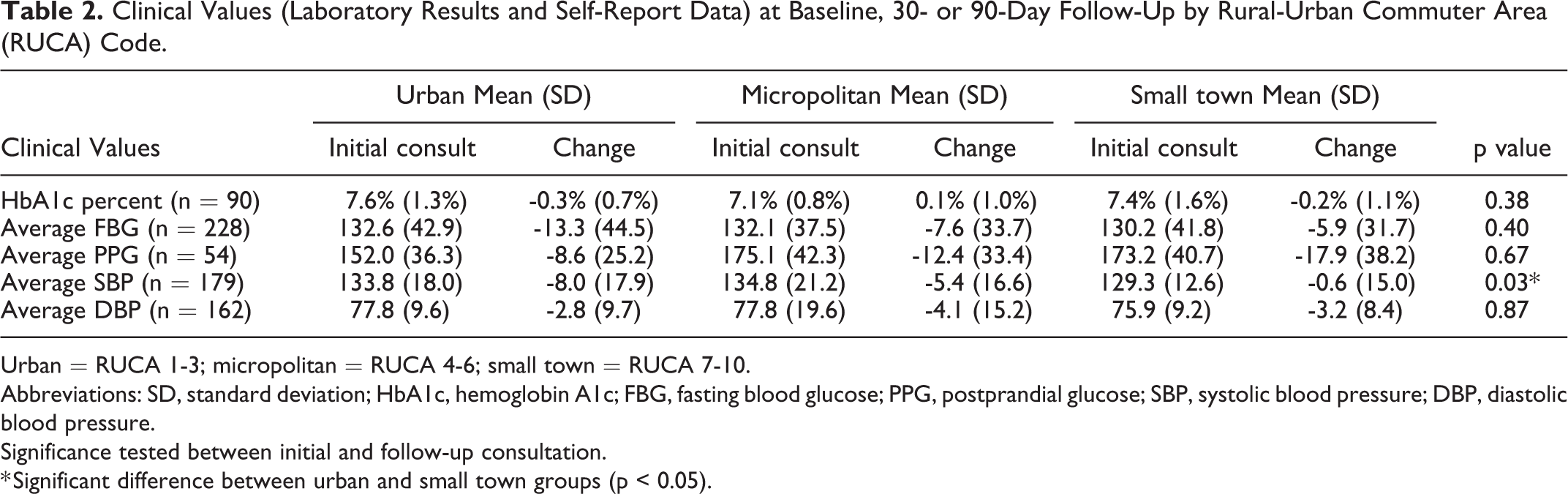
Urban = RUCA 1-3; micropolitan = RUCA 4-6; small town = RUCA 7-10.
Abbreviations: SD, standard deviation; HbA1c, hemoglobin A1c; FBG, fasting blood glucose; PPG, postprandial glucose; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Significance tested between initial and follow-up consultation.
* Significant difference between urban and small town groups (p < 0.05).
Gaps in Care and Need for Additional Therapy Based on National Consensus Guidelines
Pharmacists recommended that prescribers add a statin for 57 (21.8%) patients; of those, 19 (33.3%) additions were identified at follow-up. Adding a beta-blocker was recommended for 13 (20.6%) patients, yet only 2 additions (15.4%) were present at follow-up. Recommendations were made for adding a rescue inhaler for 7 (7.9%) patients; 3 additions (42.9%) were identified at follow-up. None of the 13 inhaled corticosteroid recommendations were present at follow-up. See Table 3 for further details.
Gaps in Care Representing Need for Additional Therapy Based on National Consensus Guidelines by Rural-Urban Commuter Area (RUCA) Code.
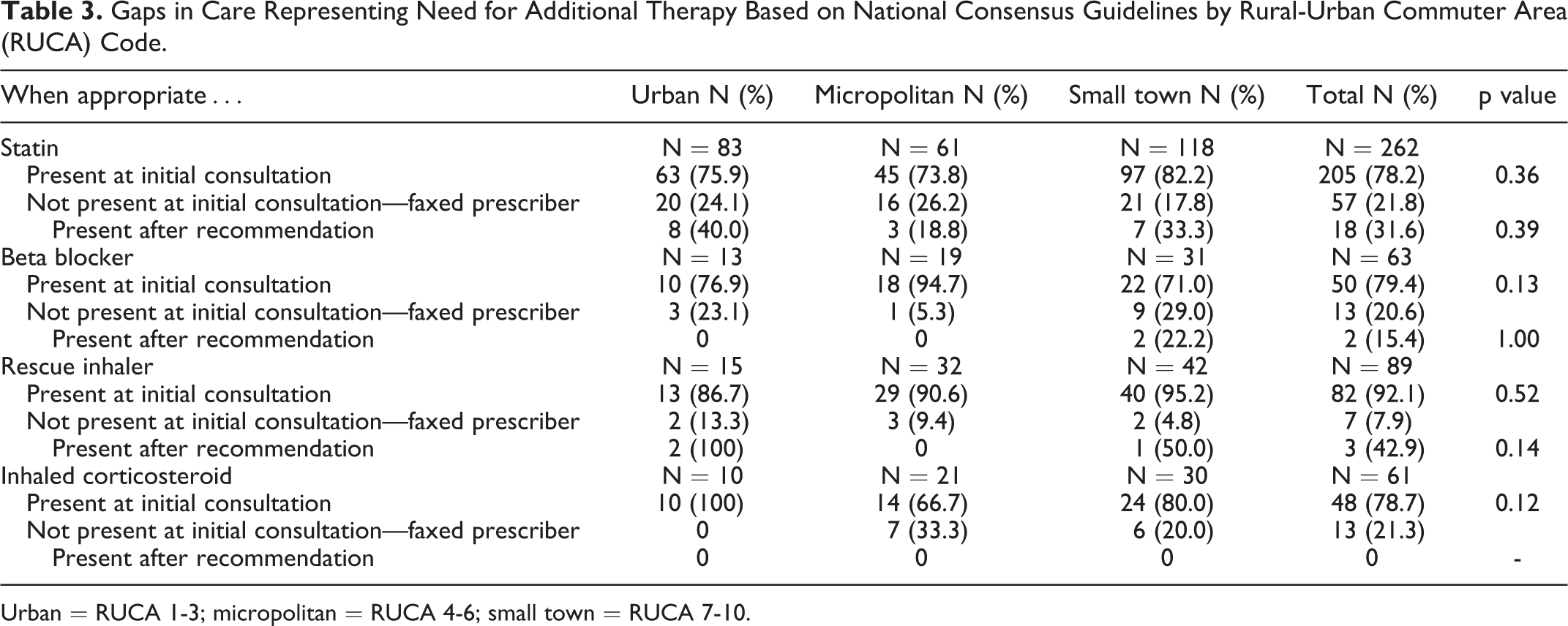
Urban = RUCA 1-3; micropolitan = RUCA 4-6; small town = RUCA 7-10.
Medication-Related Problems (MRPs)
A total of 23 (6.0%) patients had an unnecessary drug therapy, identified as a therapy duplication, and 82.6% of these were resolved at the initial consultation. In terms of cases where different drugs were needed, 15 patients (3.9%) had drug-disease interactions and significantly fewer of these individuals resided in small towns (n = 3) versus micropolitan areas (n = 7, p = 0.02) within the rural counties. Three (50.0%) of the 6 drug-disease interactions referred to the physician were accepted. Thirty-one (8.1%) patients with drug-drug interactions and 33 (8.6%) patients with dose-related safety concerns were identified. Four (40%) of the 10 drug-drug interactions and 8 (28.6%) of the 28 dose-related safety concerns referred to the physician were accepted. Fifty-one (13.3%) patients with adverse drug reactions (ADRs) were identified and resolved at the initial consultation. Thirty-nine (20.5%) patients with high-risk medications were identified in the older adult (>65 years) population; 30 (76.9%) were referred to the provider and 30.0% were accepted. No further significant differences were present between RUCA groups. See Table 4 for further details.
Medication-Related Problems (MRPs) Identified by Rural-Urban Commuter Area (RUCA) Code.
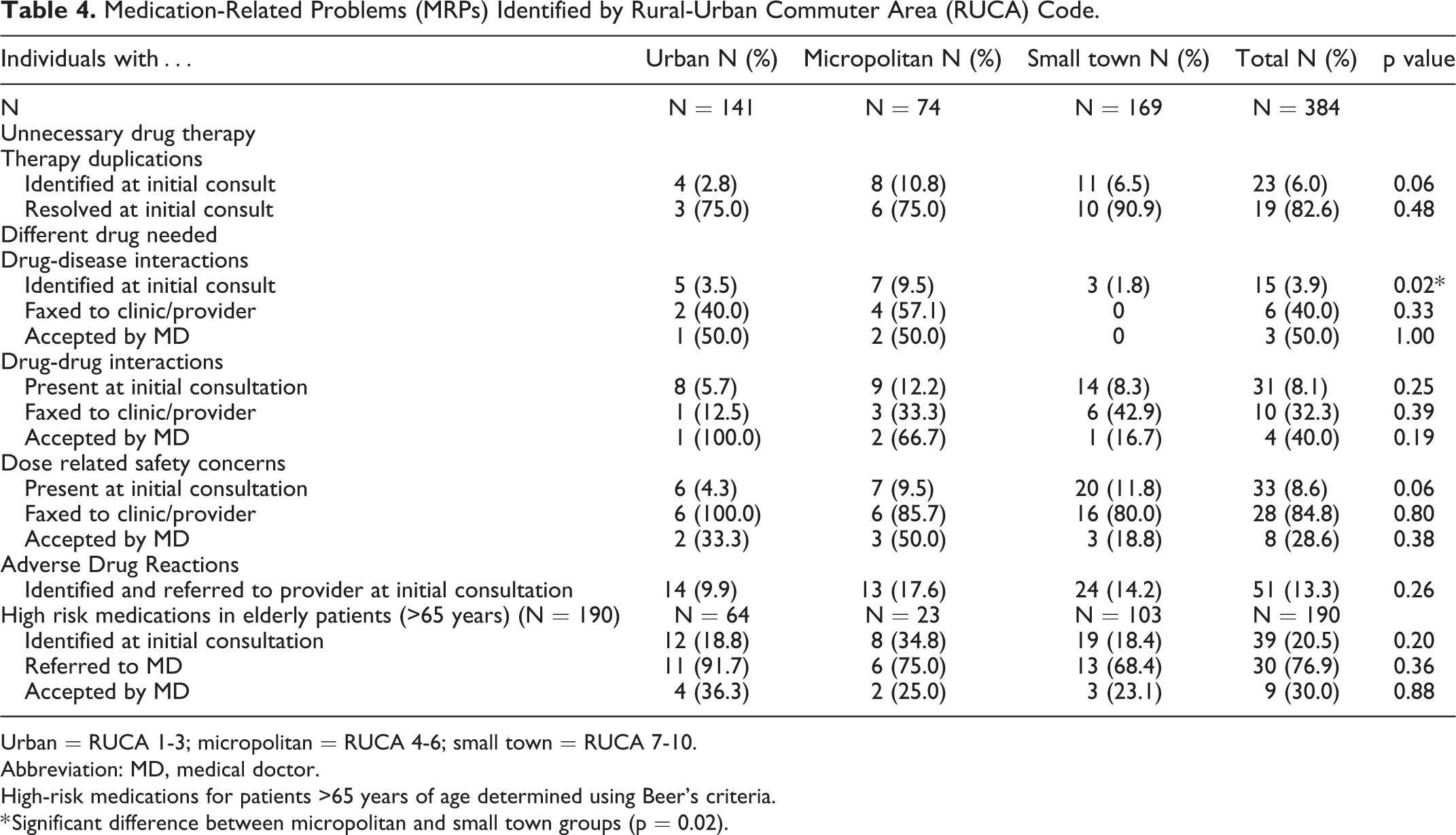
Urban = RUCA 1-3; micropolitan = RUCA 4-6; small town = RUCA 7-10.
Abbreviation: MD, medical doctor.
High-risk medications for patients >65 years of age determined using Beer’s criteria.
* Significant difference between micropolitan and small town groups (p = 0.02).
Health Promotion
Of the 283 patients with diabetes, 83 (21.6%) received glycemic event education. Utilization concerns were identified in 106 (27.6%) patients, and adherence issues (dose missed >6 times in 30 days) were identified in 39 (10.2%) patients. Administration errors were identified and corrected in 3 patients in the small-town group. A total of 123 (32.0%) patients were missing preventative screenings with significantly more of these individuals residing in micropolitan (48.6%) versus urban areas (24.1%, p = 0.0002) and small towns (31.4%, p = 0.01) within the rural counties.
Referrals to Other Healthcare Professions or Programs
Patients were referred to various other professionals or programs, including: nutritionists or dietitians (n = 6, 1.6%), endocrinologists (n = 4, 1.0%), diabetes educators (n = 4, 1.0%), primary care providers (n = 3, 0.8%), smoking cessation programs (n = 14, 3.6%), CHW (n = 6, 1.6%), or others (n = 5, 1.3%). Significantly more individuals living in micropolitan (12.2%) versus urban areas (2.1%, p = 0.002) and small towns (1.2%, p = 0.0002) within the rural counties were referred to a smoking cessation program. All 6 of the CHW referrals were to individuals in the urban group.
Vaccination Recommendations
During the initial consultation, MTM providers recommended influenza (n = 137, 46.4%), pneumococcal (n = 193, 56.3%), and shingles (n = 197, 76.7%) vaccines as appropriate. Significantly more individuals in the urban (89.4%) versus micropolitan (75.6%, p = 0.04) and small town (68.7%, p = 0.0004) groups within the rural counties received a recommendation for a shingles vaccination at the initial consult. See Table 5 for more details.
Vaccination Recommendations Made to Patients by Rural-Urban Commuter Area (RUCA) Code.
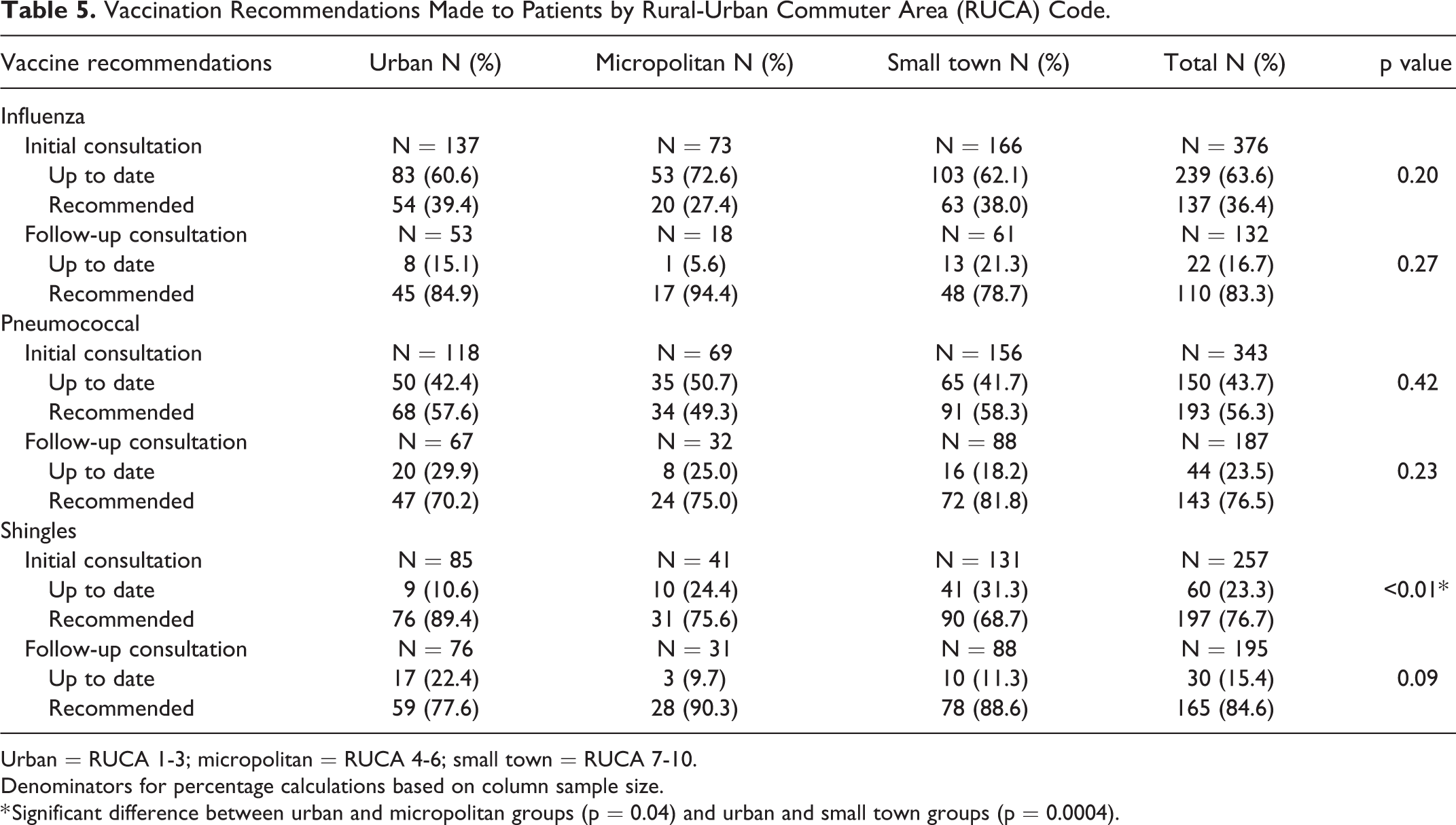
Urban = RUCA 1-3; micropolitan = RUCA 4-6; small town = RUCA 7-10.
Denominators for percentage calculations based on column sample size.
* Significant difference between urban and micropolitan groups (p = 0.04) and urban and small town groups (p = 0.0004).
Follow-Up Time
The mean follow-up period was 101.4 days (standard deviation, SD = 37.2) in the urban, 87.8 (SD = 36.7) in the micropolitan, and 96.2 (SD = 34.4) in small town groups within the rural counties, respectively. There were significant differences between the groups (p = 0.0310) with longer periods between follow-up for those in the urban group versus micropolitan group (p < 0.05) within the rural counties.
Pharmacists’ Time Spent on CMRs
Data were available for the time spent on CMRs for 365 individuals. Most CMRs took 16-30 minutes to complete (n = 172, 47.1%) followed by 31-45 minutes (n = 114, 31.2%), with fewer CMRs in the <15-minute (n = 39) and >45 minutes (n = 40) categories. There were no significant differences between groups.
Patients’ Level of Comfort Managing Chronic Diseases
A total of 250 patients were asked how they felt about managing their chronic disease before the CMR. Most reported being very comfortable (n = 116, 46.4%) or somewhat comfortable (n = 116, 46.4%). Post CMR, of the total of 176 patients responding to the same question, the majority felt very comfortable (n = 117, 66.5%) or somewhat comfortable (n = 58, 33.0%). No significant differences existed between RUCA groups based on level of rurality.
Discussion
These study findings provide evidence demonstrating the potential benefit of this pharmacist-delivered, collaborative MTM program targeting residents of rural counties. First, in general, there were significantly more individuals with chronic medical conditions in the micropolitan and small-town groups compared to their urban counterparts within rural counties. This pattern was similar for high-risk patients, further demonstrating the need for such a program to provide MTM services to individuals living in rural areas. Second, 90 recommendations were made to add a medication in accordance with national guidelines for the rural patient sample. Furthermore, over 200 therapy duplications, drug-disease interactions, drug-drug interactions, dose-related safety concerns, adverse drug reactions, and high-risk medications in the elderly were identified for this rural sample. Identification of this magnitude of issues among this sample of 384 individuals was quite concerning from a clinical standpoint, yet suggests the scale of healthcare benefits that may be realized if similar numbers of recommendations were identified and acted upon if this program were offered to larger, rural populations. Previous evaluations of novel pharmacist-provided MTM services have identified similar numbers of interventions made by pharmacists. 42 Although our intention was for this service to improve health outcomes, a 2015 meta-analysis found that MTM interventions can reduce some medication-related problems but may not improve health outcomes. Further work is therefore necessary to make sure such interventions are able to elicit the desired outcomes. 43
Recommendations for vaccinations varied considerably depending on the type of vaccine. Many patients were current with their influenza vaccines, yet approximately 30% received a recommendation for the vaccination. Fewer individuals had current pneumococcal vaccines and fewer still had up-to-date shingles vaccines. Interestingly, a significantly greater proportion of individuals were up-to-date with their shingles vaccines in the micropolitan and small town groups compared to the urban group, which highlights the notion that this service can benefit individuals living in urban centers as well.
There was only one instance of a statistically significant improvement in clinical values measured between baseline and follow up, i.e. urban-residing individuals had significantly lower mean average SBP values at follow-up compared to those living in small towns (p < 0.05). The authors recognize that interventions to improve diabetes and hypertension are often multifaceted (e.g., medications, lifestyle), thus this program only addresses the medication-related perspective of improving diabetes and/or hypertension control. This suggests that this process-oriented service is not improving outcomes as desired, and perhaps other approaches such as a collaborative practice agreement (CPA) could be used to improve outcomes. 44
One of the most concerning findings was that the number of pharmacists’ recommendations accepted or acted upon by providers was generally low, yet ranged considerably from 0% to 100%. Previous studies have also identified this trend. For example, Doellner et al. found that prescribers accepted 20% of pharmacists’ recommendations to initiate a statin, and 59% of recommendations to discontinue a high-risk medication. 45 Axon et al. also reported that pharmacists’ recommendations were inconsistently acted upon, and found that communication preferences were an important component for physician acceptance. 46 Therefore, further investigation is warranted to better understand the reasons why physicians sometimes fail to act on pharmacists’ recommendations. Without buy-in and action from physicians to address medication issues, the recommendations’ made by pharmacists are likely to have a limited impact on health outcomes and overall heath.
Self-reported medication adherence among this sample was relatively high (89.8%), but the MTM pharmacist was unable to investigate adherence in detail due to time constraints. Further work into medication adherence measures is therefore warranted.
This study also tracked the time for each pharmacist consultation to provide an estimate of the time spent with the individual patients. While most consultations took less than 45 minutes to complete, one-tenth (11%) lasted longer. The length of the consultation was carefully balanced to allow the pharmacist to conduct a comprehensive medication review and address any issues identified, while also being respectful of the patient’s time. However, it is possible that some participants, particularly older adults, may have found it challenging to concentrate on the details of the conversation for longer periods of time. This program was limited to patients with diabetes and/or hypertension, however the more lengthy consultations might be attributable to those individuals with other complex medical conditions and medication-related issues, requiring the pharmacist’s attention and additional time. Another possible explanation is that these patients were more engaged in their own healthcare and may have taken the opportunity to discuss management of their condition based on the pharmacist’s immediate availability, particularly given the well documented health workforce shortages in rural areas. 47 While diabetes and hypertension were the focus of the current study, these patients received a comprehensive medication review from the MTM pharmacist. However, future work could include expansion of service to patients with other chronic diseases and their associated medications.
For this project, the pharmacist-delivered medication therapy management (MTM) provided was reimbursed through the contract. Reimbursement for MTM services provided is an important consideration as the time spent by pharmacists providing services can vary between patients, particularly when the pharmacist has other competing tasks to accomplish. However, it is feasible that these billable, clinical services are reimbursable through chronic condition management (CCM) codes. Another alternative is to bill for services using the Current Procedural Terminology (CPT)-specific codes for MTM services. Relevant codes include: 99605 for initial consultations limited to 15 minutes; 99606 for follow-up consultations limited to 15 minutes; and 99607 for an additional 15 minutes when billed in tandem with either an initial (99605) or follow-up (99606) consultation.
This study utilized telephonic consultations to conduct comprehensive medication reviews. The main advantage of this approach is the ability to reach rural patients in their own communities and provide access to healthcare services, thus not requiring them to travel elsewhere (sometimes long distances) to receive care. Alternatives such as video-conferencing technology may enable the sharing of images such as medication bottles and labels. However, this would require the patient to have access to the Internet services, amenities that may be more limited or nonexistent in some rural areas. If they do have Internet access, they may incur additional data fees as a result, potentially creating a financial hardship for some of these individuals.
There were limitations associated with this study. First, defining rural populations can present challenges given the variety of definitions that exist; however, RUCA coding is a commonly used method for categorizing rurality and using these codes aligned with our study aims. Second, only specific disease-state parameters were available. Some clinical measures were self-reported by patients when the information was unavailable in their health record, and thus, may provide inaccuracies and/or inconsistencies in the data. Socioeconomic data that may help explain differences between groups also were unavailable. Third, the community partner sites were responsible for participant recruitment and that may have led to respondent bias. Likewise, self-selection bias may have occurred if more highly motivated individuals chose to participate in the study. However, self-selection should not have influenced the safety and preventative health findings observed in the study, as they were independent of the patient motivation. Fourth, the pre-post study design lacked a control group so it was impossible to investigate differences between those who received and those who did not receive MTM. Finally, many individuals referred to this service were ultimately ineligible to participate, and a further group of individuals were lost to follow-up (i.e., completed an initial CMR yet lacked a follow-up consultation for an unknown reason); the characteristics of these individuals could have been considerably different from those of the actual participants. It is also important to note that descriptive data relating to non-diabetes and non-hypertensive conditions should not be interpreted as a population prevalence as only diabetic and/or hypertensive patients were sampled. These findings may not be generalizable to other rural communities.
Conclusion
This evaluation of a collaborative partnership between an academic-based MTM provider and community pharmacies highlights the benefits of programs such as these for individuals living in rural areas, and offers a successful model for other researchers to consider. The authors recommend expansion of this MTM service to additional rural locations and evaluation of this expanded service as future research. It is possible that a similar workflow and focused, interprofessional communication could be achieved with more diverse populations and in other settings. While pharmacists identified over 200 medication-related problems, variation existed in the extent that providers accepted these recommendations, suggesting the need for expanded efforts geared toward provider outreach and improving acceptance of the pharmacist’s recommendations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: David Rhys Axon, Stephanie Forbes, Elizabeth Anderson, Ann M. Taylor, & Terri Warholak received funding from SinfoniaRx. Melissa Johnson, Brittany Abeln, Ann M. Taylor, Terri Warholak, & Elizabeth Hall-Lipsy received funding from the Arizona Department of Health Services. Teresa Aseret-Manygoats is an employee of the Arizona Department of Health Services.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the Grant or Cooperative Agreement Number, DP004793, funded by the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services. This work also was supported, in part, by SinfoniaRx.