
Abstract
Despite advances in diabetes technology, the proportion of patients with type 2 diabetes achieving recommended glycemic goals remains suboptimal. There is a growing interest in flash continuous glucose monitoring (CGM) among patients, pharmacists and providers. Pharmacists are well positioned to collaborate with patients and providers in ambulatory care or community-based settings to allow a greater number of patients with diabetes to harness the benefits of flash CGM. The purpose of this narrative review is to provide pharmacists with a background on flash CGM technology, review the data supporting pharmacist-driven flash CGM services, and address common questions that arise in pharmacy practice surrounding flash CGM.
Keywords
Background
Hemoglobin A1c (HbA1c) and self-monitoring of blood glucose (SMBG) are recognized as the standard of care for assessment of glycemic control. 1 However, HbA1c and SMBG have limitations, such as regression to the mean (HbA1c), and evaluation of only one glucose reading without trends in glycemia (SMBG). Accordingly, the use of novel glycemic metrics from continuous glucose monitoring (CGM) systems are more frequently being used in clinical practice owing to a more comprehensive assessment of glycemic control. The glycemic metrics which can be obtained from CGM systems include glycemic variability (GV), mean glucose, time in range (TIR), time above range (TAR), time below range (TBR), and the estimated HbA1c (termed the glucose management indicator). 2 Similar to HbA1c, a high GV, and TIR are associated with poor glycemic control, and both microvascular and macrovascular diabetes complications.3-7
The newest form of CGM is flash CGM, which is more affordable and convenient for patients as compared with real-time CGM. 8 At the time of writing, Abbott Pharmaceuticals manufactures 3 flash CGM devices (FreeStyle Libre, FreeStyle Libre Pro, and FreeStyle Libre 2). Each flash CGM device uses a sensor that can be worn for up to 14 days on the back of the arm, and when scanned using a reader or compatible smartphone, displays real-time interstitial glucose and glucose trend arrows. 9 This data can help patients make immediate drug therapy decisions and/or lifestyle modification. 9 Barriers hindering widespread adoption and use of flash CGM exist, such as inexperience in determining appropriate candidates for use, as well as lack of familiarity with interpreting glycemic data from flash CGM to inform clinical decision-making,10,11
The majority of people with diabetes are cared for in ambulatory care settings, where pharmacists are becoming recognized as integral members of the interprofessional team. 12 Extensive literature supporting team-based care practice models suggest that integration of a pharmacist into ambulatory care settings may improve clinical and economic outcomes related to diabetes,13-15 and is supported by several organizations.12,16,17 Additionally, pharmacists in the community setting are highly accessible and have been called upon by the Centers for Disease Control & Prevention to deliver diabetes education and prevention. 18 Given the need for frequent glycemic monitoring in patients with diabetes, there is an opportunity for pharmacists to develop clinical services aimed at improving adoption and use of flash CGM. Additionally, pharmacists can play a role selecting appropriate candidates for flash CGM and can help patients use flash CGM data to make treatment decisions. There are also billing opportunities for pharmacists involved in providing services for patients using flash CGM. 19 Therefore, the purpose of this narrative review is to address commonly encountered questions faced in clinical practice surrounding flash CGM for pharmacists.
Methods
Search Strategy
A literature search was conducted in PubMed (inception-December 17, 2020) for English language articles (no filters on study design) published using MeSH terms “flash continuous glucose monitoring,” “intermittent-scanned continuous glucose monitoring,” “libre,” and “diabetes.” The same search strategy was applied to identify outcomes from pharmacist-led flash CGM studies although with the inclusion of the MeSH term “pharmacist.”
Evidence for Pharmacist-Driven Flash CGM Services
Despite growth in flash CGM use, only 2 studies have been published to date identifying pharmacist-driven implementation of flash CGM. 20 In the first study, Van Dril and Schumacher conducted a retrospective, pre-post analysis in 29 patients with type 2 diabetes (T2D) using blinded flash CGM with at least 24 hours of CGM data interpreted by a pharmacist under a collaborative practice agreement (CPA). 20 The primary outcome was to determine if pharmacist-driven CGM improved short-term glycemic metrics. The investigators found no significant difference in the mean percentage of TIR [between group difference: 0.2% ± 21.4 (p = 0.966)], or mean estimated average interstitial glucose [between group difference: −3.0 mg/dL ± 58.4 (p = 0.779)], from baseline to post-intervention. 20 However, there was a non-significant mean reduction in HbA1c of 0.7% from baseline to post-intervention (p = 0.156). 20
In the second study, Sherrill and colleagues conducted a single-center retrospective cohort analysis in patients with uncontrolled T2D (mean baseline HbA1c of 9%). 21 All patients received blinded flash CGM, and results were compared between patients seeing a pharmacist under a CPA for 1 (n = 52) or 2 encounters (n = 58), versus usual care with a physician (n = 171). 21 At 6 months, the greatest mean reduction in HbA1c was found in those seeing the pharmacist for 2 encounters, and was significantly greater than the HbA1c reduction found in the usual care group [between group difference in HbA1c: 0.8% (p = 0.005)]. 21 Interestingly, the study found that patients not being treated with insulin at baseline had a 0.5% greater HbA1c reduction (p = 0.01) as compared with patients using insulin. 21 Although these findings suggest a clinical, and significant benefit to flash CGM use in patients with T2D not using insulin, several confounders among patients using insulin exist such as compliance, injection technique, correct dose, and timing of insulin which must be considered. Additionally, the baseline HbA1c in this study was 9%, suggesting that patients using insulin were either noncompliant or inappropriately managed. Additional research is needed to confirm these findings in a larger population of patients with T2D not using insulin.
Considerations for Flash CGM
Question 1. What is the rationale for flash CGM?
As a largely self-managed chronic condition, diabetes often involves frequent glycemic monitoring through patient SMBG in conjunction with HbA1c testing. 22 Since HbA1c is an average of glycemia over 2-3 months, there is a wide variability in the mean glucose range at any HbA1c level. 23 Moreover, patients with similar HbA1c levels can have dissimilar trends in glucose. 23 HbA1c is also unreliable under many hematologic conditions (i.e., anemia, sickle-cell disease), physiologic states (i.e., pregnancy), disease states (i.e., hyperbilirubinemia, cirrhosis), and with use of many medications (i.e., opioids, aspirin, vitamin C). 24 Limitations also extend to SMBG, as it only provides glucose data at one point in time, and is often infrequent or intermittent. 2 Additionally, SMBG does not provide real-time alerts for hypoglycemia or hyperglycemia, and cannot detect nocturnal hypoglycemia. Flash CGM can be used to monitor glycemic metrics beyond HbA1c and SMBG, such as GV, TIR, TBR, TAR, and magnitude and frequency of glucose fluctuations. 25 CGM also provides a more comprehensive analysis of glycemia through collecting several glucose values per hour. 22 When evaluated and used appropriately, these metrics can not only inform immediate drug therapy decisions and/or lifestyle modification from the patient, but also allow for a greater level of actionable information to inform clinical decision-making. 25
Question 2. Who is most likely to benefit from flash CGM?
The 2020 American Diabetes Association (ADA) Standards of Medical Care in Diabetes guidelines recommend that use of flash CGM may lower HbA1c and/or reduce hypoglycemia in patients with type 1 diabetes (T1D), and among patients with T2D using insulin who are not meeting glycemic goals. 2 However, emerging evidence suggests that flash CGM use may lower HbA1c among patients with T2D not using insulin.26,27 Based on a review of the literature,28,29 and in the author’s clinical experience, we also outline patients treated in the outpatient setting who may be most likely to benefit from flash CGM:
Those who experience Somogyi effect (rebound hyperglycemia in response to hypoglycemia) or Dawn Phenomenon (early morning hyperglycemia)
Those with hypoglycemia unawareness or frequent episodes of hypoglycemia or hyperglycemia (FreeStyle Libre 2® due to alarm feature)
Those with dexterity issues and who cannot handle SMBG testing supplies
Those who prefer a more discrete method of glucose testing
Those with a high level of glycemic variability
Those with an HbA1c that does not correlate with SMBG readings
Those with kidney disease or gastroparesis
Prior to April 2020, flash CGM was not approved for use within the inpatient setting. However, in April 2020, the U.S. Food and Drug Administration did not object to using flash CGM within the inpatient setting in response to the COVID-19 pandemic. 30 This has allowed frontline healthcare workers to remotely monitor glucose, limit exposure to COVID-19, and has preserved personal protective equipment. 31 Though not extensively studied, flash CGM may reduce nursing workload through fewer finger-sticks, which are often required several times daily in hospitalized patients with diabetes using insulin. 31
Few studies have evaluated flash CGM use within the inpatient setting. Accordingly, at the time of writing the use of flash CGM should be considered investigational within the inpatient setting. 31 CGM accuracy has been questioned in the perioperative period, and although studied in critically ill patients (i.e., shock, hypotension, burns or hemodialysis), use should be cautioned due to study limitations such as small sample size, heterogeneity in study design and heterogeneity in prespecified outcomes. 32 Additional considerations for when flash CGM is not well-studied includes those using an insulin pump, or during pregnancy. 8 Flash CGM is also contraindicated with magnetic resonance imaging, computerized tomography scan, and diathermy. 8 As such, the device should be removed prior to these procedures. 8 Based on expert opinion,31-34 clinical situations in which flash CGM may be considered within the inpatient setting are as follows:
Type 1 diabetes
Ongoing use of flash CGM in the outpatient setting
Use of high insulin doses or multiple daily insulin injections
Long-standing history of diabetes
Newly diagnosed diabetes
Significant glucotoxicity or extreme insulin resistance upon presentation
Iatrogenic hyperglycemia secondary to steroids or medical nutrition therapy (enteral or parenteral nutrition)
Frail patients, or comorbidities which increase hypoglycemia risk (i.e., poor nutrition, kidney disease or advanced age)
Question 3. What are the differences among flash CGM devices?
In 2017, the U.S. Food & Drug Administration approved the first flash CGM device for adults aged 18 years and older, the FreeStyle Libre®, manufactured by Abbott. In June 2020, Abbott cleared it’s second-generation flash CGM device, the FreeStyle Libre 2®, for use in pediatrics and adolescents aged 4 years and older. The major differences between these 2 devices are outlined in Table 1.
Selected Differences in Flash Continuous Glucose Monitoring Devices.
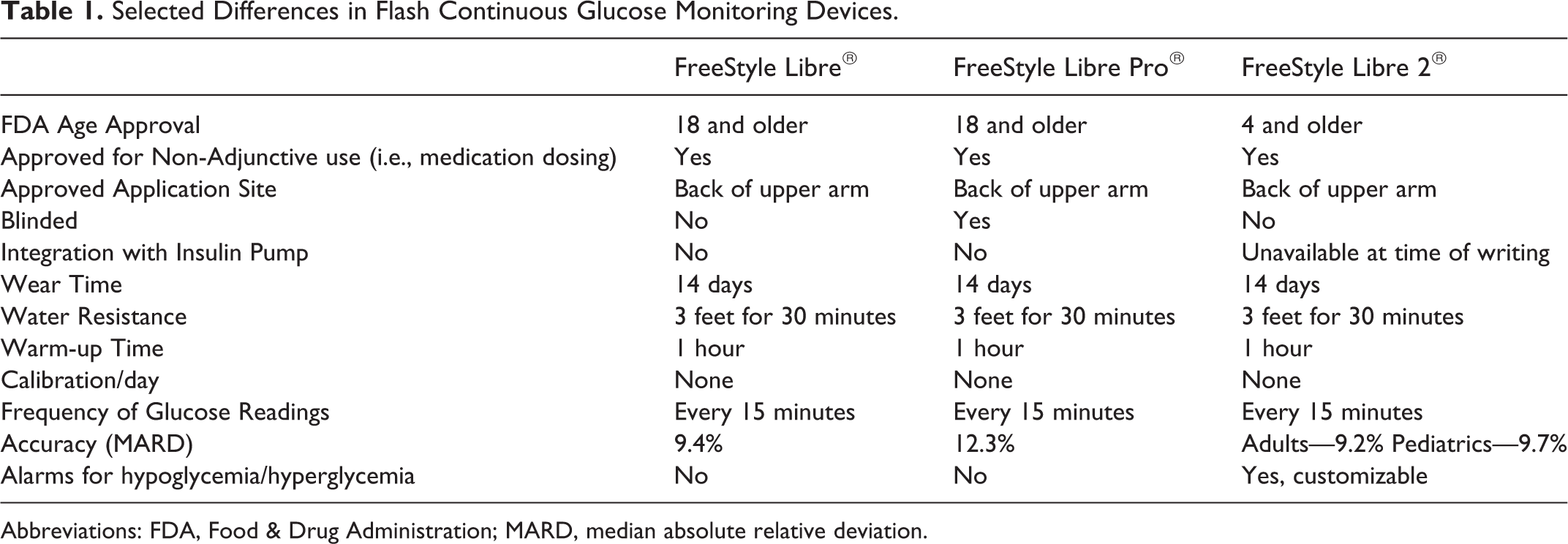
Abbreviations: FDA, Food & Drug Administration; MARD, median absolute relative deviation.
Question 4. What is the difference between blinded and un-blinded flash CGM?
Flash CGM is currently available either blinded (FreeStyle Libre Pro®) or un-blinded (FreeStyle Libre®). 35 Blinded flash CGM keeps track of blood glucose data, but does not provide the glucose data to the patient. 35 Un-blinded devices present glucose data to the patient when the flash CGM device is scanned using a reader. 35 Blinded CGM use may be appropriate when no patient interference is desired (i.e., during a clinical trial designed to study a drug), or if short term CGM is desired (i.e., to rapidly and safely titrate insulin). 35 However, for the vast majority of patients, un-blinded CGM is appropriate because it allows flash CGM to be used as a tool to empower patient’s with diabetes to recognize how variables such as dietary habits, physical activity, and medications impact glucose levels. 36
Question 5. How accurate is flash CGM?
Guidelines for assessing CGM sensor accuracy do not exist. 22 Most studies evaluate the accuracy of flash and real-time CGM using the mean absolute relative difference (MARD), whereas studies evaluating standard glucometers use the International Standardization Organization (ISO) criteria. 22 MARD is the average of absolute error between CGM values and a set of matched reference values. 37 A low MARD indicates that bias and imprecision is small, and in general, a MARD < 10% indicates strong accuracy.22,37 The overall MARD for most commercially available real-time CGMs labeled for non-adjunctive use range from 10-12%.38,39 Differences in MARD for available flash CGM devices are shown in Table 1. Comparing accuracy of flash and real-time CGM devices with glucometers is difficult since the ISO requirements and MARD values cannot be directly compared.22,40 However, the accuracy of flash CGM compared to capillary and venous glucose testing has been shown to be acceptable across a range of individuals with T1D and T2D. 41 The accuracy between real-time CGM (Dexcom G4 and G5) has shown good agreement with flash CGM (FreeStyle Libre).42-44 Nonetheless, caution should be taken in drawing direct comparisons on accuracy between CGM systems due to heterogeneity in study design, methodology, study population, and metrics used across studies.40,45 Pharmacists should be aware that certain substances have been shown to interfere with accuracy of flash CGM readings. In a study conducted by the manufacturer of the FreeStyle Libre ® flash CGM device, it was determined that ascorbic acid (>1,000 mg/day) may falsely raise flash CGM readings, and salicylic acid (>650 mg/day) may falsely lower flash CGM readings. 46
Question 6. How can flash CGM data be used in clinical decision making?
Flash CGM provides meaningful glycemic data on a standardized printout called the ambulatory glucose profile (AGP). 47 Summarized below is a suggested approach to analyzing the AGP to inform clinical decision making based on evidence-based recommendations.25,47,48 Where noted, high risk is defined as those at increased risk for diabetes related complications, comorbid conditions (i.e., cognitive deficits, kidney disease, joint disease, osteoporosis, fracture, cardiovascular disease), or adults requiring assisted care. 25
Check for adequate data and ensure sensor was worn for an appropriate amount of time. It is recommended to wear the sensor for 14 days and the sensor data should be reflective of at least 70% of time over the sensor wear period. 25
Identify patterns of low glucose. From a clinical management perspective, the first priority between managing TIR, TBR and TAR is to address TBR, then TIR or TAR, given the negative health outcomes associated with hypoglycemia. 25 Goals for TBR < 70 mg/dL and < 54 mg/dL should be < 4% and < 1% of total CGM readings per day, respectively. 25 For older adults and high risk adults the TBR of < 70 mg/dL should be <1% of total CGM readings per day. 25
Identify patterns of high glucose. TAR > 180 mg/dL should be minimized to < 25%, and > 250 mg/dL to < 5% of total CGM readings per day. 25 For older adults and high risk adults, the TAR of > 250 mg/dL should be < 10% of total CGM readings per day. 25
Review time in the normal glycemic range. TIR is the percentage of time spent in the target glycemic range (typically defined as 70-180mg/dL and 63-140mg/dL during pregnancy). 25 Since it is unrealistic for patients with diabetes to have a TIR of 100%, recommendations have been developed which outline the TIR and a set of targets for the time per day as a percentage of total CGM readings. 25 The percentage of readings per day within the glycemic range should be > 70% for most patients and > 50% in older and high-risk adults. 25 A TIR of 70% and 50% are strongly associated with an HbA1c of 7% and 8%, respectively. 49 Additionally, a 10% increase in the TIR corresponds to a decrease in the HbA1c of 0.8%. 49
Identify variability in glucose. The first parameter to evaluate is the coefficient of variation (CV) along with its standard deviation (SD). The target for %CV is ≤ 36%. 25 It may be recommended to target a %CV of <33% in those receiving insulin or sulfonylureas.50-52 The SD should be less than the average glucose divided by 3. 48 On the AGP, GV is further differentiated (visually) into the interquartile range (IQR, 25th-75th percentile) and the interdecile range (IDR, 10th-90th percentile). IQR is mostly affected by treatment-related factors such as incorrect insulin sensitivity factor, incorrect correctional factor, and inappropriate basal insulin rates or basal insulin dose. The IDR is reflective of behavioral factors such as skipped meals, inappropriate insulin injection to meal interval, irregularity in daily routines, exercise or alcohol intake. Examples of typical trends in IQR and IDR and their interpretation are provided in Table 2. Incretins (glucagon-like peptide 1 receptor agonists and dipeptidyl peptidase-4 inhibitors) have been shown to reduce glycemic variability.53-55
Identify if HbA1c is discordant from SMBG. The AGP provides the average glucose over the sensor wear period along with a metric called the glucose management indicator (GMI), which is used to estimate HbA1c from the average glucose. 56 The GMI can be used to explore reasons for the discordant results, if applicable.
Sample Interpretation of the Interquartile Range (IQR) and Interdecile Range (IDR) for Flash Continuous Glucose Monitoring.
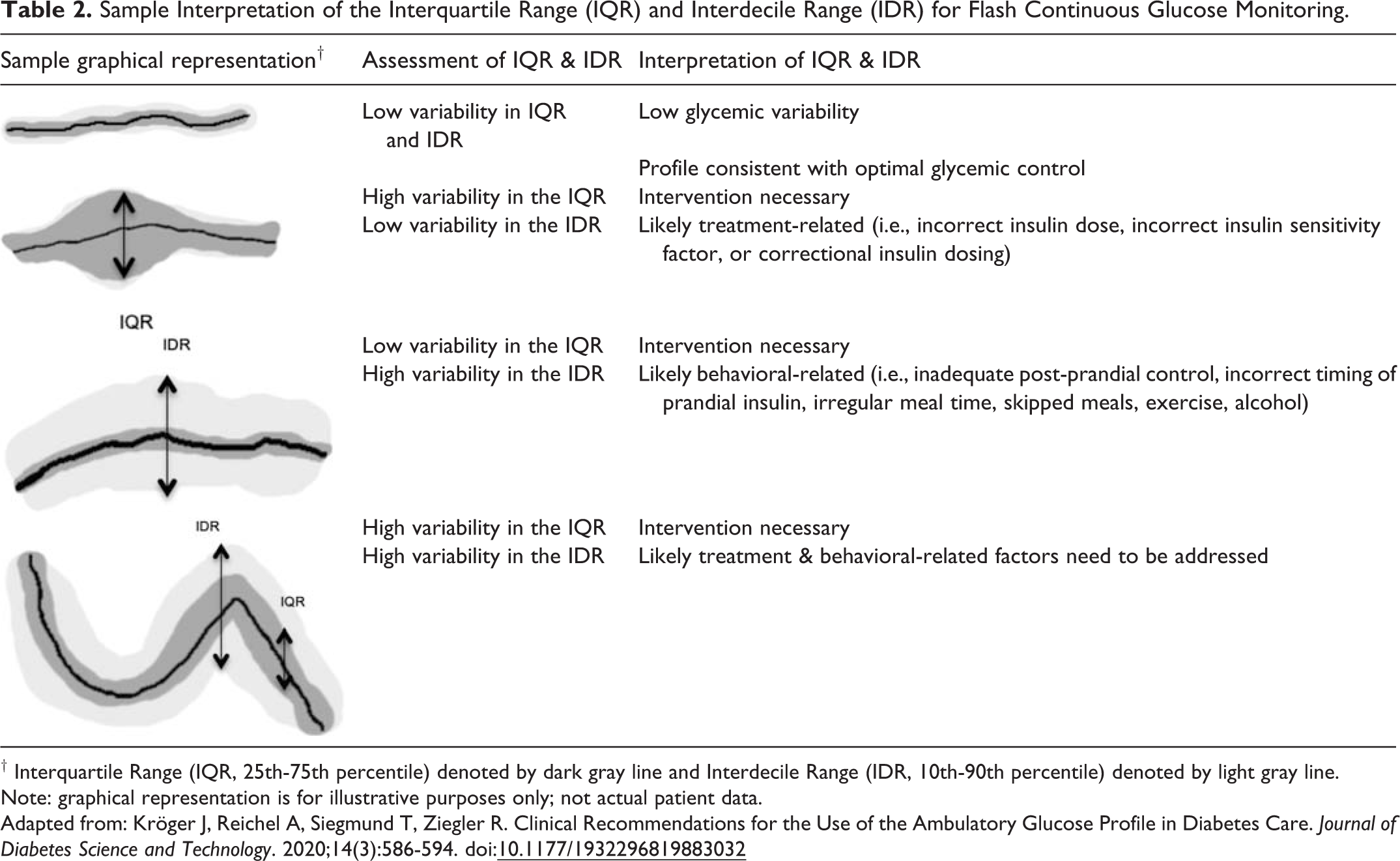
† Interquartile Range (IQR, 25th-75th percentile) denoted by dark gray line and Interdecile Range (IDR, 10th-90th percentile) denoted by light gray line.
Note: graphical representation is for illustrative purposes only; not actual patient data.
Adapted from: Kröger J, Reichel A, Siegmund T, Ziegler R. Clinical Recommendations for the Use of the Ambulatory Glucose Profile in Diabetes Care. Journal of Diabetes Science and Technology. 2020;14(3):586-594. doi:
Question 7. How can patients use trend arrows to inform treatment decisions?
Flash CGM is approved for non-adjunctive use, meaning the device is suitable for making therapeutic decisions (i.e., insulin dosing) by the patient based on the glucose data. However, the FreeStyle Libre® is not currently approved to be used in a hybrid closed-loop system where insulin dosing decisions are made passively based on CGM readings. When the flash CGM sensor is scanned, a trend arrow based on rate of change (ROC) of glucose is provided to the user. The ROC is calculated using the glucose levels per minute over the previous 15 minutes. 57 While this is a significant advancement in diabetes technology, the approach to using trend arrows from flash CGM to make clinical decisions is not without concerns.58,59 Therefore, some important caveats are necessary for the patient and pharmacist to understand prior to using, or recommending that treatment decisions be based on trend arrows. First, incorporation of trend arrow data to make treatment decisions from flash CGM has not been well studied in a controlled clinical trial. 58 In a study conducted by Freckmann and colleagues which included a small number of subjects using a flash CGM device, trend indicators did a poor job of matching future glucose change, notably within the first few hours of carbohydrate intake and insulin administration. 60 The majority of ROC indicators were shown to overestimate glucose change, which could lead to hypoglycemia. 60 Second, flash CGM is not well studied in patients not using insulin. Therefore, the recommendations for acting on trend arrows mainly apply to adults with diabetes using continuous subcutaneous insulin infusions (CSII) or multiple daily insulin injections. 61 Third, in order to make treatment decisions based on trend arrows, the patient must have a basic understanding of flash CGM, along with an understanding of how to use the insulin-to-carbohydrate ratio and correctional factors to dose insulin. 61 Although several experts have described various methods to base treatment decisions on trend arrow data,61-63 additional evidence is needed to better understand ROC with the flash CGM device.
Question 8. What is the optimal scanning frequency to recommend to patients?
When a flash CGM sensor is scanned by the user, an interstitial glucose reading, trend arrow (indicating glucose rate of change), and a small graph of the previous 8-hours of readings is provided. In a study conducted by Dunn and colleagues, estimated HbA1c decreased from 8% to 6.7% as flash CGM scan rate increased from the lowest to highest scan rate users (∼4 to ∼48 scans daily, respectively). 64 Flash CGM users with higher scan rates also had lower incidence of hypoglycemia. 64 Although optimal scan rate has not been determined, the previous data suggests that higher scan rates may be associated with improved glycemic control. It’s important to counsel patients that although flash CGM generates a new glucose value every minute and records the reading every 15 minutes, the sensor must be scanned at least every 8 hours to support a continuous stream of glucose data. 2 If more than 8-hours pass between the sensor being scanned, the only viewable glucose information will be from the most recent 8-hours before the last scan.
Question 9. Does flash CGM need to be calibrated?
Flash CGM is factory calibrated, and therefore does not require routine SMBG to verify accuracy of sensor readings. 8 However, it is important to recognize that flash CGM measures glucose from the interstitial fluid through a filament inserted in the subcutaneous tissue. 8 While glucose levels in the interstitial fluid correlate well with glucose levels in the blood, there are times (i.e., physical activity, hypoglycemia) when glucose levels are changing rapidly, which can result in a lag time in detecting hypoglycemia or hyperglycemia. 65 Lag times can range from 5 to 15 minutes. 66 Therefore, SMBG should be used in addition to flash CGM under these conditions to verify glucose levels.
Question 10. What are the risks associated with flash CGM use?
There are several reports of patient’s developing contact dermatologic reactions after applying the flash CGM sensor. 67 This is thought to originate from isobornyl acrylate, a compound found in the sensor. 68 However, the overall incidence of dermatologic complications from flash CGM use appears to be low based on available evidence (estimated to be 1 event per 8 weeks of sensor wear-time). 69 Additionally, the severity of dermatologic complications leading to discontinuation of flash CGM across several studies was low. 69 According to the manufacturer, local erythema, infection, inflammation, pain, discomfort, bruising, and scarring may occur at the site, although risk is low.
It is in the authors’ clinical experience that despite appropriate application, the flash CGM sensor may routinely fall off. This has also been documented in the literature. 20 To prevent periodic replacement of sensors, ensure that any soap, lotion, shampoo or conditioner is removed from the skin prior to application. 70 The skin should be cleaned with soap and water, dried thoroughly, and wiped with an alcohol pad prior to application. 70 Hair may also interfere with skin and sensor adhesion, so the site should clean-shaven. 70 In the event that this approach is followed and still not effective, a hypoallergenic and latex-free skin barrier (Skin Tac® or Mastisol®) can be applied in between the sensor and the skin surface. 70 Alternatively, bandages (i.e., Tegaderm®) can be applied over the sensor without interfering with communication of the sensor and scanning device. 70
Question 11. What is payer coverage for flash CGM?
Medicare eligibility for flash CGM at the time of writing requires a diagnosis of diabetes along with use of 3 or more insulin injections daily or 4 or more blood glucose checks daily. 71 Commercial payer criteria for flash CGM use can be similar to Medicare, but criteria for coverage can also vary. For example, some commercial insurers only provide coverage for patients with T1D. Therefore, each patient’s insurance plan should be reviewed for eligibility.
Question 12. What reimbursement opportunities exist for pharmacists?
Pharmacists are not currently recognized under title XVIII of the Social Security Act as providers, and are therefore not eligible to bill independently for clinical services under Medicare Part B. 72 For pharmacists working in ambulatory clinics, alternative mechanisms to receive indirect reimbursement exist through “incident-to” billing under the direct supervision of a recognized provider under Medicare Part B (i.e., physician, physician assistant, or nurse practitioner). 72 As shown in Table 3, pharmacists are eligible to bill “incident-to” a qualified health care provider for CPT codes 95249 or 95250. 19 A third code, CPT 95251, involves the interpretation and analysis of the flash CGM glycemic data. While pharmacists may collaborate with a provider to interpret, analyze and make recommendations based on flash CGM glycemic data, a physician or licensed non-physician provider is only allowed to bill for the “analysis and interpretation” (e.g., CPT 95251) at the time of writing. 19 Since some states (i.e., Washington and Tennessee at the time of writing) recognize pharmacists as providers under their state-run health plan, it is advisable to check with the local institutions compliance officer to inquire regarding billing considerations for CPT 95251. Nonetheless, since the average payment for CPT 95250 is $100 more than CPT 95251, there is an opportunity for pharmacists to create a financially sustainable practice model through providing education and placement of professional flash CGM devices (e.g., FreeStyle Libre Pro) as long as “incident-to” guidelines are followed.
Flash Continuous Glucose Monitoring Reimbursement and Billing Opportunities for Pharmacists.
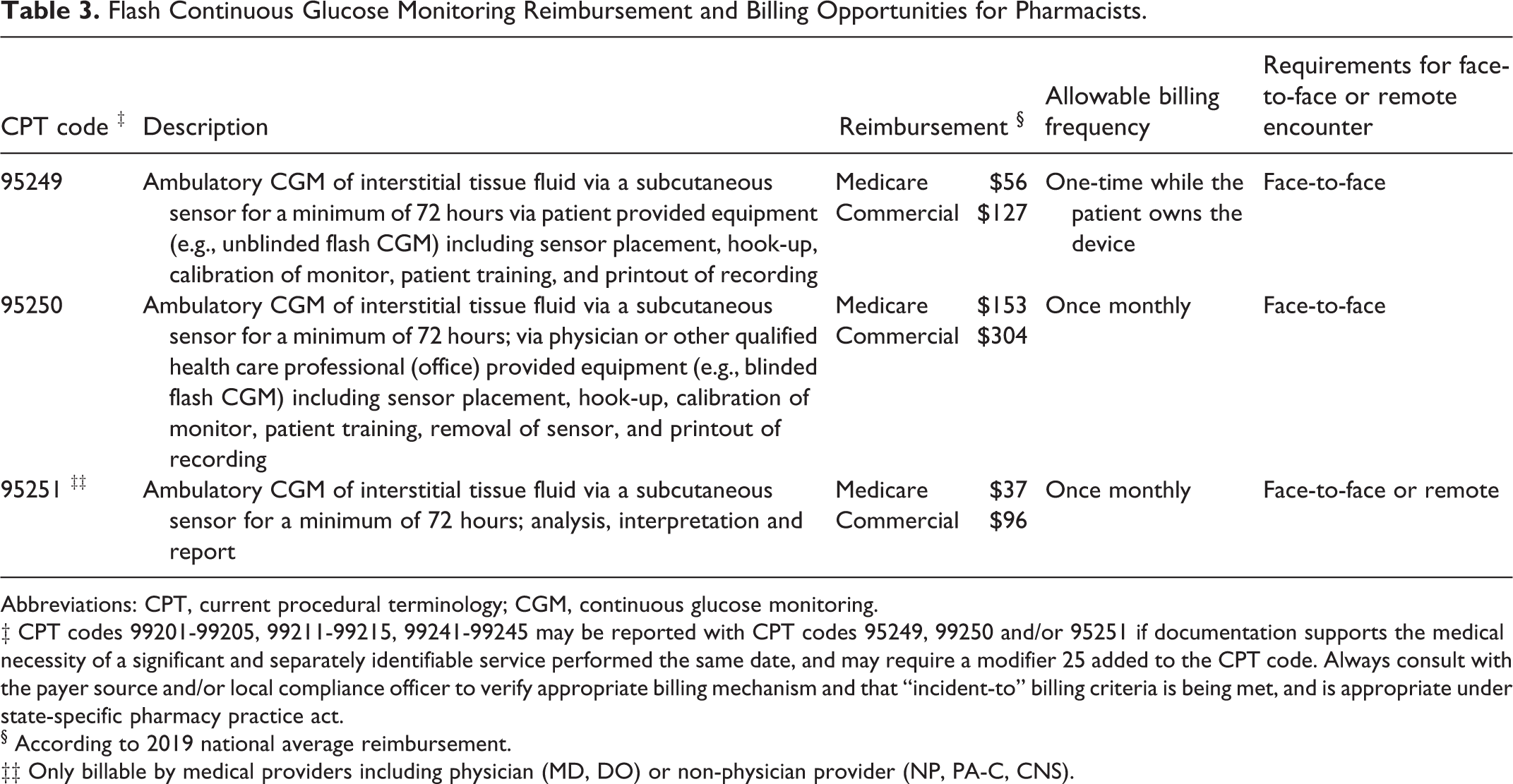
Abbreviations: CPT, current procedural terminology; CGM, continuous glucose monitoring.
‡ CPT codes 99201-99205, 99211-99215, 99241-99245 may be reported with CPT codes 95249, 99250 and/or 95251 if documentation supports the medical necessity of a significant and separately identifiable service performed the same date, and may require a modifier 25 added to the CPT code. Always consult with the payer source and/or local compliance officer to verify appropriate billing mechanism and that “incident-to” billing criteria is being met, and is appropriate under state-specific pharmacy practice act.
§ According to 2019 national average reimbursement.
‡‡ Only billable by medical providers including physician (MD, DO) or non-physician provider (NP, PA-C, CNS).
Call to Action
In summary, HbA1c and SMBG are currently the standard of care for assessment of glycemic control from a health policy and quality perspective. Widespread changes to policy and adoption of routine use of flash CGM to incorporate it’s additional glycemic metrics into patient assessment will require clinical evidence that this parameter is simple, feasible and correlates to relevant endpoints, such as reductions in microvascular or macrovascular complications. Recent evidence confirms correlations of TIR with diabetes complications,73,74 so we are likely to see increased adoption of these metrics into clinical practice as the clinical benefits from flash CGM are realized. In light of only 2 small, retrospective, pharmacist-driven CGM studies,20,21 there is a clear need for additional prospective analyses which evaluate the impact of pharmacist-driven CGM on meaningful outcomes such as attaining goal TIR, reductions in diabetes complications, as well as improved patient and provider satisfaction.
Despite advances in diabetes technology, the proportion of patients with T2D achieving recommended glycemic goals remains suboptimal. 75 Pharmacists are well positioned to collaborate with providers in ambulatory care or community-based settings to allow a greater number of patients with diabetes to harness the benefits of flash CGM. Interventions that close the knowledge and confidence gap in interpreting CGM data from the AGP are warranted. Further investigation into how trend arrows can be used by patients to support diabetes self-management is also necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.