
Abstract
Alemtuzumab is an anti-CD52 monoclonal antibody used to treat relapsing-remitting multiple sclerosis following failure of second-line medications. It is administered intravenously in 2 treatment sequences 1 year apart. This drug is frequently associated with mild infusion reactions within days of administration, increased infection risk, and long term adverse events from secondary autoimmunity. Alemtuzumab-induced serious immune-mediated thrombocytopenia (ITP) is well-reported and occurred in 1.0-2.2% of participants in initial phase 2 and 3 trials for multiple sclerosis. Significant neutropenia, however, is rare and was only observed in 0.1% of study participants. Delayed neutropenia and/or ITP is thought to occur from secondary autoimmunity. Few case reports have described severe neutropenia occurring beyond 2 months of last alemtuzumab dose. We present an unusual case of delayed combined neutropenia and thrombocytopenia that occurred 15 months after the second infusion of alemtuzumab. The patient was asymptomatic and presented following discovery of neutropenia and thrombocytopenia during routine laboratory studies. The patient responded to steroids initially and was discharged, although outpatient cell counts subsequently revealed recurrent neutropenia and ITP. The adverse drug reaction probability (Naranjo) scale was completed and showed probable likelihood that the adverse event was alemtuzumab-related. Long term screening for delayed hematologic abnormalities, at least 4 years after initial dose, is necessary when using alemtuzumab. Greater research is needed to understand the mechanism of drug-associated neutropenia.
Introduction
Relapsing-remitting multiple sclerosis (RRMS) is an uncommon and complex autoimmune condition which results in the destruction of myelin sheaths surrounding axons of the central nervous system (CNS) by inappropriately primed immune cells. This condition most frequently manifests in a relapsing-remitting fashion wherein the patient experiences rapid-onset focal CNS dysfunction and damage, followed by remission with partial recovery. Without disease-modifying treatment, recurrent relapses can cause progressive demyelination and neurodegeneration, leading to worsening disability. 1
The underlying principle of management of multiple sclerosis consists of disease modifying agents to prevent relapses through targeted immunosuppression and limiting neuronal damage if relapses occur. Disease modifying agents include immunomodulatory small molecules and cytokines such as interferon beta-1b, interferon beta-1a, glatiramer acetate, mitoxantrone, fingolimod, teriflunomide, laquinimod, azathioprine, and dimethyl fumarate. In the past 2 decades, targeted monoclonal antibodies such as natalizumab, alemtuzumab, daclizumab, ocrelizumab, and most recently, ofatumumab have been used for disease modifying treatment of RRMS.2,3 In acute relapse, glucocorticoids are the mainstay of treatment, with plasmapheresis reserved for severe cases refractory to glucocorticoid treatment. 4
Alemtuzumab is an anti-CD52 monoclonal antibody that is used when treatment failure from 2 or more conventional drugs occurs in the treatment of RRMS. 5 In pivotal phase 2 and 3 clinical trials, alemtuzumab significantly reduced the risk of disability from RRMS compared to interferon beta-1a.6,7 Alemtuzumab suppresses the immune system through depletion of circulating T and B lymphocytes via antibody and complement-dependent cytotoxicity. 7 The drug is administered intravenously at 12 mg daily for 5 consecutive days, followed by a second treatment of 12 mg daily for 3 consecutive days at 12 months. While the elimination half-life of alemtuzumab is relatively short at 2 weeks, the duration of action is long. 5 Depletion of both T and B cell populations occurs within weeks following the first administration and persists until repopulation begins thereafter, with B cells reaching baseline in 8.4 months, and T cells recovering by approximately 20 months post-infusion.5,7
Adverse effects from alemtuzumab include infusion reactions, increased risk of infection and secondary autoimmunity. The most common adverse effects noted in clinical trials were infusion-associated reactions, which occurred within 24 hours of initiation of alemtuzumab infusion.5,7,8 Delayed-onset secondary autoimmunity is thought to be due to repopulation with self-reactive B cells without sufficient regulatory signaling from T cells. 9 This begins to occur 1 month after infusion but can occur up to 5 years later; the thyroid gland is most commonly affected. 7 Currently, baseline thyroid function testing, a complete blood count with differential, and renal function testing is recommended prior to initiation of alemtuzumab therapy. After administration, thyroid function testing is recommended every 3 months, whereas complete blood count and renal function testing are recommended every month up to 48 months after last dose.5,9
Serious immune-mediated thrombocytopenia (ITP) (platelets < 150,000/µL) has been well documented with a reported incidence of 1.0-2.2%, with all reported cases presenting within 48 months of last dose.6,7,10 On the contrary, alemtuzumab-induced neutropenia (ANC < 1500/µL) was not well documented in initial phase 2 and 3 trials but has since been identified in a few case studies. Coincident thrombocytopenia and neutropenia are exceedingly rare. We present an unusual case of delayed-onset alemtuzumab-associated neutropenia with thrombocytopenia occurring 15 months after second alemtuzumab infusion.
Case
A 45-year-old male with RRMS and post-ablative hypothyroidism for Graves’ disease presented to the emergency department after routine outpatient laboratory studies revealed 2 weeks of worsening severe neutropenia and thrombocytopenia (Table 1). On admission, he complained only of worsening acne for several weeks. He denied having symptoms of RRMS exacerbation or a history of hematologic conditions. Physical examination revealed scattered petechiae over the left thigh and subjective right lower extremity paresthesia. The paresthesia was unchanged from prior examinations and there was no evidence of acute RRMS exacerbation.
Trend of Complete Blood Count With Differential.
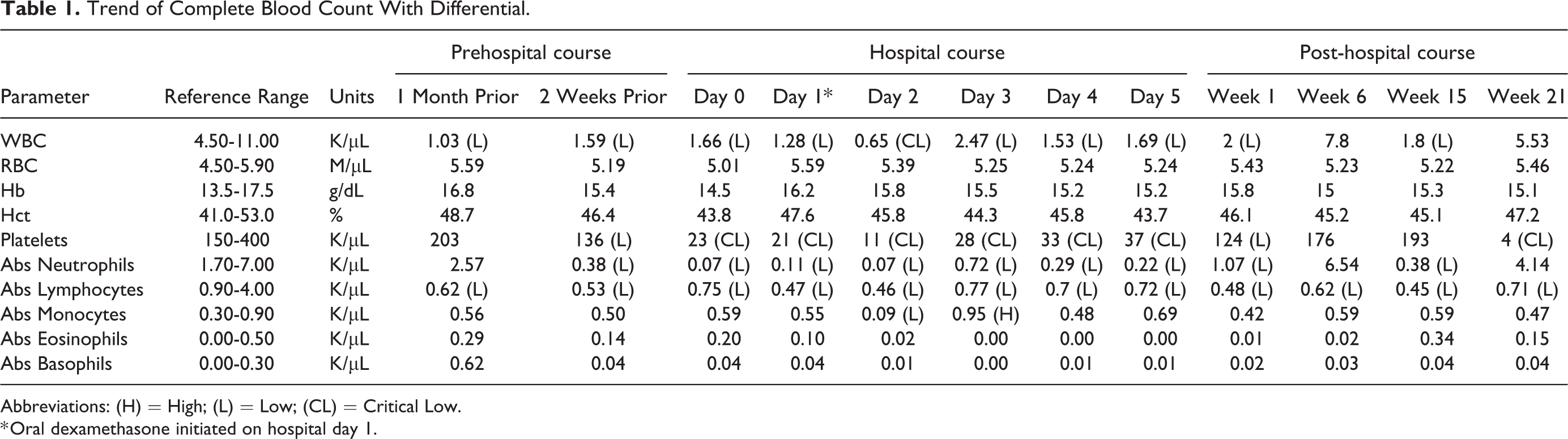
Abbreviations: (H) = High; (L) = Low; (CL) = Critical Low.
* Oral dexamethasone initiated on hospital day 1.
The patient received alemtuzumab for treatment of RRMS at 28 months and 15 months prior to presentation. His previous failed treatment protocols were; interferon beta due to development of neutralizing antibodies, fingolimod 9 years prior due to elevations in liver transaminases, and dimethyl fumarate 3 years prior due to John Cunningham virus. He also received intravenous immunoglobulin (IVIG) intermittently for 7 years prior to the initiation of alemtuzumab and declined treatment with rituximab. Of note, the patient’s Graves’ disease preceded the first alemtuzumab infusion by 10 months and methimazole was discontinued 5 months prior to the first infusion after thyroid ablation. Other medication history included a brief course of corticosteroids 4 months prior for an upper respiratory infection and a single dose of amoxicillin 1-month prior for prophylaxis prior to a dental procedure. His medications included bupropion 300 mg daily, gabapentin 300 mg 3 times a day, simvastatin 40 mg nightly, modafinil 200 mg daily and acyclovir prophylaxis. A drug-drug interaction was determined to be unlikely given that none of the patient’s current medications are known to produce thrombocytopenia or neutropenia.
Following his first dose of alemtuzumab (12mg/day for 5 days), he developed profound fatigue, otalgia, and sore throat 1-week post-infusion. All symptoms resolved spontaneously over the following week and did not recur. Monthly complete blood counts with differential (CBC) revealed absolute lymphopenia with a CD4 count <200 after first infusion, and acyclovir 400 mg twice daily was initiated for HSV prophylaxis, an anticipated infection risk of alemtuzumab therapy. The second dose was administered 15 months prior to presentation at 12 mg/day for 3 days without complications.
The patient was admitted (day 0) with an absolute neutrophil count (ANC) and platelet count of 70/µL and 23,000/µL respectively, after routine outpatient laboratory studies revealed 2 weeks of worsening severe neutropenia and thrombocytopenia (Table 1). Severe neutropenia was defined as less than 500/µL and thrombocytopenia was defined as less than 150,000/μL. On hospital day 2, the ANC and platelet count nadired at 70/µL and 11,000/µL respectively, with a hemoglobin of 15.8 g/dL. During this time there were no changes to his physical examination or signs of infection. The patient did admit to mild bleeding from the gums on hospital day 2 during the nadir of his platelet count, however this quickly resolved. Additional workup including vitamin B12, folate, fibrinogen, and haptoglobin were within normal limits. Anti-hepatitis A, B, and C IgM, and HIV screening were negative. Peripheral blood smear showed absolute neutropenia and lymphopenia but no blasts or atypical promyelocytes. Flow cytometric analysis of peripheral blood was unremarkable. A bone marrow biopsy revealed mild hypocellularity without evidence of dysplasia, leukemia or chromosomal abnormalities.
The patient remained neutropenic but afebrile throughout admission. Dexamethasone therapy was initiated on hospital day 1 at 40 mg daily for 4 days and he was discharged on prednisone 60 mg daily with close follow up by hematology consultants. One month after discharge, the patient’s petechiae, absolute neutropenia, and thrombocytopenia resolved (Table 1) and prednisone was tapered and discontinued.
Four months after admission, routine bloodwork revealed recurrence of neutropenia with a leukocyte count of 1800/µL and ANC of 385/µL. Prednisone 20 mg daily was restarted and neutropenia resolved after 1 month; however, he required readmission for recurrent ITP with platelets of 4000/µL. Thrombocytopenia resolved within 1 week following 2 infusions of IVIG and dexamethasone 40 mg daily. Current maintenance therapy is prednisone 10 mg daily. The patient is asymptomatic in regard to his RRMS and no future treatment is planned at this time.
Discussion
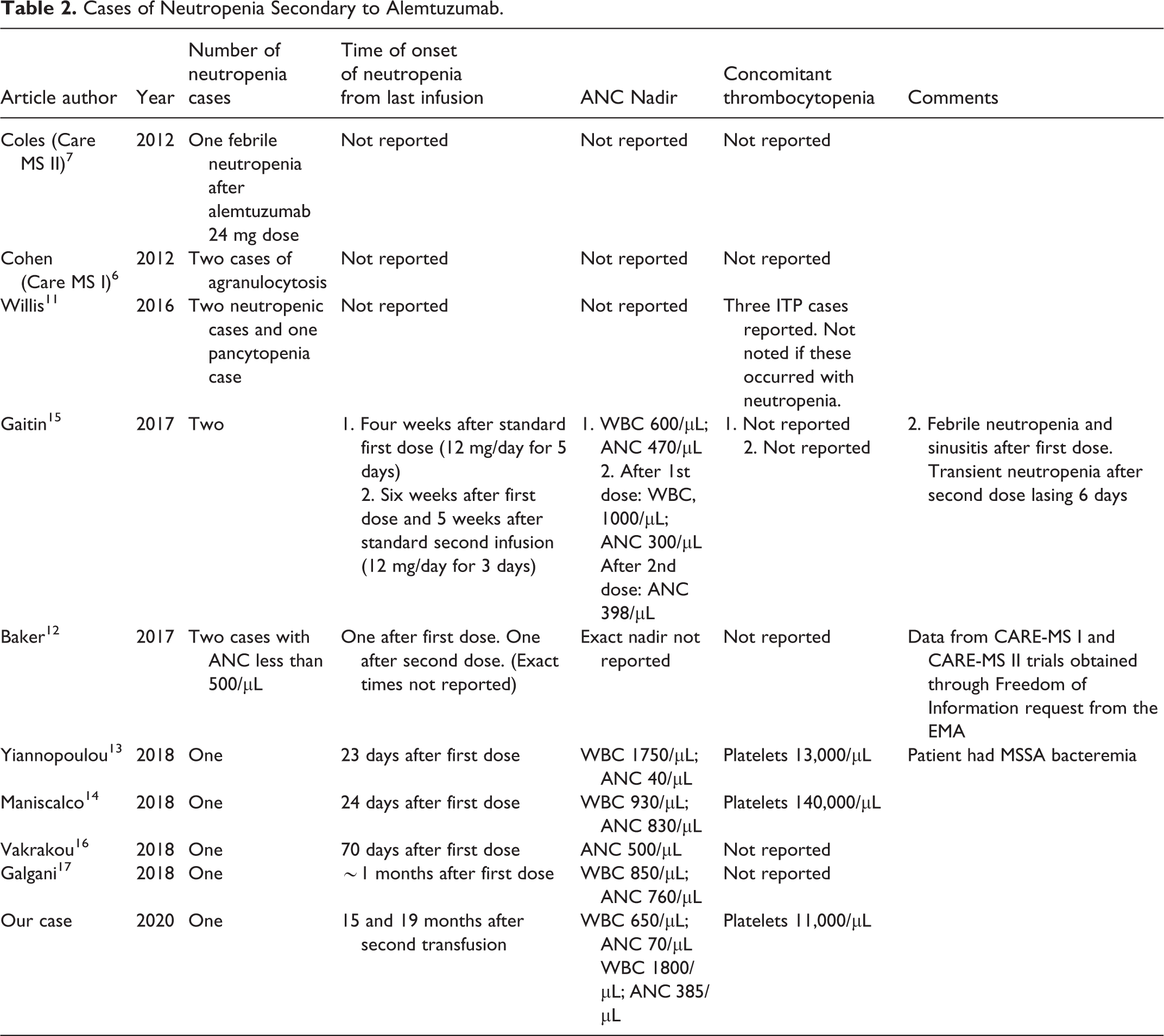
Delayed thrombocytopenia, as long as 48 months, is a well-reported adverse reaction following alemtuzumab, but very few reports of concurrent neutropenia as an adverse reaction have been reported, especially with delayed onset as seen in this case (Table 2). 10 In the pivotal trials of alemtuzumab in RRMS, CARE MS I and II, 2 cases of agranulocytosis and one case of febrile neutropenia were reported without details of timing of occurrence or magnitude. A third case of presumed autoimmune pancytopenia occurred 6 months after treatment and resulted in death after noncompliance with corticosteroid therapy. 11 Baker et al. evaluated the degree of neutrophil depletion in the cohorts of CARE MS I and II using data from the European Medicines Agency (EMA) regulatory submission and concluded grade 4 neutropenia (< 500/μL) occurred in only 2 cases (Table 2). 12 In 2016, Willis et al. looked at long term follow up of alemtuzumab across 3 centers in the UK and noted 2 cases of neutropenia and one case of pancytopenia. Most autoimmune disorders in this study were within 5 years of last treatment but details of timing or severity of neutropenia were not reported. 11 Since then, an additional 8 cases have been reported, within 2.5 months of alemtuzumab dosing (Table 2). Only 3 cases describe combined neutropenia and thrombocytopenia; 2 at 23 and 24 days after first infusion and one with unknown time of onset.11,13,14 Interestingly, our patient complained of new acne which was also reported in one other case. 14
Cases of Neutropenia Secondary to Alemtuzumab.
There are multiple hypotheses regarding the etiology of neutropenia in association with alemtuzumab. Neutropenia that occurs shortly after alemtuzumab administration (less than 1 month) is thought to be secondary to direct bone marrow toxicity since alemtuzumab targets CD52 which is expressed by polymorphonuclear neutrophils.12,18 Alternately, alemtuzumab is also known to cause secondary B-cell autoimmunities due to immune reconstitution and autoreactivity after depletion from the drug; specifically, autoreactivity may occur through B-cell reconstitution prior to T regulatory and suppressor cell return. 12
We suggest that concurrent neutropenia and thrombocytopenia in this case represents a secondary autoimmune event. Utilizing the Naranjo Algorithm to quantify the likelihood of an adverse reaction resulted in a score of 6, or probable likelihood of an adverse drug reaction (addendum). 19 Prior to this case, the longest reported delay of neutropenia alone was 2.5 months after the first dose and a little over 1 month after the second dose.15,16 This case presents a delay of 15 months following last infusion and is one of very few reported cases of combined thrombocytopenia and neutropenia.
It is unlikely that previous treatments and current medications were implicated as a cause of the delayed neutropenia and thrombocytopenia. The most recent disease-modifying agent was last administered greater than 27 months prior and his most recent course of steroids was a low dose taper for an upper respiratory infection 4 months prior. Per literature review, interferon has not been associated with neutropenia. Fingolimod has been associated with ITP during use of the drug. 20 After discontinuation of the drug, one study noted no neutropenia less than 1000/µL after 3 years and another study noted no neutropenia after 12 months.16,21 Dimethylfumarate can cause neutropenia while taking the medication but no delayed neutropenic effect has been reported. 22 IVIG can also induce immediate neutropenia that resolves in 1-2 weeks.23,24 One case report demonstrated neutropenia after a 5 day course of amoxicillin/clavulanic acid secondary to direct bone marrow toxicity. 25 Contrarily, our patient took a single dose. Lastly, we found only one case report of neutropenia and thrombocytopenia with acyclovir usage; the case detailed a child with an acute viral infection whose neutropenia/thrombocytopenia resolved after resolution of the infection and discontinuation of acyclovir 200 mg BID. 26 Other reports of concurrent neutropenia and thrombocytopenia secondary to acyclovir or his other current medications are lacking. Overall in the literature, none of these drugs have been associated with late neutropenia and thrombocytopenia from secondary autoimmunity.
Conclusion
Concurrent neutropenia and ITP is a rare adverse event secondary to alemtuzumab in the treatment of RRMS and can occur as late as 15 months after last transfusion. Alemtuzumab was implicated in this case for multiple reasons. First, laboratory workup and bone marrow biopsy ruled out other potential secondary causes of neutropenia and ITP. Literature review of the patient’s prior disease modifying agents and current medications did not reveal reports of combined and late neutropenia and thrombocytopenia. Additionally, a Naranjo adverse drug reaction score indicated that the likelihood of alemtuzumab inducing these adverse events was “probable” with a score of 6. Lastly, successful treatment with steroids and IVIG suggests an autoimmune component in the nature of the disease.
Secondary autoimmunity occurs with repopulation of self-reactive B cells without sufficient regulatory signaling from T cells and is a known adverse effect of alemtuzumab. It is likely that this patient’s delayed neutropenia and ITP were due to secondary autoimmunity, but greater research is needed to understand the exact mechanism of delayed neutropenia. It remains important to monitor CBC well after administration of the last dose of alemtuzumab. Current recommendations suggest surveillance with CBC, serum creatinine and urine analysis up to 48 months after last treatment dose.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.