
Abstract
Background
Rapid sequence intubation (RSI) is a stepwise process that includes the successive administration of an induction and neuromuscular blocking agent (NMBA) in order to quickly secure an emergent airway.1,2 Rocuronium is an intermediate-acting non-depolarizing NMBA frequently used in the emergency department (ED) for RSI and is often selected over succinylcholine, a depolarizing NMBA, in an effort to avoid potential adverse effects. 3 Compared to succinylcholine, rocuronium has a longer duration of action, 45–70 minutes vs 5–15 minutes.2,4 Additionally, several factors may prolong the duration of action of rocuronium such as patient age, comorbidities, pharmacokinetic interactions, and a dose-dependent neuromuscular blocking effect. 5 The prolonged effects of rocuronium may prevent the ability to conduct a meaningful neurological examination, thereby delaying appropriate diagnosis and treatment. However, rocuronium-induced neuromuscular blockade can be overcome via pharmacologic intervention, allowing for more timely evaluation by clinicians.6,7
Neostigmine, a cholinesterase inhibitor, has traditionally been used to reverse the effects of non-depolarizing NMBAs.7,8 Neostigmine administration, however, increases susceptibility to cholinergic adverse effects such as bradycardia, hypotension, bronchoconstriction, nausea, and vomiting.7,8 Therefore, a muscarinic antagonist, such as glycopyrrolate, should be administered prior to or with neostigmine in order to mitigate these cholinergic effects.7-9 Additionally, patients with specific co-existing conditions such as coronary artery disease, cardiac arrhythmias, recent acute coronary syndrome, and myasthenia gravis may be at an increased risk for adverse reactions. 7 Alternatively, sugammadex, a modified gamma-cyclodextrin, forms a complex with rocuronium in the serum, reducing the amount of NMBA available to bind to nicotinic cholinergic receptors. 6 In contrast to neostigmine and other cholinesterase inhibitors, sugammadex does not produce cholinergic effects. 8 However, adverse effects such as hypotension and bradycardia have been observed after its use.6,8,10 By decreasing the amount of paralytic available in a dose-dependent manner, sugammadex provides the ability to quickly and reliably reverse deep neuromuscular blockade after rocuronium administration.10,11 Neostigmine, on the other hand, is mostly unable to quickly or reliably reverse deep neuromuscular blockade. 9
Current evidence comparing the efficacy and safety of sugammadex vs neostigmine with glycopyrrolate in adults is primarily limited to those who received non-depolarizing NMBAs for elective inpatient or day-case surgical procedures. 8 The safety of sugammadex vs neostigmine with glycopyrrolate for the reversal of rocuronium in the ED has not been well described. The primary objective of this study was to evaluate hemodynamic instability that required escalation of treatment following administration of sugammadex or neostigmine with glycopyrrolate in the ED for the reversal of rocuronium.
Methods
This was a single-center, retrospective, cohort study of adult patients that received sugammadex or neostigmine with glycopyrrolate in the ED for the reversal of rocuronium between January 1, 2015 and November 30, 2020. Patients were identified based on medication administration documentation of sugammadex or neostigmine in the ED after receiving rocuronium in the ED or prior to arrival. This cohort included patients ≥18 years of age who received one dose of either sugammadex or neostigmine concurrently with glycopyrrolate in the ED. Patients were excluded if medication administration records or medical records were incomplete, patients received both sugammadex and neostigmine, or neostigmine was administered without glycopyrrolate. Local institutional review board approval was obtained via expedited review.
The primary objective of this study was to determine the occurrence of hemodynamic instability that required escalation of treatment within 30 minutes of receiving either sugammadex or neostigmine with glycopyrrolate in the ED for the reversal of rocuronium. Escalation of treatment was defined as the use of one or more of the following: initiation or increased infusion rate of a vasopressor, administration of one or more push doses of phenylephrine or epinephrine, or administration of atropine. Secondary outcomes include incidence of hypotension (at least one measured systolic blood pressure ≤90 mmHg), bradycardia (at least one measured heart rate ≤60 beats per minute), or cardiac arrest events within 30 minutes of sugammadex or neostigmine with glycopyrrolate administration.
Manual chart review was performed and data were entered into a REDCap® database (Vanderbilt University, Nashville, TN). The following data points were extracted: age, sex, weight, height, body mass index (BMI), temperature, blood pressure, and heart rate before and after administration of sugammadex or neostigmine with glycopyrrolate, train of four (TOF) assessment, initial Glasgow Coma Scale (GCS), and initial serum creatinine. Additional data points included paralytic administered in ED vs pre-hospital and time between paralytic dose and administration of sugammadex or neostigmine. Medication-related information collected included dosing of sugammadex, neostigmine, glycopyrrolate, and rocuronium. Specific vasopressor dose and infusion rate was also collected.
For categorical variables, frequencies and column percentages were reported and P values were calculated utilizing Fisher’s exact tests. For all other variables, medians and first and third quartiles (Q1, Q3) were reported. P values ≤.05 were considered statistically significant. Missing observations were reported and excluded on an analysis-by-analysis basis. All statistical analysis was conducted utilizing STATA Statistical Software: Release 16 (StataCorp LLC, College Station, TX).
Results
Patient Characteristics.
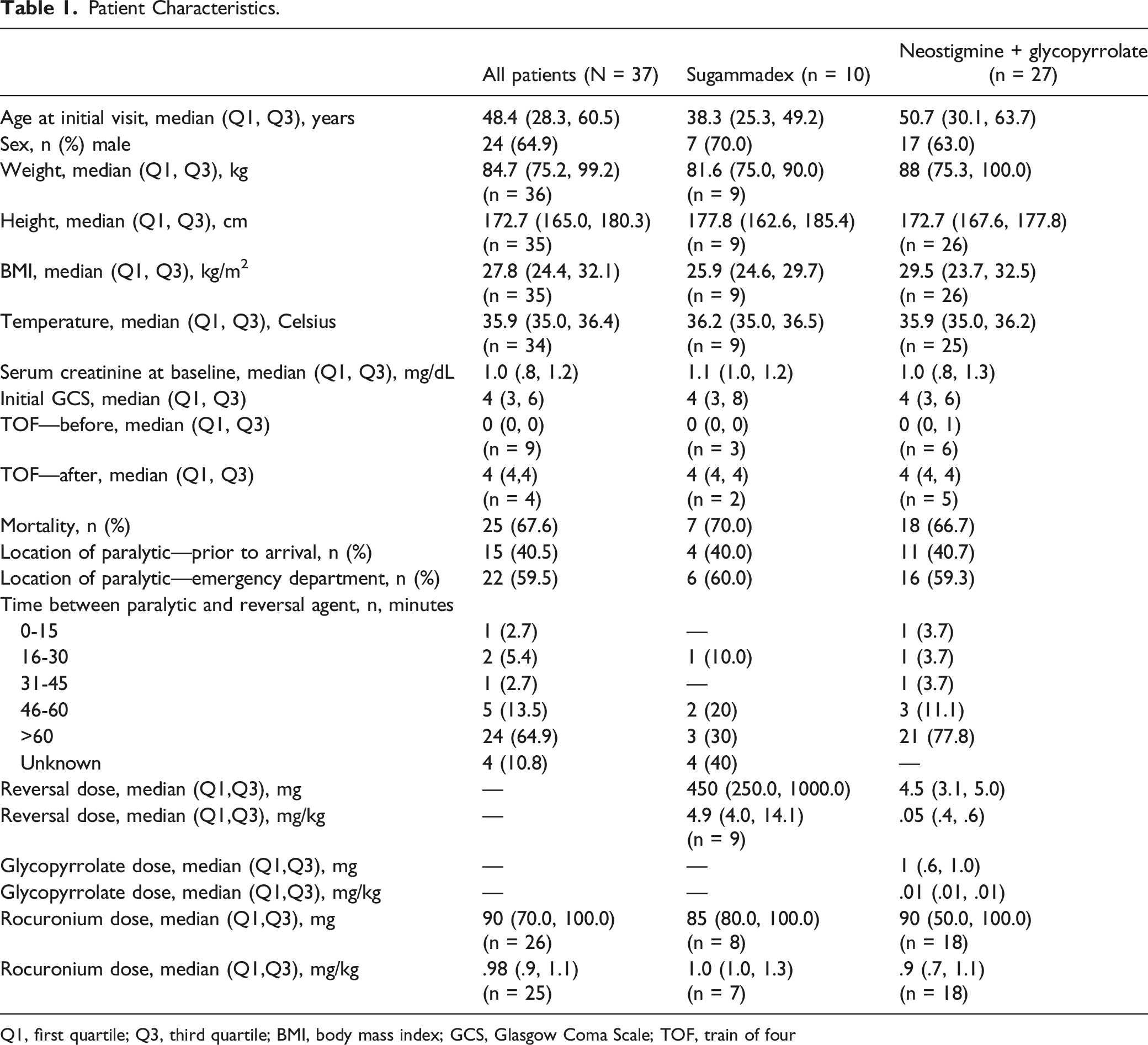
Q1, first quartile; Q3, third quartile; BMI, body mass index; GCS, Glasgow Coma Scale; TOF, train of four
Patient Outcomes.
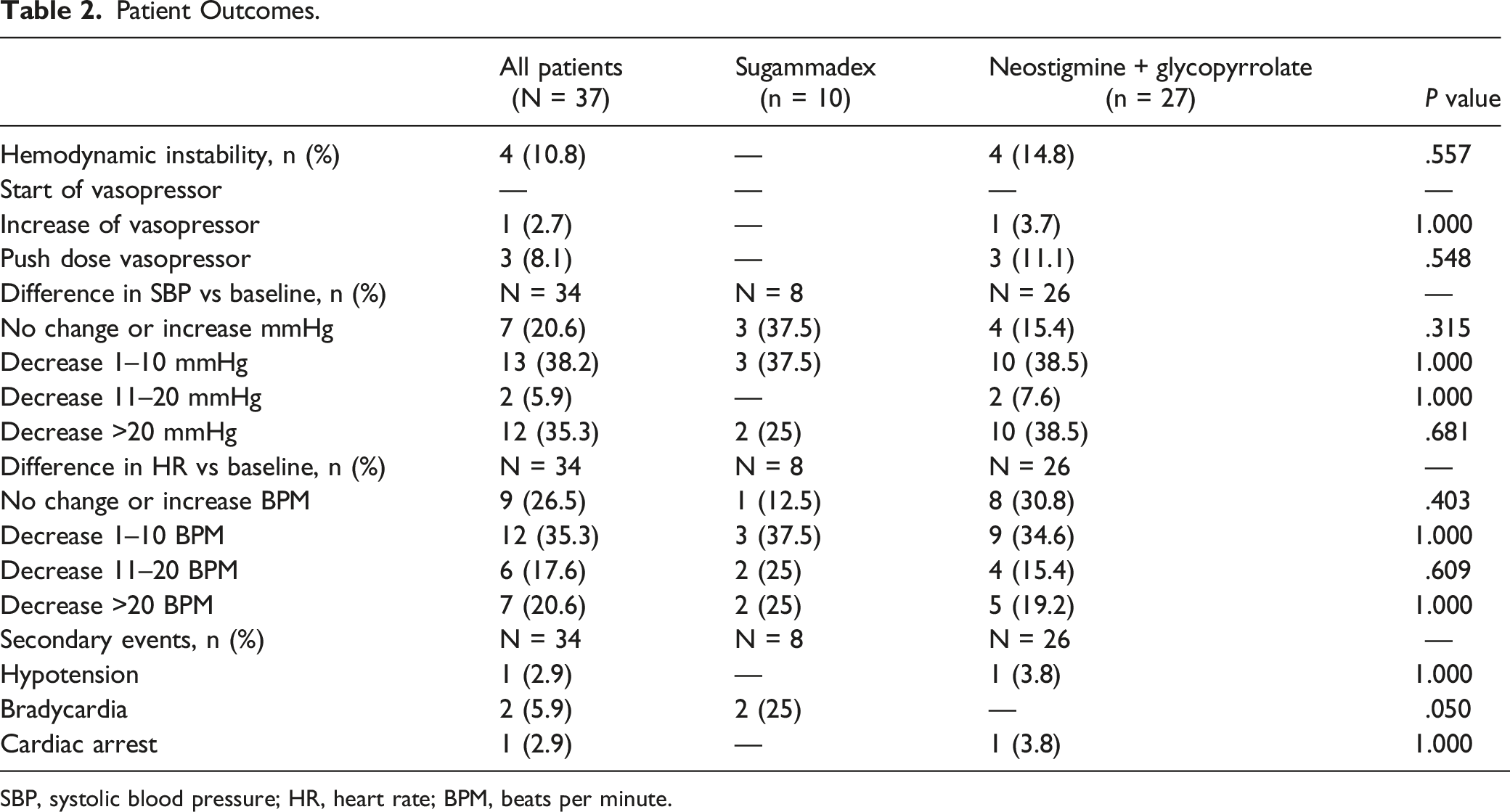
SBP, systolic blood pressure; HR, heart rate; BPM, beats per minute.
Discussion
In this single-center, retrospective, cohort study involving patients who received sugammadex or neostigmine with glycopyrrolate for the reversal of rocuronium, there was no statistically significant difference between the two groups in regard to occurrence of hemodynamic instability that required escalation of treatment. The indications for rocuronium reversal were to conduct meaningful neurological examinations, thereby quickly determining appropriate diagnosis and treatment options. Overall, the majority of our study’s population suffered from heterogeneous intracranial hemorrhages (ICHs) secondary to blunt and penetrating traumatic brain injuries (TBIs), as well as spontaneous, nontraumatic bleeding. The mortality rate in our study was high, yet expected, given mechanism of injury and high case fatality rate of intracerebral hemorrhages. 12 In those that survive the initial traumatic event, secondary insults such as hypoxia, hypotension, hematoma expansion, cerebral edema, brain compression, intracranial hypertension, seizures, and fever may occur, thus influencing clinical outcomes. Additionally, given the varying mechanisms and severity of injuries of this population, patients may experience hemodynamic instability, regardless of pre-hospital care and initial management in the ED. 13
The exact mechanism(s) of sugammadex-induced cardiovascular and hemodynamic instability remains unclear but reactions have been reported resulting in varying degrees of severity and hemodynamic response. 14 Additional cardiovascular events, such as profound bradycardia, transient third-degree atrioventricular block, and cardiac arrest have been reported following sugammadex administration.6,15-18 These adverse effects are thought to be transient and dose related. 19 The median weight-based dose of sugammadex in our study was 4.9 mg/kg. The recommended dose for the reversal of rocuronium-induced paralysis ranges from 2 to 16 mg/kg dependent on depth of paralysis (e.g.,, post-tetanic counts (PTC) and TOF stimulation), urgency of reversal, and dose and timing in relation to rocuronium administration.6,10
Furthermore, evidence of prolongation of the corrected QT interval (QTc) has been recognized; however, the clinical significance of these electrocardiogram (ECG) changes are thought to be minimal.20,21 The ability to obtain a timely ECG in this patient population and setting may be difficult. In our study, both patients that experienced a bradycardic event did not receive an ECG prior to or immediately following the administration of sugammadex. Cardiovascular collapse and hemodynamic instability may also present as hypotension.20,22,23 Therefore, atropine and vasoactive medications should be readily available for administration.6,15,16,19 Increases in coagulation parameters, activated partial thromboplastin time (aPTT), and prothrombin time/international normalized ratio [PT (INR)] have been observed following the administration of sugammadex. Although these changes likely do not translate to clinically significant bleeding and hemodynamic compromise, they may complicate the clinical scenario.24,25 One patient in our study was on apixaban (Eliquis®) for prior deep vein thrombosis. Prior to administration of sugammadex, the patient’s INR and PT were elevated at 1.81 and 25.6 seconds, respectively. However, subsequent lab values after the administration of sugammadex were normalized, likely secondary to the patient receiving 4-factor prothrombin complex concentrate (Kcentra®).
All patients in our study who received neostigmine concurrently received glycopyrrolate.7,8 The median total doses of neostigmine and glycopyrrolate in our study were 4.5 mg (.05 mg/kg) and 1.0 mg (.01 mg/kg), respectively. The recommended dose for neostigmine for reversal of NMBAs with shorter half-lives (e.g.,, rocuronium) is .03 mg/kg and .07 mg/kg for longer half-lives (e.g.,, vecuronium and pancuronium), maximum 5 mg. 7 Glycopyrrolate dosage for prevention against muscarinic adverse effects of cholinergic agents used for the reversals of NMBAs is .2 mg for each 1 mg of neostigmine, maximum 1 mg. 9 Although our study found no difference between the two groups in regard to the occurrence of hemodynamic instability, 4 patients in the neostigmine group required escalation of therapy. One individual experienced a pulseless electrical activity (PEA) cardiac arrest event; however, this may have occurred secondary to the severity and mechanism of injury and not related to medication administration.
The majority of the patients in our study received sugammadex or neostigmine with glycopyrrolate greater than 60 minutes after rocuronium administration. Several factors may prolong the duration of action of rocuronium such as age, weight, comorbidities, renal function, temperature, pharmacokinetic interactions, and dose-dependent neuromuscular blocking effect.5,26 The mean duration of rocuronium at higher doses (.9 mg/kg-1.2 mg/kg) have been shown to be between 53 and 73 minutes. 27 The median dose of rocuronium in our study in the sugammadex group was 1.0 mg/kg and .9 mg/kg in the neostigmine group. Additionally, the weight used to calculate the patient’s rocuronium dose in our study was actual body weight. The duration of action of rocuronium may be prolonged in overweight and obese patients when actual body weight is used vs other methods.28-30
Given the single-center, retrospective design of this study, inherent limitations such as the possibility for confounding factors and patient selection bias may exist. Concomitant administration of blood products, fluids, or additional medications in pre-hospital setting and within the ED may alter hemodynamic parameters. Injury-related hemodynamic changes not related to medication adverse effects cannot be ruled out. Additionally, our study’s sample size is small with a majority of patients suffering from heterogeneous ICHs secondary to blunt and penetrating traumatic brain injuries (TBIs), as well as spontaneous, nontraumatic bleeding, potentially limits the generalizability of our results. The lack of documentation of the TOF assessment limited the ability of our study to compare the effectiveness of sugammadex and neostigmine with glycopyrrolate. Although no formal documentation was required, it is common practice for a TOF assessment to be conducted to ensure appropriateness of medication administration. Furthermore, the ability to complete a timely and accurate TOF assessment in the ED setting may be an additional limitation in some scenarios.10,11 Additionally, no institution-specific protocol exists to determine which medication is utilized, or which specific monitoring parameters are measured post-administration. Despite these limitations, this study may serve as guidance for institutions that are evaluating the use of sugammadex or neostigmine with glycopyrrolate for the reversal of rocuronium in the ED.
Further institution-specific considerations may include product availability, financial implications, or other restrictions that hinder the use of these agents in the ED. Economic evaluations and cost-effectiveness analyses of sugammadex compared to neostigmine focus on the potential financial benefits of sugammadex in terms of time saved in the operating room (OR) and peri-operative settings.31-33 However, medication acquisition costs and extrapolation of these potential financial benefits to the ED setting should be considered.
The objective of this study was to evaluate the occurrence of hemodynamic instability post-administration of sugammadex vs neostigmine with glycopyrrolate in the ED for the reversal of rocuronium. These data did not demonstrate a difference in the likelihood of developing hemodynamic instability requiring escalation of therapy following sugammadex vs neostigmine with glycopyrrolate administration. Although the mechanism(s) of sugammadex-induced cardiovascular collapse has not been well defined, clinicians in the ED should be attentive to the risk of hemodynamic changes similar to those receiving neostigmine. 19
Conclusion
In this single-center retrospective cohort study of patients receiving sugammadex or neostigmine with glycopyrrolate for the reversal of rocuronium, there was no difference in the occurrence of hemodynamic instability requiring escalation of treatment. Given the small sample size, future studies are warranted to further delineate the roles of sugammadex and neostigmine with glycopyrrolate in the ED.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.