
Abstract
Background
Literature has shown the integration of electronic alerts into patient care has the potential to improve clinicians’ workflow by saving time, increasing efficiency, and improving patient safety. However, despite these possible benefits of alerts, studies have shown that alerts are often overridden by clinicians.
Background and Significance
There has been a rapid increase in the use of computerization within healthcare that has benefited clinicians and patients. Many healthcare organizations utilize tools within the electronic medical records (EMR) in order to assist clinicians at the point-of-prescribing. The integration of electronic alerts into patient care has the potential to improve clinicians’ workflow by saving time, increasing efficiency, and improving patient safety. However, despite these possible benefits of alerts, studies have shown anywhere from 49 to 96% of alerts are overridden by clinicians.1,5
Many barriers to the acceptance of electronic alerts can be identified based on existing literature and pharmacists’ experiences with clinical informatics.2,3 Informatics pharmacists may help to improve the acceptance of electronic alerts by helping to build, implement, and maintain alerts and technology within the EMR in order to optimize pharmacy practice, medication use, clinical decision-making, and patient safety outcomes. 6 However, lack of awareness of clinical guidelines, unfamiliarity with the high cost of medications, or disagreement with the suggestion can all lead to clinicians’ refusal.2-4 Furthermore, alert fatigue, which is the desensitization that occurs with the notification of too many warnings or alerts, may have a significant impact on alert acceptance.1,4
At Atrius Health, the acceptance rate of homegrown medication point-of-prescribing alerts has historically been 3%, which is slightly lower than what is seen in the current literature. Various organizations have recognized that they had low acceptance rates, made improvements as a result, and noticed an increase in their acceptance rate.4,7,8 Shah, et al. showed that minimizing clinicians’ workflow disruptions and keeping only alerts for drug contraindications of high clinical importance on, which led to a higher acceptance rate. 7 Wright et al. demonstrated that switching from a highly tailored alerting system to a more general one may decrease the acceptance rate of alerts and increase alert burden on users. 8 At Atrius Health, we identified a subset of point-of-prescribing alerts on high-cost medications and made changes to optimize the alert while providing an equally safe and effective low-cost alternative medication. In doing so, our goal was to increase alert acceptance rate and thereby limiting the prescribing of high-cost medications, reducing drug costs for the organization and patients, and showcasing the role of informatics in clinical pharmacy to help improve prescribing patterns.
Objective
The purpose of this study is to assess and optimize existing point-of-prescribing alerts within the EMR to increase the acceptance rate of high value alerts. Consequently, it may help with cost-savings, reduce alert fatigue, and make point-of-prescribing clinical decision tools more efficient.
Materials and Methods
This study was conducted at Atrius Health, a nonprofit, multi-site, ambulatory care organization that delivers care across 31 medical practice locations, serving over 740,000 adult and pediatric patients across Eastern Massachusetts. The protocol for this prospective, observational, single center study was approved by the Institutional Review Board at MCPHS University and Atrius Health.
Design
The clinical pharmacy informatics team evaluated 101 homegrown medication point-of-prescribing alerts and examined the estimated annualized cost-savings of switching high-cost medications to a lower cost alternative. The primary outcome was to determine whether optimization of high value alerts with low acceptance rates would lead to an increase in the alert acceptance rate at the point-of-prescribing. The exploratory outcome was to determine the estimated health system cost-savings when a point-of-prescribing alert was accepted and an alternative, less expensive medication was prescribed. Estimated health system cost-savings were calculated using the primary outcome, and the average expected unit cost of each prescription.
Medication point-of-prescribing alerts with high clinical significance were defined as those that provided a safer or more effective alternative medication. High value alerts were defined as a medication point-of-prescribing alert for which the suggested alternative medication would result in an annual savings of ≥$1000 for chronic therapy or cost ratio of ≥50:1 for short course therapy. The alerts compared the monetary value of high-cost medications that were being ordered to lower cost alternatives. Informative point-of-prescribing alerts that provided only prescribing guidance to clinicians with no suggested alternative medication option were excluded, as acceptance rates could not be assessed. Additionally, point-of-prescribing alerts that were created after Quarter 1, 2019 were excluded in order to directly compare Quarter, 12 019 to Quarter, 12 020. No new alerts were created throughout the study. All patients within Atrius Health’s EMR could potentially be participants with no exclusion criteria. The exploratory outcome criteria included any point-of-prescribing alerts with cost-savings alternatives that fire during the study timeframe.
The design and content of all alerts were streamlined and optimized in an effort to increase alert acceptance. Alert acceptance rate is defined as a measure of the rate at which clinicians choose to accept the alert to substitute an alternative medication and was also calculated as an exploratory outcome during the intervention.
When a medication point-of-prescribing alert fires within the EMR, clinicians have the option to (1) Accept the alert: select one of the suggested alternatives, (2) cancel the alert: prescribe no medication, or (3) continue through the alert: dismiss the alert and prescribe the original medication.
Data Collection
The study timeframe included a pre-modification period, Quarter 1, 2019 (January 1st, 2019–March 31st, 2019) as well as a post-modification period, Quarter 1, 2020 (January 1st, 2020–March 31st, 2020). Data on all alerts that fired at the point-of-prescribing during these time periods as well as clinician response (accept, cancel, or continue) were pulled from the EMR, EpicCare®, and stored within Microsoft® Excel®.
Intervention
All point-of-prescribing alerts were assessed and analyzed based on the clinical significance and costs. The design and content of all alerts were optimized to provide concise and clear instructions to help with clinicians’ decision-making and aid them to accept an alternative medication. Figure 1 shows the alert design prior to modification. Alert prior to alert modification.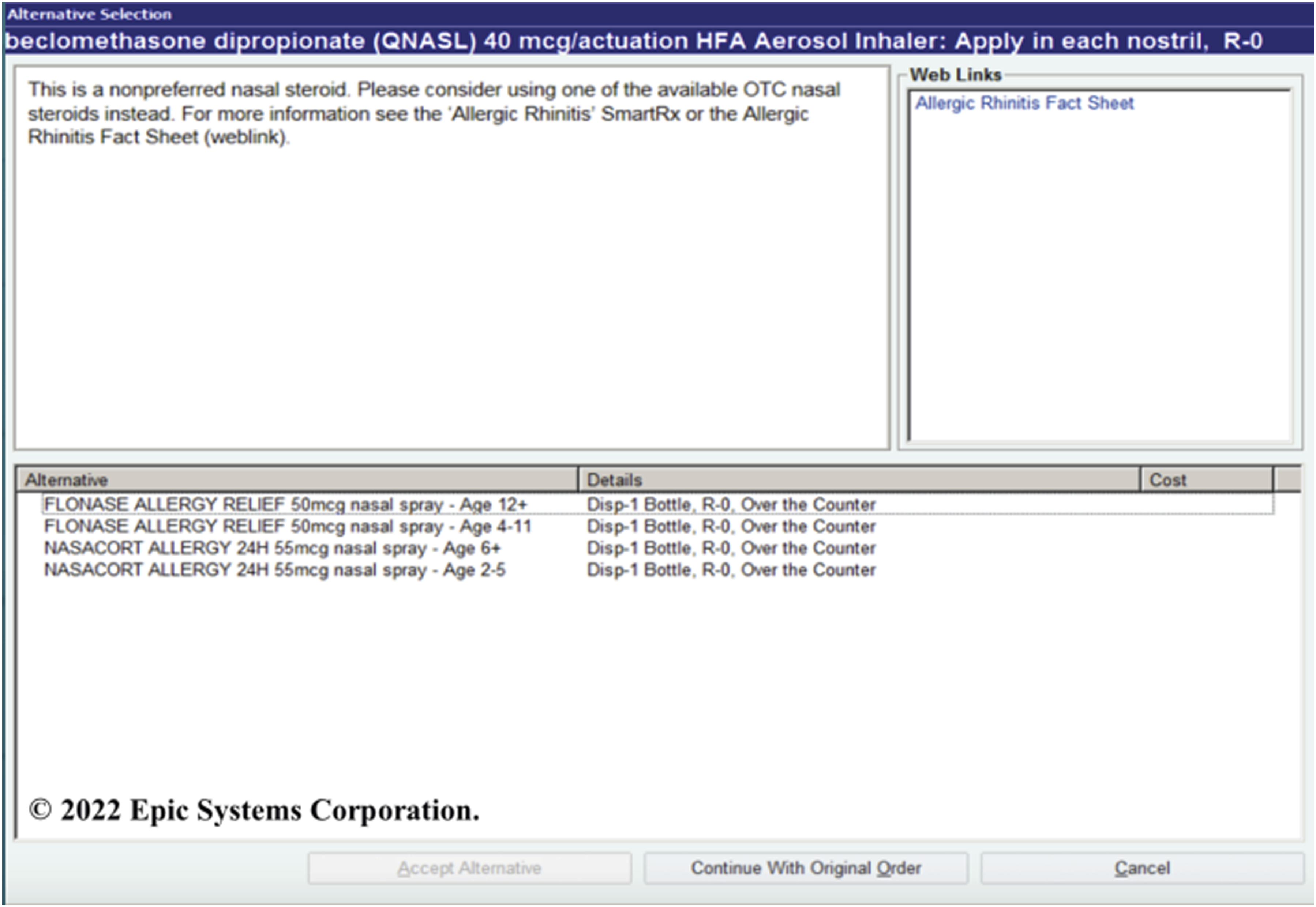
Figure 2 represents the point-of-prescribing alerts after the alerts were modified. Modifications included a bolded title to highlight that the recommendation was coming from the Atrius Pharmacy & Therapeutics Committee; a main message highlighted in red; approximate cost difference between the ordered medication and the suggested alternative; and a brief explanation or clinical pearls on how to switch to the alternative medication. Alert after modification.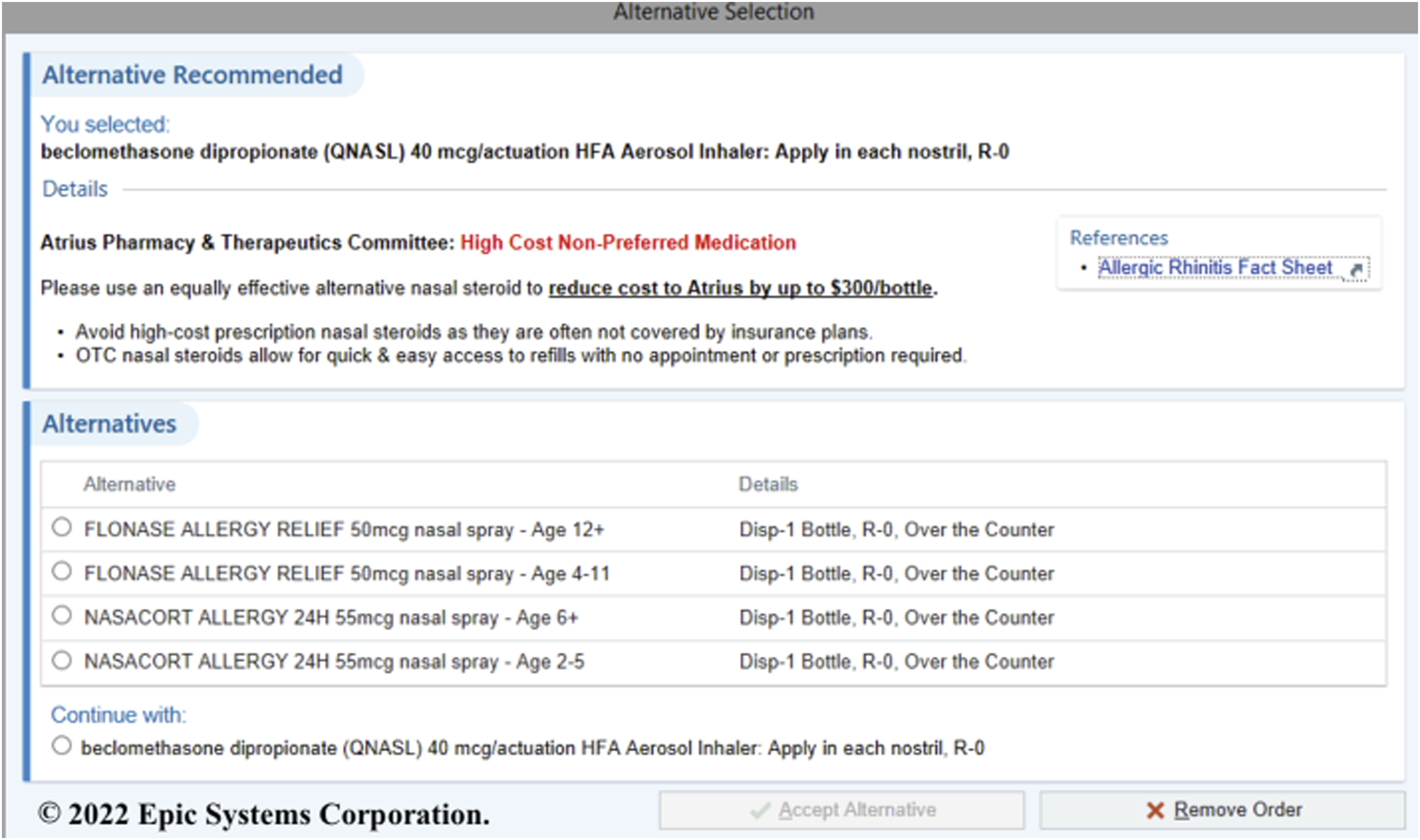
In a study titled “Impact of color on marketing,” researchers found that 62–90% of initial decisions made about products or ideas can be based on color alone. 9 Therefore, the bolded title and red were utilized in order to help capture the attention of the clinician.
Each alert provided the approximate cost differences between the ordered medication and the suggested alternative to allow clinicians to see the estimated cost-savings associated with the medication switch. The estimated cost difference was calculated based on the wholesale acquisition cost. Wholesale acquisition costs were obtained from the Atrius Health drug wholesaler (McKesson Corp, San Francisco, CA) in October 2019. For medications that provided acute treatment or that were utilized for a short course of therapy, the cost was determined using the average cost per therapy. The information regarding cost differences allows clinicians to see the potential cost-savings for the organization.
Last, brief explanations or clinical pearls were developed and incorporated into each alert to provide clinicians with information at a quick glance on why the switch is recommended and how to prescribe the alternative medication. This information was either bulleted or included in table format for ease of use. For example, when switching from a high cost, branded ICS/LABA inhaler to a generic fluticasone propionate/salmeterol inhaler, the alert provided a conversion chart with the most accurate dose equivalents.
Sample Size Determination
There were 101 medication point-of-prescribing alerts evaluated. A total of 17 informative alerts were excluded because they provided no alternative medication. The remaining 84 alerts were then organized into four groups based on cost and clinical significance: high value, high clinical significance; high value, low clinical significance; low value, high clinical significance; and low value, low clinical significance. (Figure 3). All high value alerts (51 alerts) were modified. Low value alerts (33 alerts total) were assessed for retirement in an effort to reduce alert fatigue. Alerts were retired if they had low clinical significance and low acceptance rates during the pre-modification period (Quarter 1, 2019). As a result, 12 alerts were retired, and 21 alerts were left unchanged because they were determined to have high clinical significance or high acceptance rates even though the value was low. High vs low clinical significance and cost.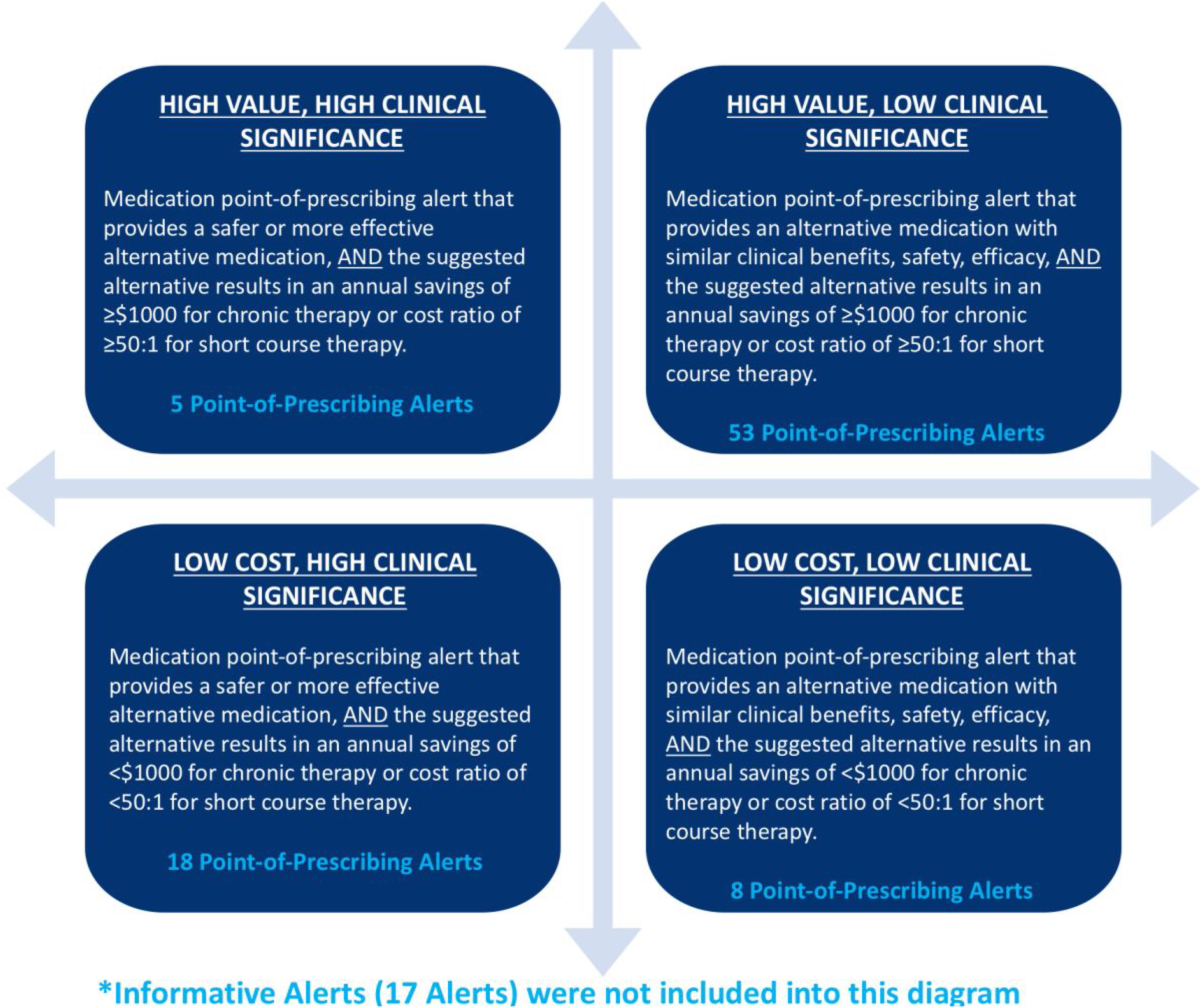
Statistical Analysis
Statistical analyses were conducted using NCSS (Number Cruncher Statistical System) 2007 and Microsoft® Excel®. During Quarter 1, 2019, there were a total of 101 point-of-prescribing alerts assessed by the clinical pharmacy informatics team at Atrius Health. Approximately 3.2% of these homegrown alerts were accepted at the point-of-prescribing. After our optimization process was implemented, we expected this acceptance rate to increase to at least 5% during the first quarter of 2020. Therefore, in order to detect an increase of approximately 1.8% at the 5% level of significance with 80% power, we would need to change at least 50 of the existing medication point-of-prescribing alerts. All expected and ideal percentages were determined together by the statistician and clinical pharmacy team.
Results
Change in the acceptance rates of modified point-of-prescribing alerts in Quarter 1.
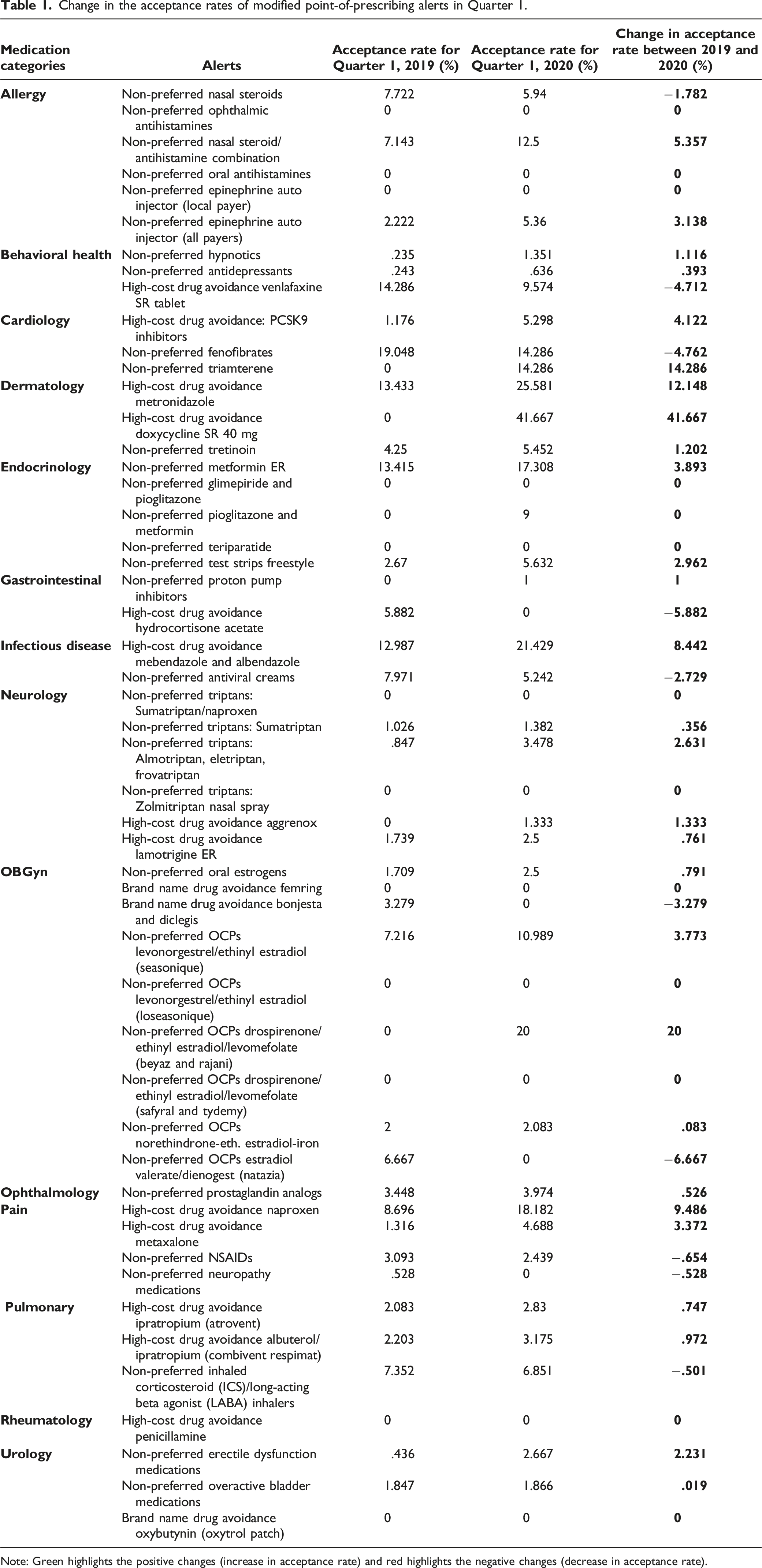
Note: Green highlights the positive changes (increase in acceptance rate) and red highlights the negative changes (decrease in acceptance rate).
Figure 4 summarizes the actions taken by clinicians with each point-of-prescribing alert; whether each alert was accepted, canceled, or continued, and the total number of alerts for Quarter 1, 2019 and Quarter 1, 2020. Based on the acceptance rate, there was an increase of 5.5% in the acceptance rate of point-of-prescribing alerts in Quarter 1, 2020, as compared to 3.2% in Quarter 1, 2019 (P <.001).10,11 Actions taken for each point-of-prescribing alert (Quarter 1, 2019 [left]; Quarter 1, 2020 [right]).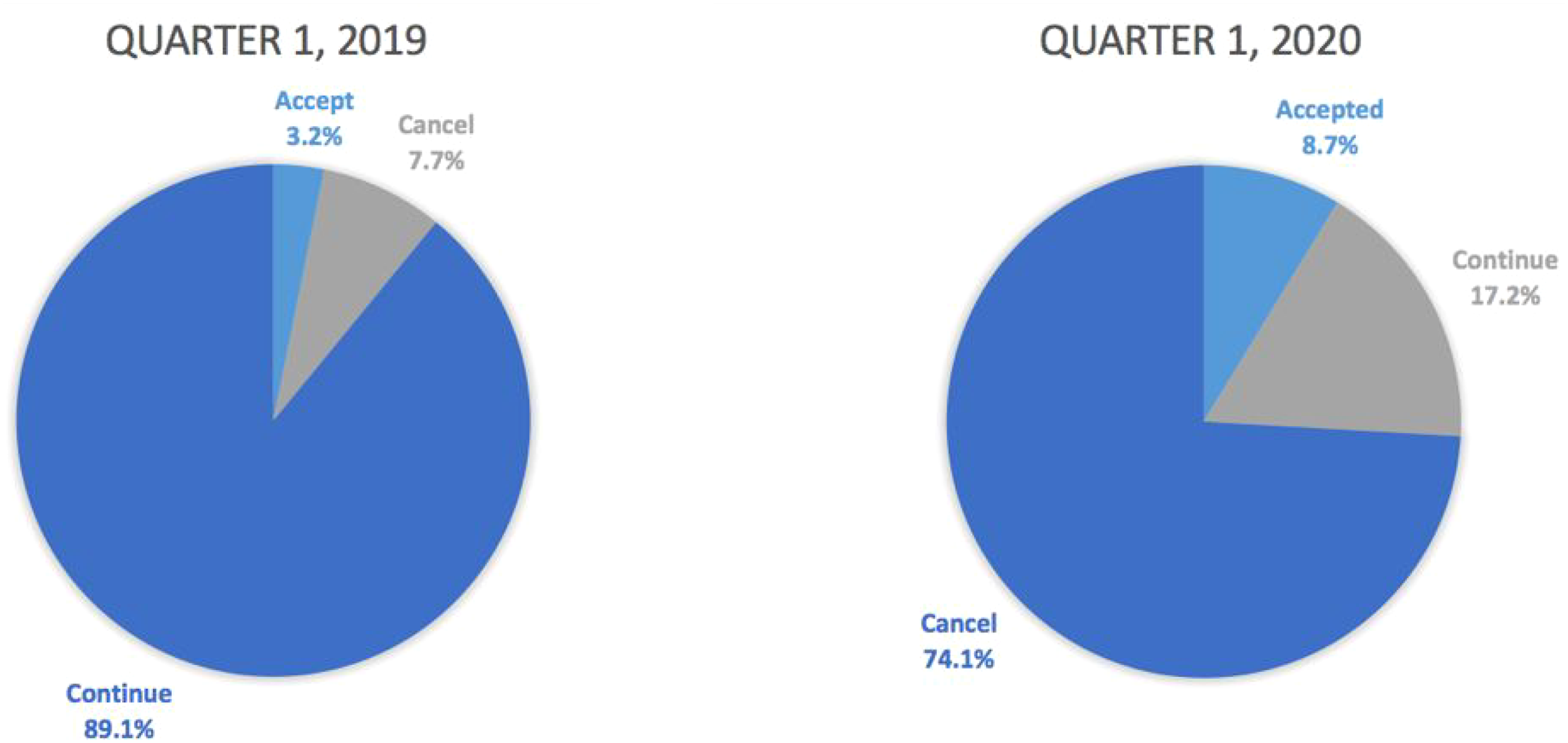
The acceptance of the point-of-prescribing alerts prompted orders for less costly alternative medications, which translates into an estimated annual cost-savings of $2.05 million to Atrius Health in 2020. The prescription cost-savings projection reflects savings for Atrius Health; it does not take into account savings for individual patients (i.e., copays). Despite an increase in the acceptance rate in Quarter 1, 2020, the cost-savings, when compared to the estimated annual cost-savings of $2.08 million in Quarter 1, 2019, is slightly lower.
Discussion
This study aimed to use retrospective and prospective data regarding the acceptance rates of a subset of point-of-prescribing alerts in order to enhance acceptance rates and provide health system cost-savings.
Regarding the point-of-prescribing acceptance rate, there was a slight increase in the acceptance rate after alerts were optimized. Our results demonstrated that point-of-prescribing alerts that provide a clear reason for an alternative medication, key points/clinical pearls, and cost transparency can increase the acceptance rate at the point-of-prescribing in a real-world healthcare delivery setting.
Although the acceptance rate was higher for Quarter 1, 2020, the estimated cost-savings was lower when compared to Quarter 1, 2019. The estimated cost-savings may have been lower in Quarter 1, 2020 due to a lower percentage of high value alerts being accepted in comparison to Quarter 1, 2019. However, the fluctuating medication prices likely explain this finding as well. Medication prices may vary based on drug availability, which can be impacted by drug shortages in production and distribution, market forces, and/or recalls that limit the availability of drugs. The acceptance rate of lower cost alternative medications may fluctuate as well based on what clinicians are prescribing. Thus, when comparing each quarter or year, the cost-savings value may fluctuate based on what is being prescribed.
Results from this study may help outline what to expect with the use of homegrown point-of-prescribing alerts, and the importance of optimizing information and providing specific cost comparisons in an ambulatory care setting. With new generic alternatives or alternative drug formulations becoming available on the market, there will likely be many opportunities for healthcare organizations to pursue similar analysis. Although the number of alerts and data for this study is relatively small, it may help to highlight that an increase in clinicians’ awareness increases the likelihood of accepting a point-of-prescribing alert. This study also shows cost-savings when switching to an equally safe and effective low-cost alternative.
Limitations
There were several limitations with this study. First, there were no methods to determine whether a point-of-prescribing alert was accepted as a new prescription order, as opposed to an alert being accepted for a refilled prescription order. A clinician may be more likely to accept the alert recommendation as a new prescription because it would be a new therapy for the patient. However, if a patient is already using an existing medication, the clinician may be reluctant to accept the alternative medication. As a result, they may cancel the alert recommendation or continue with their original medication choice. Additionally, during Quarter 1, 2020, the organization underwent an upgrade to the EMR that caused the point-of-prescribing alerts to appear slightly different. This altered appearance may have caused clinicians to accept alerts more often because they assumed it was new functionality.
Drug shortages and insurance coverage changes may cause clinicians to disregard medication alerts. For example, during Quarter 1, 2020, there was a shortage in fluticasone propionate/salmeterol inhalation powder; therefore, clinicians may have stopped accepting the alert.
Finally, the short time frame and small subset of point-of-prescribing alerts of this study may limit generalizability. In the future, whether for research or operational purposes, by extending the time frame of this study and including a broad spectrum of medications, it would allow healthcare organizations to identify trends in the alert acceptance rates. It may also be beneficial to have access to real-time pharmacy benefit technology. These advancements can help monitor the frequent changes in costs, and benefit design. Thus, it would be beneficial to follow up with clinicians and determine why they did not accept the alternative and to further understand their prescribing behaviors. Furthermore, Atrius Health and other healthcare organizations can utilize this data to implement future changes or help in the creation of new point-of-prescribing alerts in the EMR.
Conclusion
The use of homegrown point-of-prescribing alerts with optimized clinical information and specific cost comparisons in an ambulatory setting led to an increase in acceptance rates of point-of-prescribing alerts and more cost-effective prescribing. However, further research and development is needed to predict which alerts will be most effective.
Footnotes
Authors’ Note
American Society of Health-System Pharmacists (ASHP): Midyear Clinical Meeting, Las Vegas, NV, December 11, 2019.
Acknowledgments
Robert Belsher, Epic® Systems Analyst at Atrius Health for developing the database to track recommendations, Luis Carpio, MBA, Data Analyst III at Atrius Health for retrieving data, and Gary Tataronis, MS, Associate Professor of Statistics and Mathematics at MCPHS University for employing statistical methods.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.