
Abstract
End stage renal disease (ESRD) patients on renal replacement therapy (RRT) have an increased risk of morbidity and mortality due to healthcare associated infections (HCAIs). The aim of this study is to determine the prevalence, microbial etiology, and risk factors associated with HCAIs among ESRD patients on RRT. A multicenter, retrospective study was conducted from June to December 2019. ESRD patients with minimum of 6 months on RRT were included, while pregnant patients and patients <18 years were excluded. To reduce the risk of selection bias, all patients were randomly selected using a simple random sampling technique. The prevalence showing the proportion of patients that acquired HCAI since the initiation of dialysis until 2019 was calculated using the European patients’ academy (EUPATI) formula. Risk factors were assessed using univariate and multivariate regression analysis. The prevalence of HCAI among ESRD patients was 174/400 (43.5%). Catheter related bloodstream infection (CRBSI) was the most common infection [64(36.8%)], followed by peritonitis [45(25.8%)] and pneumonia [37(21.2%)]. Out of 382 total pathogens identified, 204 (53.4%) were Gram positive and 162 (42.4%) were Gram negative. Both methicillin sensitive staphylococcus aureus (MSSA) and methicillin resistant staphylococcus aureus (MRSA) showed statistically significant associations (p<0.05) with CRBSI. Use of multiple accesses, increased blood sugar levels, low serum sodium levels and higher CRP concentration increased the occurrence of HCAIs. The burden of HCAIs among the patients undergoing RRT is high. Preventive strategies and optimum empirical therapy of antibiotics should be used to reduce the risk of these infections among ESRD patients.
Keywords
Introduction
In recent years, end stage renal disease (ESRD) has emerged as one of the leading causes of morbidity and mortality throughout the world. 1 According to an estimate, the global prevalence of ESRD as well as the use of renal replacement therapy (RRT) will double by 2030.1,2 Additionally, the number of ESRD patients in some Asian countries, including Malaysia and Philippines is increasing by 10% every year. 3 A study has shown that ESRD patients undergoing RRT can easily develop severe complications such as bleeding, fluid loss, hypovolemia, and increased susceptibility to infection. 4
Infection has now become one of the major causes of mortality in ESRD patients, accounting for up to 20% of total deaths in these patients. 5 These patients are more susceptible to healthcare associated infections (HCAIs), due to the increased number of hospital visits and frequent interaction with other healthcare settings. 6 Several factors, such as chronic uremia, various comorbid conditions, anemia due to renal failure and malnutrition, potentially predispose these patients to infections by contributing directly to an immunocompromised state. 5 Furthermore, these patients have an additional risk of bloodstream infections as many of them need dialysis catheter as vascular access especially at the initiation stage of dialysis, which carry a high risk of microbial colonization. 7 According to the United States renal data system, almost 20% of all patients on RRT have at least one episode of bacteremia. 8 The pathogens associated with HCAIs varied among different studies in the past,9,10 and antimicrobial-resistant pathogens, particularly vancomycin resistant enterococci (VRE) were found to be prevalent among patients on RRT. 11
HCAIs contribute directly to substantial increase in the number of deaths, decreased health related quality of life (HRQoL) and extra economic burden. Only sparse information exists on the burden of HCAIs among ESRD patients on RRT, due to poorly developed surveillance systems and inexistent control methods. Moreover, various aspects of these infections, such as clinical epidemiology and microbial etiology, have not been extensively elucidated. Hence, to develop effective prevention strategies and treatment guidelines, these infections need to be thoroughly investigated in this high-risk patient population. The present study was performed to determine the prevalence, microbial etiology and risk factors associated with HCAIs among ESRD patients on RRT.
Methodology
Study Setting and Study Design
A multicenter, cross sectional, retrospective study was conducted at two study sites in Malaysia, including University Malaya Medical Centre, and Serdang Hospital. UMMC is a tertiary hospital, located in Kuala Lumpur, Malaysia. The UMMC services over 900 inpatients and approximately 1500 outpatients daily. The dialysis unit offers hemodialysis and peritoneal dialysis service. On average, 80 to 90 patients undergo hemodialysis in this hospital. Hospital Serdang is a tertiary hospital situated in the Sepang District in Selangor. It has 100 hemodialysis patients and more than 300 patients on peritoneal dialysis (PD). Both hospitals are government funded.
Patient Population
ESRD patients who were receiving outpatient dialysis services for a minimum period of 6 months were included, while patients who were pregnant, <18 years and those who have undergone kidney transplantation were excluded. Data of patients who were diagnosed with ESRD (defined as those classified with the international classification of diseases (ICD)-10-CM code N18.6 for ESRD) from 2015 to 2019 were extracted from the hospital’s medical records computerized system. All patients were then screened to see if they fit the study’s inclusion/exclusion criteria. The medical records and laboratory data were reviewed using the hospital’s total hospital information system (THIS) to confirm the diagnosis of any HCAI. All data were collected from the time of initiation of dialysis for each patient until 2019. A data collection form was used to retrieve patient demographics and clinical information.
The sample size required for determining prevalence was 400 case records (with 80% power and 95% confidence interval. To reduce the risk of selection bias, a simple random sampling technique—a research randomizer 12 was used. Research randomizer utilizes the total number of patients and the sample size to generate random numbers. Each number was noted, and the patient associated with that number on the list was selected.
Definitions/HCAI criteria For the purpose of this study, the modified definition from Friedman et al. (2002) was adopted as the initial definition of HCAIs,
13
where. HCAI is defined as “an infection present at the time of hospital admission or within 48 hours of admission, resulting from medical care or treatment in a hospital, primary healthcare setting, nursing home, or patient’s home.” An infection was said to be healthcare associated, if the patient had fulfilled any of the following criteria,
13
including (1)received any intravenous therapy, wound care or specialized nursing care at home or through a healthcare agency or had self-administered intravenous therapy in 30 days before the infection, (2)had a hospital visit or received intravenous chemotherapy in the previous 30 days, or (3)was hospitalized in an acute care hospital for 2 or more days in the previous 90 days.
Prevalence of HCAI Infections
The prevalence of HCAIs among the ESRD cohort was calculated as a percentage using a criterion discussed by Spronk et al. (2019), which showed the proportion of patients that acquired HCAI since the initiation of dialysis until 2019. 14 For this purpose, the formulas mentioned by European patients’ academy (EUPATI) were used, with numerator and denominator representing total number of cases of HCAIs and sample size, respectively. Note that only the first infection was identified and used to calculate prevalence and lab values associated with the first infection in any patient were drawn and used in analysis.
Risk Factors Assessment
The demographics and clinical characteristics of ESRD patients with and without HCAIs were recoded into variables. Risk factors were assessed using regression analysis (univariate and multivariate) with recoded patient characteristics against HCAIs.
Statistical Analysis
Data were coded into nominal, ordinal and continuous variables using the Statistical Package for Social Sciences version 20.0 (SPSS Inc., Chicago, IL). Normality was assessed using the Kolmogorov–Smirnov test. Both descriptive and inferential statistics were applied to achieve the objective of this study. A descriptive analysis of patients’ data was conducted to examine the variables of interest. Categorical variables were presented as absolute frequencies and percentages, while continuous variables were represented as median and interquartile range as normality could not be assumed. Primary outcome was the presence of HCAI among the patients. All associations involving categorical variables were assessed using chi square and Fisher’s exact test. The significantly associated variables were preselected to be assessed using regression analysis. As the dependent variable was of categorical type, binary logistic regression was used to analyze the relationship between independent variables and dependent variable; HCAI. Both univariate and multivariate logistic regression were used to identify independent risk factors associated with HCAIs. A P-value of <.05 was considered to be statistically significant.
Results
Patient Demographic
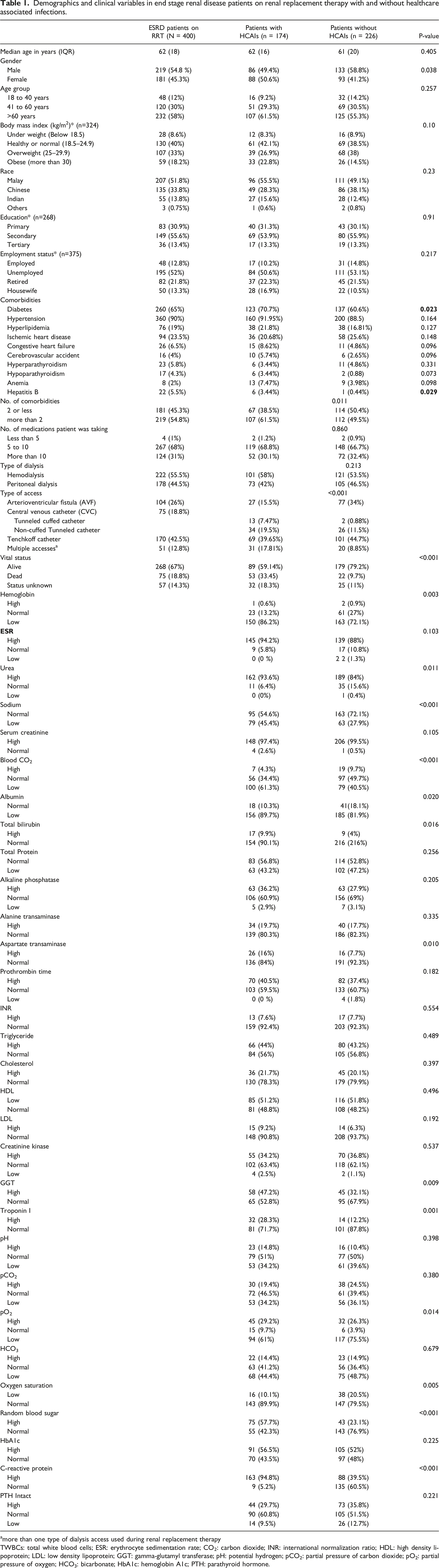
A total of 670 records were retrieved, and 400 patients were included in this study based on the inclusion criteria (Figure 1). Clinical and sociodemographic variables, such as gender, diabetes, hepatitis B, number of comorbidities, type of access, patient’s vital status, hemoglobin levels, C-reactive protein (CRP) concentration and blood sodium and magnesium levels were found to be statistically significant in patients with and without HCAIs. The demographic characteristics of participants are shown in Table 1. Identification and selection process of end stage renal disease patients on renal replacement therapy Demographics and clinical variables in end stage renal disease patients on renal replacement therapy with and without healthcare associated infections. amore than one type of dialysis access used during renal replacement therapy TWBCs: total white blood cells; ESR: erythrocyte sedimentation rate; CO2: carbon dioxide; INR: international normalization ratio; HDL: high density lipoprotein; LDL: low density lipoprotein; GGT: gamma-glutamyl transferase; pH: potential hydrogen; pCO2: partial pressure of carbon dioxide; pO2: partial pressure of oxygen; HCO3: bicarbonate; HbA1c: hemoglobin A1c; PTH: parathyroid hormone.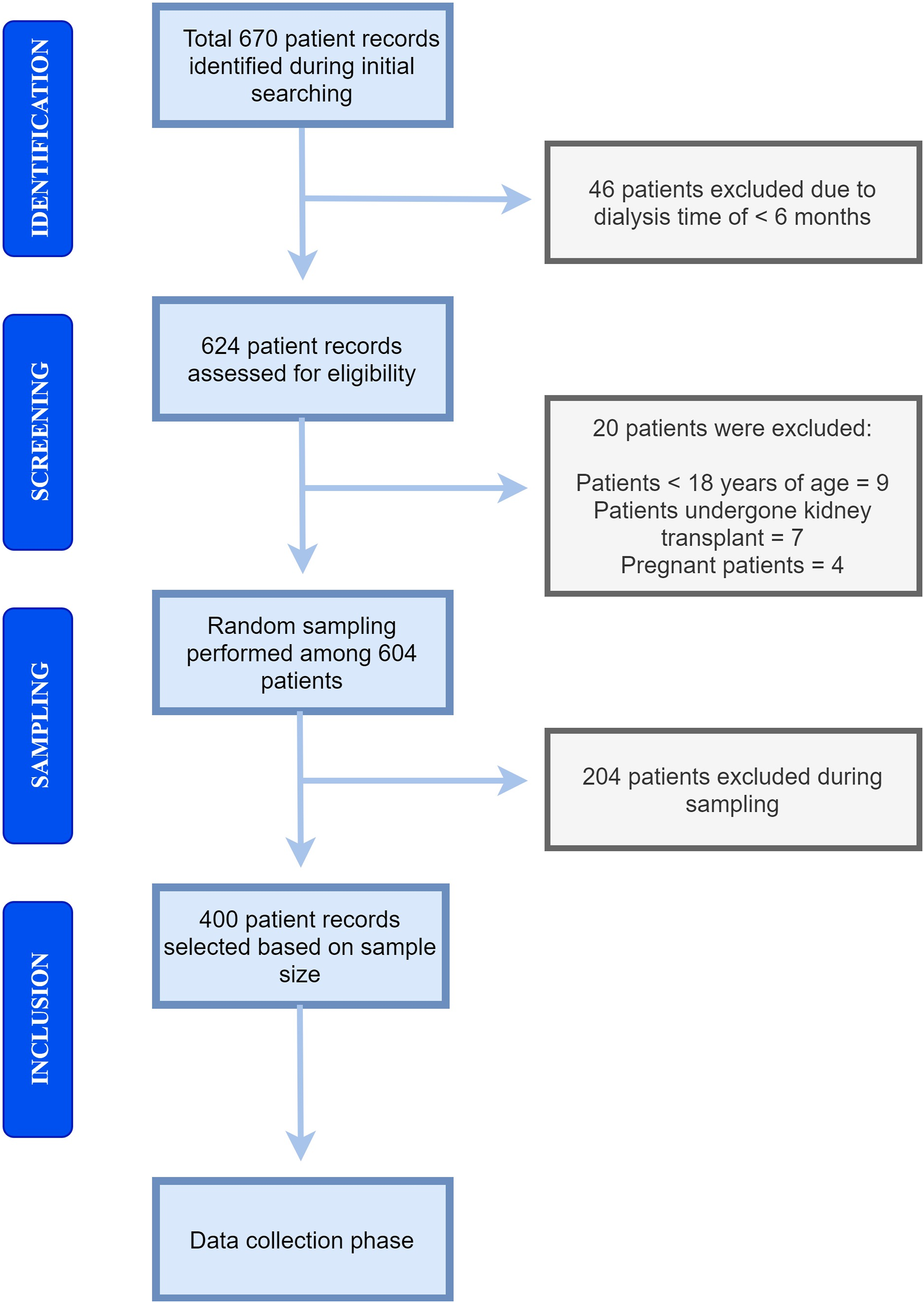
Prevalence
The prevalence of patients with at least one episode of HCAI was 174 (43.5%). However, there were a total number of 194 episodes, as there were some patients with more than one episode of HCAIs. Catheter related bloodstream infection (CRBSI) was the most common infection [64 (36.8%)], followed by peritonitis [45 (25.8%)] and pneumonia [37 (21.2%)]. The other common infections were bacteremia [23 (13.2%)], exit site infection [19 (10.9%)] and UTI [6 (3.4%)]. The different types of HCAIs are depicted in Figure 2. The prevalence of different types of healthcare associated infections *Catheter related bloodstream infection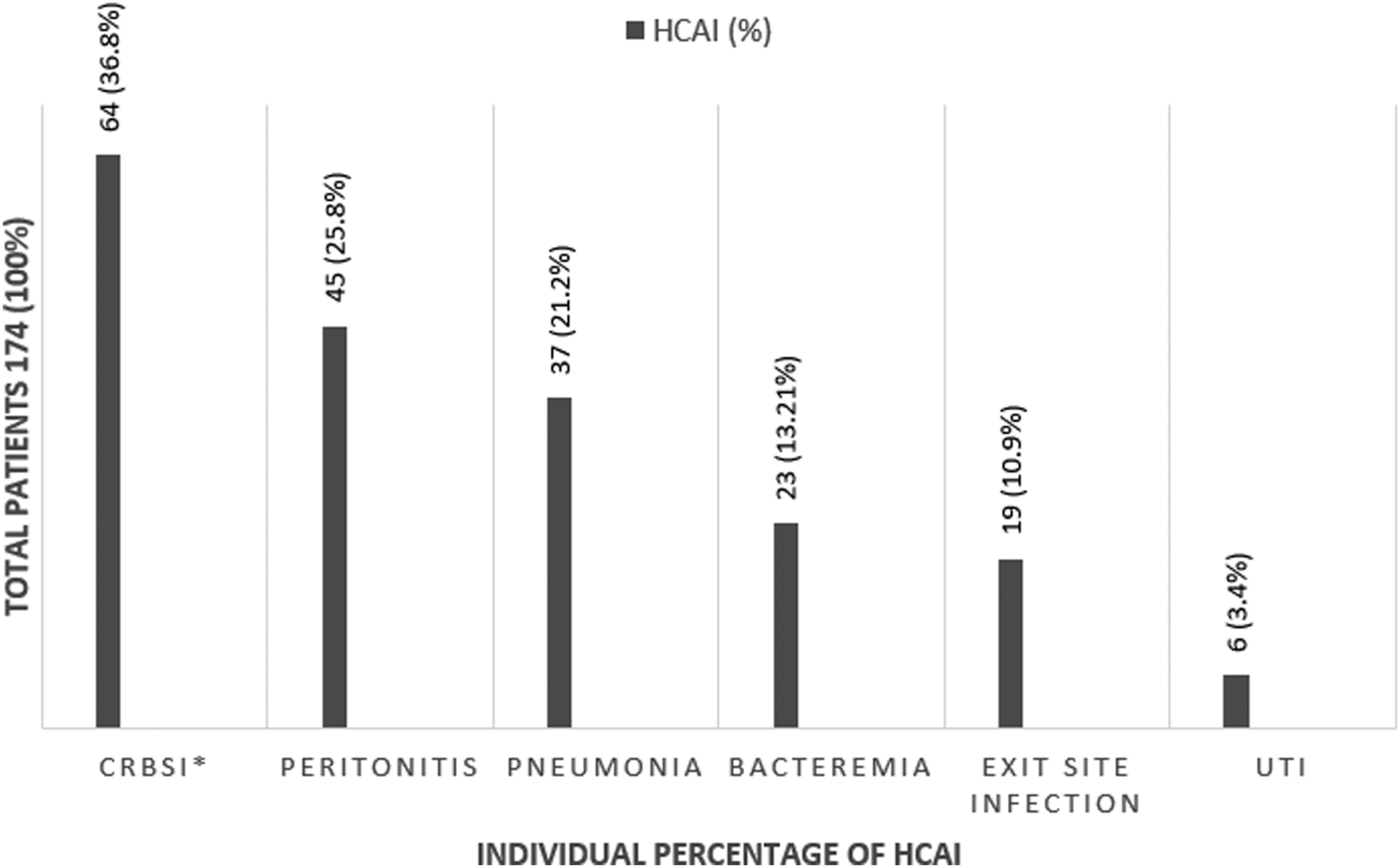
Microbial Etiology
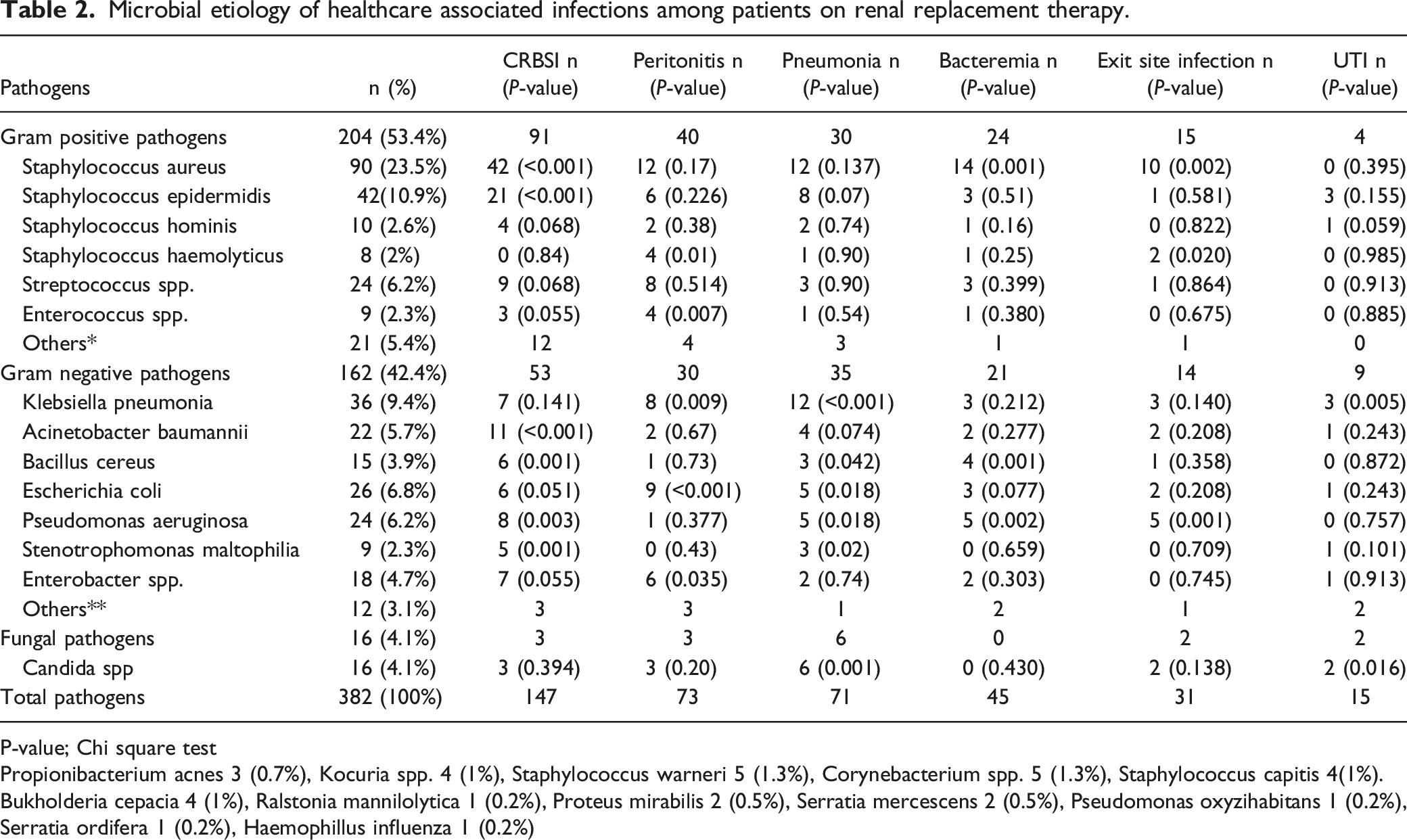
Microbial etiology of healthcare associated infections among patients on renal replacement therapy.
P-value; Chi square test
Propionibacterium acnes 3 (0.7%), Kocuria spp. 4 (1%), Staphylococcus warneri 5 (1.3%), Corynebacterium spp. 5 (1.3%), Staphylococcus capitis 4(1%).
Bukholderia cepacia 4 (1%), Ralstonia mannilolytica 1 (0.2%), Proteus mirabilis 2 (0.5%), Serratia mercescens 2 (0.5%), Pseudomonas oxyzihabitans 1 (0.2%), Serratia ordifera 1 (0.2%), Haemophillus influenza 1 (0.2%)
Seventy (78%) out of 90 coagulase negative S. aureus were sensitive to cloxacillin (also known as methicillin sensitive S. aureus or MSSA), while the remaining 20(22%) were resistant to cloxacillin but sensitive to vancomycin (also known as methicillin resistant S. aureus or MRSA). Out of the 42 S. epidermidis species found, 17(40.4%) were sensitive to cloxacillin (MSSE), while the remaining 25(59.6%) were resistant to cloxacillin but sensitive to vancomycin (MRSE). Among the remaining Staphylococcus spp., methicillin resistant S. haemolyticus and S. hominis were most common. Among the 24 Streptococcus spp. identified in this study, Streptococcus agalactae [6(25%)] was most common, followed by Streptococcus mitis (4(16.6%)) and Streptoccoocus pyogenes 3(12.5%). Eight (88.8%) out of 9 Enterococcus spp. were found to be Enterococcus faecalis, while 3(60%) of the 5 Corynebacteium spp. were Corynebacterium amylocatum.
Among the 18 Enterobacter spp., Enterobacter cloacae (7(40%)) and Enterobacter aerogenes (7(40%)) were most frequently found. Pathogens, such as S. aureus, S. epidermidis, pseudomonas aeruginosa, Stenotrophomonas maltophilia, and Acinetobacter baumannii showed statistically significant associations (P = < .05) with CRBSI, while S. epidermidis, E. coli, Bacillus cereus, and Klebsiella pneumonia showed similar associations (P = < .05) with pneumonia (Table 2).
Risk Factors
Univariate and multivariate logistic regression analysis.
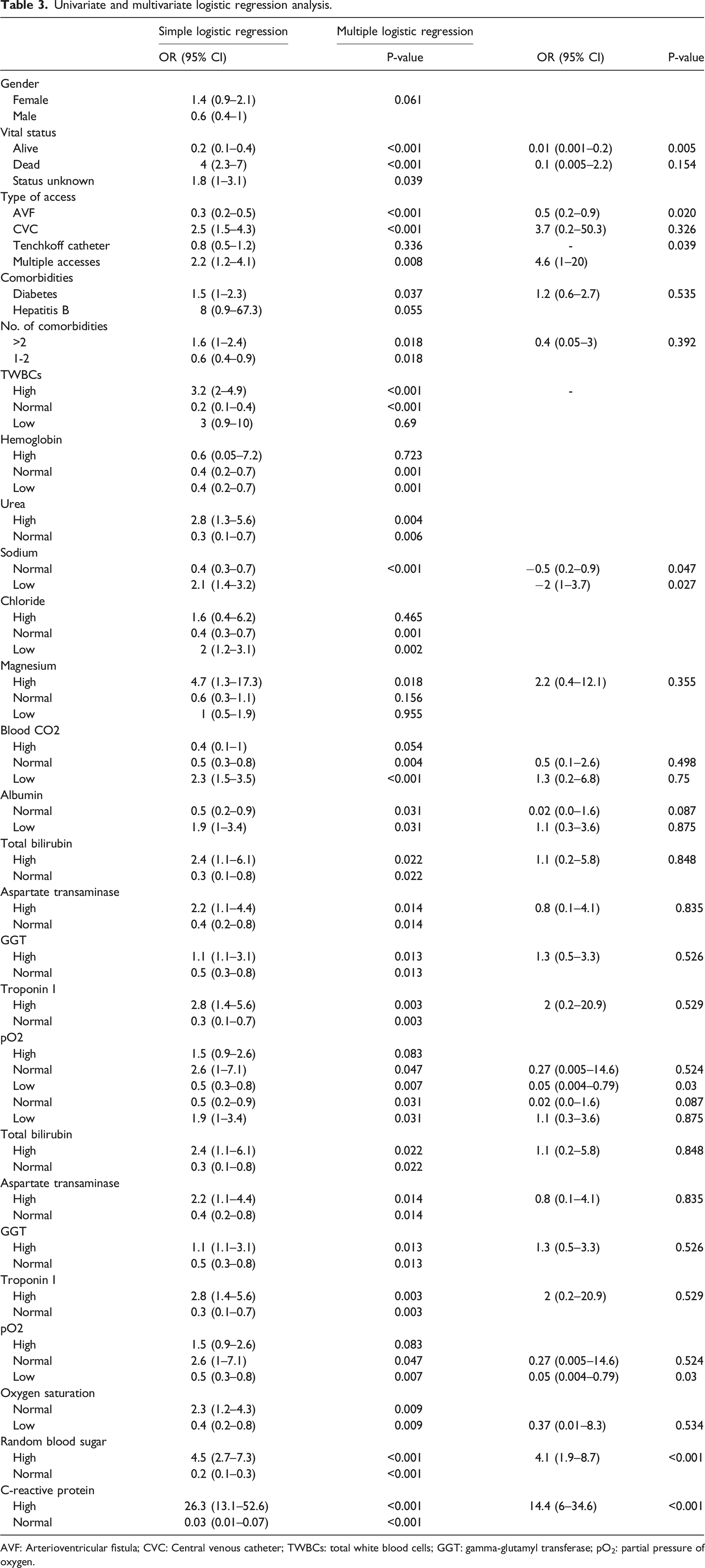
AVF: Arterioventricular fistula; CVC: Central venous catheter; TWBCs: total white blood cells; GGT: gamma-glutamyl transferase; pO2: partial pressure of oxygen.
Discussion
A high prevalence (43.5%) of HCAIs among patients on RRT was found in this study, which shows the burden of this complication on this high-risk population. Most of the studies in the past were conducted on individual infections, such as hemodialysis-associated bloodstream infection (HABSI), 9 hospital acquired pneumonia (HAP),10,15 and certain viral infections, 16 while no such study that estimated the prevalence of HCAIs in this patient population has been performed. A study conducted among hemodialysis patients showed the rate of nosocomial infections in these patients as 12.4%. 17 A comparatively higher prevalence of HCAIs in our study was due to their broader diagnostic criteria, as these infections can also be acquired at healthcare settings other than hospitals, which is not the case with nosocomial infections.
The use of central venous catheter (CVC) has been associated with increased risk of catheter related infections 18 and death from sepsis, 19 and studies from all over the world have reported high occurrence of CRBSI in patients on RRT.9,20 Infectious peritonitis; both bacterial and fungal, is a major complication in patients on peritoneal dialysis, which leads to technique failure, increased mortality 21 and longer hospitalizations. 22 Similarly, the frequent occurrence of healthcare associated pneumonia (HCAP) in this study is consistent with the results of several past studies.10,15 UTI was the least common infection found, which is not recognized as a major infection in patients on RRT because these patients have low urinary output, but few studies have shown otherwise.17,23
The patients whose vital status was identified as dead, had a strong and significant association with HCAIs, showing 4-folds increase in chances of having HCAI in these patients. Similar results were seen in many past studies suggesting higher mortality rates in patients with infectious complications during RRT.5,8,24 A study done in United States showed that 9.6% of all deaths in incident dialysis patients were caused by infections. 24 Similarly, according to latest report of Malaysian dialysis and transplant registry (MDTR), 28% of total deaths among dialysis patients were caused by sepsis. 25
In univariate logistic regression, the patients’ characteristics most strongly associated with HCAIs included, more number of comorbidities, having diabetes or high blood sugar levels, use of CVCs and multiple accesses, low albumin concentration (hypoalbuminemia), low serum sodium level (hyponatremia), low bilirubin levels (hypobillirubinemia), high CRP concentration. In multivariate logistic regression, use of multiple accesses, hyponatremia and increased blood sugar levels (hyperglycemia) were found to be independent risk factors for HCAIs, while high CRP level was identified as an independent predictor. CRP levels are increased in infections as well as many other types of inflammations. 26
High blood sugar level or hyperglycemia increased the chances of HCAIs by 4.5-folds. Both cellular and humoral immunity mechanisms are altered in hyperglycemic environment, leading to favorable environment for pathogens. 27 Increased stress among patients undergoing RRT can produce hyperglycemia even in non-diabetes population, which should be carefully monitored and treated. 27 Moreover, presence of coexisting diseases, such as diabetes was found as a predisposing factor in this study, subsequently increasing the risk of acquiring HCAIs by 1.6-folds. This result is congruent with the results of studies that showed increased risk of infection in diabetes patients receiving RRT,9,18,23,28 hence these patients have higher mortality rates due to infections than non-diabetes patients. Furthermore, good glycemic control even in diabetes patients has been associated with longer survival in ESRD as compared to poor glycemic control.29,30
Regarding the use of access, both CVCs and multiple accesses have shown a significant association with HCAIs; increasing the risk of these infections by 2.5-folds and 2.2-folds, respectively. It is well documented that more than any other type of access, use of CVCs is associated with higher rates of bloodstream infections (BSIs).31-33 In one study, Lemaire et al. (2009), reported that CVC use increase the risk of death from sepsis in patients undergoing hemodialysis, 19 while several other studies showed a significant increase in morbidity, mortality and cost of therapy due to CVC related infections.18,34,35 Moreover, according to studies in the past, patients with multiple catheter sites are more likely to acquire HCAIs than patients with single catheter site.17,36,37
Current study demonstrated that patients with low serum sodium (sNa) levels or hyponatremia had 2.1-folds increase in HCAIs. Waiker et al. also showed a constant connection between decreased sNa levels and hemodialysis mortality due to infections. 38 Another study reported a similar result where hyponatremic hemodialysis patients have shown increased infection-related hospitalizations and mortality. 39 Latest research suggested that high concentration of sNa promoted differentiation of CD4+ cells into T-helper 17 (Th17) cells, while its low concentration inhibited Th17 cells, hence decreasing a protective action against microorganisms.39,40
Two-folds increase in risk of HCAIs was seen in patients with low serum albumin concentration or hypoalbuminemia. According to Tang and Chen (2006), hypoalbuminemia is a sign of malnutrition in patients undergoing RRT, which leads to immune dysfunction and increases risk of infections. 17 Several other studies showed significant association between hypoalbuminemia and infections,41-45 and according to one study, hypoalbuminemia at initiation of peritoneal dialysis therapy is an independent predictor of infectious peritonitis. 45
Normal oxygen saturation and partial oxygen pressure (pO2) produced more than 2-folds increase in risk of HCAIs, while low oxygen saturation and pO2 subsequently decreased that risk. A recent study demonstrated that tissue hypoxia regulates several transcription factors that play a critical role in both innate and adaptive immunity, ultimately hindering both the occurrence and progression of bacterial infection. 46
Regarding the spectrum of pathogens, Gram positive organisms (53.4%) were more common than Gram negative organisms (42.4%). S. aureus was the most common Gram positive microorganism seen, most of which were MSSA (78%), while 22% were MRSA. MSSA being the part of normal flora makes patients on RRT more susceptible to staphylococcus infections, where vascular access plays a major role in entry of these organisms. 47 Therefore, according to national antibiotic guidelines (NAG) of Malaysia, i.v cloxacillin or cefazolin should be the drug of choice as an empiric treatment until microbial culture and sensitivity test is performed. Similarly, MRSA is associated with high mortality rates in RRT patients, and is a major nosocomial pathogen worldwide. 48 A study showed that use of CVCs is a major factor for infections with MRSA and its nosocomial colonization. 49 This is the reason that both MSSA and MRSA have shown significant associations (P-value = <0.05) with CRBSI in this study. Hence, vancomycin should always be considered for the empiric treatment in these patients with suspected vascular access related infections.
Both MSSE and MRSE were also commonly isolated among Gram positive organisms and showed significant associations (P-value = <0.05) with CRBSI and pneumonia. Most common Gram negative organisms, such as Klebsiella pneumonia and Acinetobacter baumanni demonstrated significant associations (P-value = <0.05) with pneumonia and CRBSI, respectively. A study done by Jae-Uk et al. (2017) showed similar results and identified S. aureus as the main pathogen in hemodialysis patients, followed by Klebsiella pneumonia. 10 Another study reported staphylococcus spp. and candida spp. as major organisms found in HCAIs among hemodialysis patients. 9 DAgata et al. (2000), reported candida species (spp) as the most common pathogens involved in infections among hemodialysis population, 23 which were the only fungal species found in the current study. Several past studies supported the observation that antimicrobial-resistant pathogens, particularly vancomycin resistant enterococci (VRE), are of major concern among patients receiving RRT, as these patients have increased number of infections and chances of vancomycin administration is 11-folds higher than patients without RRT. 50
Our study had few limitations. Although being a multicenter study, the data was collected from two hospitals only, which limits the generalizability of results. Sufficient number of patients was included in this study to reduce the effect of this limitation to a minimum level. Second, due to retrospective nature of the study, only the data available in the medical records were collected. However, patients’ record at the hospitals was completed with great care and organization. Additionally, microbial cultures and laboratory tests were performed using standardized protocols in these two hospitals, hence it is unlikely that any event of HCAI remained undiagnosed. Moreover, the authors did their best to make sure that the data collection phase was completed with great caution, and in case of any ambiguity, contacted staff and co-investigators from the hospitals immediately. The third limitation of this study is inherent to the search of patients. Patients were searched using ICD codes for ESRD, hence there is a chance of skipping any patient that fulfilled the criteria for inclusion but was diagnosed with different ICD code. However, random sampling technique employed in this study might overcome the problem of this sort.
Conclusion
The burden of HCAIs among the patients undergoing RRT is alarmingly high. Several potentially correctable factors, such as use of multiple accesses, hyperglycemia, and hyponatremia have been found as independent risk factors for these infections. Moreover, elevated CRP levels can be considered as an independent predictor for HCAIs in this high-risk patient population. Blood glucose and sodium levels should be frequently monitored in patients on RRT to strengthen the preventive measures against the risk of infections associated with these factors. Use of CVCs and multiple accesses should be avoided, and AVF should be used on priority basis for RRT. Empirical therapy with antibiotics against MSSA and MRSA should be used when there is risk of catheter related infection. Furthermore, microbiological profiles of these patients should be carefully monitored to help in choosing optimum empirical therapy. Efforts should be made to minimize the exposure of ESRD patients to hospitals and other healthcare settings to reduce the risk of HCAIs. A reduction in infectious complications in this patient population may decrease number of hospital admissions and economic burden, while improving patient’s health related quality of life (HRQoL) and more importantly reducing mortality. Future prospective studies and randomized control trials should provide a narrow focus on individual infections and their associated risk factors, which will further clarify the burden and effect of these contributing factors.
Footnotes
Acknowledgments
The authors would like to acknowledge the Centre for Higher Degrees by Research (CHDR) of Taylor’s University for providing fellowship for Mr. Saad Hanif Abbasi. The authors wish to pay gratitude to the staff members of University of Malaya Medical Centre and Serdang hospital as well as members of Clinical Research Committee (CRC) for providing their support in data retrieval phase.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the University Malaya Medical Research Ethics Committee (MREC ID NO: 2019320-7245) and the National Malaysian Research Registry (NMRR-19-777-47089) before the initiation of study.