
Abstract
Background
The prevalence of polypharmacy has significantly increased over the past decades due to a rise in the aging population with multimorbid conditions, which results in the use of multiple medications and complex disease-based care.1,2 Polypharmacy is defined as the chronic usage of five or more medications. Polypharmacy may result in a myriad of adverse drug reactions, reduction in physical and cognitive function, and increased health care costs.2,3 The burden of polypharmacy is becoming increasingly relevant for patients with chronic diseases, particularly those with type 2 diabetes (T2DM) and heart failure (HF).4,5 Patients with T2DM tend to receive intensive treatment for glycemia, blood pressure, and cholesterol to ensure optimal clinical outcome and to prevent disease sequelae. 5 Clinical guidelines emphasize the intensification of therapy especially in diabetics with cardiovascular risk factors. 5 Hence, the potential of overtreatment is common in this patient population. Similarly, patients diagnosed with HF with a reduced ejection fraction (HFrEF) are required to be on guideline-directed medical therapy (GDMT), which includes at the very least four medications. Currently, there are 8 different drug classes in the armamentarium of GDMT for HFrEF, many of which are recommended for concurrent use. 4 The benefit of GDMT can improve survival and left ventricular ejection fraction. 6 Further, chronic heart failure (CHF) patients are likely to be on multiple other medications for other comorbidities resulting in polypharmacy.
According to the Institute of Medicine Report, an estimated 1.5 million preventable drug-related injuries occur annually, resulting in an additional $3.5 billion cost spending. 7 This is largely due to mismanagement of complex medication regimens among older adults with cardiovascular disease. In a retrospective analysis evaluating the association of chronic disease states and polypharmacy, patients diagnosed with T2DM, CHF, end-stage renal disease, respiratory conditions, and hypertension demonstrated significant associations with medication-related problems. 8 Furthermore, the addition of a chronic medication resulted in a 10% increase in the odds of incurring a medication-related problem. 8
Deprescribing is the act of reducing or stopping medication that is no longer necessary or that may result to harm, which is relevant for patients with polypharmacy.2,3 Barriers to deprescribing include lack of time from physicians, lack of awareness in the potential medication harms, incomplete medical or medication history, reluctance to change the specialists’ medications, and fear of withdrawal symptoms or patient criticism. 9 In the D-Prescribe randomized clinical trial, the pharmacist-led intervention group was compared to usual care, resulting in a greater discontinuation of inappropriate medications. 9 Similar findings were noted in another study conducted by Ammerman et al., resulting in 121 (26.80%) potentially inappropriate medications (PIMs) —as identified in the 2015 American Geriatric Society (AGS) Beer’s Criteria list— being deprescribed by the interdisciplinary team, which included a clinical pharmacist specialist. 8 Studies evaluating deprescribing in various disease states are emerging; however, they commonly include either patients older than 65 years of age, patients with a higher comorbidity burden, or patients who are close to end of life. 2 Additionally, although these studies primarily focus on PIMs defined by the AGS Beer’s Criteria list, a consistent improvement in surrogate markers has not been demonstrated.1,2 This may be explained by the fact that a majority of the medications taken by older adults with multiple chronic diseases are chronic medications and not PIMs. 1
Further, patients are often overwhelmed with the burden of multiple chronic disease states, which frequently leads to suboptimal medication adherence. Unlu et al. found that the prevalence of polypharmacy in HF patients has increased, with the majority of medications prescribed being non-cardiovascular in nature, which makes the evaluation of this subset of medications critical. 4 Although deprescribing-related cardiovascular studies have demonstrated that deprescribing can improve medication adherence, prevent medication-related problems, and increase quality of life, these studies have offered limited insights regarding clinical outcomes. 2 To date, studies evaluating the pharmacists’ role in deprescribing and evaluating the impact on surrogate markers in patients with chronic disease states is limited.
Objectives
The primary objective of this research was to assess the impact of a pharmacist-led intervention as compared to usual care, regarding the deprescribing of inappropriate medication for patients with chronic disease states within a four-month study period. Secondary objectives included investigating the types of interventions, the number of PIM as those defined by 2019 AGS Beer’s Criteria list (for patients aged 65 and older), the differences in blood pressure and other surrogate markers between the pharmacist-led intervention group and usual care, as well as assessing predictors for deprescribing.
Methods
Study Design
This was a single-center, institutional review board approved, retrospective cohort study conducted at NYU Langone Health (NYULH), an 825-bed academic medical center. We extracted medical record data from NYULH’s electronic health record (EHR) between August 2019 and April 2021. The study followed the Reporting of Observational Studies in Epidemiology reporting guideline. For patients to be included in the intervention group, a NYULH provider had to refer them. In addition, these patients met the criteria of polypharmacy, needed management of chronic disease states, they were non adherent to medication regimens, they had poor health literacy, or they required medication titration for HF GDMT. Patients were included in the usual care group (control group) if they were managed by a NYULH provider without pharmacy intervention, and they met the criteria of polypharmacy or they required medication titration for HF GDMT. A PGY-2 ambulatory care pharmacy resident led the medication management clinic, and every intervention was supervised by an ambulatory care clinical pharmacist. For the selection of patients in the usual care group, we ensured that patients had not received any pharmacy intervention, and based on the pool of patients in the EHR, we randomly extracted data for patients who had visited the NYULH providers during the same period.
Patients’ demographics, comorbidities, laboratory data, number of medications prior to pharmacy visit, number of PIMs listed in the 2019 AGS Beer’s List (patients older than 65 years), details of pharmacotherapy (medications, doses, frequencies, and duration), and number of pharmacotherapeutic recommendations (medication adjustment, therapeutic duplication, drug-drug interaction, drug-disease interaction, wrong indication, medication omission, medication commission) were collected based on the retrospective review of EHR.
Intervention and Participants
Patients in the intervention group were seen by a clinical pharmacist in a pharmacist-led medication management clinic, in addition to usual care. Usual care was defined as interactive face-to-face with the physician or nurse practitioner without any pharmacy intervention. The pharmacy visit involved a comprehensive medication review, medication reconciliation, and educational sessions with the patient. The interactive face-to-face visit involved collecting patient-specific data, assessment of medication therapies to identify medication-related problems, prioritizing a list of medication-related problems, and creating a plan to resolve with the provider and the patient. Patients who were 65 years and older were also evaluated for any PIM listed in the 2019 AGS Beer’s list. Pharmacotherapeutic recommendations or discrepancies, such as medication adjustment, repeating laboratory values, therapeutic duplication, drug-drug interaction, drug-disease interaction, incorrect indication, medication omission, or medication commission were documented in the EHR and were communicated with the patients’ provider. Medications that were deemed inappropriate or no longer needed by the patient were communicated to the patients’ provider and were discontinued. Select patients were seen bi-weekly or tri-weekly for medication box fills. Educational materials such as a complete medication list with drug name, strength, frequency, indication, and counseling points were provided to patients at the end of each pharmacy visit. Patients in the control group received usual care without any pharmacy intervention.
Statistical Analysis
We initially analyzed our data by calculating descriptive statistics in the form of means, medians, and standard deviations for our continuous variables and in the form of frequencies and percentages for our categorical variables. We also performed paired samples t-test comparisons regarding several patients’ characteristics (eg, systolic blood pressure) measured before their visit to the pharmacy and again within a 4-month period following the pharmacist-led intervention. For the comparison of the patients’ ejection fraction before and after the pharmacist-led intervention, a 12-month comparison period was used. In addition, to achieve our primary endpoint, we conducted an independent sample t-test to compare differences in the number of deprescribed medications between the pharmacist-led patient group and the control patient group, which had not participated in the pharmacy intervention.
Furthermore, we performed correlations analyses between the difference in the number of medications within the 4-month period after the pharmacist-led intervention (ie, deprescribing) and the patients’ characteristics, which had been measured before their visit to the pharmacy. Lastly, we employed regression analyses to further assess the role of patients’ demographic characteristics in explaining the number of deprescribed medications as a result of the pharmacist-led intervention. We ran two regression models: the first one was based on data from 71 patients, whereas the second one was based on data from 68 patients because the ejection fraction percentages for three patients had not been measured. In the first regression model, the dependent variable was the difference in the number of medications after the pharmacist-led intervention (ie, deprescribing), and the independent variables were the patients’ characteristics: gender, age, systolic blood pressure, pulse, body mass index, creatinine clearance, and initial number of medications (before the pharmacist-led intervention). In the second regression model, we additionally included the independent variable: ejection fraction. In our regression analyses, we assessed the possibility of multicollinearity issues, taking into consideration the correlations among the independent variables that we included in our models. 10 The analysis of our data was performed using SPSS 26.
Sample Size
To proactively ensure the robustness of the study results, we carefully considered the power of our potential analysis. First, for the paired sample before and after t-tests in the group of patients enrolled in the pharmacist-led intervention, we conducted an a priori power analysis concerning the required sample size. For an effect size of .5 at the level of .80, and α equal to .05, we confirmed that the robust calculation of means differences for matched pairs required a sample size equal to 54. Second, for the independent samples t-test between the group of patients enrolled in the pharmacist-led intervention and those in the usual care group, we performed a priori power analysis of the required sample size. For a hypothesized effect size of .5 at the level of .80, and α equal to .05, we confirmed that the robust calculation of means differences for independent samples required 51 participants in each group. Thus, we set the goal of collecting data from 75 patients in each of the two groups, allowing for the possibility of up to 28% of participation attrition without observing a negative impact on the robustness of our findings. Our finally collected samples of a total of 142 patients met both requirements. We used G*Power version 3.1.9.7 to perform our analyses.
Results
Baseline Characteristics.
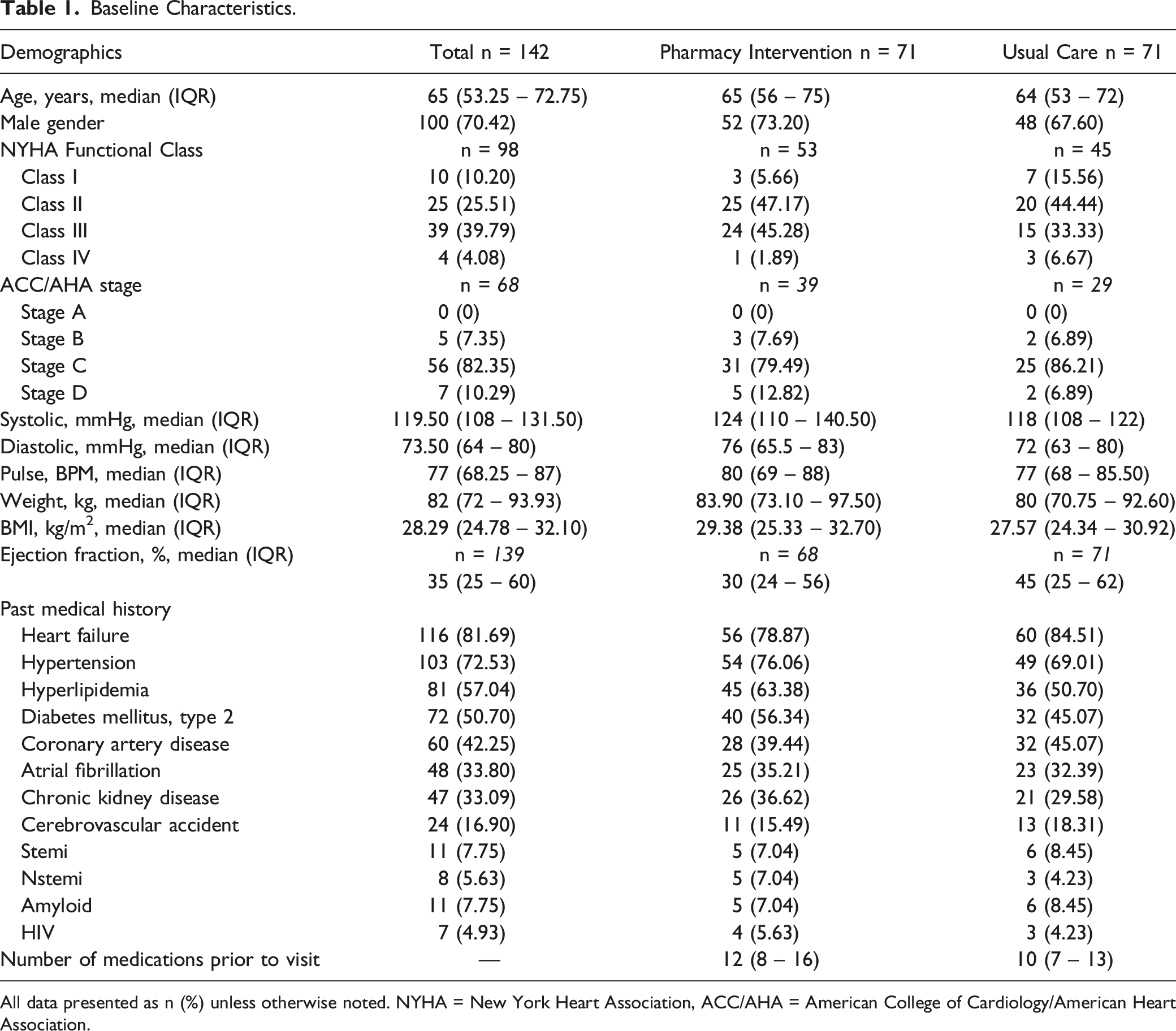
All data presented as n (%) unless otherwise noted. NYHA = New York Heart Association, ACC/AHA = American College of Cardiology/American Heart Association.
Secondary Endpoints.
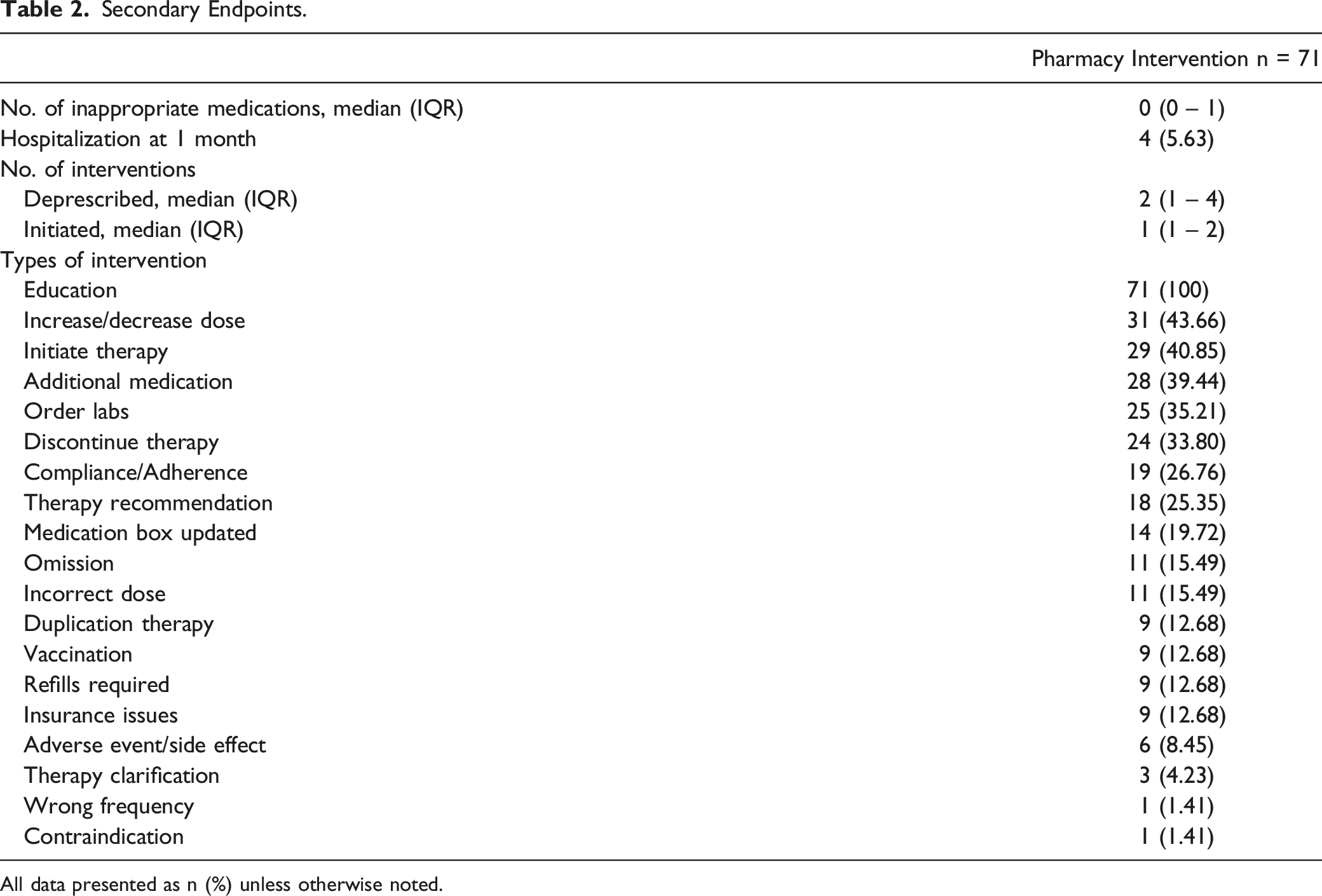
All data presented as n (%) unless otherwise noted.
Based on our results, among the 71 patients enrolled in the pharmacist-led intervention, an average of one medication was deprescribed (m = −1.00, sd = 2.57) during the four-month period. Among the patients included in the control group, an average of 0.44 medications (m = 0.44, sd = 3.32) were prescribed during the four-month period. The findings of the independent sample t-test for equality of mean scores in our balanced dataset indicated a statistically significant difference (t = −2.88, df = 140, mean difference = −1.44, standard error difference = 0.50, P = 0.005) between the 71 patients enrolled in the pharmacist-led intervention and the 71 patients of the control group regarding the number of medications deprescribed. Examples of deprescribing interventions included discontinuation of antihypertensives, such as amlodipine and amiloride in patients who achieved blood pressure control (BP < 130/80 mmHg) or experienced hypotensive episodes, discontinuation of inappropriate medications, such as ibuprofen in patients with a medical history of CHF, and discontinuation of clopidogrel after completion of dual antiplatelet therapy.
Summary of Mean Values, Standard Deviations of the Examined Variables and t tests for Equality of Mean Scores in the Pharmacist-led Intervention Group.
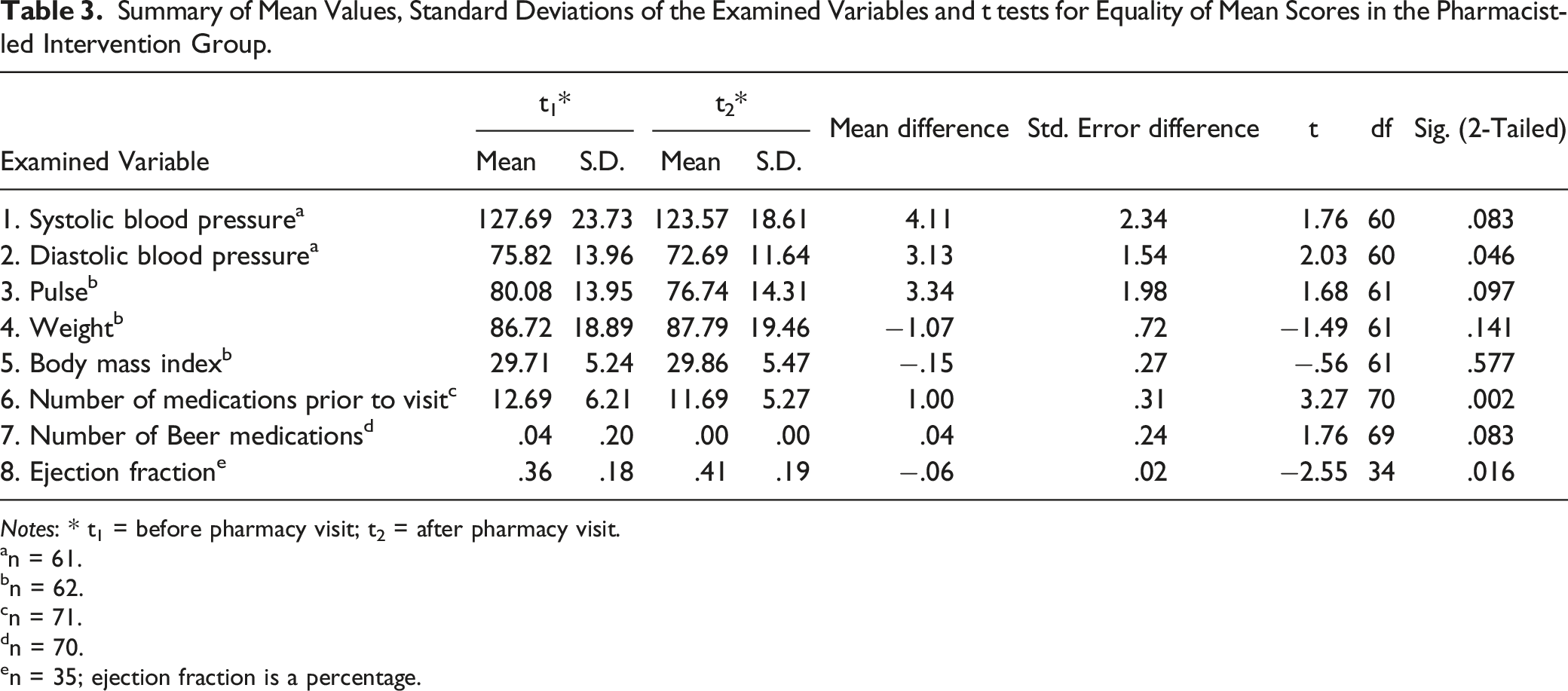
Notes: * t1 = before pharmacy visit; t2 = after pharmacy visit.
an = 61.
bn = 62.
cn = 71.
dn = 70.
en = 35; ejection fraction is a percentage.
In addition, we observed statistically significant differences (P = 0.046) in the levels of the patients’ diastolic blood pressure at t2 (m = 72.69, sd = 11.64) and at t1 (m = 75.82, sd = 13.96). Most importantly, the paired sample t test revealed a significant difference (P = 0.016) in ejection fraction of the patients at t2 (m = 41.46%, sd = 19.28%) compared to their ejection fraction at t1 (m = 35.60%, sd = 18.45%).
Descriptive Statistics and Correlations Matrix of the Examined Variables in the Pharmacist-led Intervention Group.
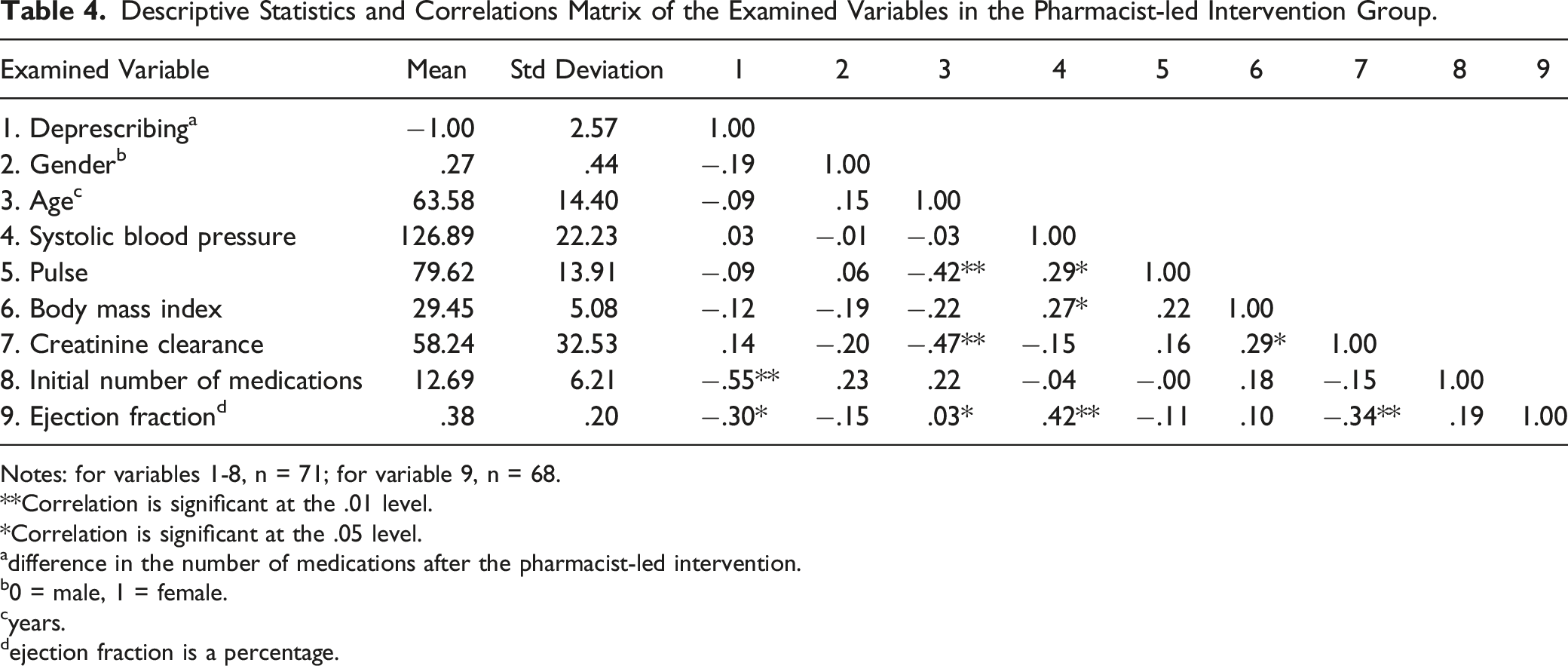
Notes: for variables 1-8, n = 71; for variable 9, n = 68.
**Correlation is significant at the .01 level.
*Correlation is significant at the .05 level.
adifference in the number of medications after the pharmacist-led intervention.
b0 = male, 1 = female.
cyears.
dejection fraction is a percentage.
Regression Analysis on Deprescribing in the Pharmacist-led Intervention Group.
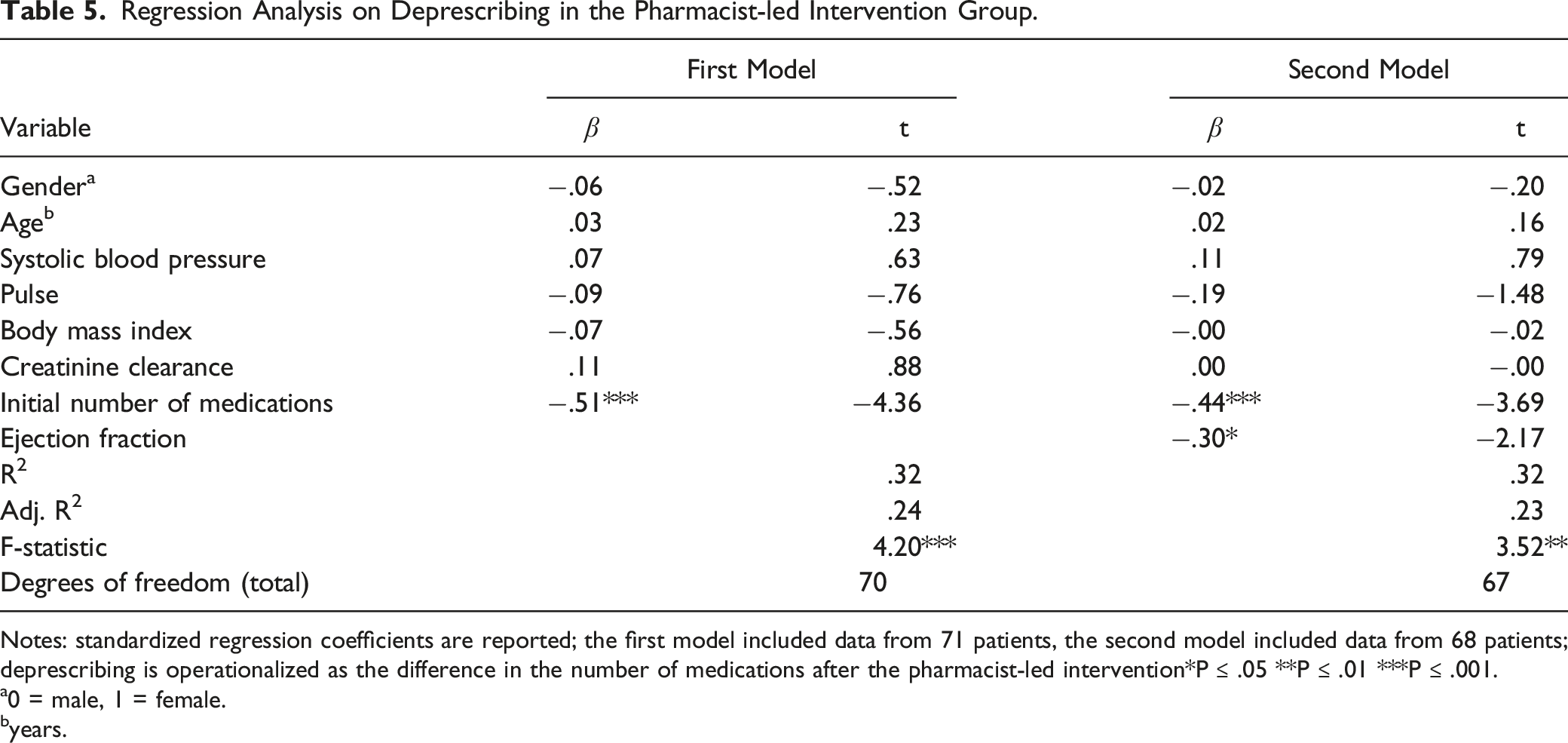
Notes: standardized regression coefficients are reported; the first model included data from 71 patients, the second model included data from 68 patients; deprescribing is operationalized as the difference in the number of medications after the pharmacist-led intervention
*P ≤ .05 **P ≤ .01 ***P ≤ .001.
a0 = male, 1 = female.
byears.
Based on the research results, we conclude that the larger the number of medications the patient initially takes, the higher the pharmacists’ influence on deprescribing. At the same time, the higher the ejection fraction, the higher the pharmacists’ impact on deprescribing. Alternately, patients taking more medications and with higher initial ejection fraction percentages were deprescribed a larger number of medications by the pharmacist.
Discussion
In this retrospective cohort review of a pharmacist-led intervention, there was an average of 1 inappropriate medication deprescribed compared to an average of 0.44 additional medications prescribed to patients who received usual care, within a 4-month period. This difference was statistically significant.
Our findings were comparable to other studies that evaluated the rates of deprescribing of inappropriate medications among older adults. Martin et al. compared the effectiveness of consumer-targeted, pharmacist-led educational intervention vs. usual care on discontinuation of inappropriate medications in a community setting. 9 Within the 6 months of the study’s duration, 43% of the patients (106 out of 248) in the intervention group no longer filled prescriptions for inappropriate medication, which was significantly higher than the 12% of patients (29 of 241) in the control group (risk difference, 31% [95% CI, 23% – 38%]). 9
Clark et al. implemented a pharmacist-provided medication review for patients who were over the age of 65 as part of their Medicare Annual Wellness Visit, with a focus on deprescribing PIM. 11 Their results demonstrated that among the 21 patients enrolled, 13 patients received a total of 20 deprescribing recommendations from the pharmacist. Whitman et al. conducted a pilot study to determine the feasibility of a pharmacist-led polypharmacy assessment in a geriatric oncology clinic. 12 Their results identified that, in a group of 26 patients, there were 73% PIMs when applying the Beers Criteria and the Medication Appropriateness Index. Two-thirds of patients reported a reduction in symptoms, such as decreased fatigue, no muscle aches, and dizziness after deprescribing medications. Ammerman et al. evaluated the effect of an interdisciplinary team, which included a clinical pharmacy specialist (GeriPACT), had on deprescribing in PIM. 13 Their results demonstrated that, among individuals aged 80 and older, there was a 26.80% decrease in PIM (nonsteroid anti-inflammatory drug (NSAID), anticholinergics, peripheral alpha-blockers, and proton pump inhibitors) deprescribed in the intervention group compared to only a 16.10% decrease observed in the usual care group.
Other studies, such as Allard et al., 14 examined the impact of an intervention team including a pharmacist reviewing patients’ medication for a number of inappropriate prescriptions and found that PIM decreased by a non-statistically significant mean of 0.24 per patient in the intervention group compared to a 0.15 in the control group. Hanlon et al. 15 evaluated the effect of clinical pharmacists’ interventions involving elderly patients with polypharmacy utilizing a medication appropriateness index (MAI). This index assessed whether there was an appropriate drug indication for clinically significant drug-drug and drug-disease interactions. Clinic-based pharmacist-led medication review of physician practices involved in-person outpatient education and resulted in a 24% reduction in MAI vs. a 6% reduction in the usual care group (P = 0.0006) within a 3-month period. Our results contribute to the reviewed literature that an interdisciplinary team, including a clinical pharmacist can effectively deprescribe inappropriate medications compared to usual care alone.
Real-world data on deprescribing for patients with polypharmacy and chronic diseases, such as T2DM and cardiovascular diseases, are limited. In patients with polypharmacy, non-cardiovascular medications are rapidly increasing compared to the number of HF-related or non-HF cardiovascular medications. 4 To our knowledge, there are limited studies evaluating the clinical outcomes of deprescribing in patients with cardiovascular diseases who are younger than 65 years old. Halliday et al. evaluated the safety of deprescribing HF medications in patients with recovered dilated cardiomyopathy (EF > 50%) with a median age of 54-56 years. It was concluded that 40% of the participants relapsed when their HF-related medications were discontinued. 16 Luymes et al. deprescribed anti-hypertensive medications and lipid-lowering agents in patients with a median age of 54-55 years and found that the predicted 10-year cardiovascular risk increased by 2% in the per-protocol group compared with 1.9% in the usual care group. 17
Beyond the aforementioned studies,4,9,11-17 our study measured various markers that demonstrated the positive impact of deprescribing on our patients. The pharmacist-led intervention group demonstrated a statistically significant improvement (P = 0.046) in patients' diastolic blood pressure at t2 (m = 72.69, sd = 11.64) compared to t1 (m = 75.82, sd = 13.96), despite a non-statistically significant improvement in systolic blood pressure. An analogous improvement (P = 0.016) was observed regarding ejection fractions before (m = 35.60%, sd = 18.45%) and after (m = 41.46%, sd = 19.28%) the intervention for patients with CHF. Interestingly, the pharmacist-led intervention group included a greater number of patients with NYHA Class III/IV and ACC/AHA Stage C/D compared to usual care. We optimized GDMT for HF based on a collaborative practice agreement and made recommendations to the patients' providers to further optimize pharmacotherapy for other chronic disease states. Pharmacists are well equipped to aid providers in managing chronic disease states, enhance drug therapy, and most importantly improve patient outcomes.15,18-21
Based on the regression results, deprescribing was beneficial for patients with larger numbers of medications, which implies that more emphasis regarding the pharmacists’ roles should be placed on patients with polypharmacy. Our findings corroborate the importance of including a clinical pharmacist as part of the health care team to address the gaps and barriers of deprescribing. Strategies that were utilized in our clinic to mitigate polypharmacy included a thorough medication reconciliation for each patient, review of each medication for an appropriate indication, counseling, education, and providing patients with pertinent educational material. Subsequently, medications that were flagged for deprescribing were discussed with the patients’ provider and with the patient, using shared decision-making with the goal of alleviating pill burden. Further, based on the regression results, deprescribing was higher for patients with a higher ejection fraction. A likely reason for that finding can be the nature of preserved HF, which does not require GDMT. The therapy for preserved ejection fraction involves controlling HF symptoms and comorbidities.
A strength of this study is the study population. To our knowledge, all the reviewed studies9,11-15 focused on the elderly populations, specifically patients older than 65 years, whereas our study included a larger range of patient ages (22 – 94 years), expanding generalizability and demonstrating that younger patients also benefit from deprescribing. In addition, although previously published literature9,11-15 addressed deprescribing PIM for elderly patients, it did not measure the effect that interventions may have on patients’ surrogate markers (blood pressure and ejection fraction). Our study demonstrated an improvement in patients’ diastolic blood pressure and ejection fraction in the pharmacist-led intervention group. These results are significant, especially because the pharmacist-led intervention group included patients with more severe conditions, with more complex medication regimens, and thus referred to the pharmacy clinic.
Our study presented several limitations including its retrospective nature and the possibility of weaknesses associated with incomplete documentation. Additionally, the examined time period of this study was four months. The intervention arm also had slightly more patients with T2DM, hypertension, and chronic kidney disease, who required frequent medication changes. Future research should focus on more longitudinal study designs, possibly including other health metrics, such as patient readmission rates, 20 survival rates, the Charlson comorbidity index, and economic indicators, such as cost-effectiveness and financial implications of deprescribing. Despite the mentioned limitations, our study highlights a real-world evaluation of deprescribing for a broader patient age group, allowing more robust conclusions regarding how pharmacist-led deprescribing intervention can alleviate pill burden, generating positive outcomes on ejection fractions and diastolic blood pressure.
Conclusion
Polypharmacy is frequently encountered in complex and chronic disease states. Therefore, deprescribing should be prioritized as a therapeutic intervention similar to initiating clinically appropriate medication, to ensure positive patient outcomes. In addition to medication optimization, polypharmacy must be addressed for all age groups of patients to ensure optimal clinical outcomes. The current research highlights the impact of a clinical pharmacist in the healthcare setting to deprescribe for a more comprehensive age range, including young and elderly patients, with chronic disease states. Clinical pharmacists are well-equipped to support healthcare providers to address the gaps, optimize pharmacotherapy and surrogate markers, and deprescribe medications deemed inappropriate.
Supplemental Material
Supplemental Material - Pharmacist-Led Deprescribing for Patients With Polypharmacy and Chronic Disease States: A Retrospective Cohort Study
Supplemental material for Pharmacist-Led Deprescribing for Patients With Polypharmacy and Chronic Disease States: A Retrospective Cohort Study by Mabel Chan, Roda Plakogiannis, Abraham Stefanidis, Mandy Chen, and Tajinderpal Saraon in Journal of Pharmacy Practice
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Note
This was a single-center, institutional review board approved, retrospective cohort study conducted at New York University Langone Health (NYULH), an 825-bed academic medical center.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.