
Abstract
This brief report describes the case of a 16-year-old girl who was commenced on sertraline for anxiety and depression, and subsequently developed severe and debilitating motor tics. Cessation of sertraline was associated with the resolution of tics; after this, paroxetine was trialled and well tolerated with good response of targeted symptoms and without re-emergence of tics. A narrative literature review yielded a retrospective observational study and eight single case reports on selective serotonin receptor inhibitor-induced motor tics (three in adolescents and five in adults). Tics are not commonly considered as a side-effect of SSRIs. This case report is novel is several aspects: the tics emergence was immediate whereas previous cases were delayed; the tics symptoms were measured and quantified by a validated scale; a dose-response relationship was observed; to our knowledge, our case was the first adolescent female reported; and finally, paroxetine was well-tolerated as a substitute, although it is unclear whether the observed tics-sparing effect is co-incidental, ideocratic or can be replicated.
Keywords
Case
Patient X is a16-year-old girl, diagnosed with mixed anxiety and depression by her general practitioner in March 2021 and was treated with fluoxetine 20 mg daily. While treated with fluoxetine, she reported an increase in suicidal ideation and self-harm behaviour. X was referred for inpatient admission treatment for worsening low mood, hopelessness, loss of interest, poor concentration, dissociation and suicidal ideation. After admission, her fluoxetine was tapered off and sertraline 25 mg was started with intended slow upward dose-titration.
On day three after being commenced on sertraline, she started experiencing motor tics. Initially, these comprised a subtle twitching of her jaw muscles and eyes. On day four, tics were more pronounced and extended to involve shoulder shrugs and head jerks. The movements characteristically worsened during distress, and were partially relieved on distraction. There were no reported past history or family history of tics or Tourette’s syndrome. She was not taking any other medications.
Although the treating team was aware of rare case reports of association between sertraline and tics, her tics were initially considered to be either co-incidental or psychogenic, given the reported rarity and lacking past or family history and that she did not develop tics while on fluoxetine. Sertraline was therefore increased to 50 mg on day five. The rationale was that her mood and anxiety were the key target clinical symptoms driving significant impairments; and tic-like behaviours could subside following reduction of depression and anxiety symptoms. Therefore, the treating team decided to increase her dose of sertraline.
However, after the dosage increase, motor tics worsened significantly. The tics started to occur almost hourly and involved multiple discrete tics plus several paroxysms of sequential complex tics that involved multiple muscle groups. Tics became marked in intensity, could not be suppressed by the patient and interfered with her verbal communication.
A Challenge-Dechallenge trial was conducted to evaluate causality. Sertraline was ceased on day five; thereafter a gradual reduction in the frequency, intensity and complexity of tics was observed. On day seven, the patient reported tics only occurring a few times throughout the day and localised to her face. These findings, as well as the response to increasing doses of sertraline are indicative of a temporal and dose-response association. Once motor tics ceased, paroxetine was substituted at 10 mg daily, and she did not experience any further motor tics. The patient remained well at a follow-up review 1 week after being discharged.
During the admission, the Yale Global Tic Severity Scale (YGTSS) 1 was used to measure the severity of tics, The total motor tic score was 22/25 and the overall impairment rating was 30 at the peak of tics on day five. After the initiation of paroxetine, the YGTSS motor tic score reduced to 0 with an overall impairment rating of 0. The treatment team obtained written consent from the patient and her parent for reporting this case.
Discussion
Selective serotonin reuptake inhibitors (SSRIs) are the most commonly prescribed antidepressants. They are effective in treating symptoms of moderate to severe depression, relatively safe and typically cause fewer side effects than other classes of antidepressants. The improved tolerability of the SSRIs is attributable to their selectivity. Serotonin receptors comprise at least seven classes, which are further divided at the receptor subtype level. These receptors mediate a variety of functions unrelated to mood, including sleep, pain perception, circadian rhythm regulation and gastrointestinal symptoms, as well as appetitive, sexual and cognitive functions. Some are heteroreceptors (i.e. 5HT2A, 5HT2c) expressed on GABA interneurons, dopaminergic and norepinephrinergic neurones; by these, serotonin can influence other neuromodulator systems. 2
The most frequently reported side effects of sertraline are dry mouth, headache, dizziness, nausea, diarrhoea, insomnia, somnolence, delayed ejaculation and fatigue. However, tics as an adverse reaction of SSRI is controversial and under-explored, as only several rare cases have been reported in literature. Worsening or emergence of tics with SSRIs treatment has been reviewed within the context of the known connections between dopaminergic and serotoninergic systems. 3 The potential pathophysiological mechanisms are unknown given the complexity of the connections between these 2 systems. Specific 5HT receptor subtypes, including 5-HT(1A), 5-HT(1B), 5-HT(2A), 5-HT(3) and 5-HT(4) receptors facilitate dopamine release; however, 5-HT (2C) agonism inhibits both tonic and evoked dopamine release in nigrostriatal and mesolimbic pathways. 4
Published Case Reports of Selective Serotonin Reuptake Inhibitor-Induced tics and Our Current Case.
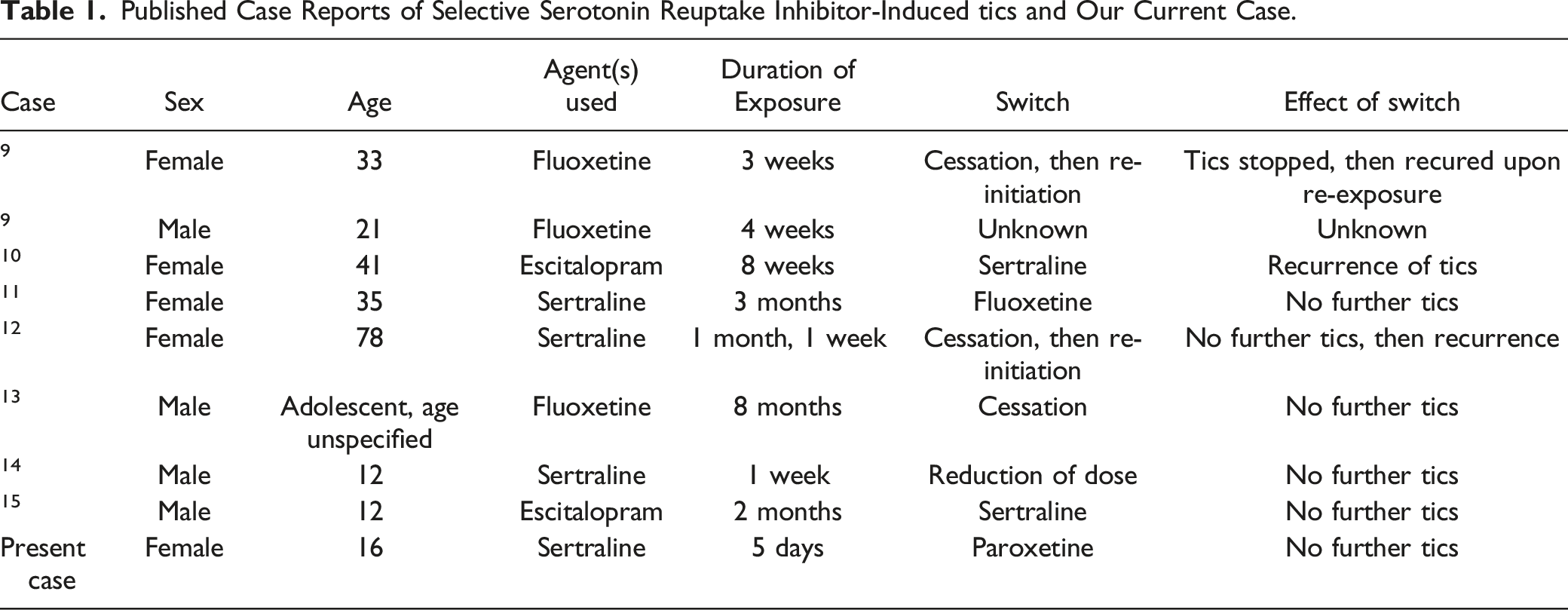
Ref. 13 first reported the case of a male adolescent with depression who experienced motor tics within eight months of commencing fluoxetine. These gradually subsided 6 months after cessation. Ref. 14 detail the case of a 12-year-old boy with obsessive compulsive disorder whose sertraline was increased from 100 mg to 125 mg. After a week at this higher dose, he experienced repetitive shoulder shrugging and blinking. Upon reduction of the dose back to 100 mg, these tics stopped. More recently, Ref. 15 described a 12-year-old boy who experienced involuntary eye twitching after 2 months of taking 20 mg escitalopram. These symptoms ceased after stopping his escitalopram. Sertraline 50 mg was introduced as a substitute and did not precipitate re-emergence of further tics. Overall, these single case reports described delayed emergence of motor tics after a prolonged period of exposure ranging 2 to 8 months and different SSRIs were involved. Sertraline appeared to induce tics in 1 case, but was well-tolerated in another.
There are also five case reports of tics among adult patients. Ref. 9 outline 2 cases. One was a 33-year-old woman who was commenced on 20 mg of daily fluoxetine, and experienced twitching of her left eye after 3 weeks and subjective paroxysms of hearing loss in her left ear. These symptoms initially resolved with cessation of the drug. Re-commencement of the drug again precipitated twitching and hearing loss. The other case was a 21-year-old man who was commenced on 20 mg of fluoxetine which was titrated upward to a dose of 40 mg daily. After four weeks of therapy, he started experiencing twitching of his left eye. The resolution of this case was not outlined in the report. Ref. 11 described a 35-year-old housewife who experienced rapid involuntary blinking of her right eye three months after commencing sertraline which stopped after cessation of this drug. Fluoxetine was then substituted, and she did not experience any further involuntary movements. Ref. 12 reported the case of a 78-year-old woman who started experiencing involuntary eyebrow, shoulder shrugging and gasping 1 month after being started on a daily dose of 50 mg of sertraline, prescribed for depression. These stopped after cessation, however she was recommenced on the same dose 1 year later, and she started experiencing the same symptoms after 1 week. Ref. 10 described the case of a 41-year-old woman who was prescribed escitalopram for panic disorder and started experiencing involuntary motor tics of her right eye and forehead after eight weeks. These stopped after cessation of escitalopram, but when sertraline was introduced 2 months later, she started to experience the same tics after 3 weeks of treatment. Again, these tics stopped after cessation of her sertraline.
Overall, all adult case reports described delayed emergence of motor tics after a prolonged exposure ranging from 1 month to 3 months. The short lag-time to reaction of sertraline after 3 weeks described by Ref. 10 could arise from sensitisation or potentiation by eight weeks of preceeding escitalopram exposure. Among these adults, again different SSRIs were involved; and sertraline was not tolerated as a substitute in 1 case.
Of the eight cases reviewed, there is wide variation in the duration of treatment, choice of SSRI and method of treatment in these cases. The immediate cessation and trial of alternative antidepressants has been shown to be effective in some cases, but has precipitated further tics in others. In the present case paroxetine was selected as a substitute as there is evidence it can reduce dissociative symptoms. 16
In 2020, a retrospective observational review was performed on cases of medication-induced tics reported to the French pharmacovigilance database and World Health Organisation pharmacovigilance database over the past few decades. This included both adolescent and adult patients. The drugs with the strongest association with tics were psychostimulants and mood stabilisers, and there were a small number of cases involving the antidepressants mirtazapine and venlafaxine. Sertraline was not identified as a major cause of tics and paroxetine was not evaluated for any tics-sparing property. 17
Our case report embodies novelties and differs from previous reports in several ways. First, the adverse reaction was immediate; second, the emergence of tics occurred at low subtherapeutic dosage of sertraline. Third, the tics symptoms were measured and quantified by a validated scale. Fourth, there appears a dose-response relationship showing more tics in intensity and kinds after dosage increase of sertraline. Fifth, our case was the first adolescent female reported in the literature. Sixth, paroxetine was tried and well-tolerated and it remains unknown whether the tic-sparing effect in this case is co-incidental, ideocratic or can be replicated.
As such, in our study, the consideration for causation rather than association could derived from three specific observations in line with Bradford Hill criteria 18 : (1) Temporality (the temporal association was immediate in our case, contrasting with delay effects previously reported); (2) Biological Gradient (the dose-response effect was observed); and (3) Experiment (the partial Challenge-DeChallenge experiment further confirmed likely causal relationship, but we considered it unethical to re-challenge this patient by re-introducing sertraline). One case by Ref. 9 demonstrated ‘Challenge-Dechallenge-Rechallenge’ relationship with fluoxetine ‘Exposed-Unexposed-Reexposed’ sequence. However, the criterion for Biological Plausibility remains unclear as inferred by known pharmacological mechanisms.
The mechanism by which SSRIs induce tics is not fully understood. The neural substrates for motor tics and Tourette’s syndrome have been postulated to involve the dopaminergic system, as inferred from the therapeutic effect of neuroleptics with dopamine antagonism property. Overall, the structures within the cortical–striatal–thalamo-cortical (CSTC) circuits have been implicated. These circuits involve the projections of cerebral cortex to striatum and other basal ganglion structures, with loops which feedback back to the cortex via the thalamus. The neural circuitries involved in tics have been reviewed elsewhere and include the direct pathway, indirect pathway and hyperdirect pathway within CSTC circuitry loops, which are influenced by neural modulators at the cortical, striatal and thalamic levels.19,20
Selective serotonin reuptake inhibitors are known to decrease norepinephrine and dopamine release via 5HT(2C) agonism. However, fluoxetine has specific 5HT(2C) antagonism property which could be posited as the pharmacological mechanism for elevating dopamine and norepinephrine. 2 However, citalopram, fluvoxamine, paroxetine and sertraline have been shown to lack such property in an animal study. 21 The role of dopamine excess and dysregulation in tics has been implicated by treatment effect of stimulants. Overall, our case and other eight reported cases suggest that 5HT(2C) antagonism may not be the mechanism by which tics were induced, because there is no consistent pattern regarding the tics-sparing effects of fluoxetine and other SSRIs. Notably, fluoxetine was well-tolerated in the case described by Ref. 11 and tics-sparing effect was noted in our case prior to admission, whereas sertraline and escitalopram both induced tics in our case and others. Ref. 3 reviewed SSRIs in relation to tics and Tourette’s syndrome with a review of three cases described in our narrative review, and also identified improvement of tic symptoms in 2 patients following initiation of sertraline and no change in another study of 14 patients when treated with fluoxetine.8,22 In summary, we cannot identify a plausible pharmacodynamic mechanism to meet the biological plausibility criterion in our consideration of Bradford Hill causality analysis. Additionally, there is no evidence to suggest that any specific first-line SSRI is associated with a reduced risk of tics. 23
Our findings provide very preliminary support for an association between SSRI exposure and motor tics. It remains unclear how common is the phenomenon of SSRI-induced tics, whether immediate or delayed. Side-effects of SSRIs are especially relevant to adolescents with depression and anxiety, as they are often commenced on antidepressants for the first time at this age. Compliance and positive engagement with health professionals are strongly affected by their response to medications. We therefore report this case and provide a narrative review of the literature to raise awareness and stimulate interest in this area.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.