
Abstract
Introduction
Pain is defined as an “unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage”. 1 Clinical practice guidelines state that intensive care unit (ICU) pain exists both at rest and during procedures in the ICU, and recommend routine monitoring and treatment of pain, with opioid analgesics serving as the mainstay of therapy.2,3 A number of studies have reported ICU-related acute pain as contributory to the development of chronic pain syndromes. 4 However, the incidence of chronic pain following ICU discharge is difficult to determine given there is no widely accepted definition and inconsistencies exist with etiology and associated risk factors. 5 Long-term consequences of chronic pain are likely not purely physical in nature, but may be associated with decreased quality of life, decreased psychosocial functioning, and the development of post-traumatic stress. 6 Critical care clinicians must balance appropriate management of pain in the ICU, while also limiting adverse effects and the potential for chronic opioid use disorders.
The association between acute hospitalization and post discharge opioid use has been described in medical and surgical populations, specifically opioid-naïve and Medicare populations.7-9 Unfortunately, many of these studies have not focused specifically on critically ill patients; therefore, application may be limited to opioid use on medical/surgical wards and its application to post hospital discharge. Retrospective studies examining opioid use after ICU stay are limited by a lack of data describing ICU patient management and actual opioid prescribing patterns.10-12 The primary objective of this study is to characterize opioid utilization intensity in the ICU and its association with opioid utilization across hospital care transitions and upon discharge.
Materials and Methods
This is a prospective cohort study which included consecutive patients admitted to the pulmonary critical care service between September 2019 to November 2019. Patients admitted to the medical intensive care unit (MICU) or the medical-surgical intensive care unit (MSICU), survived to hospital discharge, and who had a home medication history completed by a pharmacist were eligible for inclusion. Patients were only screened and included if admitted to the pulmonary critical care service. Medication histories are traditionally not completed by pharmacists on all patients in the health system, but rather those identified as high risk (>10 medications prior to admission, readmitted within 30 days, receiving oral anticoagulants, history of transplant, or with methadone on the home medication list) or identified to have a specific need by the pharmacist, nurse, or provider. Patients with no documented opioid use on the home medication history are referred to as “opioid naïve”. All patients were managed by a multidisciplinary team under the guiding principles of evidence-based medicine. The multidisciplinary team included ICU physicians, fellows, medical residents, nurses, clinical pharmacists, dieticians, respiratory therapists, and students. Physical therapists, occupational therapists, and case managers participate in multidisciplinary rounds twice weekly. This study was approved by the institutional review board for human research.
The study team consisted of clinical pharmacists and two students. All patient information was collected by the study team (CH, RAZ and 2 students) trained on definitions and guided by RedCap data collection forms to ensure data integrity. 13 All data was abstracted by review of the electronic medical record (EPIC Systems). If a patient was transferred to the ICU more than once during the hospital encounter, only data for the first admission to the MICU or MSICU was documented. Opioid intensity was characterized by converting all opioid doses to intravenous morphine milligram equivalents (IV MME). Primary outcomes were opioid administration upon ICU discharge to the floor and opioid prescribing upon hospital discharge. Opioid prescribing upon ICU discharge to the floor was defined as either a scheduled opioid order for >24 hours following ICU discharge or administration of ≥50% of an “as needed” opioid order for >24 hours following ICU discharge. Secondary outcomes included characterization of hospital and ICU length of stay (LOS), mechanical ventilation, level of sedation, and delirium.
To compare differences in opioid utilization and outcomes within the study population, opioid cohorts based on average daily ICU opioid use were established. These cohorts included patients who received ≥50 mean IV morphine milligram equivalents per ICU day (IV MME/ICU day), 1-49 mean IV MME/ICU day, and no opioids during ICU admission. Categorical data were analyzed using the Chi square and Fisher’s exact tests as appropriate. Continuous data were analyzed using the Kruskal-Wallis one-way analysis of variance test given the non-parametric nature of data, as determined by the Shapiro-Wilk test. Post hoc pairwise comparisons between groups were performed for statistically significant results using the Bonferroni correction for multiple comparisons. Univariate analysis was performed for potential factors associated with opioid prescribing upon hospital discharge (age, sex, illicit substance use, past psychiatric diagnosis, preadmission opioid use, ICU length of stay, hospital length of stay). IBM SPSS Statistics, version 25, was used to conduct data analysis.
Results
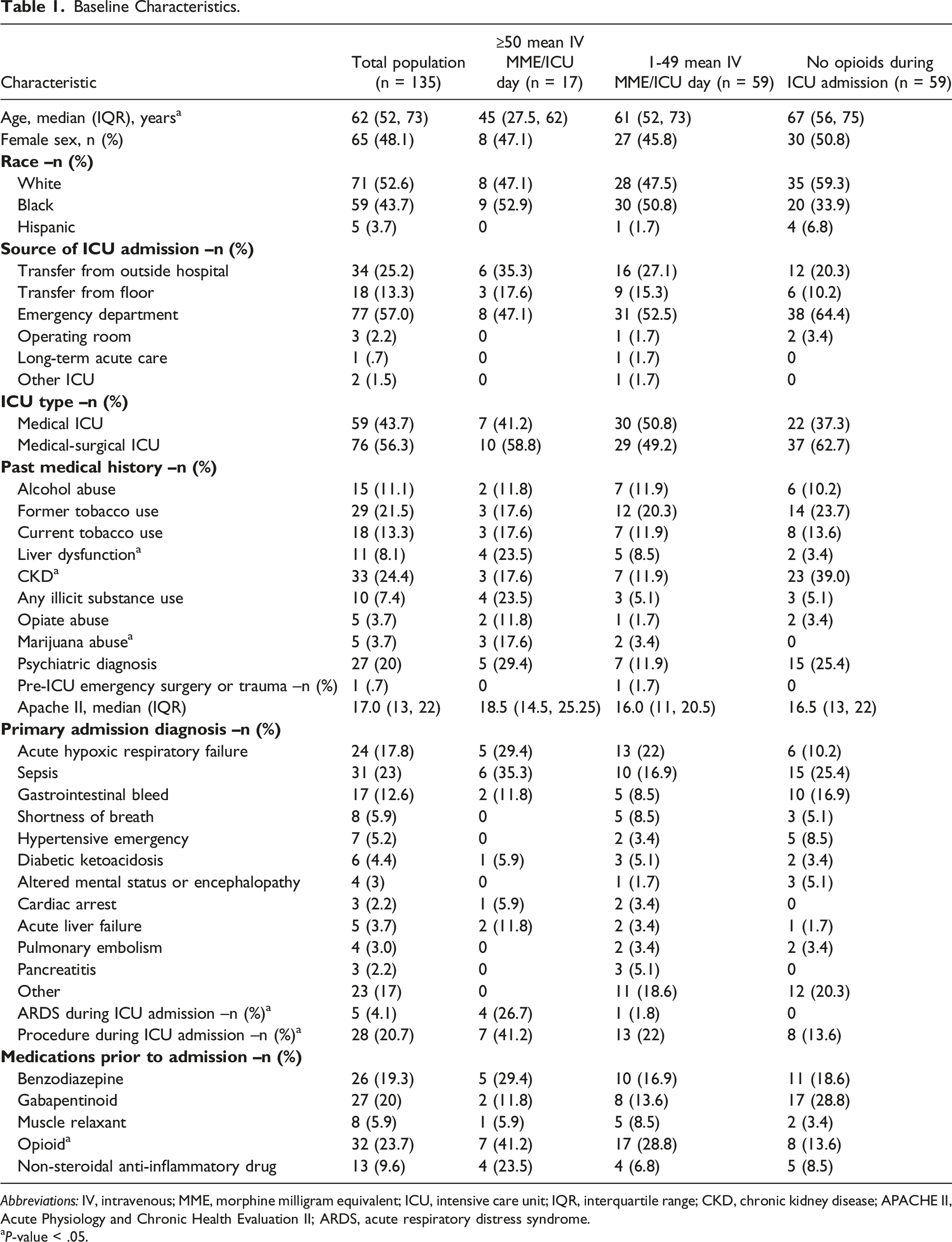
A total of 344 patients were screened during the study period. Of these, 21 patients and 188 patients were excluded due to in-hospital mortality and incomplete home medication history, respectively. The remaining 135 patients met inclusion criteria (Figure 1). Baseline characteristics of the study population are described in Table 1. There were statistically significant differences in age, liver dysfunction, chronic kidney disease, marijuana abuse, acute respiratory distress syndrome, procedures during ICU admission, and prior to admission opioid use among groups. The median APACHE II score for the total cohort was 17. Scores were not calculated when an arterial blood gas was unavailable. Of included patients, 23.7% were confirmed to be on an opioid prior to admission for the treatment of a comorbid pain syndrome. When patients were characterized based on mean IV MME/ICU day, 12.6% received ≥50 mean IV MME/ICU day, 43.7% received 1-49 mean IV MME/ICU day, and 43.7% received no opioids during ICU admission. Patient screening and inclusion. Baseline Characteristics. Abbreviations: IV, intravenous; MME, morphine milligram equivalent; ICU, intensive care unit; IQR, interquartile range; CKD, chronic kidney disease; APACHE II, Acute Physiology and Chronic Health Evaluation II; ARDS, acute respiratory distress syndrome. aP-value < .05.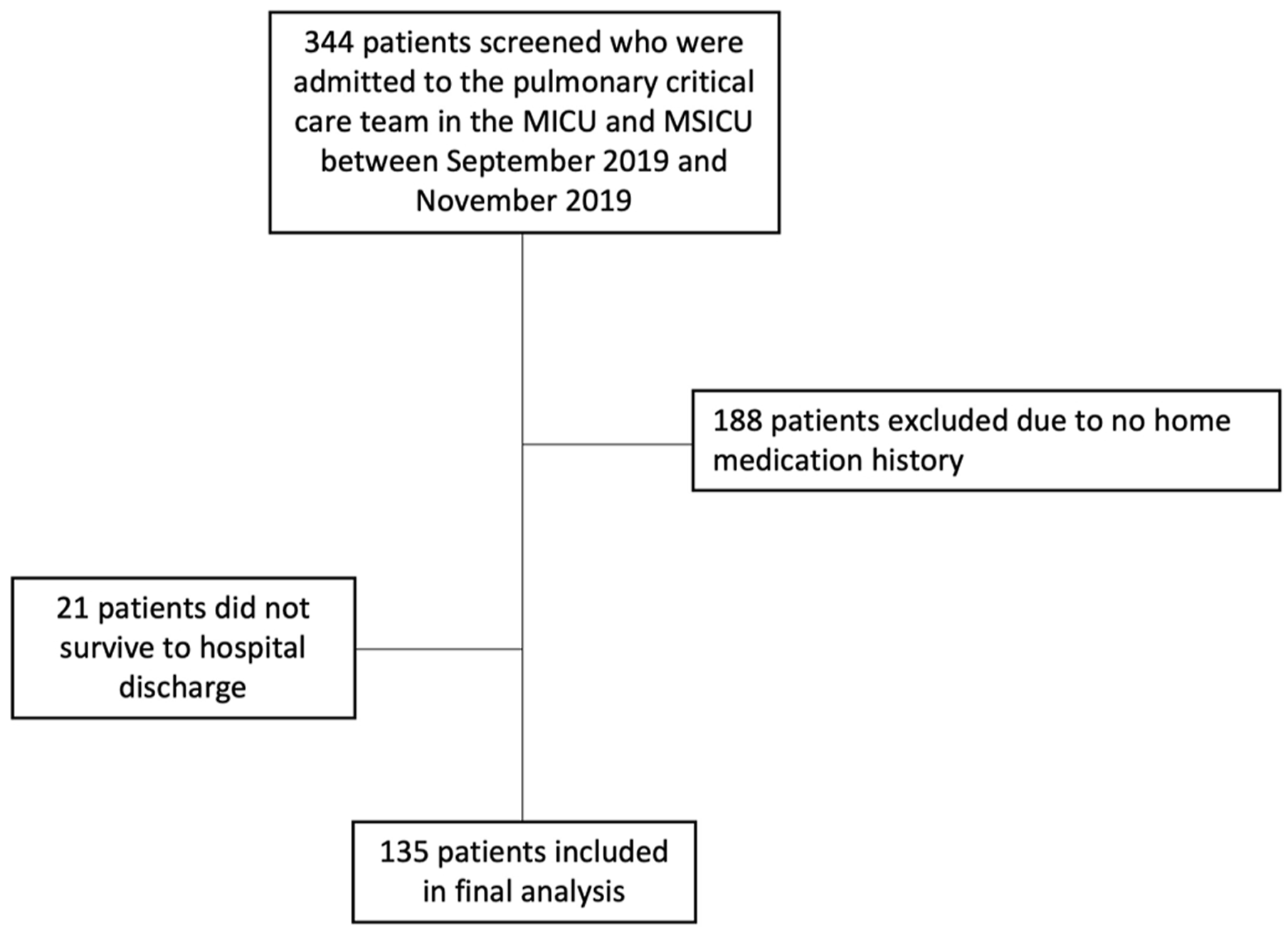
Opioid Continuation Upon ICU and Hospital Discharge.
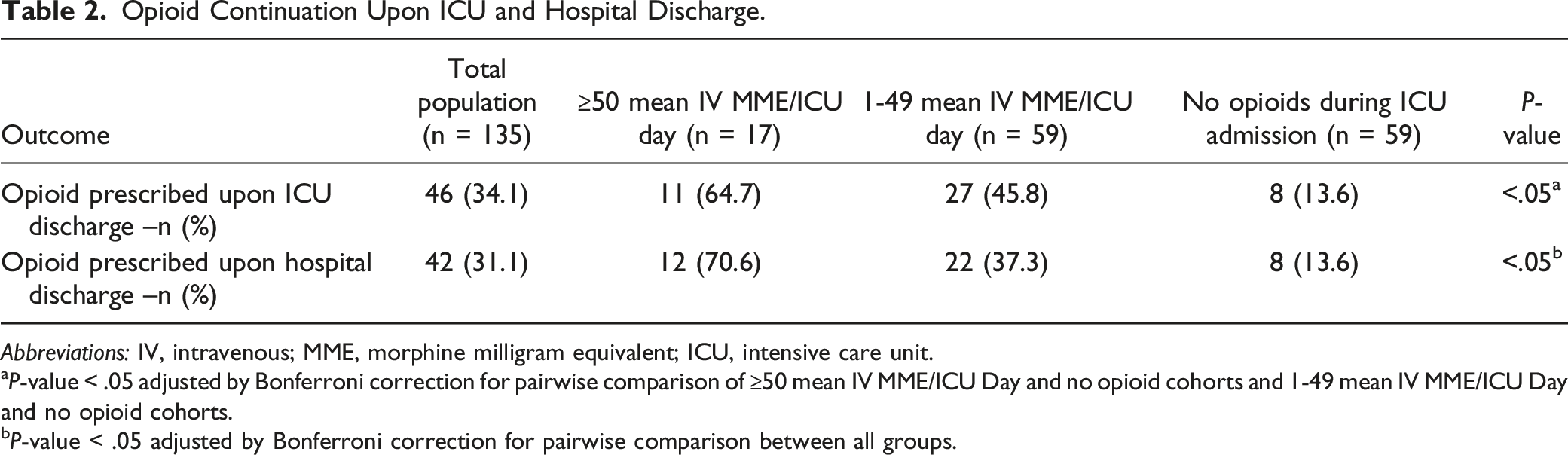
Abbreviations: IV, intravenous; MME, morphine milligram equivalent; ICU, intensive care unit.
aP-value < .05 adjusted by Bonferroni correction for pairwise comparison of ≥50 mean IV MME/ICU Day and no opioid cohorts and 1-49 mean IV MME/ICU Day and no opioid cohorts.
bP-value < .05 adjusted by Bonferroni correction for pairwise comparison between all groups.
Secondary Outcomes.
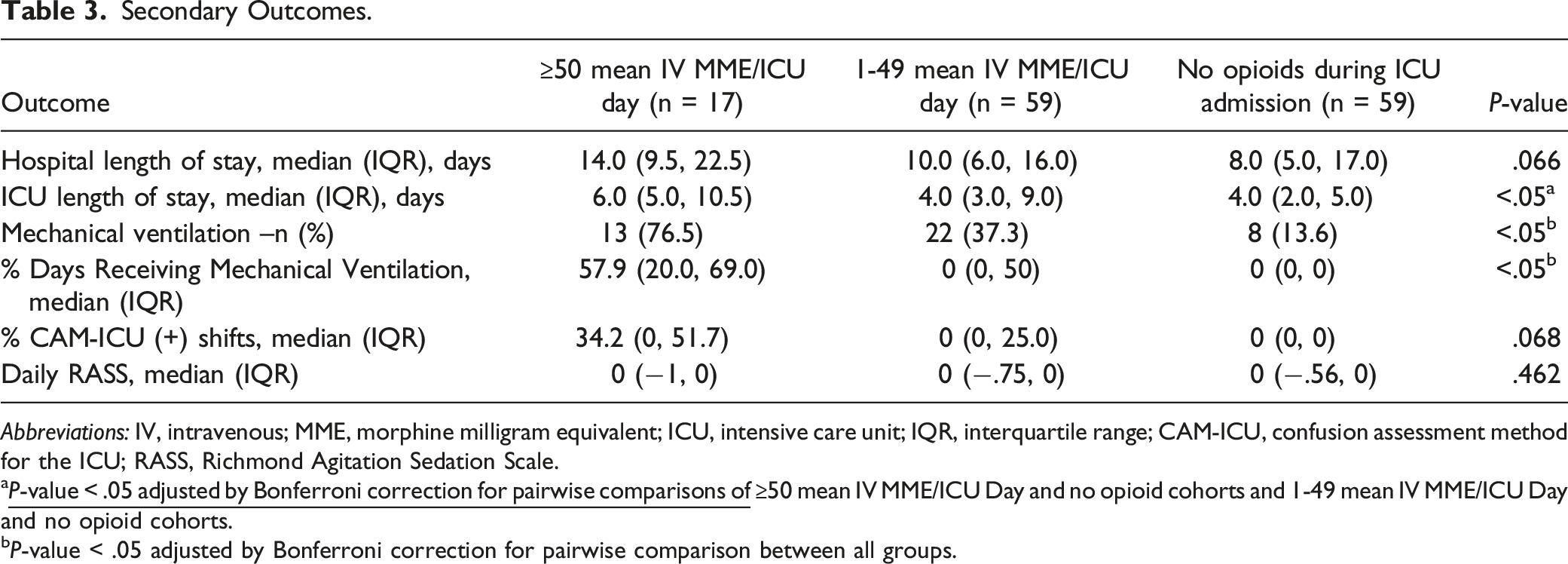
Abbreviations: IV, intravenous; MME, morphine milligram equivalent; ICU, intensive care unit; IQR, interquartile range; CAM-ICU, confusion assessment method for the ICU; RASS, Richmond Agitation Sedation Scale.
a
bP-value < .05 adjusted by Bonferroni correction for pairwise comparison between all groups.
ICU Opioid and Sedative Requirements.
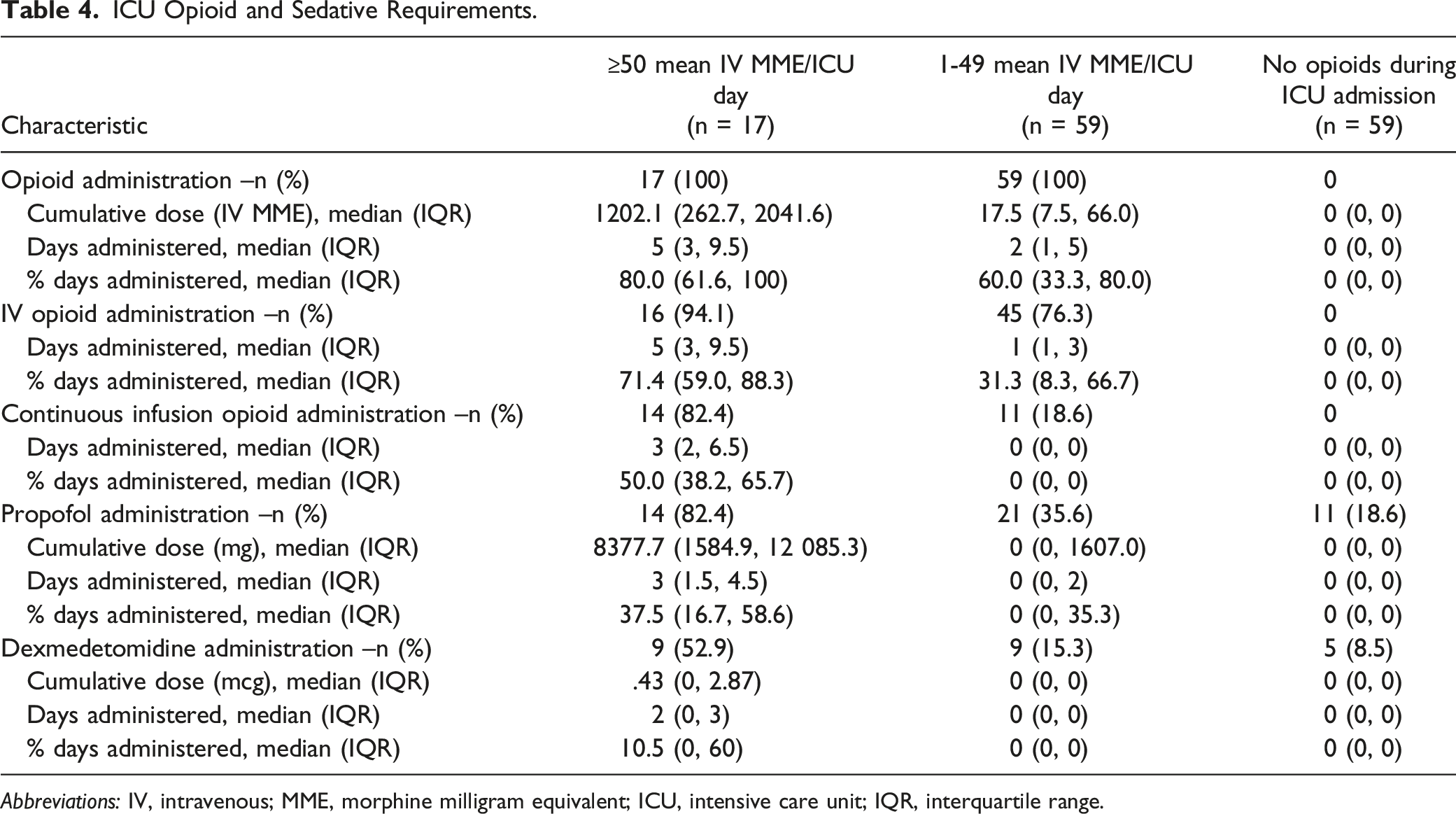
Abbreviations: IV, intravenous; MME, morphine milligram equivalent; ICU, intensive care unit; IQR, interquartile range.
Predictors of opioid prescribing upon hospital discharge.
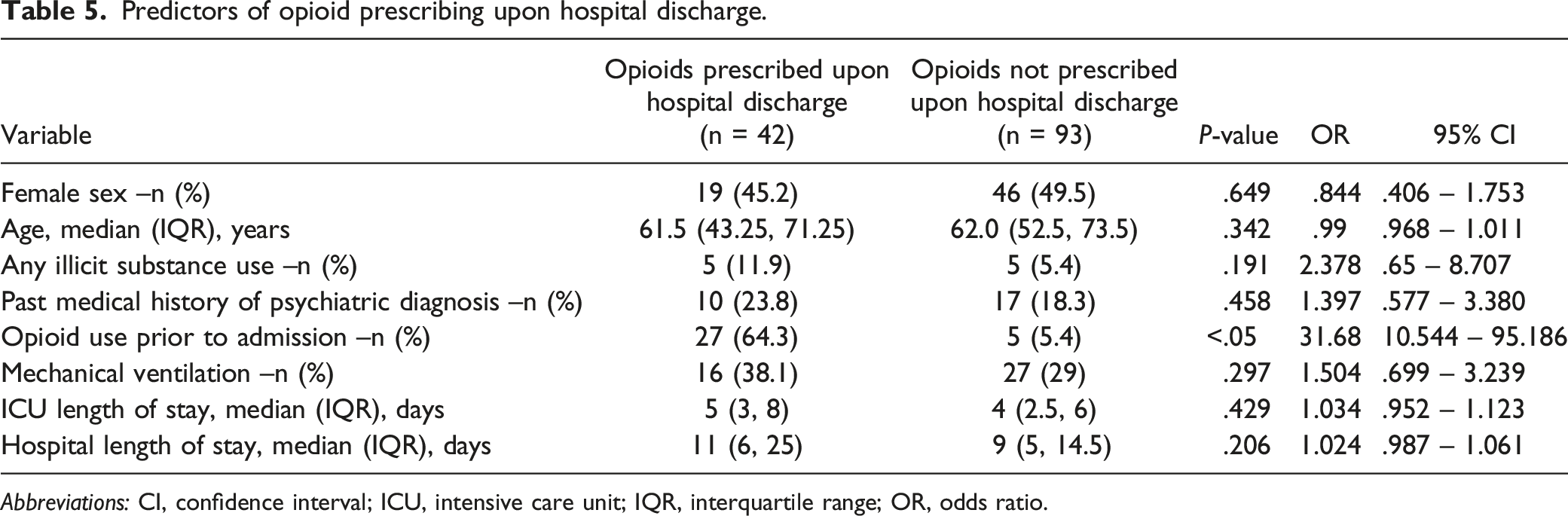
Abbreviations: CI, confidence interval; ICU, intensive care unit; IQR, interquartile range; OR, odds ratio.
Discussion
Acute pain in the ICU occurs for many reasons including procedures, injuries, comorbidities, and devices.2,4 Providers are challenged to appropriately assess and treat acute pain while also remaining vigilant to the public health crisis of opioid misuse and addiction.14,15 However, there is a lack of knowledge regarding how opioid use in the ICU impacts use across care transitions. Assessment of ICU opioid use in the overall population of this study reveals that 12.6% of patients received ≥50 mean IV MME/ICU day. Among those who did not receive ≥50 mean IV MME/ICU day, half of the patients received lower amounts while the remaining received no opioids at all.
There are several potential explanations for differences in opioid doses received among the cohorts. Preadmission opioid use is one reason for why certain patients may have received more opioids. About one-quarter of ICU patients received opioids prior to admission, which is consistent with previous studies examining opioid utilization in the ICU.10,12 Furthermore, significantly more patients who received ≥50 mean IV MME/ICU day were also taking an opioid prior to admission compared to patients receiving 1-49 mean IV MME/ICU day or no opioids. This does not, however, fully justify differences in ICU opioid use as only 41.2% of patients in the ≥50 mean IV MME/ICU day cohort were taking opioids prior to admission. Key differences in baseline characteristics and secondary outcomes offer additional possible explanations. The median age of patients receiving ≥50 mean IV MME/ICU day was 45 years, which is significantly younger than patients who received less opioids or no opioids. A potential relationship between age and inpatient opioid administration may exist. 9 However, the significance of this finding remains unclear, and warrants further research. Marijuana use was more common in patients who received ≥50 mean IV MME/ICU day. This finding aligns with the results of a recent retrospective pilot study, which suggests that marijuana use may increase opioid requirements in trauma patients. 16 However, the patients in our study were admitted to the pulmonary critical care service, and not a trauma service. Additional research investigating the effect of substance abuse on pain management in diverse ICU populations is warranted.
Though there was no difference in admission diagnosis among groups, nearly one-quarter of patients who received ≥50 mean IV MME/ICU day group experienced ARDS during ICU admission. High opioid doses in these patients may have been necessary to facilitate lung-protective mechanical ventilation and ventilator synchrony. 17 Additionally, nearly double the percentage of patients in the ≥50 mean IV MME/ICU day group experienced a procedure during ICU admission compared to patients with lower or no opioid requirements. Though our study population was admitted to the pulmonary critical care service, and management was primarily medical in nature, examples of procedures undergone by patients include biopsies, endoscopic procedures, vascular embolization, and drain insertion. Mechanical ventilation may have influenced opioid utilization as over three-quarters of patients in the ≥50 mean IV MME/ICU day group required mechanical ventilation. Finally, continuous infusion opioids likely contributed to differences in opioid utilization among cohorts as over 80% of patients in the ≥50 mean IV MME/ICU day group received a continuous infusion opioid compared to less than 20% of patients in the 1-49 mean IV MME/ICU day group.
Approximately one-third of patients in the overall study population received opioids following transfer to the floor or an opioid prescription upon hospital discharge. Patients who received more opioids in the ICU were more likely to experience both of these outcomes compared to those with lower requirements. This is demonstrated clearly as almost double the percentage and over five times the percentage of patients who received ≥50 mean IV MME/ICU day were discharged from the hospital with an opioid prescription compared to those who received 1-49 mean IV MME/ICU day and no opioids, respectively.
Although adjudication was not performed to determine specifically why opioids were prescribed upon ICU and hospital discharge, several rationalizations may be hypothesized. A recent painful procedure proximal to discharge represents one possible explanation. Additionally, chronic pain resulting from critical illness and ARDS cannot be ruled out.4,18 Pain resulting from opioid tolerance or opioid-induced hyperalgesia are additional concerns, particularly for patients with prolonged or large opioid requirements.19,20 However, basic science and clinical data for these complications are still evolving. It is noted that eight patients who received no opioids in the ICU were administered opioids upon transfer to the floor. Additionally, eight patients who received no opioids in the ICU were subsequently prescribed opioids upon hospital discharge. Inadequate assessment and management of pain in ICU represents one possibility. 21 Reassessment of home opioid use after ICU discharge is another possibility as one patient in the “opioid-free” ICU cohort who received opioids on the floor as well as six patients in the “opioid-free” ICU cohort who received an opioid prescription upon hospital discharge were taking opioids prior to admission.
The importance of opioid stewardship during transitions of care is highlighted by a recent retrospective cohort study of opioid naïve ICU patients which found that 36.7% of opioid prescriptions at hospital discharge were in excess of calculated predischarge requirements. 22 Of the 71 patients included in this study, 45% were discharged with an opioid prescription compared to 14.6% of opioid naïve patients in our study. Of note, this study utilized a mixed population of medical and cardiothoracic ICU patients, and the majority of opioid prescriptions were in patients who had been admitted to the cardiothoracic ICU. This finding correlates with other studies which have concluded that surgery is associated with persistent opioid use. 23 The population in this study was restrictive compared to our own as patients were required to receive IV opioids during mechanical ventilation. Our population may be more generalizable as less than half of patients in the overall cohort were mechanically ventilated or received IV opioids.
A recent large retrospective cohort study in Sweden found that 10.8% of patients developed chronic opioid use following ICU discharge compared to 31% of our total study population who were discharged with an opioid prescription. 23 Researchers also found several factors to be associated with continued opioid use including increased age, female sex, low education level, low income, preadmission opioid use, presence of comorbidities, surgery, and ICU LOS greater than 2 days. Of the predictors examined in our study, preadmission opioid use was the only factor found to be associated with opioid prescribing upon hospital discharge. Baseline characteristics between our population and the Swedish cohort are similar, and do not explain differences in findings. However, the median ICU LOS was 4 days compared to 1.5 days in the Swedish cohort, and it can be hypothesized that this contributed to increased prescribing. Nevertheless, rationalizing differences between this study and our own is challenging due to potential differences in practice between countries, absence of information regarding ICU opioid exposure in the Swedish cohort, and the fact that chronic opioid use was not evaluated in our study.
A retrospective review of 2595 mixed medical and surgical adult ICU patients from 2005-2008 found that only 12.2% of patients discharged from the hospital received opioids. 10 Preadmission opioid use was 23.1%, which is similar to our study. Once again, differences in practice between countries make comparison between this Canadian cohort and our study difficult. Additionally, absence of information regarding ICU patient management and opioid prescribing patterns prevents investigators and readers from making inferences as to whether ICU management contributed to differences in outpatient opioid prescribing.
Analysis of opioid prescribing in opioid naïve patients reveals that almost 30% of patients who received ≥50 mean IV MME/ICU day were opioid naïve and discharged on an opioid, which is over double compared to patients with lower or no opioid requirements. The potential effect of ICU opioid exposure on outpatient prescribing patterns in opioid naïve patients is especially significant as appropriate pain management is balanced with individual and societal risks for opioid misuse and abuse.15,23,24 A recent retrospective cohort study that evaluated opioid naïve patients who received opioids in the medical ICU or intermediate care unit found that the overall opioid continuation rate at hospital discharge was 31.8% compared to 14.6% of opioid naïve patients in our study. 25 Authors note that both hospital LOS and intubation were associated with continued opioid therapy at hospital discharge. The median hospital LOS for patients discharged on opioids was 25 days compared to 11 days in our study, and 80.9% of patients discharged on an opioid were intubated compared to 38.1% of patients in our study. Authors of this study also noted that the median pain score prior to discharge for patients discharged on opioids was zero, which would indicate that opioids had been initiated for other indications, such as sedation.
Our study expands on evolving and sparse literature characterizing opioid prescribing patterns at care transitions. These findings are unique as ICU opioid requirements are reported in a non-surgical medical ICU population consisting of patients receiving preadmission opioids as well as opioid naïve patients. Strengths of this study include documentation of pre-ICU baseline characteristics and ICU-specific patient management. Our study was prospective; this allowed for data to be verified in real time. Additionally, pharmacist-completed medication histories allow for accurate pre-admission opioid use to be ascertained. These medication histories are routinely compiled using multiple sources of information, including patients, family members, community pharmacies, as well as a state-wide prescription drug monitoring database. Several limitations must also be considered when interpreting these results. Selection bias may have been introduced since many patients were excluded due to the absence of a complete prior to admission medication history. Additionally, long-term opioid utilization cannot be established as only post-ICU and hospital discharge opioid use was examined. Although patients may have been prescribed an opioid upon discharge, it is not known whether these prescriptions were filled or taken. Conversely, it is not known whether patients who did not receive opioids on discharge were subsequently prescribed opioids in the outpatient setting due to their critical illness or another comorbidity. Absence of pain scores preclude inferences regarding the appropriateness of opioid prescriptions. Opioid adjuncts such as acetaminophen, gabapentinoids, lidocaine, and ketamine were not documented, and therefore, the potential impact on opioid prescribing patterns is not known. Finally, the single-center design is a limitation of external validity.
This study highlights the need for additional evidence in a number of areas, especially opioid stewardship. Our institution practices an analgesia-first strategy. 2 The most common IV and oral opioids in our ICUs are fentanyl and oxycodone, respectively. However, no formalized opioid weaning protocol exists to minimize inpatient opioid administration and outpatient prescribing upon hospital discharge. Considering the high percentage of patients who received continuous infusion opioids in the ≥50 mean IV MME/ICU day group, evidence examining reduction of continuous infusion opioids through utilization of “as needed” doses or oral opioids is necessary. Finally, future studies should consider the impact of ICU management and opioid intensity on long-term opioid utilization, misuse, and abuse.
Conclusion
To summarize, patients with higher mean daily ICU opioid requirements demonstrated a statistically significant increase in opioid prescribing post-ICU and hospital discharge. Despite preadmission opioid use, increased ICU opioid intensity was associated with a statistically significant increase in opioid prescribing at hospital discharge. Future research should examine opioid-minimizing strategies as well as the effect of ICU opioid use on long-term opioid prescribing patterns, abuse, and misuse.
Footnotes
Acknowledgments
The authors would like to thank Emily McTish and Lindsay Godman for their help with the data collection process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.